Annex 2: Clinical workstream
88
Annex 2: Clinical workstream Scarborough ASR | 21 January 2019
Transcript of Annex 2: Clinical workstream

Annex 2: Clinical workstream
Scarborough ASR | 21 January 2019

2
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
▪ Further refinement of clinical models and key questions
Contents

3
The Clinical Reference Group (CRG) has met four times
Discussion agenda
▪ Refine detailed descriptions of clinical models
▪ Review of activity shifts under each clinical model (following discussions with CDs/Deputy CDs and other clinical leads)
▪ Provide update on financial analysis and show preliminary outputs
▪ Refine Case for Change
▪ Explore best practice clinical pathways
▪ Explore potential clinical models for individual service lines
▪ Discuss how these come together into whole hospital clinical models taking into account key clinical interdependencies
▪ Agree long list for more detailed review and analysis
▪ Introduction, objectives and ways of working
▪ Review case for change
– Clinical
– Operational
– Workforce
▪ Discuss proposed evaluation criteria
▪ Look ahead to CRG2
– Best practice pathways
– Clinical models
Outputs
▪ Agree detailed descriptions of clinical models
▪ Finalise Case for Change
▪ Agree long list of clinical models to analyse
▪ Review case for change
▪ Agree high level evaluation criteria
1. Intro and case for change3. Refining descriptions of clinical models
19th September 1st October 24th October
2. Developing service models
4. Detailed review of clinical models
20th November
▪ Detailed discussion of each clinical model
▪ Further shortlisting of potentially viable models for further work
▪ Articulation of key questions that need to be addressed in next phase of work
▪ Selection of clinical models for further work plus key questions to be addressed
PROGRAMME OVERVIEW & GOVERNANCE
4
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
▪ Further refinement of clinical models and key questions
Contents

5
Summary case for change for Scarborough
… which will result in decreased in-hospital activity…
▪ Currently over 50% of NHS funds available for the local population are spent in the acute sector▪ The clinical evidence base suggests that a greater focus on prevention of ill health and on caring for people with LTCs and frailty in the
community can potentially reduce the need for care within the acute hospital resulting in better health status and greater independence▪ Examples from elsewhere suggest that new models of out of hospital care could reduce the amount of acute activity by ~3.5% per year
… which is good for the local population, but will put further pressure on already fragile, low volume acute hospital services
▪ Scarborough hospital is recognised as a remote site, 42 miles away from the nearest hospital, challenging collaborative working▪ As a result of population size and demographics, acute hospital services in Scarborough have relatively low volumes and acuity, and a relatively
high number of patients who could be treated in a different environment– 51% of attendances at Scarborough A&E (including the UCC) were for minor problems– 73% of all bed days were occupied by patients over 65, compared with 60% nationally– Stranded non-elective patients accounted for 65% of all bed days
▪ Services which need to be provided 24x7 are particularly difficult with relatively small numbers of patients
– Obstetrics sees ~1,400 deliveries per year, the 7th the smallest consultant led obstetric unit nationally
– There were fewer than 3,000 admissions last year to Paediatrics; the national average approaches 5,000
– Only 70% of doctors in training report adequate experience at Scarborough; the national average is 90%▪ 24/7 services are more expensive to run in Scarborough: A&E, women’s services and children’s services costs are 124%, 120% and 128% of
indexed national average assessed costs respectively▪ Staffing of services providing 24x7 care is particularly difficult to provide
– 46% of posts in Emergency and Acute medicine are not filled with a substantive appointment– 26% of consultant workforce is over 55– Locum/agency/bank expenditure at Scarborough Hospital was £10.6 million in 2016/17
… requiring a different sort of care to that historically provided…
▪ Care for people with LTCs and frailty needs to be provided in a different way & in a different place than in the past▪ It will need a more pro-active approach, delivered by multi-disciplinary teams working together, with easier access to diagnostics and specialist
opinion and more consistent quality of care ▪ It will also require greater use of technology, e.g. virtual outpatient clinics or remote monitoring
The local population is ageing and has changing health needs…
▪ Life expectancy is in Scarborough is below the national average for men, driven by high rates of stroke and coronary heart disease▪ The local population (within the catchment) is growing by 0.2% per year but ageing, with the number of people over 70 projected to grow over
the next seven years▪ This will result in a higher prevalence of people with long term conditions (LTCs) and frailty▪ Scarborough has a large and seasonal non-resident population - there are 5 million nights a year spent in the Scarborough region by tourists▪ The underlying population is projected to grow by 2.2% by 2030, in the same period demographic-related activity growth in non-elective care is
projected to increase by 10.4%
The Trust therefore needs to change its model of care to continue providing high quality sustainable services
▪ Building on experiences of similar sized hospitals elsewhere, this is likely to involve:– New forms of collaboration with neighbouring hospitals, in particular York, while remaining cognizant of travel times between the two
sites– More integrated arrangements with local primary and community care services– New workforce models and potentially greater use of technology– Identifying opportunities to utilise the Bridlington site
CASE FOR CHANGE
FULL CASE FOR CHANGE IN ANNEX 2
6
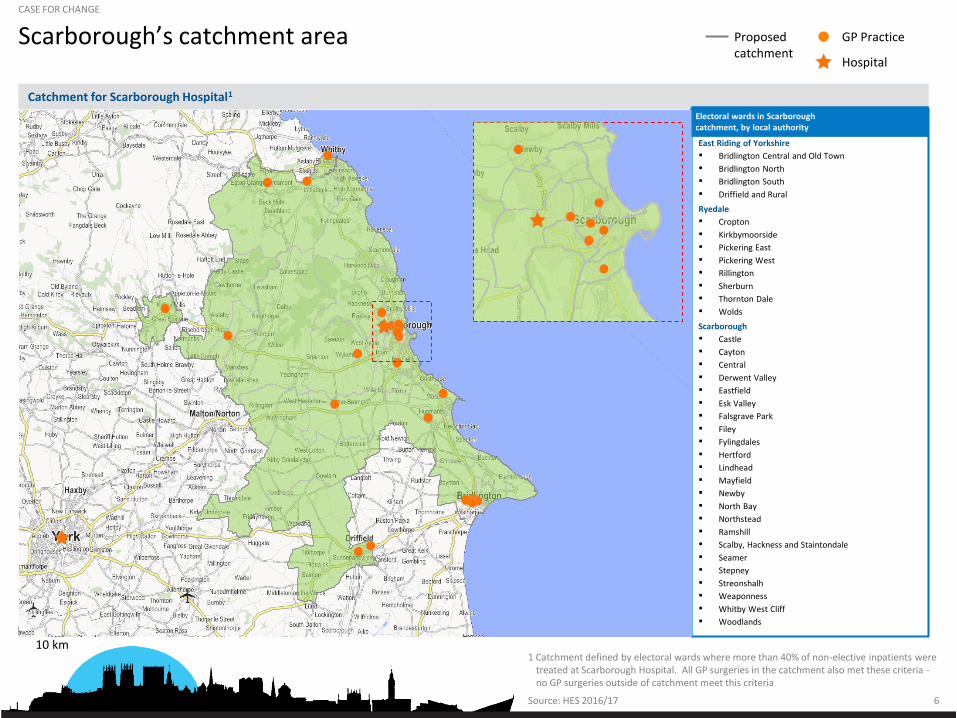
Scarborough’s catchment area
Source: HES 2016/17
10 km
Catchment for Scarborough Hospital1
East Riding of Yorkshire
▪ Bridlington Central and Old Town
▪ Bridlington North
▪ Bridlington South
▪ Driffield and Rural
Ryedale
▪ Cropton
▪ Kirkbymoorside
▪ Pickering East
▪ Pickering West
▪ Rillington
▪ Sherburn
▪ Thornton Dale
▪ Wolds
Scarborough
▪ Castle
▪ Cayton
▪ Central
▪ Derwent Valley
▪ Eastfield
▪ Esk Valley
▪ Falsgrave Park
▪ Filey
▪ Fylingdales
▪ Hertford
▪ Lindhead
▪ Mayfield
▪ Newby
▪ North Bay
▪ Northstead
▪ Ramshill
▪ Scalby, Hackness and Staintondale
▪ Seamer
▪ Stepney
▪ Streonshalh
▪ Weaponness
▪ Whitby West Cliff
▪ Woodlands
Proposed catchment
GP Practice
Hospital
1 Catchment defined by electoral wards where more than 40% of non-elective inpatients were treated at Scarborough Hospital. All GP surgeries in the catchment also met these criteria -no GP surgeries outside of catchment meet this criteria
Electoral wards in Scarborough catchment, by local authority
CASE FOR CHANGE

7Source: ONS 2016-based Sub National Population Projections
Population projection of catchment area
1 Catchment are defined as the following wards: Stepney; Central; Weaponness; Eastfield; Woodlands; North Bay; Newby; Filey; Falsgrave; Northstead; Cayton; Scalby; Hackness and Staintondale; Lindhead; Hertford; Castle, Derwent Valley; Ramshill; Bridlington South; Bridlington North; Seamer; Bridlington Central and Old Town; Thornton Dale; Sherburn; Fylingdales; Pickering East; Streonshalh; Whitby West Cliff; Pickering West; Rillington; Mayfield; Wolds; Cropton; Driffield and Rural; Kirkbymoorside; Esk Valley accessed online in September 2018 [http://www.localhealth.org.uk]
CASE FOR CHANGE
35 36
53 49
53 54
34 39
17832
2018 2025
70-89
90+
50-69
20-49
<20
181+0.2% p.a.
2.0%
0.1%
-1.0%
0.1%
2.2%
2018-25 CAGR, % Population projection by age, area in scope1, ‘000s
2.4
2.3
0.7
-0.2
0.6
All EnglandScarborough
8
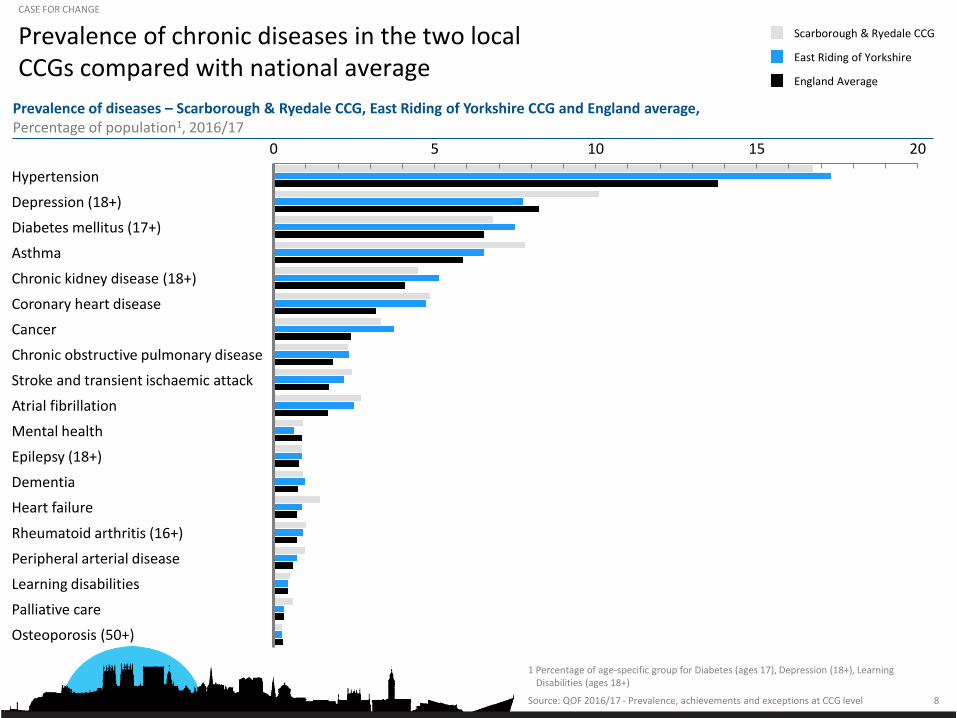
Prevalence of chronic diseases in the two local CCGs compared with national average
1 Percentage of age-specific group for Diabetes (ages 17), Depression (18+), Learning Disabilities (ages 18+)
20100 155
Depression (18+)
Hypertension
Chronic kidney disease (18+)
Mental health
Diabetes mellitus (17+)
Asthma
Coronary heart disease
Cancer
Heart failure
Chronic obstructive pulmonary disease
Stroke and transient ischaemic attack
Atrial fibrillation
Epilepsy (18+)
Dementia
Rheumatoid arthritis (16+)
Peripheral arterial disease
Learning disabilities
Palliative care
Osteoporosis (50+)
Scarborough & Ryedale CCG
East Riding of Yorkshire
England Average
Source: QOF 2016/17 - Prevalence, achievements and exceptions at CCG level
Prevalence of diseases – Scarborough & Ryedale CCG, East Riding of Yorkshire CCG and England average,Percentage of population1, 2016/17
CASE FOR CHANGE

9
Emergency hospital admissions
Source: PHE local health tool, accessed online in August 2018 [http://www.localhealth.org.uk]
CASE FOR CHANGE
Hospital admissions, all causes Standardised admissions rate in catchment relative to national average indexed to 100
100
89
104
National average Scarboroughcatchmentemergencyadmissions
Scarboroughcatchmentelectiveadmissions

10SOURCE: Performance and Information Team, York Teaching Hospital NHS Foundation
Trust
Scarborough General Hospital by treatment specialityCASE FOR CHANGE
# of admissions
Inpatient Hospital Admissions per year by treating specialty
# with a procedure carried outTreatment Specialty
Surgical
Medical
Obstetrics/gynae
Paediatrics(0 – 18y.o.)
3,187
2,829
2,670
2,460
2,223
1,230
799
415
198
4,101
3,053
2,930
2,121
1,913
1,548
1,209
548
444
309
205
139
3,222
1,379
784
2,038
1,101
168
General Surgery
Ophthalmology
Colorectal Surgery
Well Babies
Urology
Upper Gastrointestinal Surgery
Trauma & Orthopaedics
Respiratory Medicine
Accident & Emergency
Hepatobiliary & Pancreatic Surgery
Other
Obstetrics
Cardiology
Medical Oncology
Gastroenterology
Geriatric Medicine
Gynaecology
Endocrinology
Clinical Haematology
Nephrology
General Medicine
Rheumatology
Diabetic Medicine
Other
Midwife Episode
Paediatrics
Neonatology
2,905
2,829
2,513
2,460
1,227
1,053
569
415
181
1,420
1,633
2,838
1,102
908
797
1,194
359
373
303
22
113
1,295
696
281
163
78
6

11
Maternity and paediatric attendances compared with local peers and those serving similar populations
SOURCE: HES 2016/17
Average
1 Excluding sites with <100 births per year. Defined by relevant HRG codes for births 2 Emergency admissions for infants and children under 19
CASE FOR CHANGE
10
0
2
8
4
6
3.2
0
5
10
15
30
4.7
James Cook
Scarborough
Hull
York
Hereford County
Pilgrim
West Cumberland
Hereford West Cumberland
YorkScarborough
Hull
JamesCook
Pilgrim
Emergency pediatric spells2
Maternity deliveries1
Activity level by site across England 16/17, ‘000s

12
Patients attending Scarborough A&E who live outside of local area by month
8.2 7.7
9.2 9.6
13.8
9.2
6.8
4.5 4.6
2.93.7
5.0
NovApr2017
May JulJun Aug OctSep Mar2018
Dec Jan Feb
Percentage of patients attending Scarborough A&E who live outside of local area1
% of all A&E attendances (Apr 2017-Mar 2018)
SOURCE: Performance and Information team, York Teaching Hospitals NHS Foundation Trust
1 Local area defined as the following CCGS: East Riding of Yorkshire, Harrogate and rural district CCG, Hambleton Richmondshire and Whitby CCG, Scarborough & Ryedale CCG, Vale of York CCG, Wakefield CCG
CASE FOR CHANGE

13
A&E attendances to Scarborough A&E by severity
50
1,152
1,495
8,235
1,820
930
4,834
8,220
8,464
19,725
VB07Z - Cat 2 Ix with Cat 2 Rx
VB01Z - Cat 5 Rx
VB05Z - Cat 2 Ix with Cat 3 Rx
VB04Z - Cat 2 Ix with Cat 4 Rx
VB02Z - Cat 3 Ix with Cat 4 Rx
VB03Z - Cat 3 Ix with Cat 1-3 Rx
VB06Z - Cat 1 Ix with Cat 3-4 Rx
VB10Z – Emergency dental
VB08Z - Cat 2 Ix with Cat 1 Rx
VB09Z - Cat 1 Ix with Cat 1-2 Rx
VB11Z - No sig Ix or Rx
1
All attendances1
A&E attendances (‘000), 2016/17
54,928Total2
Major
Normal
Minor
20%
29%
51%
CASE FOR CHANGE
1 Includes Type 1 (regular ED) and Type 3 (GP led UCC) attendances 2 VB99Z excluded (Dead on arrival- 2 patients both attending Type 1 A&E)
SOURCE: Performance & Information Team, York Teaching Hospital NHS Foundation Trust
50
1,152
1,491
8,234
1,820
903
4,793
7,790
4,359
1,300
1
Attendances to Type 1 A&E only
34%
48%
18%
31,895

14
Attendances at all A&E types for local CCGs compared with peers
SOURCE: HES 2016/17 M13 A&E, c/o NHS Digital
1 Peer group defined as the 10 CCGs most similar to Scarborough and Ryedale by NHS Right Care (Hastings and Rother, Great Yarmouth and Waveney, West Norfolk, South Kent Coast, Isle of Wight, Lincolnshire East, Hereford, Airedale, Wharfedale and Craven, Lincolnshire West, and Harrogate and Rural District)
CASE FOR CHANGE
527.3376.4 325.1 266.4
360.0 296.5
133.7160.8 170.1 158.2 174.8 156.4
392.7
204.2151.7 107.2
172.8 121.9
A&E attendances at all A&E Types per 1,000 weighted population
Total A&E attendances
Minor A&E attendances
Major/ normal A&E attendances
East Riding of Yorkshire CCG
Peer group average
Peer group top quartile
England average
Scarborough & Ryedale CCG
England top quartile
CCG performanceabove England average
CCG performance at, orbelow, England average

