Suicide Prevention in Healthcare Settings Southeast Nebraska Suicide Prevention Project 2003.
63
Suicide Prevention in Suicide Prevention in Healthcare Settings Healthcare Settings Southeast Nebraska Southeast Nebraska Suicide Prevention Suicide Prevention Project Project 2003 2003
-
Upload
elmer-wilkins -
Category
Documents
-
view
228 -
download
5
Transcript of Suicide Prevention in Healthcare Settings Southeast Nebraska Suicide Prevention Project 2003.
Suicide Prevention in Suicide Prevention in Healthcare SettingsHealthcare Settings
Southeast Nebraska Suicide Southeast Nebraska Suicide Prevention Project Prevention Project
20032003
What Healthcare Settings?What Healthcare Settings?
Emergency DepartmentsEmergency DepartmentsGeneral Hospital Units after admissionGeneral Hospital Units after admissionCommunity mental health agenciesCommunity mental health agenciesPrivate mental health practicesPrivate mental health practicesMental Health Inpatient UnitsMental Health Inpatient UnitsDoctor’s OfficeDoctor’s OfficeServices such as youth health services, Services such as youth health services, postnatal services, etcpostnatal services, etc
Why Focus on Suicide Prevention Why Focus on Suicide Prevention In Healthcare Settings?In Healthcare Settings?
Luoma, Martin, and Pearson (2002) Examined Luoma, Martin, and Pearson (2002) Examined rates of contact with primary care and mental rates of contact with primary care and mental health care professionals by individuals before health care professionals by individuals before they died by suicidethey died by suicide
*Results of this study showed:*Results of this study showed:-Contact with primary care providers in time -Contact with primary care providers in time leading up to suicide is commonleading up to suicide is common
-3 out of 4 suicide victims had contact with -3 out of 4 suicide victims had contact with their primary care providers within the year of their primary care providers within the year of suicidesuicide
Why Focus on Healthcare Why Focus on Healthcare Settings? (cont.)Settings? (cont.)
-1/3 of the suicide victims had contact -1/3 of the suicide victims had contact with mental health serviceswith mental health services
-1 in 5 suicide victims had contact with -1 in 5 suicide victims had contact with mental health services within a mental health services within a month before their suicidemonth before their suicide
-Older adults had higher rates of -Older adults had higher rates of contact with primary care providers contact with primary care providers within 1 month of suicide than within 1 month of suicide than younger adultsyounger adults
Luoma, Martin, and Pearson, Am. J Psychiatry 159:6 June 2002Luoma, Martin, and Pearson, Am. J Psychiatry 159:6 June 2002
Additional Stats Additional Stats
Physicians detect only 1 of 6 patients who Physicians detect only 1 of 6 patients who later go on to commit suicide (Blumenthal, later go on to commit suicide (Blumenthal, 1990)1990)
More than 80% of patients experiencing a More than 80% of patients experiencing a first psychiatric crisis seek medical rather first psychiatric crisis seek medical rather than psychiatric treatment (Blumental, than psychiatric treatment (Blumental, 1990)1990)
Healthcare StaffHealthcare Staff
Have a long and close contact with the Have a long and close contact with the community and are well accepted by local community and are well accepted by local peoplepeopleProvide the vital link between the community Provide the vital link between the community and healthcare systemand healthcare systemKnowledge of the community enables them to Knowledge of the community enables them to gather support from family, friends, and gather support from family, friends, and organizationsorganizationsIn position to provide continuity of careIn position to provide continuity of careEntry point to health services for those in Entry point to health services for those in distressdistressAvailable, accessible, knowledgeable, and Available, accessible, knowledgeable, and committed to providing carecommitted to providing careSource: World Health Organization 2000Source: World Health Organization 2000
Surgeon General’s Call To Action Surgeon General’s Call To Action 19991999
Intervention: Enhance services and Intervention: Enhance services and programs, both population-based and programs, both population-based and clinical careclinical careImprove the ability of primary care Improve the ability of primary care providers to recognize and treat providers to recognize and treat depression, substance abuse, and other depression, substance abuse, and other major mental illnesses associated with major mental illnesses associated with suicide risk. Increase the referral to suicide risk. Increase the referral to specialty care when appropriatespecialty care when appropriate
Understanding Components of Understanding Components of Suicidal ActSuicidal Act
The common cause: The common cause: – unendurable psychological stressors unendurable psychological stressors
The stressors leading to the suicide act: The stressors leading to the suicide act: – related to the frustrated psychological needs related to the frustrated psychological needs
of the personof the person
The purpose: The purpose: – to find a solution to problemsto find a solution to problems
(Ed Schniedman )(Ed Schniedman )
Understanding Components of Understanding Components of Suicidal ActSuicidal Act (cont.) (cont.)
