Addressing Suicide with Community Prevention and Clinical ...
31
Addressing Suicide with Community Prevention and Clinical Intervention: New York State’s Suicide Prevention Plan 2016-17 Jay Carruthers MD Director, Suicide Prevention Office April 18, 2017
Transcript of Addressing Suicide with Community Prevention and Clinical ...

Addressing Suicide with Community Prevention and Clinical Intervention: New York State’s
Suicide Prevention Plan 2016-17
Jay Carruthers MDDirector, Suicide Prevention OfficeApril 18, 2017

2
LearningObjectives
1. Describe the scope of the problem around suicide in New York State
2. Identify the 3 tiers or pillars of the NYS Suicide Prevention Plan 2016-17
3. Explain specific projects and programs used by New York State to prevent suicide

3
Suicide: An Enormous Public Health Problem
Copy (Arial Regular)
Nationally: 44,193 suicide deaths in the US in 2015*. § Surpassed annual deaths by motor vehicle accidents,
homicides, and breast cancer§ 10th leading cause of death for all ages§ National suicide rate: 13.3 per 100,000
New York State in 2014: 1,700 suicide deaths (only 4 states had more) § NYS suicide rate: 8.6 per 100,000§ 2.5x the number of homicides§ >75% of NYS suicides are male§ Suffocation (37%), firearms (28%), poisoning (17%)
Consistent with national trends: § NY state suicides have increased by 32% in last decade § Rate increase from 6.26 per 100,000 in 1999 to 8.6 in 2014§ Rate for those with SMI is 5-6x that of general population

4
-40%
-30%
-20%
-10%
0%
10%
20%
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
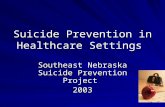
PercentChangeinAge-AdjustedDeathRatessince2003byCauseofDeath,2003-2013
Suicide Heartdisease Cancer Stroke All-cause
Suicide: An Enormous Public Health Problem
“From1999through2014,theage-adjustedsuiciderateintheUnitedStatesincreased24%,from10.5to13.0per100,000population”
NCHSDataBriefNo.241,April2016CenterforDiseaseControlandPrevention

5
NYSSuicideDeathRatebyCounty,2011-2013
2015Age-AdjustedSuicideRateRural=12.5per100,000Urban=7.5per100,000

6
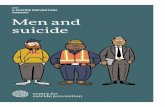
SuicideDeathsandHospitalizationsandEDVisitsforSelf-InflictedInjury,byGender,Age-AdjustedRateper100,000,NYS,2012-2014
12.9
46.8 45.1
3.9
61.557.3
0
10
20
30
40
50
60
70
Deaths Hospitalizations EDVisits
Rateper100
,000
Male Female
Source:NYSDepartmentofHealthhttps://www.health.ny.gov/statistics/prevention/injury_prevention/suicide_selfinflicted.htm
Men75%morelikelytodiebysuicide
Women22-34%morelikelytomakeanattemptandbehospitalizedortreatedinED

7
SuicideDeathsandHospitalizationsandEDVisitsforSelf-InflictedInjury,byAge,Age-AdjustedRateper100,000,NYS,2012-2014
1.2 5.1 8 9.2 12.7 9.7
36.6
111.6
94.5
73.2
55.4
22.3
87.9
192.9
116
61.2
26.7
6
0
20
40
60
80
100
120
140
160
180
200
10-14 15-19 20-24 25-44 45-64 65+
Rateper100
,000
Deaths Hospitalizations EDVisits
Source:NYSDepartmentofHealthhttps://www.health.ny.gov/statistics/prevention/injury_prevention/suicide_selfinflicted.htm
YouthhavehigherratesofEDvisitsandhospitalizationsforself-inflictedinjuries.
AmongNYShighschoolstudents:• 29%feltsad/hopeless• 16%seriouslyconsidered
suicide• 10%attemptedsuicide• 4%hadasuicideattemptthat
hadtobetreatedbyamedicalprofessional(YRBS,2015)

8
Suiciderateper100,000byage,raceandgender,NYS,2013-2015
Source:CDCWISQARShttps://webappa.cdc.gov/cgi-bin/broker.exe
11.6
15.817.4
23.922.3
21.0 20.6
23.9
0
5
10
15
20
25
15-24 25-34 35-44 45-54 55-64 65-74 75-84 85+
Rateper100
,000
AgeWhiteMen BlackMen AsianMen HispanicMen WhiteWomen

9
Drug,Alcohol,andSuicideMortality,ages50-54
Case&Deaton,2017

10
The New York State Suicide Prevention Plan 2016-17
4/22/17 10

11
https://www.omh.ny.gov/omhweb/resources/publications/suicde-prevention-plan.pdf

