Anatomy and Physiology, Seventh Edition Rod R. Seeley Idaho State University Trent D. Stephens Idaho...
41
Anatomy and Physiology, Seventh Edition Rod R. Seeley Idaho State University Trent D. Stephens Idaho State University Philip Tate Phoenix College Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. *See PowerPoint Image Slides for all figures and tables pre-inserted into PowerPoint without notes. Chapter 24 Chapter 24 Lecture Lecture Outline Outline *
-
Upload
elfrieda-spencer -
Category
Documents
-
view
217 -
download
0
Transcript of Anatomy and Physiology, Seventh Edition Rod R. Seeley Idaho State University Trent D. Stephens Idaho...

Anatomy and Physiology, Seventh Edition
Rod R. SeeleyIdaho State UniversityTrent D. StephensIdaho State UniversityPhilip TatePhoenix College
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
*See PowerPoint Image Slides for all figures and tables pre-inserted into PowerPoint without notes.
Chapter 24Chapter 24
Lecture OutlineLecture Outline**

Digestive Process
Figure 23.2

GI Tract
• External environment for the digestive process
• Regulation of digestion involves:– Mechanical and chemical stimuli – stretch
receptors, osmolarity, and presence of substrate in the lumen
– Extrinsic control by CNS centers– Intrinsic control by local centers
Receptors of the GI Tract
• Mechano- and chemoreceptors respond to:– Stretch, osmolarity, and pH– Presence of substrate, and end products of
digestion
• They initiate reflexes that:– Activate or inhibit digestive glands – Mix lumen contents and move them along

Nervous Control of the GI Tract
• Intrinsic controls– Nerve plexuses near the GI tract initiate short
reflexes– Short reflexes are mediated by local enteric
plexuses (gut brain)
• Extrinsic controls– Long reflexes arising within or outside the GI tract – Involve CNS centers and extrinsic autonomic
nerves

Nervous Control
of the GI Tract
Figure 23.4

Secretions of the Stomach• Chyme: ingested food plus stomach secretions• Mucus: surface and neck mucous cells
– Viscous and alkaline– Protects from acidic chyme and enzyme pepsin– Irritation of stomach mucosa causes greater mucus
• Intrinsic factor: parietal cells. Binds with vitamin B12 and helps it to be absorbed. B12 necessary for DNA synthesis
• HCl: parietal cells– Kills bacteria– Stops carbohydrate digestion by inactivating salivary amylase– Denatures proteins– Helps convert pepsinogen to pepsin
• Pepsinogen: chief cells. Packaged in zymogen granules released by exocytosis. Pepsin catalyzes breaking of covalent bonds in proteins.
• G-cells: secrete the hormone gastrin which stimulates HCl secretion from parietal cells

Hydrochloric Acid Production
1. CO2 and Cl- diffuse from the blood into the stomach cell.2. CO2 combines with H2O to form H2CO3.
3. H2CO3 dissociates into bicarbonate (HCO3-) and H+.4. H+ combines with Cl- in duct of gastric gland to form HCl-.5. An ATP pump is necessary to pump the HCl- into the duct since the concentration of
HCl- is about a million times more concentrated in the duct than in the cytosol of the cell.

Regulation of Gastric Secretion
• Neural and hormonal mechanisms regulate the release of gastric juice
• Stimulatory and inhibitory events occur in three phases– Cephalic (reflex) phase: prior to food entry– Gastric phase: once food enters the stomach– Intestinal phase: as partially digested food enters
the duodenum

Release of Gastric Juice
Figure 23.16

Cephalic Phase• The taste or smell of food, tactile
sensations of food in the mouth, or even thoughts of food stimulate the medulla oblongata.
• Parasympathetic action potentials are carried by the vagus nerves to the stomach.
• Preganglionic parasympathetic vagus nerve fibers stimulate postganglionic neurons in the enteric plexus of the stomach.
• Postganglionic neurons stimulate secretion by parietal and chief cells (HCl and pepsin) and stimulate the secretion of the hormone gastrin.
• Gastrin is carried through the circulation back to the stomach where it stimulates further secretion of HCl and pepsin.

Gastric Phase
• Distention of the stomach activates a parasympathetic reflex. Action potentials are carried by the vagus nerves to the medulla oblongata.
• Medulla oblongata stimulates further secretions of the stomach.
• Distention also stimulates local reflexes that amplify stomach secretions.