The goal: The goal: – to end ‘consciousness’ and escape to end ‘consciousness’ and escape
psychological distresspsychological distress
The emotion: The emotion: – hopelessness-helplessnesshopelessness-helplessness
The action: The action: – aimed at finding a ‘way out’ or escapeaimed at finding a ‘way out’ or escape
(Ed Schniedman cont)(Ed Schniedman cont)
Suicide and Mental IllnessSuicide and Mental Illness
Epidemiologist Eve K. Moscicki remarked, Epidemiologist Eve K. Moscicki remarked, “A psychiatric disorder is a necessary “A psychiatric disorder is a necessary condition for suicide to occur”.condition for suicide to occur”.
However, the presence of a psychiatric However, the presence of a psychiatric disorder is not sufficient cause.disorder is not sufficient cause.
Mental IllnessMental Illness
The majority of people who The majority of people who commit suicide have a commit suicide have a diagnosable mental disorderdiagnosable mental disorder
Suicide and suicidal behaviors Suicide and suicidal behaviors are more frequent in are more frequent in psychiatric patients.psychiatric patients.World Health Organization 2000World Health Organization 2000
Mental Disorders That Increase Mental Disorders That Increase Suicide RiskSuicide Risk
All forms of depressionAll forms of depressionPersonality disorder (antisocial and Personality disorder (antisocial and borderline personality with traits of borderline personality with traits of impulsivity, aggression and frequent mood impulsivity, aggression and frequent mood changes)changes)SchizophreniaSchizophreniaAlcohol AbuseAlcohol AbuseOrganic mental disorderOrganic mental disorderOther mental disordersOther mental disorders
Most CommonMost Common
The most common psychiatric disorders associated with completed suicide are major depression and alcohol abuse.
DepressionDepression
Symptoms include:Symptoms include:
– Feeling sad during most of the day, every dayFeeling sad during most of the day, every day
– Losing interest in usual activitiesLosing interest in usual activities
– Losing weight (when not dieting) or gaining weightLosing weight (when not dieting) or gaining weight
– Sleeping too much or too little or waking too earlySleeping too much or too little or waking too early
– Feeling tired and weak all the timeFeeling tired and weak all the time
Depression (cont.)Depression (cont.)