15
Attendances to type 1 A&Es for local CCGs compared with peers
SOURCE: HES 2016/17 M13 A&E, C/o NHS Digital
1 Peer group defined as the 10 CCGs most similar to Scarborough and Ryedale by NHS Right Care (Hastings and Rother, Great Yarmouth and Waveney, West Norfolk, South Kent Coast, Isle of Wight, Lincolnshire East, Hereford, Airedale, Wharfedale and Craven, Lincolnshire West and Harrogate and Rural District)
CASE FOR CHANGE
289.7182.0
252.7 237.7 276.6 234.1
132.2 117.2158.0 149.6 162.7 144.0
157.5
64.8 93.3 84.2 113.3 83.5
A&E attendances at all A&E Types per 1,000 weighted population
Total A&E attendances
Minor A&E attendances
Major/ normal A&E attendances
East Riding of Yorkshire CCG
Peer group average
Peer group top quartile
England average
Scarborough & Ryedale CCG
England top quartile
CCG performanceabove England average
CCG performance at, orbelow, England average
16
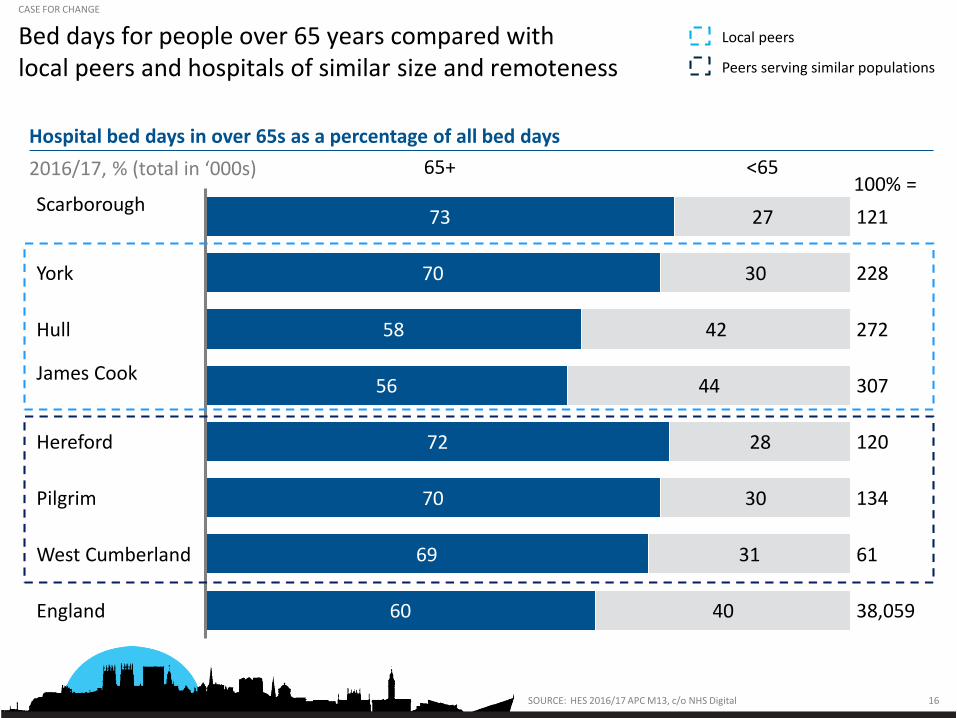
Bed days for people over 65 years compared with local peers and hospitals of similar size and remoteness
Hospital bed days in over 65s as a percentage of all bed days
SOURCE: HES 2016/17 APC M13, c/o NHS Digital
73
70
58
56
72
70
69
60
27
30
42
44
28
30
31
40
121
Hull
Scarborough
West Cumberland
100% =
York
England
James Cook
Pilgrim
Hereford
<6565+
228
272
307
120
134
61
38,059
Local peers
Peers serving similar populations
CASE FOR CHANGE
2016/17, % (total in ‘000s)

17
65% of bed days at Scarborough hospital are occupied by stranded patients with length of stay 8 days or longer (majority aged over 65)
1 Excluding RA (regular attenders) and Other (not recorded type), Paediatrics patients are defined by age 0 – 18 years old; 2 Figures calculated assuming that all patients in this category currently stay for 31 days, will go down to trust average LOS for NEL patients, and each reduction of a 20 bed unit saves a hospital £2 million
SOURCE: HES 2016/17
8%
10
Other non-elective
32%
4%
Maternity
17%
18%
2%
3
Non-elective aged 65+
0
Elective
9%
Paeds
2%
1%
6%
2%
131 1
100%= (in ‘000s) = 46,000
bed days
8-30 days
Patients with LOS of 0-7 days and days 0-7 of patients with LOS >7 days
31+ days2016/17 bed days by LOS band and POD1
Total bed days and % of POD
CASE FOR CHANGE

18
18 week RTT performance for local CCGs
95
85
93
83
82
88
84
97
86
89
87
90
91
92
96
94
Q2Q4 Q3
2013-2014, Q1 Q3Q2 Q3 Q4
2014-2015, Q1
2015-2016, Q1Q2 Q3 Q4
2016-2017, Q1
92
Q2
East Riding of Yorkshire CCG National top quartileScarborough & Ryedale CCG National average
SOURCE: HSJ Intelligence 2018
CASE FOR CHANGE
RTT performance against 18 week target, %

19
Costs related to smallness and remoteness
Peer group2National average
Scarborough
100110
120
Total service costs1 as percentage of national average (adjusted for MFF2) FY14/15%
1 Includes costs for Critical Care, Outpatients, Elective IP, Non-elective IP, Daycase and A&E 2 MFF is market forces factor 3 Peer group considered: St Mary's Isle of Wight. West Cumberland, Cumberland Infirmary, North Devon NHS Trust
SOURCE: York Teaching Hospital NHS Trust Analysis, Benchmarking unavoidable smallness - Benchmarking and review of costs at Scarborough and Bridlington sites' 2016
100111
124
National average
Peer group2 Scarborough
A&E assessed costs as percentage of national average (adjusted for MFF), FY14/15%
100
125 120
National average
Peer group3 Scarborough2
Maternity services costs as percentage of national average (adjusted for MFF), FY14/15%
100
126 128
National average
Peer group3 Scarborough2
Children’s services costs as percentage of national average (adjusted for MFF), FY2014/15%
CASE FOR CHANGE

20
Locum spend at Scarborough and York
2%(0.2)
34%(3.1)
39%(4.2)
33%(3.5)
2%(0.2)
11%(1.2)
15%(1.6)
Scarborough1
15%(1.4)
44%(4.0)
6%(0.5)
York
Consultant
Medical staff grade
Medical trainee
Nursing
Other
Expenditure on locum or agency staff by group, FY2017/18% (£ million)
1 Includes locum/agency spend at Bridlington
SOURCE: Expenditure team, York Teaching Hospitals NHS Foundation Trust
10.7 9.7Total locum spend(£million)
CASE FOR CHANGE

21
Agency, bank and locum spend
7%(0.2)
Q4
70%(2.4)
4%(0.1)
10%(0.3)
6%(0.2) 21%
(0.8)23%(0.8)
Q2 Q1 2018/19
29%(1.1)
16%(0.6)
73%(2.6)
4%(0.2)
Q3
78%(2.5)
18%(0.6)
62%(2.2)
4%(0.1)
Q4
75%(2.2)
22%(0.6)
27%(1.0)
68%(2.0)
3%(0.1)
11%(0.4)
Q1 2016/17
74%(2.3)
6%(0.2)
22%(0.7)
6%(0.2)
4%(0.1)
Q2
20%(0.7)
7%(0.2)
Q3
79%(2.8)
78%(2.7)
25%(0.9)
Q1 2017/18
73%(2.8)
Q2
22%(0.7)
10%(0.3)
73%(2.6) 62%
(2.3)
10%(0.4)
Q4
Average quarterly
spend £3.4 million
Q1 2015/16
84%(2.7)
16%(0.5)
Q3
LocumAgency Bank
3.5 3.3 3.5 3.2 2.9 3.1 3.5 3.6 3.5 3.9 3.0 3.7 3.6
xx Total spend£million
Agency, bank and locum spend at Scarborough Hospital 2015/16-2018/19
% (£ million)
SOURCE: Finance team, York Teaching Hospital NHS Foundation Trust
Total spend=
CASE FOR CHANGE

22
Consultant vacancies at Scarborough Hospital
83%(15)
Ort
ho
pae
dic
s
Spec
ialis
t m
edic
ine
67%(4)
Paed
iatr
ics
17%(3)
100%(8)
6
29%(4)
Wo
men
’s
98%(8)
100%(3)
Eme
rgen
cy &
Acu
te m
edic
ine
An
aest
het
ics
& C
riti
cal c
are
69%(9)
77%(5)
23%(1)
18
Eld
erly
med
icin
e
71%(9)
31%(4)
Gen
era
l su
rger
y&
Uro
logy
33%(2)
Rad
iolo
gy
58%(9)
42%(7)
Gen
eral
m
edic
ine
54%(4)
46%(3)
50%%(2)
50%(2)
413
Op
thal
mo
logy
Budgeted FTE=
8 3 8 6 12 16 7
Filled posts Vacant postsCurrent consultant establishment in ScarboroughPercentage of vacant and filled FTEs as at end of July 2018
SOURCE: Human Resources Team, York Teaching Hospitals NHS Foundation Trust; discussion between HR team and directorate managers
% (No. of FTEs)
CASE FOR CHANGE

23
Vacancies for non-consultant grade doctors at Scarborough Hospital
113%(14)
Wo
men
’s h
ealt
h
-13%(-2)
90%(11)
5%(1)
95%(19)
Paed
iatr
ics
97%(2)
Rad
iolo
gy
100%(1)
3%(0)
Spec
ialis
t M
edic
ine
Gen
eral
Su
rger
y &
Uro
logy
92%(11)
8%(1)
Ort
ho
pae
dic
s68%(10)
32%(5)
Eld
erly
Med
icin
e
Eme
rgen
cy &
A
cute
Med
icin
e
62%(30)
38%(19)
Gen
eral
Med
icin
e
60%(3)
40%(2)
49
Op
thal
mo
logy
60%(9)
40%(6)
An
aest
het
ics
& C
riti
cal C
are
35%(4)
65%(7)
Budgeted FTE= 10%
(1)
2 20 12 12
12
10155 115
Filled posts Vacant posts
SOURCE: Human Resources Team, York Teaching Hospitals NHS Foundation Trust
1 Includes Doctors in Training and Non-consultant Grade Doctors
Current non-consultant establishment1 in ScarboroughPercentage of vacant and filled FTEs as at end of July 2018
% (Number of FTEs)
CASE FOR CHANGE

24
Percentage of consultants at Scarborough Hospital who are 55 or more years old
50%(2)
All
con
sult
ant
po
sts
8
50%(2)
Ort
ho
pae
dic
s
Gen
eral
su
rger
y&
Uro
logy
74%(54)
26%(19)
An
aest
het
ics
&C
riti
cal
care
100%(2)
Op
hth
alm
olo
gy
Rad
iolo
gy
8
Eme
rgen
cy &
A
cute
med
icin
e
50%(2)
50%(2)
66%(6)
34%(3)
30%(3)
Gen
eral
med
icin
e
70%(7)
75%(6)
9
25%(2)
2
80%(6)
20%(2)
Wo
men
’s
83%(3)
17%(1)
Eld
erly
med
icin
e
86%(13)
14%(2)
87%(7)
4
13%(1)
Paed
iatr
ics
4
100%(2)
73
Spec
ialis
tm
edic
ine
Budgeted FTE = 4 10 8 15 2
Less than 55 55 or more
SOURCE: Human Resources Team, York Teaching Hospitals NHS Trust
Percentage of current workforce aged 55 years or overConsultants as at end of June 2018
% (Number of FTEs)
CASE FOR CHANGE

25
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
▪ Further refinement of clinical models and key questions
Contents

26
Evaluation criteria: overview EVALUATION CRITERIA
Focus of the evaluation by the clinical reference group
Defined asEvaluation criteria
1.1 Clinical effectiveness
1.2 Patient and carer experience
1.3 Safety
Quality of Care1
2.1 Impact on patient choice
2.2 Distance, cost and time to access services
2.3 Service operating hours
2.4 Ability for clinicians to access specialist input
Access to care2
3.1 Scale of impact
3.2 Impact on recruitment, retention, skills
3.3 Sustainability
Workforce3
4.1 Forecast income and expenditure at system and organisation level
4.2 Capital cost to the system
4.3 Transition costs required
4.4 Net present value (30 years)
Value for money4
5.1 Expected time to deliver
5.2 Co-dependencies with other strategies/strategic fit
Deliverability5

27
Proposed sub-criteria: Quality of care
Questions to test
Clinical effectiveness
▪ Does this model enable the population of Scarborough and surrounding areas to receive acute services in line with national standards and other recognised best practices?
▪ Will this model allow sufficient volumes of cases to sustain quality?
▪ Will this model result in more effective prevention in order to improve life expectancy in the system and reduce health inequalities?
▪ Will this model account for future changes in the population size and demographics?
▪ Will this model lead to more people being treated by teams with the right skills and experience?
Patient and carer experience
▪ Will this model improve continuity of care for patients? (e.g., reduce number of hand offs across teams / organisations, increase frequency of single clinician / team being responsibility for a patient)?
▪ Will this model enable greater opportunity to link with voluntary / community sector health and wellbeing services?
▪ Will this model improve quality of environment in which care is provided?
▪ Will this model allow for patient transfers/emergency intervention within a clinically safe time-frame? Will travel time impact on patient outcome?
▪ Will this model offer reduced levels of risk (e.g., staffed 24/7 rotas, provide networked care, implement standardisation)?
Patient safety
Evaluation criteria
1EVALUATION CRITERIA

28
Proposed sub-criteria: Access to care
Impact on patient choice
▪ Will this model increase or decrease choice for patients?
▪ Will this model make it easier for people to understand which services they can access when and where?
Distance, cost and time to access services
▪ Will this model increase/reduce travel time and/or cost for patients to access specific services?
▪ Will this model involve patients travelling more/less frequently, change the number of journeys to access urgent medical intervention?
▪ Will this model reduce/increase patients' waiting time to access services?
▪ Will this model increase/reduce travel time and/or cost for carers and family?
▪ Will this model support the use of new technology to improve access?
▪ Will this model improve operating hours in line with demands of the population?
▪ Will this model reduce the risk of unplanned changes and improve service resilience?Service operating hours
Questions to test
▪ Will this model increase or decrease the time to access specialist input?Ability for clinicians to access specialist input
Evaluation criteria
EVALUATION CRITERIA
2

29
Proposed sub-criteria: Workforce
Scale of impact▪ What proportion of current staff will be impacted by the changes across the
system?
Impact on recruitment, retention, skills
▪ Will this model improve the recruitment and retention of permanent staff with the right skills, values and competencies?
▪ Is the staff travel, relocation or retraining required for this option acceptable?
▪ Is it possible to develop the skills base required in an acceptable time frame?
▪ Will this model enable accountability and governance structures to support staff?
▪ Will this model increase multi-disciplinary / cross-organisational working?
▪ Is this model likely to improve or maintain job satisfaction?
Questions to test
Sustainability
▪ Will this model enable staff to maintain or enhance competencies? (e.g., impact on volumes of activity / specialism; increased training / opportunity for accreditation and career progression)
▪ Will this model optimise the use of clinical staff and enable them to work at the “top of their license” versus being spread thinly?
Evaluation criteria
EVALUATION CRITERIA
3
30
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
▪ Further refinement of clinical models and key questions
Contents

31
The CRG has developed and refined best practice pathways in four areas
▪ Elective care pathway2
▪ Maternity and paediatric pathway3
▪ Urgent and emergency care pathway
1
▪ People with long term conditions (LTCs) and frailty
4
BEST PRACTICE CARE PATHWAYS

32
▪ Patients can access information rapidly to guide them to the appropriate level of care based on the severity of their illness
▪ Interaction with overlapping pathways (e.g. frailty and mental health) to guide patients to most appropriate care
▪ Patients have easy access (local, short travel, easy parking, etc.); Wait times are reasonable and communicated accurately
▪ Should be able to have easy access in extended hours
▪ Investigation given right away at point of contact or same day, as close to 1st contact as possible (e.g. one-stop ambulatory care if possible)
▪ Real-time tests are used to help inform decision
▪ Minimum amount of investigations at appropriate time required to provide an accurate diagnosis
▪ Onsite or remote support, including reporting as required
▪ Consistent investigations with same standards in all locations
▪ Focus on completing diagnosis to rule out major illness/injury vs minor problems
▪ Clear and easy route to escalation if indicated by investigation or examination
▪ Timely, appropriate care▪ Good communication that gives
patient understanding of the problem, including potential complications
▪ Patient is discharged as quickly as possible
▪ Patients given good advice and simple explanations of next steps for recovery
▪ Any follow-up is as convenient as possible for the patient (e.g., virtual/remote, local)
▪ If complications arise, patients have clear pathway and can follow it easily and quickly
Minor illness (e.g., urinary symp-toms)
▪ Timely, appropriate care in a single encounter
▪ Good communication that gives patient understanding of the problem, including potential complications
▪ Patient is discharged as quickly as possible
▪ Patients given understanding of follow-up required (best case: no follow-up)
▪ Follow-up (when required) is easy to schedule and conveniently located for patient
▪ If complications arise, patients have clear pathway and can follow it easily and quickly
▪ Patients can publicly access information rapidly to guide them to the appropriate level of care based on the severity of their injury (e.g. 111, pharmacies)
▪ Patients are able to access a convenient location nearby where they can be seen relatively quickly / are clearly communicated as to what the timing will be
▪ Low level diagnostics (incl. X-rays) as required - only relevant tests completed
▪ Simple, quick, focused investigation, where the results are explained quickly and easily understandable
▪ Onsite or remote support, including reporting as required
▪ Clear and easy route to escalate into major injury category if indicated by investigation or examination
Minor Injuries (e.g., laceration requiring stitches)
Triage and first contact with healthcare professional
Investigations Treatment Follow-up
BEST PRACTICE CARE PATHWAYS
Urgent and emergency care pathway: ‘minor’ patients REVISED PATHWAY1