Intestinal Phase• Chyme in the duodenum with a
pH less than 2 or containing lipids inhibits gastric secretions by three mechanisms
1. Sensory input to the medulla from the duodenum inhibits the motor input from the medulla to the stomach. Stops secretion of pepsin and HCl.
2. Local reflexes inhibit gastric secretion
3. Secretin, gastric inhibitory polypeptide, and cholecystokinin produced by the duodenum inhibit gastric secretions in the stomach.

Regulation of Gastric Emptying
• Gastric emptying is regulated by:– The neural enterogastric reflex– Hormonal (enterogastrone) mechanisms
• These mechanisms inhibit gastric secretion and duodenal filling
• Carbohydrate-rich chyme quickly moves through the duodenum
• Fat-laden chyme is digested more slowly causing food to remain in the stomach longer
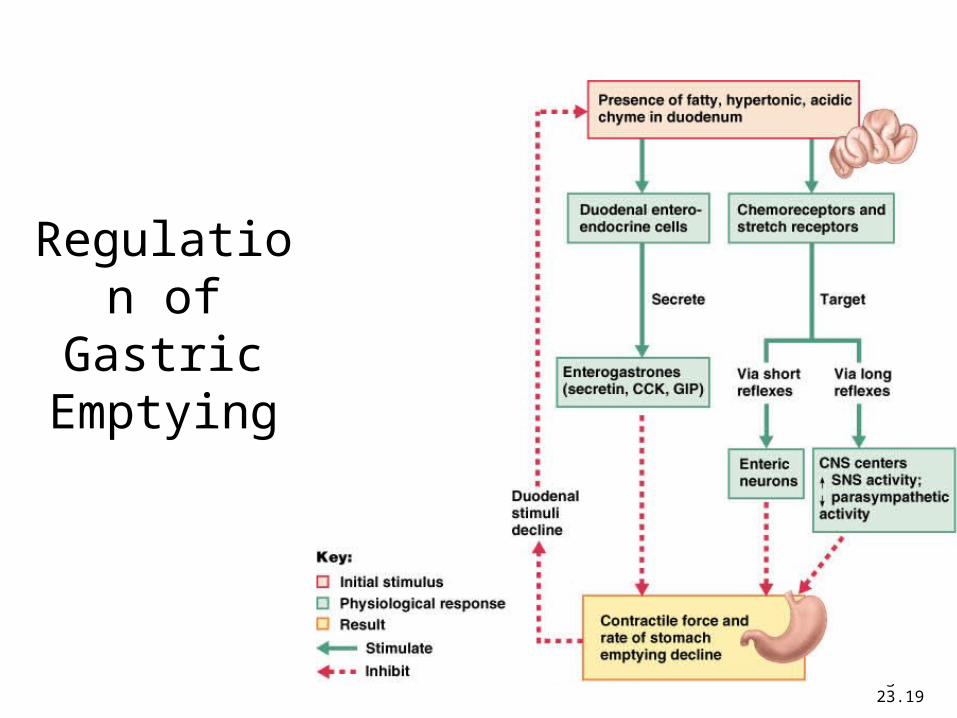
Regulation of Gastric Emptying
Figure 23.19
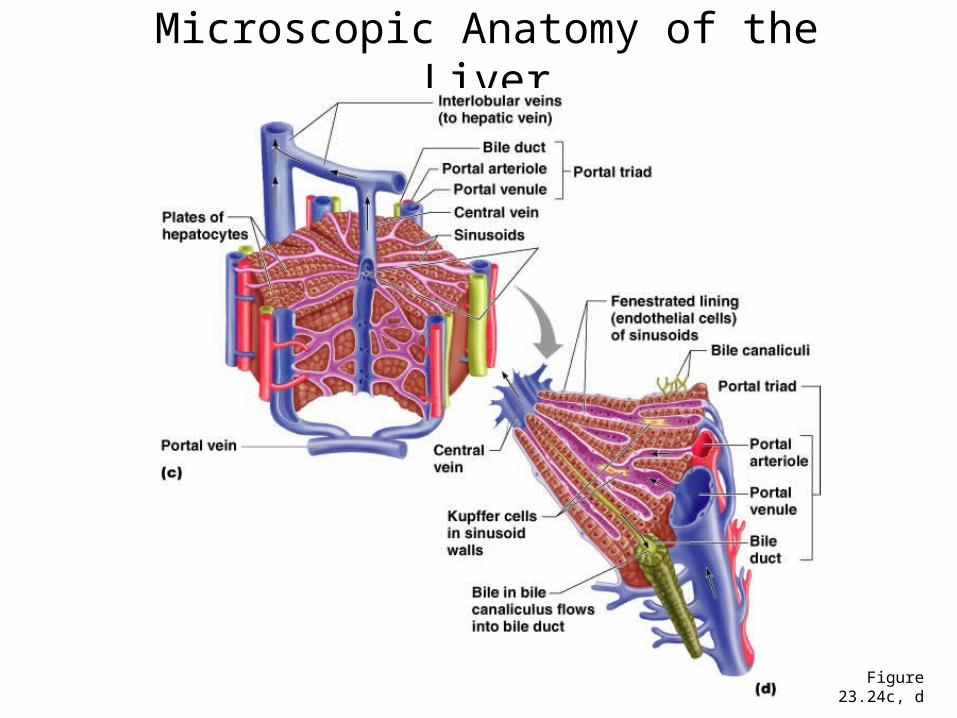
Microscopic Anatomy of the Liver
Figure 23.24c, d