– Feeling worthless, guilty or hopelessFeeling worthless, guilty or hopeless
– Feeling irritable and restless all the timeFeeling irritable and restless all the time
– Having difficulty in concentrating, making decisions or Having difficulty in concentrating, making decisions or
remembering thingsremembering things
– Having repeated thoughts of death and suicideHaving repeated thoughts of death and suicide
Adapted from World Health Organization 2000Adapted from World Health Organization 2000
Why is Depression MissedWhy is Depression Missed
Variety of treatments are available for Variety of treatments are available for depression, there are several reasons why depression, there are several reasons why this illness is often not diagnosedthis illness is often not diagnosed– People are embarrassed, consider it a sign of People are embarrassed, consider it a sign of
weaknessweakness– People are not familiar with symptoms and do People are not familiar with symptoms and do
not recognize itnot recognize it– People have another physical illness which People have another physical illness which
makes it difficult to detect the depressionmakes it difficult to detect the depression– Patients with depression may present with a Patients with depression may present with a
wide variety of aches and painswide variety of aches and painsAdapted from World Health Organization 2000Adapted from World Health Organization 2000
Depression in Primary CareDepression in Primary Care
5 to 9 percent of adult patients in primary 5 to 9 percent of adult patients in primary care settings have depressioncare settings have depression
50 percent of those go undiagnosed & 50 percent of those go undiagnosed & untreateduntreated
Women, family history of depression, Women, family history of depression, unemployed, chronic diseased, are among unemployed, chronic diseased, are among those at increased risk for depressionthose at increased risk for depression
U.S. Preventive Services Task Force Press Release May 20, 2002U.S. Preventive Services Task Force Press Release May 20, 2002
Screening for DepressionScreening for Depression
Formal screening makes it easier to detect Formal screening makes it easier to detect depressiondepression
If screening, have systems in place to If screening, have systems in place to assure accurate diagnosis, effective assure accurate diagnosis, effective treatment, and follow-uptreatment, and follow-upU.S. Preventive Services Task Force Press Release May 20, 2002U.S. Preventive Services Task Force Press Release May 20, 2002
Screening for DepressionScreening for Depression
Many tools available to screen for depressionMany tools available to screen for depressionLittle evidence to recommend one over the otherLittle evidence to recommend one over the other““Our panel found that asking two simple Our panel found that asking two simple questions – over the past 2 weeks, have you questions – over the past 2 weeks, have you ever felt down, depressed, or hopeless, and ever felt down, depressed, or hopeless, and have you felt little interest or pleasure in doing have you felt little interest or pleasure in doing things-may be as effective as using longer things-may be as effective as using longer screening instruments”. screening instruments”. U.S. Preventive Services Task Force Chairman Dr. Alfred Berg, Chair U.S. Preventive Services Task Force Chairman Dr. Alfred Berg, Chair
of the Department of Family Medicine, University of Washington, Seattle.of the Department of Family Medicine, University of Washington, Seattle.
Affirmative response to the two questions may Affirmative response to the two questions may indicate need for more in-depth diagnostic toolsindicate need for more in-depth diagnostic tools
Children’s DepressionChildren’s Depression2% of children and 4.5% of adolescents in 2% of children and 4.5% of adolescents in primary care settings have depressionprimary care settings have depression
