Apoprotein E Polymorphism and Coronary Artery...
6
Apoprotein E Polymorphism and Coronary Artery Disease Increased Prevalence of Apolipoprotein E-4 in Angiographically Verified Coronary Patients Timo Kuusi, Markku S. Nieminen, Christian Ehnholm, Hannele Yki-Jarvinen, Matti Valle, Esko A. Nikkila, and Marja-Riitta Taskinen Several studies have Indicated that genetic polymorphism of apolipoprotein (apo) E Is related to coronary artery disease (CAD). We therefore determined the apo E phenotype In 91 consecutive Finnish men with angiographically confirmed CAD. The apo E phenotype distribution differed significantly from that observed In the Finnish population (p<0.05). In the patient group, the frequency of the e4 allele was 0.324, which Is 1.4-fold higher than In the normal Finnish population and twice as high as In other Caucasian populations. Serum llpoprotelns and postheparin plasma llpase activities did not display any significant variation according to apo E phenotype. These studies confirm and extend, In a population with high e4 allele frequency, the previous data on the Impact of the e4 allele on the risk of CAD and suggest that the high e4 allele frequency In the Finnish population may be one factor contributing to Finns' Increased susceptibility to CAD. (Arteriosclerosis 9:237-241, March/April 1989) A polipoprotein E (apo E), a normal constituent of plasma chyiomicrons, very low density lipoproteins (VLDL), and high density lipoproteins (HDL), 1 binds with high affinity to receptors in liver and extrahepatic cells, thereby mediating the uptake of apo E-containing lipopro- teins, especially the cholesterol-enriched remnants of triglyceride-rich lipoproteins. 2 In addition, it is considered that an HDL subtraction containing apo E plays an impor- tant role in the reverse transport of cholesterol from peripheral cells to the liver. 23 The genetic polymorphism of apo E is due to three common alleles, c2, e3, and €4, at a single autosomal gene locus. 4 - 7 These alleles determine the six pherto- types E2/2, E3/3, E4/4, E4/2, E4/3, and E3/2. The isopro- tein apo E-2, a product of the e2 allele, is a mutant differing from the most common isoprotein apo E-3 by a single amino acid interchange (arg158 -> cys158). This mutation leads to a protein that has a much lower affinity for the cellular apolipoprotein receptor. 8 The other mutant, apo E-4, differs from the parent apo E-3 by a single cys112 -»• arg112 interchange. 9 Low density lipoprotein (LDL) metabolism is associated with the apo E polymor- phism, and as much as 16% of the genetic variance in LDL concentration can be accounted for by allelic differ- From the First, Second, and Third Departments of Medicine and the Department of Radiodiagnostics, University of Helsinki, and the National Public Health Institute, Helsinki, Finland. Esko A. Nikkila died on September 21, 1986. This research was supported by grants from the Finnish State Medical Research Council, the Finnish Heart Foundation, the Sigrid Juselius Foundation, and the University of Helsinki. Address for reprints: Timo Kuusi, M.D., Second Department of Medicine, University of Helsinki, Haartmaninkatu 4, 00290 Hel- sinki, Finland. Received July 7,1987; revision accepted November 1,1988. ences at the apo E gene locus. 10 Thus, subjects with the phenotype E3/2 have, on the average, 20% lower, and E4/3 subjects have 10% higher levels of LDL cholesterol than do subjects with phenotype E3/3. 11 Since LDL metab- olism is closely associated with atherogenesis, it is plau- sible to presume that the apo E genotype may convey a susceptibility to atherosclerosis. The apo E gene frequency has been determined in survivors of myocardial infarctions 12 ' 13 and in subjects with angtographlcalry verified coronary artery disease (CAD). 1416 These studies indicated that the «4 allele is associated with early development of coronary heart disease (CHD), whereas the e2 allele is less common in coronary patients. In a recent study, the Finns were shown to have a markedly higher «4 allele frequency than other Caucasian popula- tions studied (0.227 vs. 0.11 to 0.175), whereas the «2 allele frequency was low (0.041 vs. 0.08 to 0.17). 1817 It was suggested that this might be one of several factors respon- sible for the high incidence of CHD in Finland. To evaluate the significance of the apo E polymorphism as a risk factor for CAD, we determined apo E phenotypes in 91 consec- utive male patients who underwent coronary angiography before coronary bypass surgery. Methods Subjects Patients were recruited for the study between 1985 and 1986 from the First Department of Medicine, University of Helsinki. All patients younger than 60 years of age who were to have coronary angiography because of long- standing angina were contacted at their admittance; the purpose of the study was explained, and informed con- sent was obtained. The study protocol was approved by the Ethical Committee of Meilahti Hospital. The study 237 by guest on June 14, 2018 http://atvb.ahajournals.org/ Downloaded from
Transcript of Apoprotein E Polymorphism and Coronary Artery...