33
Urgent and emergency care pathway: ‘major’ patients
▪ Patient has immediate access to assessment at correct place of treatment, the appropriate clinician (e.g. correct skills) is available to provide an accurate diagnosis
▪ Assessment by (consultant) within 12 hours
▪ Explanations are simple, advice is clear, next steps are described, easy access for patients to ask questions
▪ Sufficient diagnostic facilities to allow initial triage for >90% of patients to correct transfer location
▪ Full range of assessments available as required, quickly
▪ Rapid access to specialist opinion within appropriate timescale
▪ On site 24/7 care available▪ Care given in one place, as quickly
as necessary▪ Care provided by specialist where
appropriate▪ All types of assessments required
given (e.g., scans, blood, etc.), as regularly as required
▪ Access to ICU if required▪ Access to medical or surgical
opinion and surgery if necessary
▪ Discharged as soon as possible▪ Follow up is provided to patients
with part of their care team or another specialist, as conveniently as possible for the patient
▪ Re-entry into appropriate pathways supported should issues arise
Standard/major Illness (e.g., chest pain and fever)
First contact with healthcare professional
Investigations Treatment Follow-up
Moderate trauma (e.g. #NOF)
▪ On site 24/7 care available▪ Treatment in line with national
standards e.g. for #NOF▪ Clinicians with relevant training
available▪ Enhanced recovery + rehab (e.g.
PT / OT) given as required▪ Discharged as quickly as possible▪ Clear and speedy escalation
pathway if necessary
▪ Follow-up with member of patient treatment team as local as possible
▪ Patients able to recover as close to home as possible / at home if possible
▪ Re-entry into appropriate pathways supported should issues arise
▪ Patient seen in appropriate centreas local as possible
▪ Support from relevant specialty available within acceptable timeframe at the location or remotely where appropriate
▪ Support services available as required
▪ Additional assessments given as required (X rays, CT, etc.)
▪ Diagnosis made quickly on one site or remotely and communicated clearly, with treatment options provided / explained
▪ Patient is taken to agreed major trauma centre to ensure quality of care
▪ Support available immediately at the location
▪ Treatment ideally given at only one place
▪ Full range of complex support services available as required
▪ Additional assessments given as required (X rays, CT, etc.)
▪ Diagnosis made quickly on one site and communicated clearly, with treatment options provided / explained
▪ Specialists available within appropriate timeframe
▪ On site 24/7 care available▪ Clinicians with adequate relevant
training in issue available▪ Enhanced recovery and access to
other specialists given as required▪ Access to ICU if required▪ Discharged as quickly as possible
▪ Follow up available with member of patient treatment team as local as possible
▪ Patients able to recover as close to home as possible / at home if possible
▪ Re-entry into appropriate pathways supported should issues arise
Major complex condition or Trauma (e.g., major RTA)
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY1

34
Urgent and emergency care pathway: clinical standards and best practice evidence
First contact with healthcare professional Investigations Treatment Follow-up
‘Minor’ patients
▪ Integrated primary care to reduce avoidable emergency admissions (GMS Contract, 2014/15)
▪ Every emergency department should have a co-located primary care out-of-hours facility (Acute and emergency care: prescribing the remedy, 2014)
▪ Treatment at scene (or transfer to primary/community care) where appropriate (Transforming NHS Ambulance Services, NAO, 2011)
▪ Each emergency department and acute admissions unit has an IT infrastructure that effectively integrates clinical and safeguarding information across all parts of the urgent and emergency care system (Seven Day Clinical Standards, NHS England, 2014)
▪ Community and social care must be coordinated effectively and delivered 7 days a week to support urgent and emergency care services (Acute and emergency care: prescribing the remedy, 2014)
▪ All hospitals admitting medical and surgical emergencies should have access to all key diagnostic services (e.g., diagnostic imaging, interventional radiology, interventional endoscopy, bronchoscopy, pathology) in a timely manner 24 hours a day, 7 days a week, to support decision making (The Royal College of Emergency Medicine, Emergency Department Capacity Management Guidance, 2015)
▪ Critical Care Unit should have dedicated medical cover present in the facility 24 hours per day, 7 days per week (NHS Services, Seven Days a week, 2013)
▪ Radiological services, including ultrasound and CT scanning, should be available 7-days per week to aid sepsis diagnosis and potentially drain infected collections. If applicable, source control (percutaneous drainage/surgery) should be undertaken as soon as practically possible and within 12 hours. (Guidelines for Provision of Intensive Care Services, 2016)
▪ Triage, treatment and discharge or admission within 4 hours (national standard)
▪ Senior decision-makers at the front door of the hospital, and in surgical, medical or paediatric assessment units, should be normal practice, not the exception (CEM, Workforce Recommendations, 2010; and The Way Ahead 2008-2012, 2008)
▪ Any surgery conducted at night should meet NCEPOD requirements and be under the direct supervision of a consultant surgeon (NHS London, Adult emergency services: Acute medicine and emergency general surgery commissioning standards, 2011)
▪ Provide consultant-delivered emergency general surgery in each trust (GIRFT general surgery report, 2017)
▪ Acute medicine inpatients should be reviewed daily be a relevant consultant (Transforming urgent and emergency care services in England, 2015)
▪ There must be rapid 24/7 availability of a doctor with advanced airway and resuscitation skills (Guidelines for Provision of Intensive Care Services, 2016)
▪ Admission to Intensive Care must occur within 4 hours of making the decision to admit (Guidelines for Provision of Intensive Care Services, 2016)
▪ Units must not utilise greater than 20% of registered nurses from bank/agency on any one shift when they are NOT their own staff. (Guidelines for Provision of Intensive Care Services, 2016)
▪ When on-take for emergency / acute medicine and surgery, a consultant and their team are to be completely freed from any other clinical duties / elective commitments that would prevent them from being immediately available (Transforming urgent and emergency care services, 2015)
▪ All emergency admissions to be seen and assessed by a relevant consultant within 12 hours of the decision to admit or within 14 hours of the time of arrival at the hospital ( Transforming urgent and emergency care services in England, 2015)
▪ Prompt screening of all complex needs inpatients should take place by a multi-professional team which has access to pharmacy, psychiatric liaison services and therapy services (including physiotherapy and occupational therapy, 7 days a week with an overnight rota for respiratory physiotherapy) (NHS England , Commissioning Standards Integrated Urgent care, 2015)
▪ Where available resources mandate a combined rota with ICM and non-ICM consultant staff, to ensure the provision of an appropriate adult critical care service, there should be:
– Dedicated daytime consultant ICM cover 7 days per week
– Availability of advice from intensivists where needed
(Interim guidance on governance for smaller remote and smaller rural Intensive Care units, ICS, 2018)
Standard/ major Illness (e.g., chest pain and fever)
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY1

35
Elective care pathway: low complexity
▪ Initial investigations done at point of first contact or as quickly as possible / close to patient as possible
▪ All investigations required are provided quickly and closely (e.g., pathology / imaging/endoscopy)
▪ Early communication of results & immediate referral of urgent problems (as per protocol)
▪ One clinical information system for use
▪ Day surgery when possible
▪ No cancellations
▪ All appropriate equipment available for the procedure
▪ All pre-op assessment standardised, carried out at initial decision to treat and carried out locally
▪ Seamless package of care
▪ Procedures to be provided locally
▪ Surgeons and teams are provided adequate volumes & avoid duplication of services
▪ Appropriate level of in hours cover
▪ High calibre out of hours cover
▪ Services ensure quality patient experience & satisfaction
▪ Continued provision of an appropriate training environment
▪ Early decision confirming patient suitable for local treatment
▪ Robust rescue plan and escalation policy for the deteriorating patient including access to HDU or ICU either locally or within network
▪ Delivery of upper quartile outcomes standardised mortality
▪ Openness and clear communication to patient on what is being provided
▪ One clinical information system
▪ Clear patient ownership during inpatient stay
▪ Full use of processes to enable early discharge
▪ All to be provided locally including out of hospital
▪ Clear protocols for post operative management
▪ Follow ups minimised and only as required
▪ High-quality electronic discharge summary
▪ Access is standardised across populations, with minimal delays and referrals prioritised based on patient problems. Patients are triaged as required depending on urgency of condition
▪ No patient is not provided access
▪ Clear to patients who they should be seeing and why (e.g., referral from GP)
▪ Wait times are in line with or better than national targets including for 2 week rule referrals and patients suspected of cancer
▪ Openness and clear communication to patient on what is being provided
▪ High-quality advice and guidance provided to inform patients of choice and next steps
▪ Technology leveraged to facilitate process (e.g., electronic communication) with rapid communication back to referrer
▪ One clinical information system for use
▪ Care is provided across specialties as much as possible with provision of elective outpatient care aligned with need for specialist presence in acute hospital to cover urgent and emergency care
▪ Care completed as locally as possible
▪ Access is standardised across populations
▪ Wait times are less than 7 days
▪ Local referral protocols standardised & followed
▪ Consistent, standardised advice and guidance process (on things like local policy) using up-to-date technology to ensure one seamless pathway
▪ One clinical information system for use
▪ Clear communication to patient on what is being provided
▪ Direct access to intervention through multiple providers (e.g., physio)
▪ Direct access to investigation
Primary careFirst acute contact with healthcare professional
Investigations Interventions Follow-up
Majority of planned care occurs in primary care
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY2

36
Elective care pathway: high complexity
▪ As in Low Complexity
▪ Interventional treatment done locally when possible but may need to be referred to specialist centrefor low volume complex procedures in high risk patients
▪ As in Low Complexity
▪ All preop assessment standardised, carried out at initial decision to treat and carried out locally wherever possible
▪ Early decision confirming if patient suitable for local treatment or if patient unsuitable for local treatment and has to be transferred to another centre
▪ As many procedures as possible to be provided locally
▪ Surgeons and teams are provided adequate volumes
▪ Robust out of hours cover aligned with the complexity of the procedure and the comorbidities of the patient
▪ Robust rescue plan and escalation policy for the deteriorating patient including access to HDU or ICU either locally or within network
▪ Seamless package of care irrespective of location of that care
▪ Minimum length of stay if patient transferred to another centre for treatment with consideration of transfer back to local centrefor post operative care if appropriate
▪ Full use of processes to enable early discharge both locally and when care provided in other centres
▪ As much as possible to be provided locally irrespective of location of surgery
▪ Clear protocols for post operative management
▪ Follow ups minimised and only as required
▪ High quality electronic discharge summary with clear guidelines for the management of complications
▪ Access is standardised across populations, with minimal delays and referrals prioritised based on patient problems. Patients are triaged as required depending on urgency of condition
▪ No patient is not provided access
▪ Clear to patients who they should be seeing and why (e.g., referral from GP)
▪ Wait times are in line with or better than national targets including for 2 week rule referrals and patients suspected of cancer
▪ Openness and clear communication to patient on what is being provided
▪ High quality advice and guidance provided to inform patients of choice and next steps
▪ Technology leveraged to facilitate process (e.g., electronic communication) with rapid communication back to referrer
▪ One clinical information system for use
▪ Care is provided across specialties as much as possible with provision of elective outpatient care aligned with need for specialist presence in acute hospital to cover urgent and emergency care
▪ Care completed as locally as possible
▪ Access is standardised across populations
▪ Wait times are less than 7 days
▪ Local referral protocols standardised & followed
▪ Consistent, standardised advice and guidance process (on things like local policy) using up to date technology to ensure one seamless pathway
▪ One clinical information system for use
▪ Clear communication to patient on what is being provided
▪ Direct access to intervention through multiple providers (e.g., physio)
▪ Direct access to investigation
Majority of planned care occurs in primary care
Primary careFirst acute contact with healthcare professional
Investigations Interventions Follow-up
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY2

37
Elective care pathway: clinical standards and best practice evidence
▪ Require reversible risk factors to be addressed prior to non-urgent procedures, using a patient-centredapproach utilizing shared decision-making (GIRFT general surgery report, 2017)
▪ Patients should be admitted in ring-fenced beds, on the day of surgery where possible (RCSI Model of Care for Elective Surgery, 2013)
▪ Enhanced recovery and discharge planning should begin at the outset of the patient’s elective surgical journey (RCSI Model of Care for Elective Surgery, 2013)
▪ Ensure that every patient is reviewed by a consultant surgeon, seven days a week (RCS Good surgical practice 2014
▪ When complexity is an issue as appropriate, patients should be transferred to another unit where resources and skills are available (RCS Good surgical practice, 2018)
▪ Ensure that diagnostic and therapeutic interventions can be undertaken in the right setting including one-stop outpatient facilities to minimise disruption to patients whilst enabling effective use of resources (RCS Outpatients clinics: a guide to good practice, 2017)
▪ Community rehabilitation services should be adequately resourced to provide early, intense and frequent rehabilitation to all hip fracture patients (British Orthopaedic Association, A national review of adult elective orthopaedic services in England, 2015)
▪ Radiology, laboratory and other tests are performed as expeditiously as possible, necessitating a minimum number of hospital visits for the patient. Hospital outpatient clinics should be coordinated where possible (RCSI Model of Care for Elective Surgery, 2013)
▪ Ensure all units are operating within a hub and spoke network model, as defined by the national service specification, emulating the most advanced hub and spoke models that exist currently. This in turn should deliver improved early decision-making capability and access to diagnostics, allowing early treatment, prioritised by degree of urgency (GIRFT Vascular Surgery report, 2018)
Primary careFirst acute contact with healthcare professional
Investigations Admission for surgery Follow-up
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY2

38
Paediatrics: best practice care for acutely unwell child
▪ Easy access to information to support parental decision making – on phone/online/ applications
▪ Parental education through health visitors and other parental groups
▪ Parents have easy access (local, short travel, easy parking, etc.); Wait times are reasonable and communicated accurately
▪ Should be able to have easy access –same day and extended hours
▪ Standardised screening tests and protocol
▪ Parent able to obtain same day appointment in out of hospital setting
▪ Suitably qualified staff e.g. GP/nurse with experience in paediatrics
▪ Access to paediatric expertise in person (e.g. MDT or specialist clinics in primary care) or over the phone/online (e.g. specialist number, via e-referral system) to allow speedy and appropriate escalation
▪ Treatment as per protocols
▪ Shared records with parents and inpatient/referral unit
Unwell child
Immediate assessment and treatment
Treatment Follow-up TreatmentTriage and first contact Follow-up
▪ Direct referral to hospital as per standardisedprotocols
▪ Paediatric expertise (nurse, consultants, middle grade, ANP) available on site during opening hours
▪ If <1 year, child should be seen by consultant paediatrician
▪ Safeguarding expertise available if required
If admitting:▪ Direct transport to IP
unit, with barrier free transfer
▪ Quick referral systems, uninterrupted, no ability to refuse or delay a referral
▪ Shared staffing with ED
▪ Shared records through online secure system
If observing:▪ Assessment unit
should have a minimum of 2 registered children’s nurses at all times
▪ Wards should have extended opening hours
If discharging: ▪ Follow up phone call
next day for those discharged from SSAU
▪ Shortest stay possible in IP unit
▪ Early discharge with monitoring in community
▪ 7 day community services to enable early discharge
▪ 1:4 nursing ▪ Consultant presence
24x7 (10 WTE paediatric consultants)
▪ Follow up done in community with access to specialists in clinic next day as required (SSPAU or community access)
▪ Consultant to follow up if needed or community nurses or GP to be done in home, hospital, or GP practice
▪ Assessment unit (SSPAU) has ambulatory care and follow ups
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY3