Insufficient evidence to recommend for or Insufficient evidence to recommend for or against screening for children or against screening for children or adolescentsadolescents
Screen children and adolescents for Screen children and adolescents for suicidalitysuicidality
Parents were relieved that a clinician was Parents were relieved that a clinician was delving into a topic that they feared delving into a topic that they feared discussing with their childrendiscussing with their children
More details are in “Detecting suicide risk in a pediatric emergency department: Development of a brief More details are in “Detecting suicide risk in a pediatric emergency department: Development of a brief screening tool, “ by Dr. Horowitz, Phillip S. Wang, M.D., Dr. P.H. Gerald P. Koocher, Ph.D, and screening tool, “ by Dr. Horowitz, Phillip S. Wang, M.D., Dr. P.H. Gerald P. Koocher, Ph.D, and others, in the May 2001 Pediatrics 107 (5), pp. 1133-1137others, in the May 2001 Pediatrics 107 (5), pp. 1133-1137
SchizophreniaSchizophrenia
Adults with Schizophrenia have increased risk of suicide:Adults with Schizophrenia have increased risk of suicide: Young, Single, Unemployed MalesYoung, Single, Unemployed Males In the early stage of illnessIn the early stage of illness DepressedDepressed Prone to frequent relapsesProne to frequent relapses Highly educatedHighly educated ParanoidParanoid
10% of people with schizophrenia commit suicide10% of people with schizophrenia commit suicide
SchizophreniaSchizophrenia
People with Schizophrenia are most at risk…People with Schizophrenia are most at risk… in the early stages of illness, when confused and/or in the early stages of illness, when confused and/or
perplexedperplexed early in recovery, when outwardly their symptoms are early in recovery, when outwardly their symptoms are
better but internally they feel vulnerablebetter but internally they feel vulnerable early in relapse, when they feel they have overcome the early in relapse, when they feel they have overcome the
problem, but the symptoms recurproblem, but the symptoms recur soon after discharge from hospitalsoon after discharge from hospital
Adapted from World Health Organization 2000Adapted from World Health Organization 2000
Implications for Health ServicesImplications for Health Services
Mental health clients are 10X more at risk of suicide than Mental health clients are 10X more at risk of suicide than the general populationthe general population
Mental health clients are 100X more at risk of suicide at Mental health clients are 100X more at risk of suicide at the time of discharge from inpatient carethe time of discharge from inpatient care
-Mixed level of precaution and supervision-Mixed level of precaution and supervision-Perceived loss in level of support-Perceived loss in level of support-Possible relapse due to exposure of home -Possible relapse due to exposure of home
circumstancescircumstances-May not be fully recovered-May not be fully recovered-Non adherence to treatment regimes-Non adherence to treatment regimes-Stigma?-Stigma?
Centre for Mental Health, NSW Health Department 1999Centre for Mental Health, NSW Health Department 1999
Alcoholism/Substance Abuse and Alcoholism/Substance Abuse and DepressionDepression
Alcoholism in adultsAlcoholism in adults
Substance abuse in adolescentsSubstance abuse in adolescents
Alcoholism/substance abuse coupled with Alcoholism/substance abuse coupled with a mood disorder dramatically increases a mood disorder dramatically increases the riskthe risk
Adapted from N. Gregory Hamilton, MDAdapted from N. Gregory Hamilton, MD
Vol 108/No 6/November 2000/PostGraduate MedicineVol 108/No 6/November 2000/PostGraduate Medicine
AlcoholismAlcoholism
One third of persons completing suicide were dependent on alcohol