Apoprotein E Polymorphismand Coronary Artery Disease
Increased Prevalence of Apolipoprotein E-4 inAngiographically Verified Coronary Patients
Timo Kuusi, Markku S. Nieminen, Christian Ehnholm, Hannele Yki-Jarvinen,Matti Valle, Esko A. Nikkila, and Marja-Riitta Taskinen
Several studies have Indicated that genetic polymorphism of apolipoprotein(apo) E Is related to coronary artery disease (CAD). We therefore determined theapo E phenotype In 91 consecutive Finnish men with angiographically confirmedCAD. The apo E phenotype distribution differed significantly from that observed Inthe Finnish population (p<0.05). In the patient group, the frequency of the e4 allelewas 0.324, which Is 1.4-fold higher than In the normal Finnish population and twiceas high as In other Caucasian populations. Serum llpoprotelns and postheparinplasma llpase activities did not display any significant variation according to apo Ephenotype. These studies confirm and extend, In a population with high e4 allelefrequency, the previous data on the Impact of the e4 allele on the risk of CAD andsuggest that the high e4 allele frequency In the Finnish population may be one factorcontributing to Finns' Increased susceptibility to CAD.(Arteriosclerosis 9:237-241, March/April 1989)
A polipoprotein E (apo E), a normal constituent ofplasma chyiomicrons, very low density lipoproteins
(VLDL), and high density lipoproteins (HDL),1 binds withhigh affinity to receptors in liver and extrahepatic cells,thereby mediating the uptake of apo E-containing lipopro-teins, especially the cholesterol-enriched remnants oftriglyceride-rich lipoproteins.2 In addition, it is consideredthat an HDL subtraction containing apo E plays an impor-tant role in the reverse transport of cholesterol fromperipheral cells to the liver.23
The genetic polymorphism of apo E is due to threecommon alleles, c2, e3, and €4, at a single autosomalgene locus.4-7 These alleles determine the six pherto-types E2/2, E3/3, E4/4, E4/2, E4/3, and E3/2. The isopro-tein apo E-2, a product of the e2 allele, is a mutantdiffering from the most common isoprotein apo E-3 by asingle amino acid interchange (arg158 -> cys158). Thismutation leads to a protein that has a much lower affinityfor the cellular apolipoprotein receptor.8 The other mutant,apo E-4, differs from the parent apo E-3 by a singlecys112 -»• arg112 interchange.9 Low density lipoprotein(LDL) metabolism is associated with the apo E polymor-phism, and as much as 16% of the genetic variance inLDL concentration can be accounted for by allelic differ-
From the First, Second, and Third Departments of Medicineand the Department of Radiodiagnostics, University of Helsinki,and the National Public Health Institute, Helsinki, Finland.
Esko A. Nikkila died on September 21, 1986.This research was supported by grants from the Finnish State
Medical Research Council, the Finnish Heart Foundation, theSigrid Juselius Foundation, and the University of Helsinki.
Address for reprints: Timo Kuusi, M.D., Second Department ofMedicine, University of Helsinki, Haartmaninkatu 4, 00290 Hel-sinki, Finland.