39
Paediatrics: clinical standards and best practice evidence for care of the acutely unwell child
Unwell child: Clinical standards and best practice evidence
Immediate assessment and treatment Treatment Follow-up TreatmentTriage and first contact
▪ Whole pathway commissioning for children’s services that includes ED attendance or hospital admission avoidance by easy availability of GP urgent appointments and consultant led provision of rapid access paediatric clinics (Joint Statement by RCGP, RCN, RCPCH and CEM on the urgent & emergency care of children and young people, 2011)
▪ Hours of operation for Short Stay Paediatric Assessment Units (SSPAU) should match times of population demand (RCPCH, Standards for SSPAU, 2017)
▪ Alternatives to full hospital admission by provision of SSPAUs (with the same role as Clinical Decision Units for adults) run in partnership with Emergency Departments, as well as early discharge enablement by community nursing and SSPAUs (Joint Statement by RCGP, RCN, RCPCH and CEM on the urgent & emergency care of children and young people, 2011)
▪ Every child or young person on the SSPAU with an acute medical problem is seen by appropriate tier-two specialist within 4 hours and consultant* within 14 hours (RCPCH, Standards for SSPAU, 2017)
▪ Contracted staffing levels and competencies for children trained clinicians (including safeguarding) must reflect the standards set by RCPCH, RCN, CEM
▪ Health professionals should have access to the child’s shared record (RCPCH, Standards for SSPAU, 2017)
▪ Effective safeguarding systems are child centred (Working Together to Safeguard Children, 2013)
▪ Evidence-based guidelines are used for the management of conditions with which infants, children and young people may be admitted to the SSPAU (RCPCH, Standards for SSPAU 2017)
▪ A consultant paediatrician* is readily available on the hospital site at times of peak activity of the SSPAU and is able to attend at all times within 30 minutes. Throughout all the hours they are open, SSPAUs have access to the opinion of a consultant paediatrician* via telephone (RCPCH, Standards for SSPAU 2017)
▪ All paediatric inpatient units adopt an “attending consultant” system
▪ All general acute paediatric consultant rotas are made up of ≥10 EWTD-compliant WTEs
▪ There should be a minimum of two registered children’s nurses at all times in all inpatient and day care areas
▪ Specialist paediatricians are available for immediate telephone advice for acute problems for all specialties and paediatricians (RCPCH Facing the Future, 2015)
▪ Before they are discharged, every child referred for a paediatric opinion is seen by, or has their case discussed with: a consultant paediatrician, a middle grade paediatrician, or an advanced children’s nurse practitioner (RCPCH Standards for Paediatric Services, 2015)
▪ Children and young people and their parents and carers are provided, at the time of their discharge, with both verbal and written discharge and safety netting information, in a form that is accessible and that they understand (RCPCH, Standards for SSPAU, 2017)
* Or equivalent
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY3

40
Maternity pathway: best practice summary
Pre-conception(in community)
Antenatal care BirthPost-natal & neonatal care
▪ Implement integrated programme of women’s health (including smoking cessation), sex education and contraception through primary care, community and schools (supported by council)
▪ Provide pre-conception advice and counselling for prospective parents on complicating factors in pregnancy
▪ Primary care ensures at risk women (social and clinical) are offered pre pregnancy advice e.g. for women with epilepsy or diabetes
▪ Booking referral by midwife by 10 weeks (National guidance)
▪ Rigorous ongoing risk assessment– Stratify patients by risk– Midwifery groups
responsibility for identifying high risk women and targeting services at them
▪ Adopt NICE guidance– 7-10 antenatal
appointments– 2 ultrasounds in low risk
pregnancy– Include all national
screening programmes in routine care
▪ Adopt midwife led care model (case loading), with direct access to midwives; access to OUs as needed
▪ Concentrate services in easy-access local community centresto facilitate registry and productivity
▪ Leverage IT-enabled solutions to increase sharing of records and improve productivity in community-based care
▪ Use MSWs to improve midwife productivity
▪ Ensure choice of location for birth, based on risk profile:– Provide high quality information e.g. risk profile of different units– Default option midwife led– Ensure clear transfer protocols for rapid transfer
▪ Ensure appropriate site staffing based on risk:– Low risk: Midwives– Medium/High risk: Midwifery, obstetric & medical consultants,
anaesthetics, ICU, neonatal ICU– Supra-specialist: Level 3 critical care, maternal and neonatal ICU
care, anaesthetics, surgery, ICU, neonatal ICU– 60-98 hrs per week of consultant presence on labour ward rising
to 168hrs in future▪ Interdependencies include:– Medium risk: anaesthesia (1 duty, 1 available on call); NICU level 1
(could be level 2 depending on the number of deliveries), blood transfusion on-site, HDU
– High risk: Complex ultrasound, endocrinology, surgery, interventional radiology, critical care, 24/7 anaesthesia, NICU level 2, blood transfusion services
– Supra-specialist: Complex surgery, medical specialists, interventional radiology, critical care, 24/7 anaesthesia, NICU level 3
▪ Ensure clear transfer protocols for rapid transfer▪ Continuity of carer throughout antenatal, birth and post natal but esp.
1:1 care during established labour through increased midwife productivity (Better Births – National Maternity Review)
▪ Provide high quality, safe maternity services– Increase percentage of normal births in low risk settings– Provide formal clinical networks– Handle complexity through specialisation
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY3
▪ Provide high-quality, routine post-natal care focused on people who need it based on social risk and clinical need– Contact with Health
Visitor within 10-14 days post-birth
– Health visitors targeted at most needy families; consider appointments in local community centres/GP practices instead of home
▪ Leverage IT-enabled solutions to increase sharing of records and improve productivity in community-based care – also using MSWs
▪ Midwife and Health visitor (post 10 days) proactively support breastfeeding to increase initiation/rates at 3/6 months
▪ Provide accessible, targeted specialist post-natal care if needed
▪ Dedicated neonatal care –separate rota from paeds
▪ Implement level 1/2/3 neonatal care
41
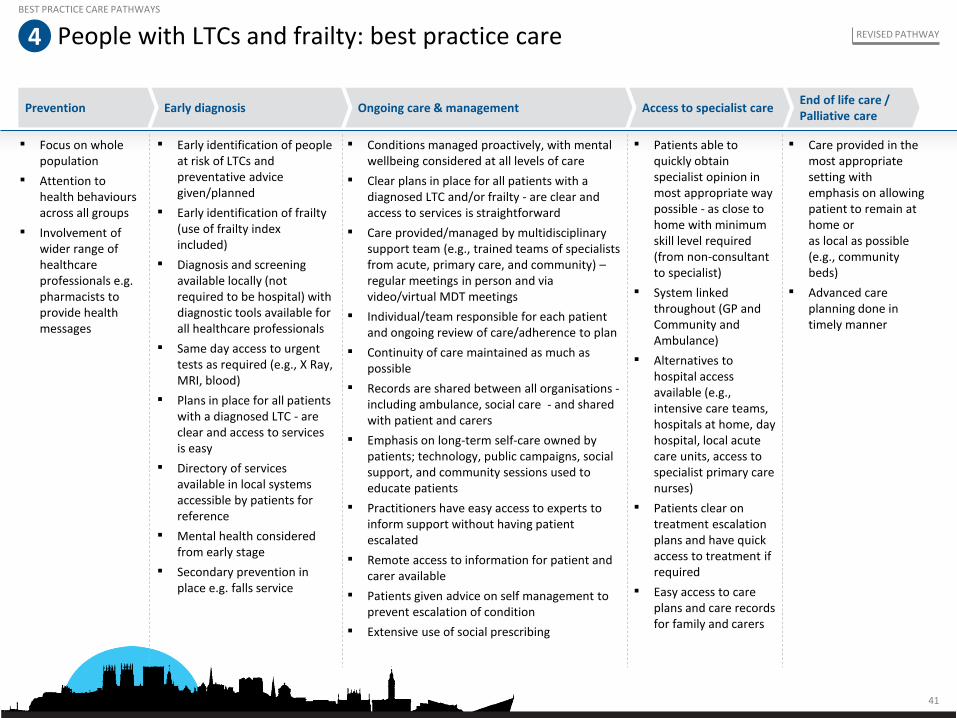
People with LTCs and frailty: best practice care
Prevention Early diagnosis Ongoing care & managementEnd of life care / Palliative care
Access to specialist care
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY4
▪ Focus on whole population
▪ Attention to health behaviours across all groups
▪ Involvement of wider range of healthcare professionals e.g. pharmacists to provide health messages
▪ Early identification of people at risk of LTCs and preventative advice given/planned
▪ Early identification of frailty (use of frailty index included)
▪ Diagnosis and screening available locally (not required to be hospital) with diagnostic tools available for all healthcare professionals
▪ Same day access to urgent tests as required (e.g., X Ray, MRI, blood)
▪ Plans in place for all patients with a diagnosed LTC - are clear and access to services is easy
▪ Directory of services available in local systems accessible by patients for reference
▪ Mental health considered from early stage
▪ Secondary prevention in place e.g. falls service
▪ Conditions managed proactively, with mental wellbeing considered at all levels of care
▪ Clear plans in place for all patients with a diagnosed LTC and/or frailty - are clear and access to services is straightforward
▪ Care provided/managed by multidisciplinary support team (e.g., trained teams of specialists from acute, primary care, and community) –regular meetings in person and via video/virtual MDT meetings
▪ Individual/team responsible for each patient and ongoing review of care/adherence to plan
▪ Continuity of care maintained as much as possible
▪ Records are shared between all organisations -including ambulance, social care - and shared with patient and carers
▪ Emphasis on long-term self-care owned by patients; technology, public campaigns, social support, and community sessions used to educate patients
▪ Practitioners have easy access to experts to inform support without having patient escalated
▪ Remote access to information for patient and carer available
▪ Patients given advice on self management to prevent escalation of condition
▪ Extensive use of social prescribing
▪ Patients able to quickly obtain specialist opinion in most appropriate way possible - as close to home with minimum skill level required (from non-consultant to specialist)
▪ System linked throughout (GP and Community and Ambulance)
▪ Alternatives to hospital access available (e.g., intensive care teams, hospitals at home, day hospital, local acute care units, access to specialist primary care nurses)
▪ Patients clear on treatment escalation plans and have quick access to treatment if required
▪ Easy access to care plans and care records for family and carers
▪ Care provided in the most appropriate setting with emphasis on allowing patient to remain at home or as local as possible (e.g., community beds)
▪ Advanced care planning done in timely manner

42
People with LTCs and frailty: clinical standards and best practice evidence
▪ All people over the age of 65 or with long term conditions will be risk stratified with appropriate pro-active care plans but in place for moderate and high risk individuals (GMS Contract, 2014)
▪ All people over the age of 75 and people with multiple long term conditions will have a named GP
▪ All moderate and high risk people will have a named care coordinator who will support them in self-care and ensure continuity of care through health services (GMS Contract, 2014
▪ All people with long term conditions will be offered information and support in self care (Integrated care and support: our shared commitment, Dept of Health 2013)
▪ In the event of a crisis, people will be appropriately triaged, and where suitable, be assisted by a multi-disciplinary rapid response team which will provide them with care in their home, and where appropriate, put in place short term home support to aid recovery at home as an alternative to hospital admission (Birmingham Community Healthcare NHS Trust, 7 Day Rapid Response Service Case Study, NHS Improvement 2011)
▪ People approaching the end of life receive consistent care that is coordinated effectively across all relevant settings and services at any time of day or night, and delivered by practitioners who are aware of the person's current medical condition, care plan and preferences (NICE guidance: End of life care for adults, 2017)
Early diagnosis Ongoing care & management Access to specialist care End of life care / Palliative care
BEST PRACTICE CARE PATHWAYS
REVISED PATHWAY4

44
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
– Shortlisting and initial combinations
– Detailed descriptions of clinical models
– Activity shift assumptions
▪ Further refinement of clinical models and key questions
Contents

45
Conceptual approach: the filtering process has narrowed down the longlist of potential models to a shortlist plus the status quo
Conceptual approach to clinical model development
Consider interdependencies to develop specialty combinations
Narrow clinical models based on high level criteria and keeping meaningfully different models only
Describe final models shortlist for full quality of care assessment
Long list of all combinations of clinical models for key service areas
Models viable from a clinical interdependency perspective, excluding current state
Models to be modelled
Identify possible range of service line models for key service areas:
▪ A&E
▪ Acute medicine
▪ Emergency surgery
▪ Critical care
▪ Elective surgery
▪ Maternity
▪ Paediatrics
1 2 3 4
Description
1 A representative sample of potential models for each clinical service lines were described, taking into account population needs
2 Combined into whole hospital clinical models taking into account interdependencies
3 Shortlist narrowed by keeping only meaningfully distinct models.▪ 6 distinct models for urgent
and emergency care are described
▪ The model for elective surgery was informed by the model of urgent and emergency care
▪ Models for paeds/maternity were informed by interdependencies with the model of urgent and emergency care
4 Eight models described following refinement with CRG
CLINICAL MODELS

46
Practical approach: shortlist of whole-hospital models was built by considering interdependencies, viability1 and distinctness in four stages
Practical approach to clinical model development
Stage one:
Narrow down UEC2
models
Stage two:
Combine UEC models with elective care model options
Stage three:
Combine UEC & elective care models with paediatric & maternity models
Stage four:
Combine with frailty / elderly care models to get whole-hospital clinical models
1 Based on reference to the evaluation criteria2 UEC is urgent and emergency care and comprises A&E, acute medicine, emergency surgery,
and critical care
CLINICAL MODELS

47
Standardised care pathways
Common approaches (integration) across whole system
Easy access to senior decision makers – on site or remotely
Remote access to specialist opinion
Mental health crisis teams available, ideally in ED/UTC
Stabilisation and rapid transfer for patients needing escalation
Transfer back from specialist centres to local units
Greater use of hot clinics
Incentivisation of recruitment & retention by developing a USP
Enhanced use of IT/technology (e.g. telemedicine, virtual clinics)
Easy step-down or transfer to community / social settings
The importance of key enablers for all modelsCLINICAL MODELS

48
A range of clinical models exist for each serviceService offering Range of models explored
Frailty Frailty unit/hub included in all configurations
Emergency surgery
OOH gen. surgery registrar (with cons support from York)
Surgery hot clinics (SAU + recovery beds)
24 x 7 emergency general surgery
Ambulatory emergency surgery only
Critical care L2 critical care+/- eICU No enhanced careL3 critical care +/- eICUL1 care plus critical care service
Elective careModerate perioperative risk elective surgery
Day cases only High perioperative risk elective surgery
Low perioperative risk elective surgery
PaediatricsPaediatric assessment unit (all walk-ins & referrals) UTC onlyInpatient
MDT led care at Front door (no paediatrician)
MaternityLower risk obstetric service with limited neonates (L1)
On-call midwife-led unit
High risk obstetric service24/7 on-site midwife-led unit
Acute medicineSelective acute take with AAU
Step up/Step down beds24 x7acute medical take with AAU
Ambulatory Assessment unit (AAU) only – no beds
A&EFront door assessment A&E model UTC only24x 7 A&E
“Medical only” A&E + UTC
Service line models can be combined to form thousands of combinations of whole-hospital clinical models
CLINICAL MODELS

49
Combining all potential UEC models alone leads to 256 potential combinations
1 Critical care support could be provided for unstable patient by anaesthetics/critical care physicians with Critical Care Outreach Team
Does not account for service lines such as maternity and paediatrics which would result in thousands of combinations
Assuming no interdependencies
Acute medicine
Critical care
Emergen-cy surgery
Rationale
No. of models
256
64 64 64
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service1
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
Medical only A&E
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service1
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
Front door assessment A&E model
64
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service1
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
UTC only24/7 A&E
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service1
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
CLINICAL MODELS

50
Stage one: clinical interdependencies within urgent and emergency care exclude some clinical models
Key interdependenciesServices
Assumes diagnostic imaging and pathology services exist in all models
▪ 24/7 A&E requires a core level of anaesthetics / critical care and medical support
▪ Front door assessment A&E model requires at least on call gen surgery
▪ UTC only does not require emergency surgery or critical care
A&E
▪ Full (unselected) acute medicine take requires access to critical care and access to emergency surgery
Acute medicine
▪ Providing inpatient emergency surgery requires L3 critical care▪ Providing inpatient emergency surgery requires acute medicine
Emergencysurgery
Critical care▪ Would not provide critical care without acute medicine take
Major trauma▪ Scarborough may need to retain trauma unit status to satisfy trauma
network requirements, which may require 24/7 emergency surgery and a consultant surgeon within 30 mins1
1 Trauma unit status would not require inpatient paediatrics, but may require 24/7 emergency surgery. This is based on initial discussions and guidance from the National Clinical Director for Trauma. Formal, written guidance has been requested by the steering group regarding this point. In the meantime it is important from a process point of view that we continue to consider and lay out the trade-offs across a broad range of clinical model options
CLINICAL MODELS

51
Stage one: filtering for first round of UEC interdependencies leads to 28 models
1 Refers to configuration of Emergency general surgery - in all models with trauma and orthopaedic in-patient services, non-resident registrar and consultant cover is considered
2 Critical care support could be provided for unstable patient by anaesthetics/critical care physicians with Critical Care Outreach Team
3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
Assumes diagnostic imaging3 and pathology services exist in all models
Acute medicine
Critical care
Emergen-cy surgery1
No. of models
28
2 12 12
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service2
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
Medical only A&E
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service2
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
Front door assessment A&E model
2
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service2
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
UTC only24/7 A&E
2
3
2
3
1
4
2
3
1
4
4
1
Level 2 + HDU
Level 1 plus critical care service2
Selective take
AAU only
Level 3 +/- eICU
No enhanced care
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24/7 emergency gen. surgery
Hot clinics only
Step up/down beds
Full medical take
CLINICAL MODELS

52
Stage one: more detail on the 28 potential clinical models for urgent and emergency care
Assumes diagnostic imaging2 and pathology services exist in all models
Model 5 Model 6 Model 11 Model 12 Model 13Model 7 Model 8 Model 9 Model 10Model 1 Model 2 Model 3 Model 4
Level 2 Level 2 Level 2 Level 2 Level 2 Level 1 plus critical care service
Level 2 Level 1 plus critical care service
Level 1 plus critical care service
Level 1 plus critical care service
Level 3 Level 3 Level 3 Level 3
Model 14
A&EMedical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
24/7 A&E 24/7 A&E Front door ass’mentA&E model
Front door ass’mentA&E model
Emergency surgery1
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Surgical hot clinics
OOH reg on site (cons support at York)
Surgical hot clinics
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Surgical hot clinics
24x7 emergency gen. surgery
OOH reg on site (cons support at York)
24x7 emergency gen. surgery
OOH reg on site (cons support at York)
Acute medicine
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Model 19 Model 20 Model 25 Model 26 Model 27 Model 28Model 21 Model 22 Model 23 Model 24Model 15 Model 16 Model 17 Model 18
Emergencysurgery1
Surgical hot clinics
Surgical hot clinics
Ambula-tory emer-gencysurgery only
Ambulatory emergency surgery only
Surgical hot clinics
Surgical hot clinics
Ambulatory emergency surgery only
Ambulatory emergency surgery only
Surgical hot clinics
Surgical hot clinics
Ambulatory emergency surgery only
Surgical hot clinics
Ambulatory emergency surgery only
Ambulatory emergency surgery only
Acute medicine
Selective medical take + AAU
Selective medical take + AAU
Step up/down beds
Step up/down beds
Step up/down beds
Step up/down beds
AAU only AAU only AAU only AAU onlySelective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Critical care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
Level 1 plus critical care service
Level 1 plus critical care service
No enhanced care
A&EUTC only UTC only UTC only UTC only UTC only UTC onlyUTC only UTC only UTC only UTC onlyMedical
only A&EMedical only A&E
UTC only UTC only
Critical care
1 Refers to configuration of Emergency general surgery. In all models with trauma and orthopaedic in-patient services, non-resident registrar and consultant cover is considered
2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

