Adrenal Lymphangioma Clinically Mimicking a …...mas.Adrenal pseudocysts are cystic lesions which...
3
SURGERY Adrenal Lymphangioma Clinically Mimicking a Cystic Pheochromocytoma: a Case Report and Literature Review Silvia Taccogna 1 & Enrico Papini 2 & Paola Alexandra Mascioli 1 & Tatiana Di Cesare 3 & Andrea Liverani 3 Accepted: 14 November 2018 /Published online: 19 November 2018 # Springer Nature Switzerland AG 2018 Introduction Adrenal cystic lymphangiomas are rare benign lesions [1], which are usually asymptomatic, and may be incidentally dis- covered at imaging work-up, at abdominal surgery or at au- topsy [2, 3]. They are quite infrequent in adult subjects, 0.06– 0.18% of the general population [3], and appear as thin- walled, fluid density lesions. At CT scan, they usually appear as hypodense, nonenhancing lesions with imaging features that may not fully discriminate lymphangiomas from malig- nant or hyperfunctioning lesions such as adrenal carcinoma or pheochromocytomas [4]. So, their surgical removal may be necessary to rule out their types of adrenal neoplasms [5–7]. We report the case of a patient with a right adrenal cystic lymphangioma clinically mimicking a pheochromocytoma and the review of the radiological and pathological features of the tumor. Case Presentation A 34-year-old male was admitted to the Endocrinology Department of our hospital because of a severe clinical con- dition characterized by recurrent episodes of headache, palpi- tation, and hypertension. Physical findings, including heart and lung examination, were unremarkable. Laboratory tests were normal. During the work-up for his hypertension, an abdominal CT scan was performed, which showed a previous- ly unrecognized mass 6.6 × 3.3 × 4.8 cm in the right adrenal gland. Cystic degeneration was present with nonvascularized walls (Fig. 1). On the basis of the clinical suspicion of pheochromocyto- ma, an iodine-123 ( 123 I)-labeled metaiodobenzylguanidine (MIBG) scintigraphy was performed as a complementary ex- amination. The test was substantially negative. The determi- nation of urinary metanephrine provided border-line results (360 mg/24 h with high-performance liquid chromatography [HPLC] method). Serum ACTH, cortisol, and aldosterone were within normal limits. Due to the ambiguous clinical pic- ture and the persistent symptoms, the patient underwent a laparoscopic right adrenalectomy. The postoperative course was uneventful. Two months after surgery, mean blood pres- sure levels returned to normal. The surgical specimen showed an undamaged adrenal gland, 7.5 × 5.2 × 1.0 cm, occupied by a well-circumscribed multicystic mass measuring 6 × 4 × 1 cm. The numerous cavities of the lesion contained watery fluid (Fig. 2). These small cystic spaces were characterize by thin walls and were lined by flat, bland endothelial cells. The fibrous septs between the cystic spaces showed foci of normal adrenal tissue (Fig. 3a). On immunohistochemical stain, the endothe- lial cells showed a strong immunoreactivity for CD31, factor VIII, CD34 and D2-40 (Fig. 3b), and absent staining for cytokeratin and calretinin. The conclusive histopathological diagnosis was adrenal cystic lymphangioma. Discussion This article reports a rare case of symptomatic cystic lymphangioma originating from the left adrenal gland in a mal patient successfully treated by complete surgical resec- tion. The majority of intra-abdominal cystic lymphangiomas This article is part of the Topical Collection on Surgery * Silvia Taccogna [email protected] 1 Department of Pathology, Regina Apostolorum Hospital, Via S. Francesco 50, 00041 Albano Laziale (RM), Italy 2 Department of Endocrinology and Metabolism, Regina Apostolorum Hospital, Albano Laziale (RM), Italy 3 Department of General Surgery, Regina Apostolorum Hospital, Albano Laziale (RM), Italy SN Comprehensive Clinical Medicine (2019) 1:93–95 https://doi.org/10.1007/s42399-018-0027-2
Transcript of Adrenal Lymphangioma Clinically Mimicking a …...mas.Adrenal pseudocysts are cystic lesions which...