Received July 7,1987; revision accepted November 1,1988.
ences at the apo E gene locus.10 Thus, subjects with thephenotype E3/2 have, on the average, 20% lower, andE4/3 subjects have 10% higher levels of LDL cholesterolthan do subjects with phenotype E3/3.11 Since LDL metab-olism is closely associated with atherogenesis, it is plau-sible to presume that the apo E genotype may convey asusceptibility to atherosclerosis.
The apo E gene frequency has been determined insurvivors of myocardial infarctions12'13 and in subjects withangtographlcalry verified coronary artery disease (CAD).1416
These studies indicated that the «4 allele is associated withearly development of coronary heart disease (CHD),whereas the e2 allele is less common in coronary patients.In a recent study, the Finns were shown to have a markedlyhigher «4 allele frequency than other Caucasian popula-tions studied (0.227 vs. 0.11 to 0.175), whereas the «2allele frequency was low (0.041 vs. 0.08 to 0.17).1817 It wassuggested that this might be one of several factors respon-sible for the high incidence of CHD in Finland. To evaluatethe significance of the apo E polymorphism as a risk factorfor CAD, we determined apo E phenotypes in 91 consec-utive male patients who underwent coronary angiographybefore coronary bypass surgery.
MethodsSubjects
Patients were recruited for the study between 1985 and1986 from the First Department of Medicine, University ofHelsinki. All patients younger than 60 years of age whowere to have coronary angiography because of long-standing angina were contacted at their admittance; thepurpose of the study was explained, and informed con-sent was obtained. The study protocol was approved bythe Ethical Committee of Meilahti Hospital. The study
237
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from

238 ARTERIOSCLEROSIS VOL 9, No 2, MARCH/APRIL 1989
Table 1. Presence of Risk Factors for Coronary Artery Disease In Subjects with DifferentApoproteln E Phenotypes
Risk factor
Smoking*
Hypertension*
Hypercholesterolemla*
Diabetes
4/4(n=8)
50(4)
50(4)
25(2)
0(0)
4/3(n=41)
59(24)
44(18)
7 (3)
5 (2)
Apo E phenotype
3/3(n=34)
62(21)
65(22)
15 (5)
0 (0)
4/2(n=2)
100(2)
50(1)
0(0)
0(0)
3/2(n=6)
67(4)
50(3)
17(1)
0(0)
The values are the percentages of numbers in the group wtth each phenotype. The numbers In parenthesesindicate the number of affected individuals.
•The observed distribution of this risk factor among the different apo E phenotype subjects did not differsignificantly (p>0.05) from the expected distribution by the x2 test
Apo=apoprotein.
Table 2. Use of Drugs among Subjects with Different Apoproteln E Phenotypes
Beta-blockers*
Diuretics*
Ca++-antagonists*
Prazosin*
Ctofibratet
4/4(n=8)
100(8)
38(3)
50(4)
13(1)
0(0)
4/3(n=41)
80(33)
29(12)
66(27)
0 (0)7 (3)
Apo E phenotype
3/3(n=34)
82(28)
32(11)
50(17)
3 (1)0 (0)
4/2(n=2)
100(2)
0(0)
100(2)
0(0)
0(0)
3/2(n=6)
50(3)
33(2)
67(4)
0(0)
17(1)
Values are the percentage of numbers in the group wtth each phenotype. The values in parentheses are thenumbers of subjects on the drug.
The observed distribution of use of this drug did not differ from the expected (p>0.05 by the x2 test).Trie x2 test was not perfonmed because of the small number of subjects taking this drug.Apo=apoprotein.
group included 91 men with positive angiography findings(see below). The mean age of the patients was 52 years(range, 37 to 60 years), and all had a well-documentedhistory of coronary symptoms for at least 2 years. Thepresence of the common CAD risk factors in the differentapo E phenotypes is shown in Table 1. The use ofcardiovascular drugs was common but similar among ourpatients belonging to different apolipoprotein E pheno-types (Table 2). Blood samples for lipoprotein and apo-protein analysis were taken at 8 A.M. after an overnightfast. This was followed by an intravenous injection of 100ILJ/kg of heparin for the collection of postheparin plasmainto precooled tubes 5 and 15 minutes later.