53
Stage one: there are six meaningfully distinct UEC models were identified
1 1 Refers to configuration of Emergency general surgery. In all models with trauma and orthopaedic in-patient services, non-resident registrar and consultant cover is considered
2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS
Assumes diagnostic imaging2 and pathology services exist in all models
Model 5 Model 6 Model 11 Model 12 Model 13Model 7 Model 8 Model 9 Model 10Model 1 Model 2 Model 3 Model 4
Level 2 Level 2 Level 2 Level 2 Level 2 Level 1 plus critical care service
Level 2 Level 1 plus critical care service
Level 1 plus critical care service
Level 1 plus critical care service
Level 3 Level 3 Level 3 Level 3
Model 14
A&EMedical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
Medical only A&E
24/7 A&E 24/7 A&E Front door ass’mentA&E model
Front door ass’mentA&E model
Emergency surgery1
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Surgical hot clinics
OOH reg on site (cons support at York)
Surgical hot clinics
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Surgical hot clinics
24x7 emergency gen. surgery
OOH reg on site (cons support at York)
24x7 emergency gen. surgery
OOH reg on site (cons support at York)
Acute medicine
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Model 19 Model 20 Model 25 Model 26 Model 27 Model 28Model 21 Model 22 Model 23 Model 24Model 15 Model 16 Model 17 Model 18
Emergencysurgery1
Surgical hot clinics
Surgical hot clinics
Ambula-tory emer-gencysurgery only
Ambulatory emergency surgery only
Surgical hot clinics
Surgical hot clinics
Ambulatory emergency surgery only
Ambulatory emergency surgery only
Surgical hot clinics
Surgical hot clinics
Ambulatory emergency surgery only
Surgical hot clinics
Ambulatory emergency surgery only
Ambulatory emergency surgery only
Acute medicine
Selective medical take + AAU
Selective medical take + AAU
Step up/down beds
Step up/down beds
Step up/down beds
Step up/down beds
AAU only AAU only AAU only AAU onlySelective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Critical care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
No enhanced care
Level 1 plus critical care service
Level 1 plus critical care service
Level 1 plus critical care service
No enhanced care
A&EUTC only UTC only UTC only UTC only UTC only UTC onlyUTC only UTC only UTC only UTC onlyMedical
only A&EMedical only A&E
UTC only UTC only
Critical care

54
Stage two: interdependencies determine what type of elective care the UEC models can provide
Key interdependenciesMajor services
▪ Would not provide high perioperative risk1 elective surgery without at least L2 critical care
Elective surgery
Assumes diagnostic imaging1 and pathology services exist in all models
1 Perioperative risk takes into account the extent and complexity of the surgery as well as the pre-morbid state of the patient. The provision of critical care (to provide increased monitoring and therapies) and the availability of emergency surgery (to manage complications of elective surgery) will impact the elective procedures that can be performed
2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

55
Stage two: the UEC model determines the complexity of the elective care provided Highest level of elective surgery that can be provided
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
2 Perioperative risk takes into account the extent and complexity of the surgery as well as the pre-morbid state of the patient. The provision of critical care (to provide increased monitoring and therapies) and the availability of emergency surgery (to manage complications of elective surgery) will impact the elective procedures that can be performed
Model 28Model 1 Model 11 Model 17Model 4
Combined with one of elective care options available:
Model 15
Critical careNo enhanced careLevel 3 Level 2 Level 1 plus critical
care serviceLevel 3 Level 1 plus critical
care service
A&EUTC only24/7 A&E Medical only
A&EUTC onlyFront door
assessment A&E model
Medical only A&E
Emergency surgerySurgical hot clinics
24x7 emergency general surgery
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Acute medicineStep up/down beds
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Assumes diagnostic imaging1 and pathology services exist in all models
Cases with low peri-operative risk2
c
Cases with moderate peri-operative risk2
b
Cases with high peri-operative risk2
a
CLINICAL MODELS

56
Stage two: There are six UEC + elective care models
Model 28Model 1 Model 11 Model 17Model 4 Model 15
Critical care
No enhanced care
Level 3 Level 2 Level 1 plus critical care service
Level 3 Level 1 plus critical care service
A&E
UTC only24/7 A&E Medical only A&E
UTC onlyFront door assessment model
Medical only A&E
Emergency surgery
Surgical hot clinics
24x7 emergency general surgery
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
Acute medicine
Step up/down beds
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Elective surgery1
Cases with low peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate peri-operative risk
Cases with high peri-operative risk
Cases with moderate peri-operative risk
1 Perioperative risk takes into account the extent and complexity of the surgery as well as the pre-morbid state of the patient. The provision of critical care (to provide increased monitoring and therapies) and the availability of emergency surgery (to manage complications of elective surgery) will impact the elective procedures that can be performed
CLINICAL MODELS

57
Stage three: interdependencies between paediatrics and maternity exclude some clinical models
Key interdependenciesMajor services
▪ Would not provide service for patients with high risk of neonatal critical care without inpatient paediatrics
Neonates
▪ Would not provide higher risk obstetrics without level 3 adult critical care and inpatient paediatrics
Maternity
Assumes diagnostic imaging1 and pathology services exist in all models
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

58
Stage three: There are seven distinct models for paediatrics & maternity
Paediatrics
Maternity
Model B
Inpatient
Lower risk obstetric service with limited neonates
Model D
Paediatricassess-mentunit
24/7 midwife led unit
Model E
MDT led care (no paedsconsultant)
24/7 midwife led unit
Model F
UTC with no facility for children
24/7 midwife led unit
Model A
Inpatient
High risk obstetric service
Model G
UTC with no facility for children
Pop-up midwife led unit
Model C
Paediatricassess-mentunit
Lower risk obstetric service with limited neonates
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
▪ These seven paediatric + maternity models are combined with the six UEC & elective care models (from first and second round) to form distinct and viable combinations
▪ Assumes diagnostic imaging1 and pathology services exist in all models
CLINICAL MODELS

59
Stage three: There are eight distinct models which combine UEC + elective with paediatrics + maternity
Model 28FModel 1C Model 11C Model 17DModel 4B Model 4C Model 15C
Assumes diagnostic imaging2 and pathology services exist in all models
Model 1A
PaediatricsMDT led carePaeds
assessment unit
Paeds assessment unit
Paeds assessment unit
Inpatient paediatrics
Paeds assessment unit
Paeds assessment unit
Inpatient paediatrics
MaternityMidwife led unit
Lower risk consultant led obstetrics
Midwife led unit
Midwife led unit
Lower risk consultant led obstetrics
Lower risk consultant led obstetrics
Midwife led unit
High risk obstetrics
Critical careNo enhanced care
Level 3 Level 2 Level 1 plus critical care service
Level 3 Level 3 Level 1 plus critical care service
Level 3
A&EUTC only24/7 A&E Medical only
A&EUTC onlyFront door
assessment model
Front door assessment model
Medical only A&E
24/7 A&E
Emergency surgery
Surgical hot clinics
24x7 emergency general surgery
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24x7 emergency general surgery
Acute medicine
Step up/down beds
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Elective surgery
Cases with low peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with low peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk1
1 Perioperative risk takes into account the extent and complexity of the surgery as well as the pre-morbid state of the patient
2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

60
Stage four: Combining clinical models with frailty / elderly care options
Key interdependencies and logic criteriaMajor services
▪ Frailty unit / service to be included in all configurationsFrailty / elderly care
Assumes diagnostic imaging1 and pathology services exist in all models
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

61
Stage four: initial shortlist of models circulated to CRG
Model 28FModel 1C Model 11C Model 17DModel 4B Model 4C Model 15CModel 1A
Paediatrics
MDT led carePaeds assessment unit
Paeds assessment unit
Paeds assessment unit
Inpatient paediatrics
Paeds assessment unit
Paeds assessment unit
Inpatient paediatrics
Maternity
Midwife led unit
Lower risk consultant led obstetrics
Midwife led unit
Midwife led unit
Lower risk consultant led obstetrics
Lower risk consultant led obstetrics
Midwife led unit
High risk obstetrics
Critical care
No enhanced care
Level 3 Level 2 Level 1 plus critical care service
Level 3 Level 3 Level 1 plus critical care service
Level 3
A&EUTC only24/7 A&E Medical only
A&EUTC onlyFront door
assessment A&E model
Front door assessment A&E model
Medical only A&E
24/7 A&E
Emergency surgery
Surgical hot clinics
24x7 emergency general surgery
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
OOH reg on site (cons support at York)
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24x7 emergency general surgery
Acute medicine
Step up/down beds
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Elective surgery
Cases with low peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
▪ Frailty unit / service included in all configurations▪ Assumes diagnostic imaging1 and pathology services exist in all models
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
CLINICAL MODELS

62
The shortlisted models were revised based on feedback from the CRG, including removing the description of a low risk obstetrics unit
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
2 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
CLINICAL MODELS
Model 17DModel 1C Model 4C Model 15DModel 3C Model 4A Model 11DModel 1A
Paediatrics
Paeds assessment unit
Paeds assessment unit
Paeds assessment unit
Paeds assessment unit
Paeds assessment unit
Inpatient paediatrics
Paeds assessment uni2
Inpatient paediatrics
Maternity
Midwife led unit2
Consultant led obstetrics
Consultant led obstetrics
Midwife led unit2
Consultant led obstetrics
Consultant led obstetrics
Midwife led unit2
Consultant led obstetrics
Critical care
Level 1 plus critical care service
Level 3 Level 3 Level 1 plus critical care service
Level 3 Level 3 Level 2Level 3
A&EMedical only A&E
24x7 A&E Front door assessment A&E model
UTC onlyFront door assessment A&E model
Front door assessment A&E model
Medical only A&E
24x7 A&E
Emergency surgery
Ambulatory emergency surgery only
24x7 emergency general surgery
OOH reg on site (cons support at York)
Ambulatory emergency surgery only
24x7 emergency general surgery
OOH reg on site (cons support at York)
OOH reg on site (cons support at York)
24x7 emergency general surgery
Acute medicine
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Elective surgery
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
▪ Frailty unit / service included in all configurations▪ Assumes diagnostic imaging1 and pathology services exist in all models

63
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
– Shortlisting and initial combinations
– Detailed descriptions of clinical models
– Activity shift assumptions
▪ Further refinement of clinical models and key questions
Contents

64
Potential acute service models for Scarborough Hospital
Enablers common to all models
Developing a USP to support recruitment
Enhanced use of IT and technology
Easy (stabilise) & transfer of pts as req.
Clinical pathways featuring in all models
Diagnostic imaging & pathology services
1A
24 x 7 medical take + AAU
24 x 7 emergency general surgery
24 x 7 A&E + UTC
Level 3 critical care
High peri-operative risk elective surgery
Inpatient paediatrics
Consultant led obstetrics
1C
24 x 7 medical take + AAU
24 x 7 emergency general surgery
24 x 7 A&E + UTC
Level 3 critical care
High peri-operative risk elective surgery
Paediatric assessment unit
Consultant led obstetrics
3C
24 x 7 medical take + AAU
24 x 7 emergency general surgery
Front door assessment A&E + UTC
Level 3 critical care
High peri-operative risk elective surgery
Paediatric assessment unit
Consultant led obstetrics
4A
24 x 7 medical take + AAU
OOH gen. surg. reg on site
Front door assessment A&E + UTC
Level 3 critical care
High peri-operative risk elective surgery
Inpatient paediatrics
Consultant led obstetrics
4C
24 x 7 medical take + AAU
OOH gen. surg. reg on site
Front door assessment A&E + UTC
Level 3 critical care
High peri-operative risk elective surgery
Paediatric assessment unit
Consultant led obstetrics
11D
Selective medical take +AAU
OOH gen. surg. reg on site
Medical only A&E + UTC
Level 2 critical care
High peri-operative risk elective surgery
Paediatric assessment unit
Midwife led unit1
15D
Selective medical take +AAU
Ambulatory emergency surgery
Medical only A&E + UTC
Level 1 plus critical care
Moderate peri-op risk elective surgery
Paediatric assessment unit
Midwife led unit1
17D
Selective medical take +AAU
Ambulatory emergency surgery
UTC only
Level 1 plus critical care
Moderate peri-op risk elective surgery
Paediatric assessment unit
Midwife led unit
Standardised care pathways
Common approaches across system
Frailty unit & hub
Easy access to senior decision maker
Remote access to specialist opinion
Mental health crisis teams
Greater use of hot clinics
1 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
DETAILED MODEL DESCRIPTIONS

65
Model 1A – 24 x 7 A&E + UTC, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, inpatient paeds, cons. led obs
1 NB – direct referrals from community GPs to AAU and Surgical assessment not included2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
Discharge
Admit
Discharge
Stabilise & transfer totertiary centres
Level 3Critical care
AMB
Ward
Discharge
Assessment
Consultant led obstetrics
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Accident & Emergency24x7
Full medical take & Medical Assessment Unit (MAU)
Surgical Assessment Unit (SAU)
Inpatient paediatrics
Non-urgent care
Stabilise & transfer
DischargeFrailty Assessment
Non-major cases
Frailty Unit/Service2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit MAU/SAU
ENP or GP
ANP GP
Initial care
Discharge
DETAILED MODEL DESCRIPTIONS
Discharge
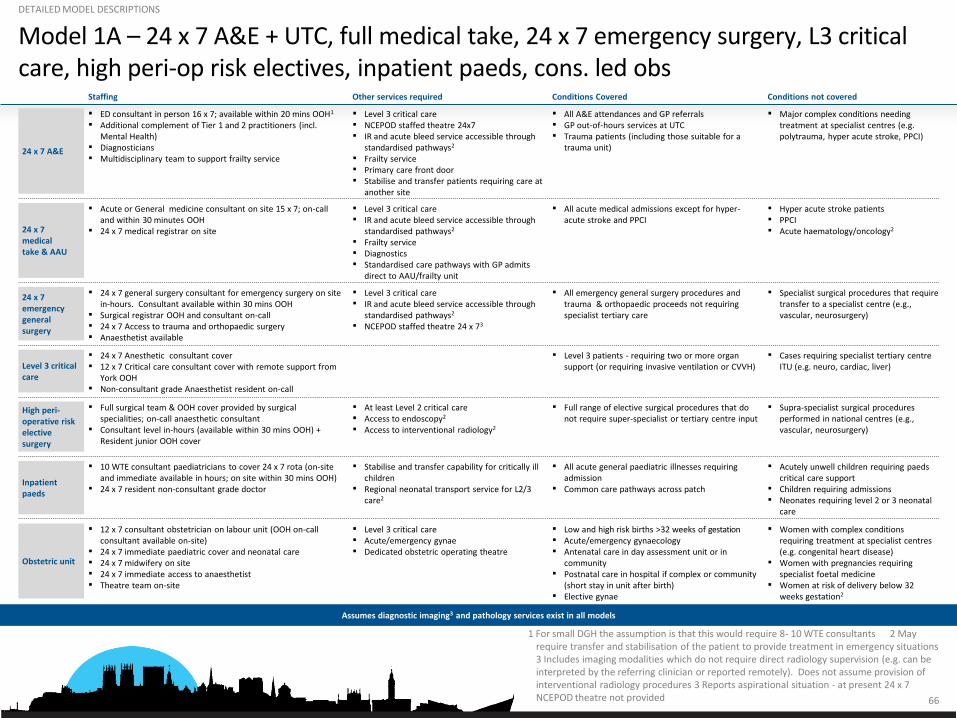
66
Model 1A – 24 x 7 A&E + UTC, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, inpatient paeds, cons. led obs
1 For small DGH the assumption is that this would require 8- 10 WTE consultants 2 May require transfer and stabilisation of the patient to provide treatment in emergency situations 3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 3 Reports aspirational situation - at present 24 x 7 NCEPOD theatre not provided
Conditions Covered Conditions not coveredOther services requiredStaffing
24 x 7 medical take & AAU
▪ All acute medical admissions except for hyper-acute stroke and PPCI
▪ Hyper acute stroke patients▪ PPCI▪ Acute haematology/oncology2
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ Frailty service▪ Diagnostics ▪ Standardised care pathways with GP admits
direct to AAU/frailty unit
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site
24 x 7 emergency general surgery
▪ All emergency general surgery procedures and trauma & orthopaedic proceeds not requiring specialist tertiary care
▪ Specialist surgical procedures that require transfer to a specialist centre (e.g., vascular, neurosurgery)
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ NCEPOD staffed theatre 24 x 73
▪ 24 x 7 general surgery consultant for emergency surgery on site in-hours. Consultant available within 30 mins OOH
▪ Surgical registrar OOH and consultant on-call▪ 24 x 7 Access to trauma and orthopaedic surgery▪ Anaesthetist available
High peri-operative risk elective surgery
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Supra-specialist surgical procedures performed in national centres (e.g., vascular, neurosurgery)
▪ At least Level 2 critical care▪ Access to endoscopy2
▪ Access to interventional radiology2
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours (available within 30 mins OOH) + Resident junior OOH cover
Obstetric unit
▪ Low and high risk births >32 weeks of gestation▪ Acute/emergency gynaecology▪ Antenatal care in day assessment unit or in
community▪ Postnatal care in hospital if complex or community
(short stay in unit after birth)▪ Elective gynae
▪ Women with complex conditions requiring treatment at specialist centres (e.g. congenital heart disease)
▪ Women with pregnancies requiring specialist foetal medicine
▪ Women at risk of delivery below 32 weeks gestation2
▪ Level 3 critical care▪ Acute/emergency gynae▪ Dedicated obstetric operating theatre
▪ 12 x 7 consultant obstetrician on labour unit (OOH on-call consultant available on-site)
▪ 24 x 7 immediate paediatric cover and neonatal care▪ 24 x 7 midwifery on site▪ 24 x 7 immediate access to anaesthetist▪ Theatre team on-site
Level 3 critical care
▪ Level 3 patients - requiring two or more organ support (or requiring invasive ventilation or CVVH)
▪ Cases requiring specialist tertiary centre ITU (e.g. neuro, cardiac, liver)
▪ 24 x 7 Anesthetic consultant cover▪ 12 x 7 Critical care consultant cover with remote support from
York OOH▪ Non-consultant grade Anaesthetist resident on-call
Inpatient paeds
▪ All acute general paediatric illnesses requiring admission
▪ Common care pathways across patch
▪ Acutely unwell children requiring paedscritical care support
▪ Children requiring admissions▪ Neonates requiring level 2 or 3 neonatal
care
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service for L2/3 care2
▪ 10 WTE consultant paediatricians to cover 24 x 7 rota (on-site and immediate available in hours; on site within 30 mins OOH)
▪ 24 x 7 resident non-consultant grade doctor
24 x 7 A&E
▪ All A&E attendances and GP referrals▪ GP out-of-hours services at UTC▪ Trauma patients (including those suitable for a
trauma unit)
▪ Major complex conditions needing treatment at specialist centres (e.g. polytrauma, hyper acute stroke, PPCI)
▪ Level 3 critical care▪ NCEPOD staffed theatre 24x7▪ IR and acute bleed service accessible through
standardised pathways2
▪ Frailty service▪ Primary care front door ▪ Stabilise and transfer patients requiring care at
another site
▪ ED consultant in person 16 x 7; available within 20 mins OOH1
▪ Additional complement of Tier 1 and 2 practitioners (incl. Mental Health)
▪ Diagnosticians▪ Multidisciplinary team to support frailty service
Assumes diagnostic imaging3 and pathology services exist in all models
DETAILED MODEL DESCRIPTIONS