SURGERY
Adrenal Lymphangioma Clinically Mimicking a CysticPheochromocytoma: a Case Report and Literature Review
Silvia Taccogna1 & Enrico Papini2 & Paola Alexandra Mascioli1 & Tatiana Di Cesare3 & Andrea Liverani3
Accepted: 14 November 2018 /Published online: 19 November 2018# Springer Nature Switzerland AG 2018
Introduction
Adrenal cystic lymphangiomas are rare benign lesions [1],which are usually asymptomatic, and may be incidentally dis-covered at imaging work-up, at abdominal surgery or at au-topsy [2, 3]. They are quite infrequent in adult subjects, 0.06–0.18% of the general population [3], and appear as thin-walled, fluid density lesions. At CT scan, they usually appearas hypodense, nonenhancing lesions with imaging featuresthat may not fully discriminate lymphangiomas from malig-nant or hyperfunctioning lesions such as adrenal carcinoma orpheochromocytomas [4]. So, their surgical removal may benecessary to rule out their types of adrenal neoplasms [5–7].
We report the case of a patient with a right adrenal cysticlymphangioma clinically mimicking a pheochromocytomaand the review of the radiological and pathological featuresof the tumor.
Case Presentation
A 34-year-old male was admitted to the EndocrinologyDepartment of our hospital because of a severe clinical con-dition characterized by recurrent episodes of headache, palpi-tation, and hypertension. Physical findings, including heartand lung examination, were unremarkable. Laboratory tests
were normal. During the work-up for his hypertension, anabdominal CTscan was performed, which showed a previous-ly unrecognized mass 6.6 × 3.3 × 4.8 cm in the right adrenalgland. Cystic degeneration was present with nonvascularizedwalls (Fig. 1).
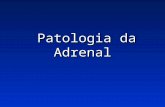
On the basis of the clinical suspicion of pheochromocyto-ma, an iodine-123 (123I)-labeled metaiodobenzylguanidine(MIBG) scintigraphy was performed as a complementary ex-amination. The test was substantially negative. The determi-nation of urinary metanephrine provided border-line results(360 mg/24 h with high-performance liquid chromatography[HPLC] method). Serum ACTH, cortisol, and aldosteronewere within normal limits. Due to the ambiguous clinical pic-ture and the persistent symptoms, the patient underwent alaparoscopic right adrenalectomy. The postoperative coursewas uneventful. Two months after surgery, mean blood pres-sure levels returned to normal. The surgical specimen showedan undamaged adrenal gland, 7.5 × 5.2 × 1.0 cm, occupied bya well-circumscribed multicystic mass measuring 6 × 4 ×1 cm. The numerous cavities of the lesion contained wateryfluid (Fig. 2).
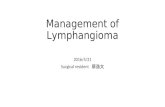
These small cystic spaces were characterize by thin wallsand were lined by flat, bland endothelial cells. The fibroussepts between the cystic spaces showed foci of normal adrenaltissue (Fig. 3a). On immunohistochemical stain, the endothe-lial cells showed a strong immunoreactivity for CD31, factorVIII, CD34 and D2-40 (Fig. 3b), and absent staining forcytokeratin and calretinin.
The conclusive histopathological diagnosis was adrenalcystic lymphangioma.