Coronary AngiographyCAD was confirmed by selective arteriography. The
standard Judkins technique for selective coronary angi-ography in multiple views was performed.18 A translumi-nal narrowing of 50% or more was defined as significant.A total of 51 subjects had triple-vessel disease, 30 haddouble-vessel disease, and 10 had-single vessel disease.In the single-vessel group, all patients had severe narrow-ing (2: 75%) of the left anterior descending vessel. Allpatients underwent bypass surgery.
Llpld and Lipoprotein AnalysesSerum total and lipoprotein cholesterol and triglycerkJe
concentrations were determined by enzymatic methodswith commercially available kits (Boehringer GmbH, FRG,
No. 236691 and No. 297771, respectively) in a Kone Olli-Canalyzer (Kone Limited, Espoo, Finland). Apo A-l and A-llwere determined by immunoturbidimetry by using mono-specific gamma globulins (Boehringer GmbH, FRG, No.726478 and No. 726486). Apo B concentration wasdetermined by radial immunodiffusion on commerciallyavailable plates (Behringwerk GmbH, FRG). The separa-tion of lipoprotein fractions was carried out by sequentialultracentrifugation with a Kontron TFT 45.6 rotor operatedat 105 gn and 4°C in a Beckman L7-70 ultracentrifuge.19
Centrifugation times of 18 hours, 20 hours, and 72 hoursat densities of 1.006 g/ml, 1.063 g/ml, and 1.21 g/ml wereused for the separation of VLDL, LDL, and HDL, respec-
Table 3. Prevalence of Apolipoprotein E PhenotypesIn Patients with Positive Coronary Anglograms
ApoE phenotype
E4/4
E4/3
E4/2
E3/3
E3/2
E2/2
CAD patients
Observed
8
41
2
34
6
0
Finnish population
Expected*
5
30
2
49
5
0
'Expected phenotype distribution obtained using the e-allelefrequencies In the Finnish population1" (*2=10.6, p<0.05).
CAD=coronary artery disease, Apo=apoprotein.
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from

e4-ALLELE FREQUENCY IN CORONARY DISEASE Kuusi et al. 239
Table 4. e Allele Frequencies In Normal Finns and In Patients with Coronary Heart Disease
Population e4 e3 e2
Normal Finns
Finns with CAD
0.227±0.013
0.324+0.037*0.733±0.0170.632±0.044*
0.041 ±0.0150.044±0.039*s
Values lnclude±SD*p<0.001, NS=not significantly different from the corresponding allele frequency in normal Finns by f test.The data on normal Finns is from reference 16.
Table 5. Plasma Llpoprotelns, Apoprotelns A and B, and Postheparln Plasma UpoprotelnLlpase and Hepatic Llpase Activities according to Apollpoproteln E Phenotype In Men withCoronary Heart Disease
Triglycerides (mmot/l)
Cholesterol (mmol/1)
VLDL cholesterol
LDL cholesterol
HDL cholesterol
Apo A-l (g/1)
Apo A-ll (g/1)
Apo B (g/1)
LPL (/imol/h/ml)
HL (/imol/h/ml)
E4/4(n=8)
2.07
(0.19)
6.68
(0.63)
0.60
(0.09)
4.80
(0.64)
1.20
(0.12)
0.93
(0.06)0.26
(0.01)
1.18
(0.13)
17.5
(1.5)
33.3
(4.2)
E4/3(n=41)
2.03
(0.17)
6.05
(0.14)
0.61
(0.05)
4.29
(0.14)
1.16
(0.04)
0.94
(0.03)
0.25
(0.01)
1.16
(0.05)
22.6
(1.4)
29.0
(2.1)
E3/3(n=34)
2.27
(0.20)
6.44
(0.19)
0.69
(0.05)
4.62
(0.18)
1.14
(0.04)
0.97
(0.03)
0.24
(0.01)
1.15
(0.07)
20.9
(1.0)
32.8
(2.8)
E4/2(n=2)
2.27
(0.48)
6.32
(0.37)
0.58
(0.13)
4.38
(0.29)
1.36
(0.05)
1.00
(0.11)
0.27
(0.05)
1.12
(0.01)
19.0
(0.2)
23.4
(1.2)
E3/2(n=6)
2.33
(0.48)
5.72
(0.59)
0.66
(0.10)
3.87
(0.59)
1.14
(0.18)
0.92
(0.07)
0.22
(0.02)
1.02
(0.07)
16.2
(2.4)
32.8
(2.8)
The values are means±SEM.The differences for all parameters between the different apo E phenotypes were tested by one-way analysis of
variance and were nonsignificant (p>0.05) in all tests.VLDL=very low density lipoproteln, LDL=low density lipoprotein, HDL=hlgh density lipoprotein, apo=apoprotein,
LPL=lipoprotein lipase, HL=hepatic lipase.