12
ZeroSuicide
CommunityInterventions
Surveillance&QIData

13
NYS Suicide Prevention Plan Strategy/Pillar 3: Better Use of Data

14
Leveraging Existing NYS Data SetsNIMRS PSYCKES/Medicaid SPARCS VitalStatistics
Other:NewYorkViolentDeathReportSystem!

15
NYS Surveillance Patterns: What We’ve Learned
• OMH (NIMRS) surveillance data suggest ~ half of all reported suicide deaths are among those that had an outpatient mental health visit within 30 prior to their death
– The highest suicide burden is among outpatient MH services, especially clinics.
– Suicides often occur within the first month of treatment. Must be ready from day 1!
• Preliminary* SPARCS and NYS vital statistics data suggest ~1:5 suicides take place within 7 days of a hospital discharge
– Improvements in transitional care are critical
15*needsfurthervalidationtesting

16
NYS Suicide Prevention Plan Strategy/Pillar 1: Zero Suicide

17
Bedrock Principles of Zero Suicide• Most suicide deaths are among people in care or recently seen in
healthcare.• Suicide prevention must become a core responsibility of health care
organizations and systems.• We have new knowledge about detecting and treating suicidality.
Very little of it is commonly used.• The gap between what we know and what we do can be fatal. We
must apply new knowledge.• Preventing suicide deaths in health care requires a systematic
clinical approach, not “the heroic efforts of crisis staff and individual clinicians.” • We have work to do.
Slide provided by Mike Hogan, PhD

18
Zero Suicide
www.zerosuicide.com

19
Seven key dimensions of the model:1. Lead–Make an explicit commitment to reduce suicide deaths2. Train–Develop a confident, competent, and caring workforce3. Identify–Identify every person at risk for suicide4. Engage–Engage clients in a Suicide Care Management Plan5. Treat–Treat suicidal thoughts and behaviors directly6. Transition–Follow patients through every care transition7. Improve–Apply data-driven quality improvement
www.zerosuicide.sprc.org
Zero Suicide Model for Suicide Prevention

WITHOUTIMPROVEDSUICIDECARE,PEOPLESLIPTHROUGHGAPS
EDC©2016.Allrightsreserved.
Ask?
ActforSafety?
TreatSuicidality?Reduce
LethalMeans?
EngagementandSupport?

THETOOLSOFZEROSUICIDEFILLTHEGAPS
EDC©2016.Allrightsreserved.

22
Zero Suicide: Early Evidence It Works
Centerstone BehavioralHealthSystem

23
Joint Commission Sentinel Event Alert 56: Detecting & Treating Suicide Ideation in All Settings
“The suggested actions in this alert cover suicide ideation detection, as well as the screening, risk assessment, safety, treatment, discharge, and follow-up care of at-risk individuals. Also included are suggested actions for educating all staff about suicide risk, keeping health care environments safe for individuals at risk for suicide, and documenting their care.”

24
Supporting Zero Suicide Implementation in NYS

25
– High Risk Suicide Care Management Plan/Pathway• Safety Plan with means restriction• Increased engagement and monitoring• Individualized plan that targets drivers
– Workforce training provided by Center for Practice Innovations at NYSPI/Columbia Univ. to support culture change
– Monthly performance metrics for CQI throughout – Project launch now:
180 mental health clinics signed up!
PSYCKES Outpatient Clinic Suicide Prevention CQI Project
Zero Suicide
Building Zero Suicide into the project architecture:– Systematic personalized screening for increased detection– Sound suicide risk assessment to guide treatment & engagement
(planning and prevention, not prediction)

26
NewYorkStateA-I-MforZeroModel• A common framework for assessing and responding to risk
mapped onto a set of best practices and tools• Common language for talking about suicide risk with patients,
family members, other medical and BH providers (eases promulgation across disciplines [MD/DO, SW, RN] within and across systems)
• Shifts mindset from prediction to prevention, facilitating immediate engagement around, and response to, risk
• Includes enhanced transitional care for those at-risk• Pilots launching in inpatient psychiatric units, EDs, and primary
care26

27
AdaptedfromPisaniCTL2015 27

28
NYS Suicide Prevention Plan Strategy/Pillar 2: Community Interventions

Developed by Mark LoMurray (1995-2004)§ Suicide prevention by adolescent Peer Leaders w/ adult mentors§ National Field Project Award – APHA (2005)
Testing/program refinement w/ U Rochester began 2006§Increases youth-adult connections, help-seeking acceptance across school populations
§First Peer Leader program to change school-wide risk-protective factors associated with reduced suicide in RCT w/ 18 schools (Wyman et al 2010, AJPH); NREPP 2012
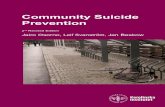
Creating Suicide Safer School Communities: Sources of Strength
29

Attempt Ideation
Node size: local network densityShading: suicide homophily
Illustrative High School Social Network w/ Sources of Strength: Clustering of High Risk Students on Periphery

31
Resources & Collaborators:Suicide Prevention Center of NY (coalitions, postvention, school and gate keeper trainings)Center for Practice Innovations SP-TIE (clinical trainings)
Save the Date: Sept 18-19 NYS Suicide Prevention Conference https://nyssuicidepreventionconference.org/
31