67
Model 1C – 24 x 7 A&E + UTC, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, SSPAU, lower risk obs
1 NB – direct referrals from community GPs to AAU and Surgical assessment not included2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
Discharge
Admit
Discharge
Stabilise & transfer toother centres
Level 3Critical care
AMB
Ward
Discharge
Assessment
Lower risk obstetrics
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Accident & Emergency24x7
Full medical take & Medical Assessment Unit (MAU)
Surgical Assessment Unit (SAU)
Short Stay PaediatricUnit (SSPAU)
Non-urgent care
Discharge
Stabilise & transfer
DischargeFrailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit MAU/SAU
ENP or GP
ANP GP
Initial care
Discharge
DETAILED MODEL DESCRIPTIONS

68
Model 1C – 24 x 7 A&E + UTC, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, SSPAU, lower risk obs
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH)
2 For small DGH the assumption is that this would require 8- 10 WTE consultants 3 May require transfer of the patient to provide treatment 4 Includes imaging modalities
which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 5 Reports aspirational situation - at present 24 x 7 NCEPOD theatre not provided
DETAILED MODEL DESCRIPTIONS
Conditions Covered Conditions not coveredOther services requiredStaffing
Assumes diagnostic imaging4 and pathology services exist in all models
▪ All A&E attendances and GP referrals▪ GP out-of-hours services at UTC▪ Trauma patients (including those suitable for a trauma
unit)
▪ Major complex conditions needing treatment at specialist centres (e.g. polytrauma, hyper acute stroke, PPCI)
▪ Level 3 critical care▪ NCEPOD staffed theatre 24x7▪ IR and acute bleed service accessible through
standardised pathways3
▪ Frailty service▪ Primary care front door ▪ Stabilise and transfer patients requiring care at
another site
▪ ED consultant in person 16 x 7; available within 20 mins OOH1
▪ Additional complement of Tier 1 and 2 practitioners (incl. Mental Health)
▪ Diagnosticians▪ Multidisciplinary team to support frailty service
24 x 7 A&E
▪ Lower risk births >36 weeks of gestation▪ Acute/ Emergency gynaecology▪ Antenatal care in day assessment unit or in community▪ Postnatal care in hospital if complex or community
(short stay in unit after birth)
▪ Women with complex conditions requiring treatment at specialist centres (e.g. Congenital heart disease)
▪ Women with pregnancies requiring specialist foetal medicine
▪ Women at risk of delivery below 36 weeks gestation
▪ Level 3 critical care▪ Acute/emergency gynae▪ Dedicated obstetric operating theatre
▪ 12 x 7 consultant obstetrician on labour unit (OOH on-call obstetrician available within 30 minutes)
▪ 24 x 7 on-site non-consultant grade obstetrician▪ 24 x 7 immediate access to advanced neonatal resuscitation (e.g.
ANNP, Middle-grade or Reg Neonates)▪ 24 x 7 midwifery on site▪ 24 x 7 immediate access to anaesthetist
Obstetric unit
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient admissions▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Consultant paediatrician on site 15 x 7▪ Shared staff with A&E with paediatric expert / ANP / SpR covering
OOH▪ Facilities for children available 7 days through SSPAU and ED/UTC
SSPAU1 + ambulatory care
▪ All acute medical admissions except for hyper-acute stroke and PPCI
▪ Hyper-acute stroke patients▪ PPCI▪ Acute haematology/oncology2
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways3
▪ Frailty service▪ Diagnostics ▪ Standardised care pathways with GP admits direct
to AAU/frailty unit
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site24 x 7 medical take & AAU
▪ All emergency general surgery procedures and trauma & orthopaedic proceeds not requiring specialist tertiary care
▪ Specialist surgical procedures that require transfer to a specialist centre (e.g., vascular, neurosurgery)
▪ Children likely to require surgery
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ NCEPOD staffed theatre 24 x 75
▪ 24 x 7 general surgery consultant for emergency surgery on site in-hours. Consultant available within 30 mins OOH
▪ Surgical registrar OOH and consultant on-call▪ 24 x 7 Access to trauma and orthopaedic surgery▪ Anaesthetist available
24 x 7 emergency general surgery
▪ Level 3 patients - requiring two or more organ support (or requiring invasive ventilation or CVVH)
▪ Cases requiring specialist tertiary centre ITU (e.g. neuro, cardiac, liver)
▪ 24 x 7 Anesthetic consultant cover▪ 12 x 7 Critical care cover with remote support from York OOH▪ Non-consultant grade anaesthetist resident on-call
Level 3 critical care
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Supra-specialist surgical procedures performed in national centres (e.g., vascular, neurosurgery)
▪ Level 2 critical care▪ Access to endoscopy3
▪ Access to interventional radiology3
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours (available within 30 mins OOH) + Resident junior OOH cover
High peri-operative risk elective surgery

69
Model 3C – Front door assessment A&E model, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, SSPAU, lower risk obs
1 NB – direct referrals from community GPs to AAU and Surgical assessment not included2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
Discharge
Admit
Discharge
Stabilise & transfer toother centres
Level 3Critical care
AMB
Ward
Discharge
Assessment
Lower risk obstetrics
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Accident & Emergency24x7 with seniordecision maker
Full surgical and medical take with combined emergency assessment unit (CEAU)
Short Stay PaediatricUnit (SSPAU)
Non-urgent care
Stabilise & transfer
DischargeFrailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit CEAU
ENP or GP
ANP GP
Initial care
Discharge
DETAILED MODEL DESCRIPTIONS
Discharge

70
Model 3C – Front door assessment A&E model, full medical take, 24 x 7 emergency surgery, L3 critical care, high peri-op risk electives, SSPAU, lower risk obs
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH)
2 May require transfer of the patient to provide treatment 3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 4 Reports aspirational situation - at present 24 x 7 NCEPOD theatre not provided
DETAILED MODEL DESCRIPTIONS
Conditions Covered Conditions not coveredOther services requiredStaffing
Obstetric unit
▪ Lower risk births >36 weeks of gestation▪ Acute/ Emergency gynaecology▪ Antenatal care in day assessment unit or in community▪ Postnatal care in hospital if complex or community
(short stay in unit after birth)
▪ Women with complex conditions requiring treatment at specialist centres (e.g. Congenital heart disease)
▪ Women with pregnancies requiring specialist foetal medicine
▪ Women at risk of delivery below 36 weeks gestation
▪ Level 3 critical care▪ Acute/emergency gynae▪ Dedicated obstetric operating theatre
▪ 12 x 7 consultant obstetrician on labour unit (OOH on-call obstetrician available within 30 minutes)
▪ 24 x 7 on-site non-consultant grade obstetrician▪ 24 x 7 immediate access to advanced neonatal resuscitation (e.g.
ANNP, Middle-grade or Reg Neonates)▪ 24 x 7 midwifery on site▪ 24 x 7 immediate access to anaesthetist
24 x 7 medical take & AAU
▪ All acute medical admissions except for hyper-acute stroke and PPCI
▪ Hyper-acute stroke patients▪ PPCI▪ Acute haematology/oncology2
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ Frailty service▪ Diagnostics ▪ Standardised care pathways with GP admits direct
to CEAU
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site
24 x 7 emergency general surgery
▪ All emergency general surgery procedures and trauma & orthopaedic proceeds not requiring specialist tertiary care
▪ Specialist surgical procedures that require transfer to a specialist centre (e.g., vascular, neurosurgery)
▪ Children likely to require surgery
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ NCEPOD staffed theatre 24 x 74
▪ 24 x 7 general surgery consultant for emergency surgery on site in-hours. Consultant available within 30 mins OOH
▪ Surgical registrar OOH and consultant on-call▪ 24 x 7 Access to trauma and orthopaedic surgery▪ Anaesthetist available
Level 3 critical care
▪ Level 3 patients - requiring two or more organ support (or requiring invasive ventilation or CVVH)
▪ Cases requiring specialist tertiary centre ITU (e.g. neuro, cardiac, liver)
▪ 24 x 7 Anesthetic consultant cover▪ 12 x 7 Critical care consultant cover with remote support from York
OOH▪ Non-consultant grade anaesthetist resident on-call
High peri-operative risk elective surgery
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Super-specialist surgical procedures performed in national centres (e.g., vascular, neurosurgery)
▪ At least level 2 critical care▪ Access to endoscopy2
▪ Access to interventional radiology2
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours (available within 30 mins OOH) + Resident junior OOH cover
SSPAU1 + ambulatory care
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient admissions▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Cons. paediatrician on site 15 x 7▪ Shared staff with A&E with paediatric expert / ANP / SpR covering
OOH▪ Facilities for children available 7 days through SSPAU and ED/UTC
▪ All A&E attendances and GP referrals▪ GP out of hours services at UTC▪ Trauma patients (including those suitable for a trauma
unit)
▪ Major complex conditions needing treatment at specialist centres (e.g. polytrauma, hyper acute stroke, PPCI)
▪ Level 3 critical care▪ Combined Emergency assessment unit▪ NCEPOD staffed theatre 24x7▪ IR and acute bleed service accessible through
standardised pathways2
▪ Primary care front door ▪ Stabilise and transfer patients requiring care at
another site
▪ Senior decision maker with appropriate skill set (e.g. Gen surgery or ED to see abdominal pain)
▪ Multidisciplinary ‘total medical workforce” to see patients at front door
▪ Advanced Nurse Practitioner (ANP) support▪ HCAs
Front door assessment A&E model
Assumes diagnostic imaging3 and pathology services exist in all models
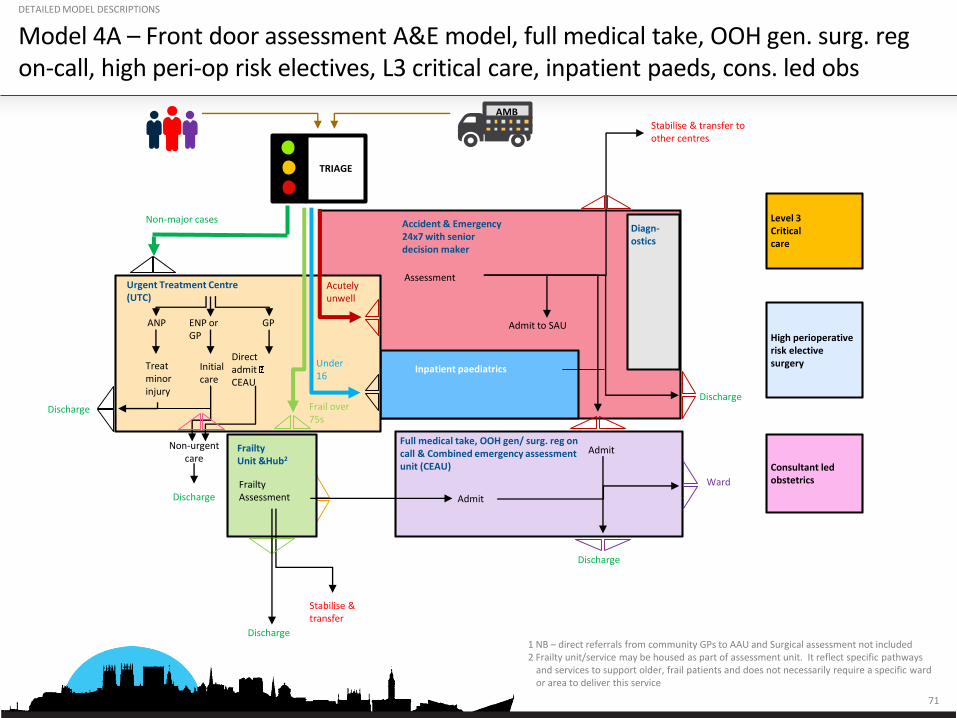
71
Model 4A – Front door assessment A&E model, full medical take, OOH gen. surg. regon-call, high peri-op risk electives, L3 critical care, inpatient paeds, cons. led obs
1 NB – direct referrals from community GPs to AAU and Surgical assessment not included2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
Discharge
Admit
Discharge
Stabilise & transfer toother centres
Level 3Critical care
AMB
Ward
Discharge
Assessment
Consultant led obstetrics
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Accident & Emergency24x7 with seniordecision maker
Full medical take, OOH gen/ surg. reg on call & Combined emergency assessment unit (CEAU)
Inpatient paediatrics
Non-urgent care
Stabilise & transfer
DischargeFrailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit CEAU
ENP or GP
ANP GP
Initial care
Discharge
DETAILED MODEL DESCRIPTIONS
Discharge

72
Model 4A – Front door assessment A&E model, full medical take, OOH gen. surg. regon-call, high peri-op risk electives, L3 critical care, inpatient paeds, cons. led obs
1 May necessitate transfer of the patient to provide treatment 2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 3 Would be available for advice with capability to attend Scarborough if patient requiring surgery is too unstable to be transferred. Would require expansion of current general surgical consultant rota
DETAILED MODEL DESCRIPTIONS
Conditions Covered Conditions not coveredOther services requiredStaffing
24 x 7 medical take + AAU
▪ All acute medical admissions except for hyper-acute stroke and PPCI
▪ Hyper acute stroke patients▪ PPCI▪ Acute haematology/oncology2
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ Frailty service▪ Diagnostics ▪ Standardised care pathways with GP admits direct
to CEAU
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site
OOH general surgery on-call reg.
▪ All trauma and orthopaedic procedures not requiring specialist tertiary care
▪ All general surgical admissions not requiring surgery overnight or tertiary centre input
▪ Specialist surgical procedures that require transfer to a specialist centre (e.g., vascular, neurosurgery)
▪ At least level 2 critical care with capacity and capability to ventilate and resuscitate
▪ NCEPOD staffed theatre 12 x 7; on-call team overnight
▪ Transfer of patients requiring urgent overnight surgical intervention
▪ 12 x 7 general surgery consultant on site▪ Surgical registrar or middle grade OOH with remote cons. support at
York▪ 24 x 7 Access to trauma and orthopaedic surgery▪ 24 x 7 Access to anaesthetics/critical care▪ 2nd on call consultant availability at York3
Front door assessment A&E model
▪ All A&E attendances and GP referrals▪ GP out of hours services at UTC▪ Trauma patients (including those suitable for a trauma
unit)
▪ Major complex conditions needing treatment at specialist centres (e.g. polytrauma, hyper acute stroke, PPCI)
▪ Level 3 critical care▪ Combined Emergency assessment unit▪ NCEPOD staffed theatre 24 x 7▪ IR and acute bleed service accessible through
standardised pathways1
▪ Primary care front door ▪ Stabilise and transfer patients requiring care at
another site
▪ Senior decision maker with appropriate skill set (e.g. General surgery or ED to see abdominal pain)
▪ Multidisciplinary ‘total medical workforce” to see patients at front door
▪ Advanced Nurse Practitioner (ANP) support▪ HCAs
Level 3 critical care
▪ Level 3 patients - requiring two or more organ support (or requiring invasive ventilation or CVVH)
▪ Cases requiring specialist tertiary centre ITU (e.g. Neuro, Cardiac, Liver)
▪ 24 x 7 Anesthetic consultant cover▪ 12 x 7 Critical care consultant cover with remote support from York
OOH▪ Non-consultant grade anaesthetist resident on-call
High peri-operative risk elective surgery
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Super-specialist surgical procedures performed in national centres (e.g., vascular, neurosurgery)
▪ At least Level 2 critical care▪ Access to endoscopy1
▪ Access to interventional radiology1
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours + OOH resident junior (OOH hours consultant support from York)
Obstetric unit
▪ Low and high risk births >32 weeks of gestation▪ Acute/emergency gynaecology▪ Antenatal care in day assessment unit or in community▪ Postnatal care in hospital if complex or community
(short stay in unit after birth)▪ Elective gynae
▪ Women with complex conditions requiring treatment at specialist centres (e.g. Congenital heart disease)
▪ Women with pregnancies requiring specialist foetal medicine
▪ Women at risk of delivery below 32 weeks gestation2
▪ Level 3 critical care▪ Acute/emergency gynae▪ Dedicated obstetric operating theatre
▪ 12 x 7 consultant obstetrician on labour unit (OOH on-call consultant available on-site)
▪ 24 x 7 immediate paediatric cover and neonatal care▪ 24 x 7 midwifery on site▪ 24 x 7 immediate access to anaesthetist▪ Theatre team on-site
Inpatient paeds
▪ All acute general paediatric illnesses requiring admission
▪ Common care pathways across patch
▪ Acutely unwell children requiring paedscritical care support
▪ Neonates requiring Level 2 or 3 neonatal care
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service for L2/3 care
▪ 10 WTE consultant paediatricians to cover 24 x 7 rota (on-site and immediate available in hours; on site within 30 mins OOH)
▪ 24 x 7 resident non-consultant grade doctor
Assumes diagnostic imaging2 and pathology services exist in all models