tivery. The lipoprotein lipase (LPL) and hepatic lipase (HL)activities of postheparin plasma were determined by animmunochemical assay.20
Apoproteln E PhenotyplngThis was done by isoelectric focusing as described.21
Statistical MethodsThe standard deviations of the gene frequencies were
calculated as described earlier.16 The differences betweenserum lipoproteins, apolipoproteins, and postheparin plasmalipase activities of various apo E phenotype subjects weretested by one-way analysis of variance. A nonpaired ftestwas used to evaluate the differences between the allelefrequencies of CAD patients and normal Finns. The devi-ation of the observed phenotype distribution from theexpected was tested using the x2 test.
ResultsOf the six common apo E phenotypes, five were
observed in the CAD patients; only the phenotype E2/2was not represented (Table 1). In this respect, our CADmaterial did not differ from that in the average Finnishpopulation. However, the observed phenotype frequen-cies were significantly different from the expected distri-bution as judged from the x2 test of the goodness-of-fit ofCAD data to the expected frequencies based on theFinnish allele frequencies Ot2=10.6, p<0.05, 5x2 com-parison) (Table 3). This was mainly due to an increase inthe number of CAD patients with the phenotypes E4/4 andE4/3 and a corresponding decrease of the E3/3 pheno-types as compared with the distribution of the E pheno-types in the Finnish population. This enrichment of apoE-4 phenotypes was independent of age and severity ofcoronary heart disease (i.e., number of narrowed vessels)as judged from the £4 allele frequencies of 0.337 in
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from

240 ARTERIOSCLEROSIS VOL 9, No 2, MARCH/APRIL 1989
a
ogj
joo
200
150
100
50
E4/4 E3/3 E4/2 E3/2
1.2
1.1
1.0
0.9
oTJ
oTJTO
w
APOLJPOPROTEIN E PHENOTYPE
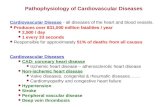
Figure 1. Mean concentrations (mg/dl) of low density lipopro-tein (LDL) cholesterol (open bars) and apoprotein (apo) B (shadedbars) in 91 coronary patients according to apo E phenotype. Thedifferences of LDL cholesterol and apo B between the apo Ephenotypes are not significant (p>0.05) by one-way analysis ofvariance.
60
iooI
20
E4/4 E4/3 E3/3 E4/2 E3/2
O
1.2 ioTJTOo
1.0 ?
0.8
0.6
APOUPOPROTEIN E PHENOTYPEFigure 2. Mean concentrations (mg/dl) of high density llpopro-tein (HDL) cholesterol (open bars) and apoprotein (apo) A-l(shaded bars) in 91 coronary patients according to apo Ephenotype. The differences of HDL cholesterol and apo A-lbetween the apo E phenotypes are not significant (p>0.05) byone-way analysis of variance.
triple-vessel disease and 0.300 in patients with mildercoronary narrowing. The c4 allele frequency in the CADpatients (0.324) was 1.4-fold higher than in the Finnishpopulation (0.227) (p<0.001), and this increase in the e4allele was compensated for by a corresponding decreasein the e3 allele frequency (Table 4).