5-10% of people who are dependent on alcohol end their life by suicide
At time of suicidal act many are under the influence of alcohol
Characteristics of the Person with Alcohol Characteristics of the Person with Alcohol Problems who SuicidesProblems who Suicides
Started drinking at young ageStarted drinking at young age
Consumed alcohol over long period of timeConsumed alcohol over long period of time
Drank heavilyDrank heavily
Poor physical healthPoor physical health
DepressedDepressed
Disturbed and chaotic livesDisturbed and chaotic lives
Recent interpersonal lossRecent interpersonal loss
Performed poorly at workPerformed poorly at work
Family history of alcoholismFamily history of alcoholismAdapted from World Health Organization 2000Adapted from World Health Organization 2000
Physical Illnesses Associated with Physical Illnesses Associated with Suicide Suicide
Central Nervous System Gastrointestinal SystemMultiple sclerosis Peptic ulcerEpilepsyTemporal lobe epilepsySpinal cord injuryDelirium Tremens Genitourinary SystemHuningtons Disease Renal failure on dialysis
Autoimmune Disorders CancerRheumatoid arthritis Maxillofacial (head and neck)Systematic lupus erythematosus (SLE) GastrointestinalDiabetes mellitus PulmonaryCushing's disease
Adapted from Comprehensive Textbook of Suicidology 2002Adapted from Comprehensive Textbook of Suicidology 2002
Medical ConditionsMedical Conditions
Be cognizant of patients’ perception of their chronic or debilitating physical illness, increased suicide risk, and suicidal behaviors
Carefully explore other risk factors and protective factors
Create treatment plan that includes risk management protocol
General Screening Guidelines General Screening Guidelines When Patient Presents With When Patient Presents With
Suicidal IdeationsSuicidal Ideations
1.1. Ask about history of substance abuse Ask about history of substance abuse and psychiatric illnessand psychiatric illness
2. Assess mood, affect, and judgment2. Assess mood, affect, and judgment
3. Look at risk factors and symptoms of 3. Look at risk factors and symptoms of suicidesuicide
4. Interview family member4. Interview family member
5. Develop treatment plan5. Develop treatment planGliatto and Raiin the march 15Gliatto and Raiin the march 15thth, 1999 issue of American Family Physician, 1999 issue of American Family Physician
General Screening Guidelines General Screening Guidelines When Patient Presents With When Patient Presents With
Suicide RiskSuicide Risk
Screen new patients using CAGE Screen new patients using CAGE questions (for substance abuse)questions (for substance abuse)
Record brief mental status exam Record brief mental status exam
Look forLook for– Evidence of depressed mood, anxiety or Evidence of depressed mood, anxiety or
substance abuse substance abuse – Recent stressors Recent stressors – Suicidal risk / warning signsSuicidal risk / warning signs
CAGE QuestionnaireCAGE Questionnaire
Alcohol Dependence is likely if the patient gives two or more positive answers to the following questions:Have you ever felt you should CUT down on your drinking?Have people ANNOYED you by criticizing your drinking?Have you ever felt bad or GUILTY about your drinking?Have you ever had a drink first think in the morning to steady your nerves or get rid of a hangover (EYE-OPENER)?
World Health Organization Guide to Mental Health in Primary CareWorld Health Organization Guide to Mental Health in Primary Care
Determining Level of SuicidalityDetermining Level of Suicidality
1. Clinical Assessment 1. Clinical Assessment a. Inquire about feelings of depression (feeling a. Inquire about feelings of depression (feeling
down/blue)down/blue)
b. Ask about length, frequency, intensity, sleep b. Ask about length, frequency, intensity, sleep interruption, concentration problems and interruption, concentration problems and appetiteappetite