73
Model 4C – Front door assessment A&E model, full medical take, OOH gen. surg. regon-call, high peri-op risk electives, L3 critical care, SSPAU, lower risk obs
1 NB – direct referrals from community GPs to AAU and Surgical assessment not included2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
Discharge
Admit
Discharge
Stabilise & transfer toother centres
Level 3Critical care
AMB
Ward
Discharge
Assessment
Lower risk obstetrics
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Accident & Emergency24x7 with seniordecision maker
Full medical take, OOH gen/ surg. reg on call & Combined emergency assessment unit (CEAU)
Short stay PaediatricAssessment Unit (SSPAU)
Non-urgent care
Stabilise & transfer
DischargeFrailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit CEAU
ENP or GP
ANP GP
Initial care
Discharge
DETAILED MODEL DESCRIPTIONS
Discharge

74
Model 4C – Front door assessment A&E model, full medical take, OOH gen. surg. regon-call, high peri-op risk electives, L3 critical care, SSPAU, lower risk obs
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH)
2 May require transfer of the patient to provide treatment 3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 4 Would be available for advice with capability to attend Scarborough if patient requiring surgery is too unstable to be transferred. Would require expansion of current general surgical consultant rota
DETAILED MODEL DESCRIPTIONS
Assumes diagnostic imaging2 and pathology services exist in all models
Conditions Covered Conditions not coveredOther services requiredStaffing
Obstetric unit
▪ Lower risk births >36 weeks of gestation▪ Acute/ Emergency gynaecology▪ Antenatal care in day assessment unit or in community▪ Postnatal care in hospital if complex or community
(short stay in unit after birth)
▪ Women with complex conditions requiring treatment at specialist centres (e.g. Congenital heart disease)
▪ Women with pregnancies requiring specialist foetal medicine
▪ Women at risk of delivery below 36 weeks gestation
▪ Level 3 critical care▪ Acute/emergency gynae▪ Dedicated obstetric operating theatre
▪ 12 x 7 consultant obstetrician on labour unit (OOH on-call obstetrician available within 30 minutes)
▪ 24 x 7 on-site non-consultant grade obstetrician▪ 24 x 7 immediate access to advanced neonatal resuscitation (e.g.
ANNP, Middle-grade or Reg Neonates)▪ 24 x 7 midwifery on site▪ 24 x 7 immediate access to anaesthetist
SSPAU1 + ambulatory care
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient admissions▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Consultant paediatrician on site 15 x 71
▪ Shared staff with A&E with paediatric expert / ANP / SpR covering OOH
▪ Facilities for children available 7 days through SSPAU and ED/UTC
24 x 7 medical take + MAU
▪ All acute medical admissions except for hyper-acute stroke and PPCI
▪ Hyper-acute stroke patients ▪ PPCI▪ Acute haematology/oncology2
▪ Level 3 critical care▪ IR and acute bleed service accessible through
standardised pathways2
▪ Frailty service▪ Diagnostics ▪ Standardised care pathways with GP admits direct
to CEAU
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site
OOH general surgery on-call reg.
▪ All trauma and orthopaedic procedures not requiring specialist tertiary care
▪ All general surgical admissions not requiring surgery overnight or tertiary centre input
▪ Specialist surgical procedures that require transfer to a specialist centre e.g., vascular, neurosurgery)
▪ Children likely to require surgery
▪ At least level 2 critical care with capacity and capability to ventilate and resuscitate
▪ NCEPOD staffed theatre 12 x 7; on-call team overnight
▪ Transfer of patients requiring urgent overnight surgical intervention
▪ 12 x 7 general surgery consultant on site▪ Surgical registrar or middle grade OOH with remote cons. support at
York▪ 24 x 7 Access to trauma and orthopaedic surgery▪ 24 x 7 Access to anaesthetics/critical care▪ 2nd on call consultant availability at York4
Level 3 critical care
▪ Level 3 patients - requiring two or more organ support (or requiring invasive ventilation or CVVH)
▪ Cases requiring specialist tertiary centre ITU (e.g. neuro, cardiac, liver)
▪ 24 x 7 Anesthetic consultant cover▪ 12 x 7 Critical care consultant cover with remote support from York
OOH▪ Non-consultant grade Anaesthetist resident on-call
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Super-specialist surgical procedures performed in national centres (e.g., vascular, neurosurgery)
▪ At least level 2 critical care▪ Access to endoscopy2
▪ Access to interventional radiology2
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours + OOH resident junior (OOH hours consultant support from York)
High peri-operative risk elective surgery
▪ All A&E attendances and GP referrals▪ GP out of hours services at UTC▪ Trauma patients (including those suitable for a trauma
unit)
▪ Major complex conditions needing treatment at specialist centres (e.g. polytrauma, hyper acute stroke, PPCI)
▪ Level 3 critical care▪ Combined Emergency assessment unit▪ NCEPOD staffed theatre 24x7▪ IR and acute bleed service accessible through
standardised pathways2
▪ Primary care front door ▪ Stabilise and transfer patients requiring care at
another site
▪ Senior decision maker with appropriate skill set (e.g. General surgery or ED to see abdominal pain)
▪ Multidisciplinary ‘total medical workforce” to see patients at front door
▪ Advanced Nurse Practitioner (ANP) support▪ HCAs
Front door assessment model A&E

75
Model 11D – Medical A&E + UTC, selective take, OOH surgical reg. on-call, L2 critical care, high peri-op risk electives, SSPAU, MW-led unit
1 NB – direct referrals from community GPs to MAU & SAU not included in this 2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
3 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
Discharge
Admit
Discharge
Stabilise & transfer toother centres
AMB
Ward
Discharge
Assessment
High perioperative risk elective surgery
TRIAGE
Admit
Diagn-ostics
Admit to SAU
Medical only A&E
Selective take & Medical assessment unit (MAU)
Short stay PaediatricAssessment Unit (SSPAU)
Stabilise & transfer
Frailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit MAU/SAU
ENP or GP
ANP GP
Initial care
Discharge
Surgical Assessment Unit (SAU)
Ambulatory CareUnit (ACU)
Non-urgent care
Discharge
DETAILED MODEL DESCRIPTIONS
Discharge
Level 3Critical care
24 x 7 Midwife –led maternityUnit3

76
Model 11D – Medical A&E + UTC, selective take, OOH surgical reg on-call, L2 critical care, high peri-op risk elective surgery, SSPAU, MW-led unit
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH) 2 May require transfer of the patient to provide treatment 3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 4 Would be available for advice with capability to attend Scarborough if patient requiring surgery is too unstable to be transferred. Would require expansion of current general surgical consultant rota 5 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
DETAILED MODEL DESCRIPTIONS
Assumes diagnostic imaging3 and pathology services exist in all models
Conditions Covered Conditions not coveredOther services requiredStaffing
Selective take + MAU
▪ All non- high acuity ▪ Stroke patients, hyper acute cardiac care, subset of patients requiring level 3 critical care
▪ Acute bleeds▪ Hepatology
▪ Acute assessment unit▪ Frailty service▪ Diagnostics▪ Standardised care pathways with GP admits direct
to AAU/frailty unit
▪ Acute or General medicine consultant on site 15 x 7; on-call and within 30 minutes OOH
▪ 24 x 7 medical registrar on site
24 x 7 Midwife led unit5
▪ Low risk births, 37 - 42 weeks of gestation▪ Antenatal care / in day assessment unit or in
community▪ Postnatal care in community (short stay in-unit after
birth)
▪ Women requiring obstetric care, high-risk pregnancies, maternal-foetal medicine, epidurals, C-sections
▪ Acute/emergency gynae
▪ Capacity to stabilise and transfer▪ Standardised protocols for in utero or neonatal
transfer within regional network▪ Gynae hot clinic
▪ 24 x 7 Midwife, support worker and HCA presence▪ Additional midwife support on call▪ Support staff▪ Primary care hubs for midwife clinics
SSPAU1 + ambulatory care
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient admission▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Consultant paediatrician on site 15 x 71
▪ Shared staff with A&E with paediatric expert / ANP / SpR covering OOH
▪ Facilities for children available 7 days through SSPAU and ED/UTC
OOH general surgery on-call reg.
▪ All trauma and orthopaedic procedures not requiring specialist tertiary care
▪ All general surgical admissions not requiring surgery overnight or tertiary centre input
▪ Specialist surgical procedures that require transfer to a specialist centre (e.g., vascular, neurosurgery)
▪ At least level 2 critical care with capacity and capability to ventilate and resuscitate
▪ NCEPOD staffed theatre 12 x 7; on-call team overnight
▪ Transfer of patients requiring urgent overnight surgical intervention
▪ 12 x 7 general surgery consultant on site▪ Surgical registrar OOH with remote cons. support at York▪ 24 x 7 Access to trauma and orthopaedic surgery▪ 24 x 7 Access to anaesthetics/critical care▪ 2nd on call consultant availability at York4
Level 2 critical care
▪ Level 2 patients - single organ support (excluding mechanical ventilation) such as ionotropes and invasive BP monitoring
▪ Patients requiring multiple organ support▪ 24 x 7 anaesthetic consultant cover▪ 12 x 7 critical care consultant cover (remote support from York OOH)▪ Non-consultant grade anaesthetist resident OOH▪ Transfer team for step up and stabilise if required▪ 1:2 RN
▪ Capability to provide short term ventilation for patients awaiting transfer
▪ Full range of elective surgical procedures that do not require super-specialist or tertiary centre input
▪ Super-specialist surgical procedures performed in national centres (e.g., neurosurgery, vascular surgery)
▪ At least level 2 critical care▪ Access to endoscopy2
▪ Access to interventional radiology2
▪ Full surgical team & OOH cover provided by surgical specialities; on-call anaesthetic consultant
▪ Consultant level in-hours + OOH resident junior (OOH hours consultant support from York)
High peri-operative risk elective surgery
▪ Medical ED attendances, minor illnesses and injuries, GP referrals
▪ Stabilise and transfer others
▪ Surgical ED attendances e.g. patients requiring laparotomy
▪ Other complex needs (any life or limb threatening conditions); conditions requiring critical care
▪ Stabilise and transfer patients requiring care at another site
▪ MAU and frailty unit on site▪ Primary care front door
▪ ED/acute medicine consultant on site in hours; available within 30 mins OOH
▪ Stabilise & transfer team (anaesthetist + ODP/Crit care nurse) on site▪ Mental Health practitioner available ▪ Multidisciplinary team to support frailty unit
Medical only A&E + UTC

77
Model 15D – Medical A&E + UTC, selective take, ambulatory emergency surgery, L1 enhanced ward care, mod peri-op risk elective surgery, SSPAU, MW-led unit
1 NB – direct referrals from community GPs to MAU & SAU not included in this 2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
3 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
Discharge
Admit
Discharge
Ward
Discharge
Assessment
Admit
Diagn-ostics
Admit to SAU
Medical only A&E
Selective take & Medical assessment unit
Short stay PaediatricAssessment Unit (SSPAU)
Stabilise & transfer
Frailty Assessment
Non-major cases
Frailty Unit &Hub2
Acutelyunwell
Under 16
Frail over 75s
Urgent Treatment Centre (UTC)
Treatminorinjury
Direct admit MAU/AES
ENP or GP
ANP GP
Initial care
Discharge
Ambulatory EmergencySurgery (AES)
Ambulatory CareUnit (ACU)
Non-urgent care
Discharge
Frail over 75s
TRIAGE Stabilise & transfer to other centres
Major emergencies
Transfer to other centres
AMBTRIAGE
DETAILED MODEL DESCRIPTIONS
Discharge
24 x 7 Midwife –led maternityUnit3
Moderate peri-operative risk elective surgery
Level 1 plus critical care service
Step up to transfer to Level 2/3

78
Assumes diagnostic imaging3 and pathology services exist in all models
Conditions Covered Conditions not coveredOther services requiredStaffing
Model 15D – Medical A&E + UTC, selective take, ambulatory emergency surgery, L1 enhanced ward care, mod peri-op risk elective surgery, SSPAU, MW-led unit
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH)
2 May require transfer of the patient to provide treatment 3 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures 4 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
DETAILED MODEL DESCRIPTIONS
Selective take + MAU
▪ All non- high acuity ▪ Patients already established on CPAP▪ Medical assessment unit▪ Frailty service▪ Diagnostics▪ Standardised care pathways with GP admits
direct to AAU/frailty unit
▪ 12 x 7 medicine consultant on site; on-call OOH and available on site within 30 mins
▪ 24 x 7 medical registrar on site
24 x 7 Midwife led unit4
▪ Low risk births, 37 - 42 weeks of gestation▪ Antenatal care / in day assessment unit or in
community▪ Postnatal care in community (short stay in-unit
after birth)
▪ Women requiring obstetric care, high-risk pregnancies, maternal-foetal medicine, epidurals, C-sections
▪ Acute/emergency gynae
▪ Capacity to stabilise and transfer▪ Standardised protocols for in utero or
neonatal transfer within regional network▪ Gynae hot clinic
▪ 24 x 7 Midwife, support worker and HCA presence▪ Additional midwife support on call▪ Support staff▪ Primary care hubs for midwife clinics
SSPAU1 + ambulatory care
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient
admissions▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Consultant paediatrician on site 15 x 71
▪ Shared staff with A&E with paediatric expert / ANP / SpRcovering OOH
▪ Facilities for children available 7 days through SSPAU and ED/UTC
Amb emergsurgery only
▪ Ambulatory surgical activity e.g., abscess drainage, non-complex gall bladders, piles (add to DC lists)
▪ All emergency procedures not required within 12 hours
▪ All high risk patients and high complexity procedures
▪ Emergency laparotomy + all non-medical abdominal pain
▪ Capacity to stabilise and transfer▪ Dedicated surgical consultant on a limited rota (e.g. 10 x 7) and on standby to offer opinion
▪ NCEPOD theatre available for ~3 hours a day
▪ Capacity to stabilise and transfer ▪ Level 1 patients only – no organ support required▪ Patients already established on CPAP
▪ Patients requiring organ support (including vasopressor support)
▪ More intensive monitoring, (e.g. cardiac monitoring) supported by transfer team
▪ Access to anaesthetist 24 x 7▪ 1:4 RN
Level 1 plus critical care service
Moderate peri-operative risk elective surgery
▪ All mid and low perioperative risk procedures▪ Endoscopy, IR + other procedures▪ On-call emergency surgery
▪ High complexity and / or high risk patients▪ Patients likely to require critical care
admissions perioperatively
▪ Level 1 enhanced ward▪ Capability to stabilise and transfer if urgent
intervention required OOH
▪ Full surgical team provided in hours; OOH support provided by junior with remote support from York
▪ 24 x 7 immediate access to anaesthetic support (on-call consultant available within 30 mins)
▪ Medical ED attendances, minor illnesses and injuries, GP referrals
▪ Stabilise and transfer others
▪ Surgical ED attendances e.g. patients requiring laparotomy
▪ Other complex needs (any life or limb threatening conditions); conditions requiring critical care
▪ Stabilise and transfer patients requiring care at another site
▪ Frailty service▪ Primary care front door
▪ ED/acute medicine consultant on site in hours; available within 30 mins OOH
▪ Stabilise & transfer team (anaesthetist + ODP) on site▪ Mental Health practitioner available ▪ Multidisciplinary team to support frailty service
Medical only A&E + UTC