Discussion
This article reports a rare case of symptomatic cysticlymphangioma originating from the left adrenal gland in amal patient successfully treated by complete surgical resec-tion. The majority of intra-abdominal cystic lymphangiomas
This article is part of the Topical Collection on Surgery
* Silvia [email protected]
1 Department of Pathology, Regina Apostolorum Hospital, Via S.Francesco 50, 00041 Albano Laziale (RM), Italy
2 Department of Endocrinology andMetabolism, Regina ApostolorumHospital, Albano Laziale (RM), Italy
3 Department of General Surgery, Regina Apostolorum Hospital,Albano Laziale (RM), Italy
SN Comprehensive Clinical Medicine (2019) 1:93–95https://doi.org/10.1007/s42399-018-0027-2

is located in the mesentery, in contrast to adrenal location thatis very rare [2]. Adrenal cysts are uncommon, with a reportedincidence of 0.06–0.18% in autopsy series [6, 7]; cysticmasses account for only about 4–22% of all adrenalincidentalomas. Adrenal cysts are usually asymptomatic; ifsymptoms do occur, they are usually related to mass effectand include pain, a gastrointestinal disturbance or a palpablemass [4]. The differential diagnosis of adrenal cysts includesprimary or metastatic adrenal tumors, benign or malignantcystic neoplasms, hemorrhage secondary to trauma, bleedingdisorder, burns, shock or toxemia, and infections [2, 8]. Cysticdegeneration of pheochromocytomas is not common [6, 9].Patients with cystic pheochromocytoma are often
asymptomatic and yield negative plasma and urine biochem-ical analysis. In a majority of cases were female, half had nosymptoms, and half had normal biochemical analysis [10].Microscopic aspect undivided four categories: parasitic, epi-thelial, pseudocysts, and endothelial in origin [8, 11]. Parasiticcysts are the least common, epithelial cysts consist of trueglandular cysts and embryonal cysts, including cystic adeno-mas. Adrenal pseudocysts are cystic lesions which arise with-in the adrenal gland. They are surrounded by a fibrous walldevoid of an epithelial lining [11]. The first case of adrenalcystic lymphangioma had been reported in 1965; recently,approximately 69 immunohistochemically cases have beenreported in the literature [10–13]. Lymphangiomas are benigncystic vascular lesions, most frequently discovered in child-hood. They are most commonly located in the neck, axillaryregion, and mediastinum (95%).The remaining 5% are foundin the abdominal cavity [1]. Adrenal cystic lymphangiomasare asymptomatic and rarely do they present labile
Fig. 2 The gross photograph of the resected specimen with cystic spaces,note the residual adrenal tissue (arrow)
a
b
Fig. 3 aMultiple dilated cystic spaces filled with pale pink proteinaceousamorphous, homogeneous fluid. The wall is made of fibrous tissue withadrenal cortex cellular groups (H&E × 40). b D2-40 antibody immuno-stain (× 40) showing positive staining of cystic lining endothelial cells(high-magnification inset)
Fig. 1 The cross-sectional CT image
94 SN Compr. Clin. Med. (2019) 1:93–95

hypertension [14]. It is issued that mass effect of the tumorwas the cause of hypertension; therefore, the blood pressurereturned to normal after removal of the adrenal mass. Pre-operative diagnosis of retroperitoneal lymphangioma, in gen-eral, is challenging and rare. Laboratory findings are nonspe-cific and are usually not helpful as a diagnostic tool. On com-puterized tomography, cystic lymphangiomas are identified ashypodense, nonenhancing lesions in the adrenal gland [15].Current treatment recommendations for adrenal cystlymphangioma are that small asymptomatic nonfunctioninglesions can simply be observed, whereas large cysts (> 5 cmin diameter), cyst with high density on unenhanced CT (>10 HU) or delayed washout of the contrast medium, signifi-cant growth of the cyst on serial imaging, functional cysts,symptomatic cysts, and cysts which can cause complicationssuch as hemorrhage, rupture, or infection should be excised[11]. Surgical resection represents the definitive treatment ifthe cystic lymphangioma is symptomatic [4]. Histologically,adrenal lymphangiomas are characterized by multiloculatedcystic cavities. The cysts are lined by a single layer of flattenedendothelial cells. Immunohistochemically, cells with an endo-thelial lining mostly stain positively for CD31, factor VIII,CD34 (endothelial specific markers), and D2-40 (lymphaticmarker). The management strategy is influenced by three fac-tors: (a) functional status of the cyst, (b) the possibility ofincidental malignancy, and (c) potential complications suchas hemorrhage or infection [6, 16].