Histology of the Liver
• Connective tissue septa branch from the porta into the interior
– Divides liver into lobules– Nerves, vessels and ducts follow
the septa
• Lobules: portal triad at each corner– Three vessels: hepatic portal vein,
hepatic artery, bile duct (hepatic duct in diagram)
– Central vein in center of lobule
• Central veins unite to form hepatic veins that exit liver and empty into inferior vena cava
• Hepatic cords: radiate out from central vein. Composed of hepatocytes
• Hepatic sinusoids: between cords, lined with endothelial cells and hepatic phagocytic (Kupffer) cells
• Bile canaliculus: between cells within cords

Functions of the Liver• Bile production: 600-1000 mL/day. Bile salts (bilirubin), cholesterol, fats, fat-
soluble hormones, lecithin– Neutralizes and dilutes stomach acid– Bile salts emulsify fats. Most are reabsorbed in the ileum.– Secretin (from the duodenum) stimulates bile secretions, increasing water
and bicarbonate ion content of the bile• Storage
– Glycogen, fat, vitamins, copper and iron. Hepatic portal blood comes to liver from small intestine.
• Nutrient interconversion– Amino acids to energy producing compounds– Hydroxylation of vitamin D. Vitamin D then travels to kidney where it is
hydroxylated again into its active form• Detoxification
– Hepatocytes remove ammonia and convert to urea• Phagocytosis
– Kupffer cells phagocytize worn-out and dying red and white blood cells, some bacteria
• Synthesis– Albumins, fibrinogen, globulins, heparin, clotting factors

Composition of Bile
• A yellow-green, alkaline solution containing bile salts, bile pigments, cholesterol, neutral fats, phospholipids, and electrolytes
• Bile salts are cholesterol derivatives that:– Emulsify fat– Facilitate fat and cholesterol absorption– Help solubilize cholesterol
• Enterohepatic circulation recycles bile salts • The chief bile pigment is bilirubin, a waste
product of heme

Regulation of Bile Release
Figure 23.25

Blood and Bile Flow
Through the Liver

Pancreas• Pancreas both endocrine and
exocrine• Head, body and tail• Endocrine: pancreatic islets.
Produce insulin, glucose, and somatostatin
• Exocrine: groups acini (grape-like cluster) form lobules separated by septa.
• Intercalated ducts lead to intralobular ducts lead to interlobular ducts lead to the pancreatic duct.
• Pancreatic duct joins common bile duct and enters duodenum at the hepatopancreatic ampulla controlled by the hepatopancreatic ampullar sphincter

Pancreatic Secretions: Pancreatic Juice• Aqueous. Produced by columnar epithelium lining smaller ducts. Na+, K+,
HCO3-, water. Bicarbonate lowers pH inhibiting pepsin and providing proper
pH for enzymes• Enzymatic portion:
– Trypsinogen– Chymotrypsinogen– Procarboxypeptidase– Pancreatic amylase– Pancreatic lipases– Deoxyribonucleases and ribonucleases
• Interaction of duodenal and pancreatic enzymes.– Enterokinase from the duodenal mucosa and attached to the brush
border activates trypsinogen to trypsin. – Trypsin activates chymotrypsinogen to chymotrypsin– Trypsin activates procarboxypeptidase to carboxypeptidase.
• Trypsin, chymotrypsin and carboxypeptidase digest proteins: proteolytic.• Pancreatic amylase continues digestion of starch• Pancreatic lipase digests lipids• Deoxyribonucleases and ribonucleases digest DNA and ribonucleic acid,
respectively