79
Model 17D – UTC only, selective take, ambulatory emergency surgery, L1 enhanced ward care, moderate peri-op risk elective surgery, SSPAU, MW-led unit
1 NB – direct referrals from community GPs to MAU & SAU not included in this2 Frailty unit/service may be housed as part of assessment unit. It reflect specific pathways
and services to support older, frail patients and does not necessarily require a specific ward or area to deliver this service
3 Model could also be delivered with lower risk consultant led obstetrics in place of Midwife led unit
Ambulatory CareUnit (ACU)
Frailty Unit and Hub2
Non-urgent
care
Stabilise & transfer
Discharge
Selective take + Medical Assessment Unit (MAU)
Admit
Ward
Discharge
Frailty Assessment
Ambulatory EmergencySurgery (AES)
AMB
Frail over 75s
Non-major cases
TRIAGE
Discharge
Urgent Care Centre (UTC)
GP direct admits+ T&O pathways(e.g. #NOF)
Diagnostics
TRIAGE
Major emergencies
Transfer to other centres
Short Stay Paediatric Assessment Unit (SSPAU)
Under 16Treat
minorinjury
Direct admit MAU
ENP or GPANP GP
Initial care
DETAILED MODEL DESCRIPTIONS
Discharge
24 x 7 Midwife –led maternityUnit3
Moderate peri-operative risk elective surgery
Level 1Care plus critical care services
Step up to transfer to Level 2/3

80
Assumes diagnostic imaging3 and pathology services exist in all models
Conditions Covered Conditions not coveredOther services requiredStaffing
Model 17D – UTC only, selective take, ambulatory emergency surgery, L1 enhanced ward care, moderate peri-op risk elective surgery, SSPAU, MW-led unit
1 Modelled as 15 hours per day but configurations open up to 24 hours per day could be considered (where consultant could be on site 12 x 7 and available within 30 mins OOH) 2 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
DETAILED MODEL DESCRIPTIONS
Amb emergsurgery only
▪ Ambulatory surgical activity e.g., abscess drainage, non-complex gall bladders, piles (add to DC lists)
▪ All emergency procedures not required within 12 hours
▪ All high risk patients and high complexity procedures
▪ Emergency laparotomy + all non-medical abdominal pain
▪ Capacity to stabilise and transfer▪ Dedicated surgical consultant on a limited rota (e.g. 10 x 7) and on standby to offer opinion
▪ NCEPOD theatre available for ~3 hours a day
Moderate peri- operative risk elective surgery
▪ All mid and low perioperative risk procedures▪ Endoscopy, IR + other procedures▪ On-call emergency surgery
▪ High complexity and / or high risk patients▪ Patients likely to require critical care
admissions perioperatively
▪ Level 1 enhanced ward▪ Capability to stabilise and transfer if urgent
intervention required OOH▪ Access to anaesthetic support 24 x 7
▪ Full surgical team provided in hours; OOH support provided by junior with remote support from York
▪ 24 x 7 immediate access to anaesthetic support (on-call consultant available within 30 mins)
24 x 7 Midwife led unit
▪ Low risk births, 37 - 42 weeks of gestation▪ Antenatal care / in day assessment unit or in
community▪ Postnatal care in community (short stay in-unit
after birth)
▪ Women requiring obstetric care, high-risk pregnancies, maternal-foetal medicine, epidurals, C-sections
▪ Capacity to stabilize and transfer▪ 24 x 7 Midwife, support worker and HCA presence▪ Additional midwife support on call▪ Support staff▪ Primary care hubs for midwife clinics
Selective take + MAU
▪ All non- high acuity ▪ Stroke patients, hyper acute cardiac care, subset of patients requiring or at risk of requiring level 2/3 critical care
▪ Acute bleeds▪ Hepatology
▪ Frailty service▪ Diagnostics▪ Standardised care pathways with GP admits
direct to MAU
▪ 12 x 7 medicine consultant on site; on-call OOH and available on site within 30 mins
▪ 24 x 7 medical registrar on site
SSPAU1 + ambulatory care
▪ Minor acute illnesses, minor trauma, burns and infections, IV antibiotics
▪ Acutely unwell children transferred to hospital with inpatient paediatrics
▪ Repatriate cases from York ED if appropriate
▪ Illness requiring >8 hours observation▪ Children likely to require inpatient surgery▪ Children likely require inpatient
admissions▪ Neonates requiring level 2/3 NICU
▪ Stabilise and transfer capability for critically ill children
▪ Regional neonatal transport service▪ Standardised protocols for transfer of patients
requiring inpatient care
▪ Consultant paediatrician on site 15 x 71
▪ Shared staff with A&E with paediatric expert / ANP / SpRcovering OOH
▪ Facilities for children available 7 days through SSPAU and ED/UTC
Level 1 plus critical care service
▪ Level 1 patients only – no organ support required▪ Patients already established on CPAP
▪ Patients requiring organ support (including vasopressor support)
▪ More intensive monitoring, e.g., cardiac monitoring supported by transfer team
▪ Access to anaesthetist 24 x 7▪ 1:4 RN
▪ Capacity to stabilise and transfer
▪ All minor illnesses and injury▪ Stabilise and transfer others
▪ Suspected complex fractures; other complex needs (any life or limb threatening conditions); conditions requiring critical care
▪ Stabilise and transfer patients requiring care at another site
▪ Possibly ambulatory care observation and assessment
▪ Frailty service
▪ GPs▪ Advanced Nurse Practitioner (ANP) support▪ HCAs▪ Multidisciplinary team of GPs, geriatricians, ANPs to support
frailty service▪ Mental Health practitioner available ▪ Remote access to A&E consultant
UTC only

81
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
– Shortlisting and initial combinations
– Detailed descriptions of clinical models
– Activity shift assumptions
▪ Further refinement of clinical models and key questions
Contents

82
Approach to preliminary activity shift assumptions
▪ Clinically-led judgement
▪ Based on interviews with Clinical Directors, Deputy Clinical Directors and other senior clinicians for key service lines
▪ Generally good alignment in perspectives between clinicians within service lines
▪ Assumptions selectively supported / informed by activity data e.g., proportion of “low risk” obstetrics patients
▪ Forms basis for more detailed bottom-up / prospective analysis of activity shifts in a later phase of work
ACTIVITY SHIFT ASSUMPTIONS
Application
Methodology
▪ Clinical activity requires bed capacity and brings income and expenditure with it
▪ Shifts in clinical activity are used to model shifts in bed capacity, income and expenditure between hospitals
These preliminary assumptions will need to be revisited as the clinical models are further developed ahead of any final evaluation

83
Clinical activity shift assumptions were developed for each model
Model 15DModel 3C Model 11D Model 17DModel 4A Model 4CModel 1A Model 1C
Paedia-trics
Obs and Gynae
A&E
Emerg-encygen. surgery
Acute medicine
Trauma & ortho-paedics
Majors 100 95 95 100 95 70 240
Minors 100 100 100 100 100 100 100100
Resus 100 97 97 100 95 65 140
Daycase 100 100 100 100 100 100 100100
Non-elective 100 100 100 95 95 90 4545
Elective 100 100 100 100 100 100 100100
Outpatient 100 100 100 100 100 100 100100
Daycase 100 100 100 100 100 100 100100
Non-elective 100 95 95 90 85 40 3030
Elective 100 100 100 100 100 100 6565
Outpatient 100 100 100 100 100 100 10095
Daycase 100 100 100 100 100 100 100100
Non-elective 100 95 95 100 100 40 3030
Elective 100 100 100 100 100 100 9595
Outpatient 100 100 100 100 100 100 13011301
Crit. care 100 100 100 90 90 70 1010
Outpatient 100 100 100 100 100 100 100100
Births 100 40 40 100 40 25 2525
Elective gynae 100 100 100 100 100 75 5050
Day case gynae 100 100 100 100 100 100 100100
Nonelective gynae 100 100 100 75 75 50 5050
Antenatal care 100 95 95 100 95 95 9595
Outpatient gynae 100 100 100 100 100 100 100100
Inpatient 100 60 60 95 60 60 6060
Neonates 100 25 25 100 25 0 00
SOURCE: Interviews with Clinical Directors and lead clinicians
1 OP likely to increase due to increased referrals to fracture clinic in UTC model
ACTIVITY SHIFT ASSUMPTIONS
X % of current Scarborough activity which would stay in Scarborough under each model

84
▪ Clinical workstream timeline
▪ Summary of the clinical case for change
▪ Evaluation criteria
▪ Best practice pathways
▪ Clinical configuration models
▪ Further refinement of clinical models and key questions
Contents

85
Taking into account clinical interdependencies, the CRG agreed to look at eight potential clinical models in more detail
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
▪ Frailty unit / hub included in all models▪ Assumes diagnostic imaging1 and pathology services exist in all models
Model 3C Model 11D Model 15DModel 4A Model 4CModel 1A Model 1C Model 17D
Paediatrics
Paeds assessment unit
Paeds assessment unit2
Paeds assessment unit
Inpatient paediatrics
Paeds assessment unit
Inpatient paediatrics
Paeds assessment unit
Paeds assessment unit
MaternityConsultant led obstetrics unit
Midwife led unit
Midwife led unit
Consultant led obstetrics unit
Consultant led obstetrics unit
Consultant led obstetrics unit
Consultant led obstetrics unit
Midwife led unit
Critical care
Level 3 Level 2 Level 1 plus critical care service
Level 3 Level 3 Level 3 Level 3 Level 1 plus critical care service
A&E
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24x7 A&E –consultant led
24x7 A&E –consultant led
UTC only
Emergency surgery
24x7 emergency general surgery
OOH middle grade on site (cons support from York)
Ambulatory emergency surgery only
OOH middle grade on site (cons support from York)
OOH middle grade on site (cons support from York)
24x7 emergency general surgery
24x7 emergency general surgery
Ambulatory emergency surgery only
Acute medicine
Full medical take + AAU
Selective medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
Selective medical take + AAU
Elective surgery
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
EVALUATION OF CLINICAL MODEL

86
These were subsequently reduced to five clinical models
Paediatrics
Maternity
Critical care
A&E
Emergency surgery
Acute medicine
Elective surgery
Model 11D
Paeds assessment unit
Midwife led unit
Level 2
24/7 A&E with front door assessment
OOH middle grade on site (cons support from York)
Selective medical take + AAU
Cases with high peri-operative risk
Model 15D
Paeds assessment unit
Midwife led unit
Level 1 plus critical care service
24/7 A&E with front door assessment
Ambulatory emergency surgery only
Selective medical take + AAU
Cases with moderate perioperative risk
Model 3C
Paeds assessment unit
Level 3
24/7 A&E with front door assessment
24x7 emergency general surgery
Full medical take + AAU
Cases with high peri-operative risk
Model 4A
Inpatient paediatrics
Level 3
24/7 A&E with front door assessment
OOH middle grade on site (cons support from York)
Full medical take + AAU
Cases with high peri-operative risk
Model 4C
Paeds assessment unit
Level 3
24/7 A&E with front door assessment
OOH middle grade on site (cons support from York)
Full medical take + AAU
Cases with high peri-operative risk
Model 1A
Inpatient paediatrics
Obstetric unit
Level 3
24x7 A&E –consultant led
24x7 emergency general surgery
Full medical take + AAU
Cases with high peri-operative risk
Model 1C
Paeds assessment unit
Obstetric unit
Level 3
24x7 A&E –consultant led
24x7 emergency general surgery
Full medical take + AAU
Cases with high peri-operative risk
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
▪ Frailty unit / hub included in all configurations▪ Assumes diagnostic imaging1 and pathology services exist in all models
Model 17D
Paeds assessment unit
Midwife led unit2
Level 1 plus critical care service
UTC only
Ambulatory emergency surgery only
Selective medical take + AAU
Cases with moderate perioperative risk
Developing and maintaining a 24/7 consultant-led A&E was considered unfeasible from a staffing perspective
A UTC model was considered to provide insufficient access to A&E for patients
Obstetric unit
Obstetric unit
Obstetric unit
EVALUATION OF CLINICAL MODELS
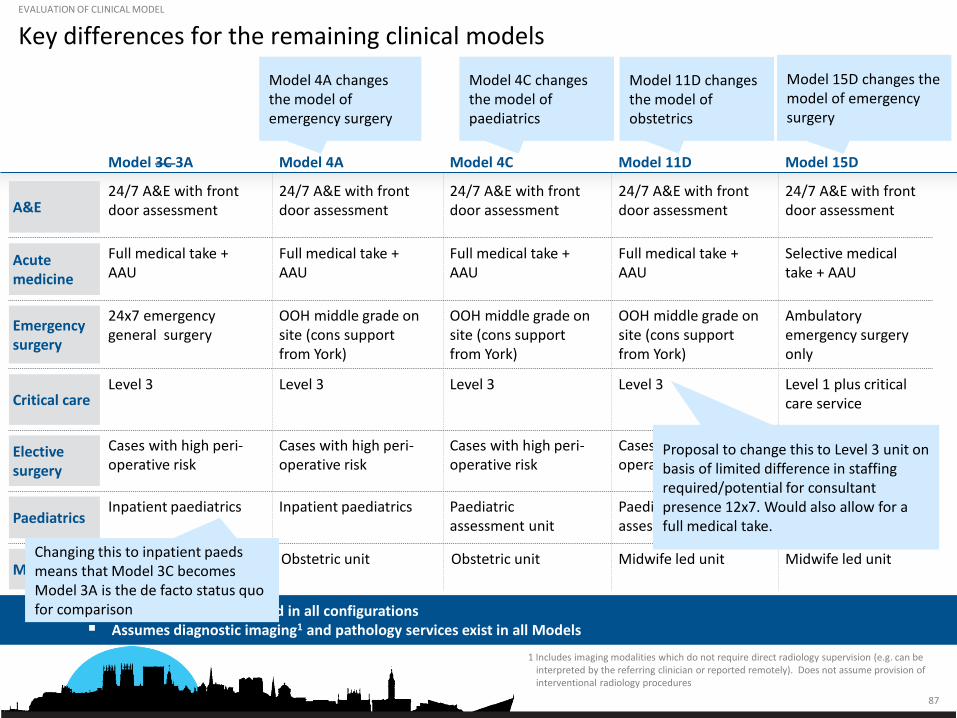
87
Key differences for the remaining clinical models
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
▪ Frailty unit / hub included in all configurations▪ Assumes diagnostic imaging1 and pathology services exist in all Models
Model 3C 3A Model 11D Model 15DModel 4A Model 4C
PaediatricsInpatient paediatrics Paediatric
assessment unitPaediatricassessment unit
Inpatient paediatrics Paediatricassessment unit
Critical careLevel 3 Level 3 Level 1 plus critical
care serviceLevel 3 Level 3
A&E24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
Emergency surgery
24x7 emergency general surgery
OOH middle grade on site (cons support from York)
Ambulatory emergency surgery only
OOH middle grade on site (cons support from York)
OOH middle grade on site (cons support from York)
Elective surgery
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Acute medicine
Full medical take + AAU
Selective medical take + AAU
Full medical take + AAU
Full medical take + AAU
Full medical take + AAU
MaternityMidwife led unit Midwife led unitObstetric unit Obstetric unit Obstetric unit
Model 4A changes the model of emergency surgery
Model 4C changes the model of paediatrics
Model 11D changes the model of obstetrics
Model 15D changes the model of emergency surgery
EVALUATION OF CLINICAL MODEL
Changing this to inpatient paeds means that Model 3C becomes Model 3A is the de facto status quo for comparison
Proposal to change this to Level 3 unit on basis of limited difference in staffing required/potential for consultant presence 12x7. Would also allow for a full medical take.

88
This results in four models to do further work on, in addition to the status quo
1 Includes imaging modalities which do not require direct radiology supervision (e.g. can be interpreted by the referring clinician or reported remotely). Does not assume provision of interventional radiology procedures
▪ Frailty unit / hub included in all configurations▪ Assumes diagnostic imaging1 and pathology services exist in all models
Model 3A (status quo) Model 11D Model 15DModel 4A Model 4C
PaediatricsInpatient paediatrics Paediatric assessment
unitPaediatricassessment unit
Inpatient paediatrics Paediatric assessment unit
Critical careLevel 3 Level 3 Level 1 plus critical
care serviceLevel 3 Level 3
A&E24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
24/7 A&E with front door assessment
Emergency surgery
24x7 emergency general surgery
OOH middle grade on site (cons support at York)
Ambulatory emergency surgery only
OOH middle grade on site (cons support at York)
OOH middle grade on site (cons support at York)
Elective surgery
Cases with high peri-operative risk
Cases with high peri-operative risk
Cases with moderate perioperative risk
Cases with high peri-operative risk
Cases with high peri-operative risk
Acute medicine
Full medical take + AAU Selective medical take + AAU
Full medical take + AAU Full medical take + AAU
Full medical take + AAU
MaternityMidwife led unit Midwife led unitObstetrics unit Obstetrics unit Obstetrics unit
EVALUATION OF CLINICAL MODELS

89
Questions that need to be addressed in the next phase of work
1. Emergency surgery: a. Would it be possible to staff a 24/7 consultant surgical rota?b. Would it be possible to recruit sufficient number of middle-grades to maintain a model of OOH on
site with consultant support from York?c. Even if it is possible, will this not result in as many transfers as if there was an ambulatory unit? If
that is the case, should the ambulatory emergency surgery model be adopted in more options e.g. Model 11D?
d. Which of these models are compatible with trauma unit status? What flexibility is there in how trauma unit status is defined?
2. Obstetrics and paediatricsa. Is there anything that could be done to make an inpatients paediatrics rota sustainable?b. What other innovative models of paediatrics could support neonatal care in a consultant led
obstetric service? For example a specialist neonatal nurse led model or a “block” staffing model with paediatricians from the wider region working a one week resident on call model?
c. Would it be possible to maintain a Midwife Led Unit given expected volumes? What staffing model would this require? Are there different models of MLUs? For example a pop up unit (or units) in different parts of the area?
3. Critical carea. Would it be possible to maintain L2/3 model of critical care without inpatient surgery?
These questions are not intended to assess clinical models – rather to establish a fact base in order that a
full assessment can subsequently take place.