Serum lipoproteins, A-l, A-ll, and B, and postheparinplasma lipolytic enzyme activities were similar in CADpatients with different apo E phenotypes as judged on thebasis of one-way analysis of variance (Table 5). However,the mean LDL cholesterol and apo B values tended todecrease from the apo E-4 phenotypes to apo E-2 phe-notypes (Figure 1), while the mean serum HDL choles-terol and A-l and A-ll levels were similar in different apo Ephenotypes (Figure 2 and Table 5). Similarly, serum
triglycerides and the postheparin plasma Upases, LPL andHL, were similar in the different apo E phenotype groups(Table 5).
Discussion
Our observation of a significantly increased frequencyof the e4 allele in patients with angiographically verifiedCAD is in accordance with some previous reports.131415
However, Utermann et al.12 were not able to confirm thisfinding. One reason for the unambiguous enrichment ofthe e4 allele among our CAD patients is probably that theclinical criteria required before a patient was subjected tocoronary angiography were strict. All patients had had awell-documented history of coronary symptoms for atleast 2 years. Another aspect is the young age of thepatients in the present study; the mean age was only 52years. Lenzen et al.15 observed significant differences inthe prevalence of apo E isoforms in patients with early andlate onset of infarction. They noted that 60% of E4/3patients had suffered infarction before the age of 60 andonly 40% later, while in E3/2 patients this age dependencywas reversed. In this respect, our increased prevalence ofe4 allele is in good accordance with earlier studies inyoung CAD patients.1315 Apolipoprotein E2-containingphenotypes are more rare in Finns than in other Cauca-sians.131617-22'23-24 The e2 allele frequency was also towin the CAD patients and did not differ from that in thegeneral population. Thus, the impact of e2 allele on theCAD risk seems to be of minor importance in Finns, unlikein other populations.12-14
Several recent studies have demonstrated associationsbetween the e4 allele and increased LDL cholesterollevels and the e2 allele and low LDL cholesterol in normalsubjects10111524; a similar association has been found inpatients with myocardial infarction.15-25 An analogoustrend was observed in the current study, although therange of serum LDL cholesterol was relatively narrow, butthis association was not statistically significant. Recentcalculations show that the variation of serum cholesterolaccording to the apo E phenotype covers only 2.8% of thevariation in the CAD risk.17 Accordingly, the apo E phe-notypes probably can influence the CAD risk throughmechanisms not related to changes in fasting plasmalipoproteins (see below). Notably, only one subject withE4/3 phenotype had hyper-B-apoproteinemia,26 thus rul-ing out the contribution of this disorder to the presentresults. However, in the different apo E phenotypes, thegenetic variation of apo B was more consistent than thatof LDL cholesterol (Figure 1). This applies especially tothe E4/3 phenotypes where the mean LDL cholesterolwas tower than expected, probably since three patients inthis group were on clofibrate treatment. In fact, the survi-vors of myocardial infarction in Finland have, at present,LDL cholesterol values quite similar to those of matchedcontrol subjects, whereas their LDL protein content iselevated.27 Thus, LDL protein appears to be a betterdiscriminator than LDL cholesterol for CAD in the Finnishpopulation.27
The VLDL and HDL lipoproteins and the postheparinplasma LPL and HL activities were similar among the
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from

64-ALLELE FREQUENCY IN CORONARY DISEASE Kuusi et al. 241
different phenotypes in the CAD patients. Also, previousstudies have shown that serum HDL cholesterol andtriglyceride concentrations do not vary significantly accord-ing to apo E phenotype.1516 This suggests that the apo Ephenotype dependent variation in LDL concentration prob-ably is not due to alterations in the VLDL-intermediatedensity lipoprotein-LDL cascade but, rather, is caused byaltered catabolism of LDL This lipoprotein class is catab-olized through receptor-mediated uptake in liver andextrahepatic tissues. These apo B/E receptors also bindapo E,28 and it is conceivable that the different bindingaffinities for the genetic isoforms of apo E to thesereceptors can up- or down-regulate them and, conse-quently, changes in LDL metabolism15.2629 result. More-over, recent studies have suggested that even the absorp-tion of dietary cholesterol30 and the clearance of dietarylipids31 are associated with the apo E phenotype. Thisvariation in lipid metabolism according to apo E pheno-type does not need to be reflected in changes of serumlipids and lipoproteins determined in fasting serum sam-ples. Overall, it is tempting to suggest that these variationsof lipoprotein metabolism according to the apo E pheno-type probably influence the atherosclerotic process and,due to the high «4 allele frequency, might also contributeto the increased prevalence of CAD in Finland.