Conclusion
Cystic lymphangioma of the adrenal gland is a rare pathologythat should be included in the differential diagnosis of cysticlesions of the adrenal glands. If the patient is symptomatic,definitive treatment is surgery. So, definite diagnosis relies onhistologic and immunohistochemical examination.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
References
1. Beham. Lymphangioma. In: WHO classification of tumours of softtissue and bone. IARC Lyon 2013. p. 144–5.
2. Ellis CL, Banerjee P, Carney E, Sharma R, Netto GJ. Adrenallymphangioma: clinicopathologic and immunohistochemical char-acteristics of a rare lesion. Hum Pathol. 2011;42:1013–8.
3. Zhao M, Gu Q, Li C, Yu J, Qi H. Cystic lymphangioma of adrenalgland: a clinicopathological study of 3 cases and review of litera-ture. Int J Clin Exp Pathol. 2014;7(8):5051–6.
4. Kasperlik-Załuska AA, Otto M, Cichocki A, Rosłonowska E,Słowinska-Srzednicka J, Zgliczyński W, et al. 1,161 patients withadrenal incidentalomas: indications for surgery. Langenbeck’s ArchSurg. 2008;393:121–6.
5. Makni A, Chebbi F, Fetirich F, Ksantini R, Bedioui H, Jouini M,et al. Surgical management of intra-abdominal cysticlymphangioma. Report of 20 cases. World J Surg. 2012May;36(5):1037–43. https://doi.org/10.1007/s00268-012-1515-2.
6. Rozenblit A, Morehouse HT, Amis ES. Cystic adrenal lesions: CTfeatures. Radiology. 1996;201(2):541–8.
7. Tagge DU, Baron PL. Giant adrenal cyst. Management and reviewof the literature. Am Surg. 1997;63:744–6.
8. Sebastiano C, Zhao X, Deng FM, Das K. Cystic lesions of theadrenal gland: our experience over the last 20 years. Hum Pathol.2013;44(9):1797–803.
9. Klingler PJ, Fox TP, Menke DM, Knudsen JM, Fulmer JT.Pheochromocytoma in an incidentally discovered asymptomaticcystic adrenal mass. Mayo Clin Proc. 2000;75:517–20.
10. Andreoni C, Krebs RK, Bruna PC, Goldman SM, Kater CE, AlvesMT, et al. Cystic phaeochromocytoma is a distinctive subgroupwith special clinical, imaging and histological features that mightmislead the diagnosis. BJU Int. 2008;101(3):345–50.
11. Bellantone R, Ferrante A, Raffaelli M, BoscheriniM, Lombardi CP,Crucitti F. Adrenal cystic lesions: report of 12 surgically treatedcases and review of the literature. J Endocrinol Investig. 1998;21:109–14.
12. Joliat GR, Melloul E, Djafarrian R, Schmidt S, Fontanella S, Yan P,et al. Cystic lymphangioma of the adrenal gland: report of a caseand review of the literature. World J Surg Oncol. 2015;13:58.
13. Liu H, Liang T, Lian J, Wang M, Liu C, Wang X, et al. Clinical andCT features of adrenal cystic lymphangioma: case series and liter-ature review. Int J Clin Exp Med. 2017;10(5):8472–80.
14. Lynn RB. Cystic lymphangioma of the adrenal associated witharterial hypertension. Can J Surg. 1965;8:92–5.
15. Guo YK, Yang ZG, Li Y, Deng YP, Ma ES, Min PQ, et al.Uncommon adrenal masses: CT and MRI features with histopath-ologic correlation. Eur J Radiol. 2007;62(3):359–70.
16. Chew SP, Sim R, Teoh TA, Low CH. Haemorrhage into non-functioning adrenal cysts report of two cases and review of theliterature. Ann Acad Med Singap. 1999;28:863.
SN Compr. Clin. Med. (2019) 1:93–95 95






![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://static.fdocuments.net/doc/165x107/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)