Bicarbonate Ion Production in Pancreas

Regulation of Pancreatic Secretion
Figure 23.28

Secretions of Large Intestine• Mucus provides protection
– Parasympathetic stimulation increases rate of goblet cell secretion
• Pumps: bacteria produce acid and the following remove acid from the epithelial cells that line the large intestine– Exchange of bicarbonate ions for chloride ions– Exchange of sodium ions for hydrogen ions
• Bacterial actions produce gases (flatus) from particular kinds of carbohydrates found in legumes and in artificial sugars like sorbitol
• Bacteria produce vitamin K which is then absorbed• Feces consists of water, undigested food (cellulose),
microorganisms, sloughed-off epithelial cells

Digestion, Absorption, Transport
• Digestion – Breakdown of food molecules for absorption into
circulation • Mechanical: breaks large food particles to small• Chemical: breaking of covalent bonds by digestive
enzymes
• Absorption and transport– Molecules are moved out of digestive tract and into
circulation for distribution throughout body


Carbohydrates: Hydrolyzed into Monosaccharides
• Glucose is transported to cells requiring energy; insulin influences rate of transport

Lipids
• Include triglycerides, phospholipids, steroids, fat-soluble vitamins
• Bile salts surround fatty acid and glycerol to form micelles
• Chylomicrons are 90% triglyceride, 5% cholesterol, 4% phospholipid, 1% protein.
• Chylomicrons enter blood stream and travel to adipose tissue. In blood, triglycerides converted back into fatty acids and glycerol where they are transported into the adipose cells, then converted back into triglycerides.

Transport of Lipids Across Intestinal Epithelium

Fatty Acid Absorption
Figure 23.36

Lipoproteins • All lipids carried in the blood are done so in combination with protein to make them soluble in plasma.
• Cholesterol: 15% ingested; 85% manufactured in liver and intestinal mucosa
• Lipids are lower density than water; proteins are higher density than water
• Chylomicrons: 99% lipid and 1% protein (extremely low density); enter lymph
• VLDL: 92% lipid, 8% protein– Form in which lipids leave the liver– Triglycerides removed from VLDL
and stored in adipose cells. VLDL has been converted to LDL.
• LDL: 75% lipid, 25% protein– Transports cholesterol to cells– Cells have LDL receptors– # of LDL receptors become less once
cell’s lipid/cholesterol needs are met.• HDL: 55% lipid, 45% protein
– Transports excess cholesterol from cells to liver

Transport of LDL into Cells

Proteins
• Pepsin breaks proteins into smaller polypeptide chains
• Proteolytic enzymes produce small peptide chains– Dipeptides, tripeptides, amino acids
• After absorption, amino acids are are carried through the hepatic portal vein to the liver.

Amino Acid Transport

Chemical Digestion: Nucleic Acids
• Absorption: active transport via membrane carriers
• Absorbed in villi and transported to liver via hepatic portal vein
• Enzymes used: pancreatic ribonucleases and deoxyribonuclease in the small intestines

Electrolyte Absorption• Most ions are actively absorbed along the length of
small intestine – Na+ is coupled with absorption of glucose and amino
acids– Ionic iron is transported into mucosal cells where it binds
to ferritin
• Anions passively follow the electrical potential established by Na+
• K+ diffuses across the intestinal mucosa in response to osmotic gradients
• Ca2+ absorption:– Is related to blood levels of ionic calcium– Is regulated by vitamin D and parathyroid hormone
(PTH)

Water Absorption• 95% of water is absorbed in the small
intestines by osmosis• Water moves in both directions across
intestinal mucosa• Net osmosis occurs whenever a concentration
gradient is established by active transport of solutes into the mucosal cells
• Water uptake is coupled with solute uptake, and as water moves into mucosal cells, substances follow along their concentration gradients

Water and Ions
• Water: can move in either direction across wall of small intestine depending on osmotic gradients
• Ions: sodium, potassium, calcium, magnesium, phosphate are actively transported