References1. Shore VG, Shore B. Heterogeneity of human plasma very
low density lipoproteins. Separation of species differing Inprotein components. Biochemistry 1973;12:502-607
2. Mahley RW. Atherogenic hyperiipoprotelnemia. The cellularand molecular biology of plasma lipoproteins altered bydietary fat and cholesterol. Med Clin North Am 1982;66575-400
3. Basu SK, Ho YK, Brown MS, Bllhelmer DW, AndersonRGW, Goldstein JL Biochemical and genetic studies on theapolipoprDtetn E secreted by mouse macrophages and humanmonocytes. J Biol Chem 198225:9788-9795
4. Utermann G, Langenbreck U, Belslgel U, Weber W.Genetics of the apollpoprotein E system in man. Am J HumGenet 1980;32:339-347
5. Zannls V, Just PW, Breslow JL. Human apolipoprotein Eisoproteln subclasses are genetically determined. Am J HumGenet 1981;33:11-24
6. Rail SC, Welsgraber KH, Mahley RW. Human apolipopro-tein E. The complete amino add sequence. J Biol Chem1982257:4171-4178
7. Ward«ll MR, Suckling PA, Janus ED. Genetic variation inhuman apolipoprotein E. J Upld Res 198223:1174-1182
8. Welsgraber KH, Innerarity TL, Mahley RW. Abnormallipoprotein receptor-binding activity of the human E apopro-tein due to cystelne-arglnlne interchange at a single she. JBiol Chem 1982257:2518-2521.
9. Welsgraber KH, Rail SC, Mahley RW. Human E apoprotelnheterogeneity. Cystelne-arginlne interchange in the aminoadd sequence of the apo-E Isoforms. J Biol Chem 1981;256:9077-9083
10. Sing CF, Davfgnon J. Role of apolipoprotein E polymor-phism in determining normal lipid and lipoprotein variation.Am J Hum Genet 1985:37268-285
11. Robertson FW, Cummlng AM. Effect of apoproteln Epolymorphism on serum lipoprotein concentration. Arterio-sderosis 1985;5:283-92
12. Utermann G, Hardewlg A, Zlmmer F. Apolipoprotein Ephenotypes in patients with myocardial Infarction. Hum Genet1984;65237-241
13. Cummlng AM, Robertson FW. Polymorphism at theapoprotein-E locus In relation to risk of coronary disease.Clin Genet 198425510-313
14. Menzel H-J, Kladetzky R-G, Assmann G. Apolipoprotein Epolymorphism and coronary artery disease. Arteriosclerosis1983:3:310-315
15. Lenzen HJ, Assmann G, Buchwalsky R, Schutte H. Asso-dation of apolipoprotein E polymorphism, low-density lipo-protein cholesterol and coronary artery disease. Clin Chem1986:325:778-781
16. Ehnholm C, Lukka M, Kuusi T, Nikklla EA, Utermann G.Apolipoprotein E polymorphism in the Finnish population:gene frequencies and relation to lipoprotein concentrations.J LJpid Res 198627227-235
17. Davlgnon J, Gregg RE, Sing CF. Apolipoprotein E polymor-phism and atherosclerosis. Arteriosclerosis 1988;8:1-21
18. Judklns MP. Selective coronary arteriography. Radiology1967:89:815-819
19. Havel RF, Eder HS, Bragdon JH. The distribution andchemical composition of urtracentrtfugally separated lipopro-teins In human serum. J Clin Invest 1955:34:1345-1353
20. Huttunen JK, Ehnholm C, Klnnunen PKJ, Nlkkila EA. Animmunochemical method for selective measurement of twotriglyceride Upases in human postheparin plasma. Clin ChimActa 1975:63335-347
21. Pagnan A, Havel RJ, Kane JP, Kotite L Characteristics ofhuman very low density lipoproteins containing two electro-phorerjc populations: double prebetalipoproteinemia and pri-mary dysbetalipoproteinemia. J LJpid Res 1977:18:613-622
22. Havel RJ. Familial dysbetalipoproteinemia: new aspects ofpathogenesis and diagnosis. Med Clin North Am 1982;66:441-454
23. Utermann G, Klndermann I, Kaffarnlk H, Stelnmetz A.Apolipoprotein E phenotypes and hyperiipidemia. Hum Genet1984;65:232-236
24. Davlgnon J, Sing CF, Lusslsr-Cacan S, Bouthllller D.Xanthelasma, latent dyslipoprotelnemia and atherosclerosis:Contribution of apo E polymorphism. In: DeGennes JL, ed.Latent dyslipoprotelnemia and atherosderosis. New York:Raven Press, 1984:213-223
25. Assmann G, Lenzen HJ. Apolipoprotein E-polymorphismus,hyperilptdamle und herzinfarktrisiko. Internist 198526:692-700
26. Snkterman A, Shapiro S, Marpote D, Skinner B, Teng B,Kwtterovlch PO Jr. Association of coronary atherosclerosiswith hyperapobetaproteinemia (increased protein but normalcholesterol levels in human plasma low density lipoproteins).Proc Nati Acad Sd USA 1980;77:604-608
27. Kaupplnen-Mflkelln R. Serum lipoproteins and postheparinplasma llpase activities in patients with myocardial infarction[Thesis]. Helsinki: University of Helsinki, 1985:1-202
28. Goldstein JL, Klta T, Brown MS. Defective lipoproteinreceptors and atherosderosis. Lessons from an animalcounterpart of familial hypercholesterolemia. N Engl J Med1983:309288-296
29. Gregg RE, Zech LA, Schaefer EJ, Stark D, Wilson D,Brewer HB Jr. Abnormal metabolism of apolipoprotein E4 inhumans. J Clin Invest 1986:78:815-821
30. Kesinleml YA, Ehnholm C, Mkrttinen TA. ApolipoproteinE phenotype is related to intestinal cholesterol absorptioneffidency. J Clin Invest 1987:80:578-581
31. Welntraub MS, Elsenberg S, Breslow JL Dietary fatdearance in normal subjects is regulated by genetic variationin apolipoprotein E. J Clin Invest 1987:80:1571-1577
Index Terms: lipoproteins • apoiipoprotein E polymorphism • coronary heart disease • atherosclerosis • genetics
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from

T Kuusi, M S Nieminen, C Ehnholm, H Yki-Järvinen, M Valle, E A Nikkilä and M R Taskinenapolipoprotein E-4 in angiographically verified coronary patients.
Apoprotein E polymorphism and coronary artery disease. Increased prevalence of
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1989 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleArteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.9.2.2371989;9:237-241Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/9/2/237World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document.Permissions and Rights Question and AnswerFurther information about this process is available in theis being requested is located, click Request Permissions in the middle column of the Web page under Services.Clearance Center, not the Editorial Office. Once the online version of the published article for which permission
can be obtained via RightsLink, a service of the CopyrightArteriosclerosis, Thrombosis, and Vascular Biology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 14, 2018http://atvb.ahajournals.org/
Dow
nloaded from


