c. Ask about hopelessness, pessimism, c. Ask about hopelessness, pessimism, discouragement. Is intensity of these feelings discouragement. Is intensity of these feelings so much that life does not seem worthwhile?so much that life does not seem worthwhile?
Determining Level of SuicidalityDetermining Level of Suicidality
d. Thoughts of suicide• persistence & intensity of thoughts• effort to resist thoughts• impulses to carry out thoughts• Plan
• taken any initial action (e.g. buying gun, hoarding pills)• how detailed are the plans, are lethal means available?
e. Can person manage feelings if they occur, is there a support system to help manage?
Determining Level of SuicidalityDetermining Level of Suicidality2. SAD PERSONS SCALE (Quick and Easy Assessment)2. SAD PERSONS SCALE (Quick and Easy Assessment)
SSexex 1 if patient is mail, 0 if female1 if patient is mail, 0 if femaleAAgege 1 if patient is (25-34; 35-44; 65+)1 if patient is (25-34; 35-44; 65+)DDepressionepression
PPrevious attemptrevious attempt 1 if present1 if presentEEthanol abusethanol abuse 1 if present1 if presentRRational thinking lossational thinking loss 1 if patient is psychotic for any reason 1 if patient is psychotic for any reason
(schizophrenia, affective illness, organic brain (schizophrenia, affective illness, organic brain syndrome)syndrome)
SSocial support lackingocial support lacking 1 If these are lacking, especially with recent loss of a 1 If these are lacking, especially with recent loss of a significant othersignificant other
OOrganized Planrganized Plan 1 if plan made and method lethal1 if plan made and method lethalNNo spouseo spouse 1 if divorced, widowed, separated, or single (for males)1 if divorced, widowed, separated, or single (for males)SSicknessickness 1 especially if chronic, debilitating, severe (e.g.; non-1 especially if chronic, debilitating, severe (e.g.; non-
localized cancer, epilepsy, MS, gastrointestinal localized cancer, epilepsy, MS, gastrointestinal disorders)disorders)
Patterson WM, Dohn HH, et al: Evaluation of suicidal patients, THE SAD PERSONS Scale, Psychosomatics, 1983Patterson WM, Dohn HH, et al: Evaluation of suicidal patients, THE SAD PERSONS Scale, Psychosomatics, 1983
SAD PERSON Guidelines for SAD PERSON Guidelines for ActionAction
0-20-2 Send home with follow-upSend home with follow-up
3-43-4 Close follow-upClose follow-up
5-65-6 Strongly consider hospitalization, Strongly consider hospitalization, depending on confidence in the depending on confidence in the follow-up arrangementfollow-up arrangement
7-107-10 Hospitalize or commitHospitalize or commit
Patterson WM, Dohn HH, et al: Evaluation of suicidal patients, THE SAD PERSONS Scale, Patterson WM, Dohn HH, et al: Evaluation of suicidal patients, THE SAD PERSONS Scale, Psychosomatics, 1983Psychosomatics, 1983
HospitalizationHospitalization
When do you hospitalize?When do you hospitalize? Patients with a plan, access to lethal Patients with a plan, access to lethal
means, recent social stressors and means, recent social stressors and symptoms suggestive of a psychiatric symptoms suggestive of a psychiatric disorder should be hospitalized disorder should be hospitalized immediatelyimmediately
HospitalizationHospitalization
Inform family of decision to admit and do Inform family of decision to admit and do not leave patient alone while he or she is not leave patient alone while he or she is transferred to a more secure environmenttransferred to a more secure environment
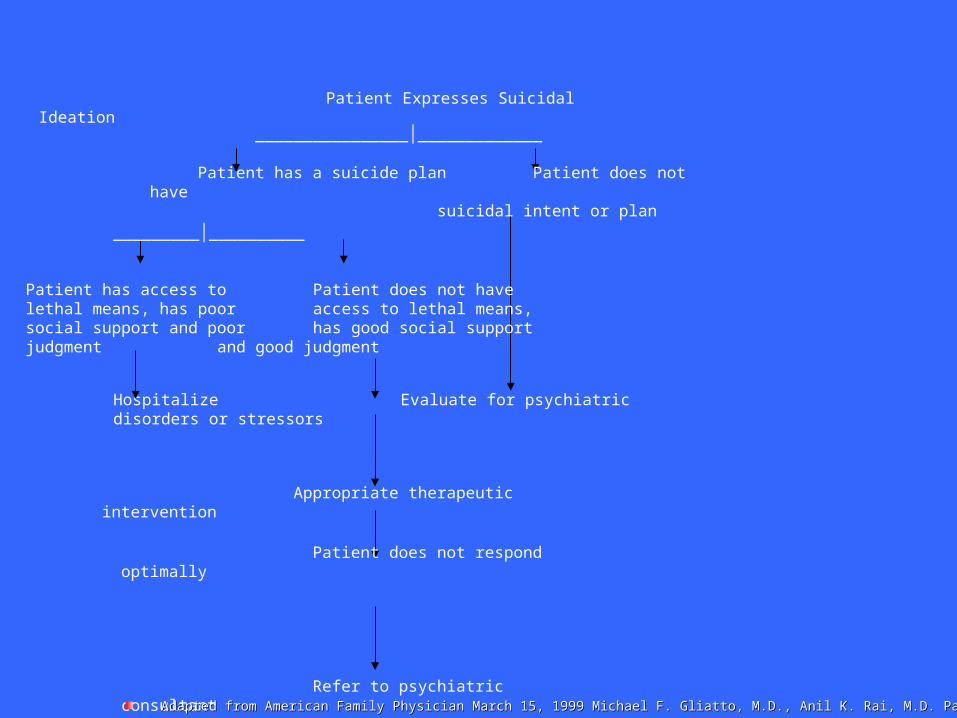
Patient Expresses Suicidal Ideation
________________│_____________
Patient has a suicide plan Patient does not have suicidal intent or plan
_________│__________
Patient has access to Patient does not havelethal means, has poor access to lethal means,social support and poor has good social supportjudgment and good judgment
Hospitalize Evaluate for psychiatric disorders or stressors
Appropriate therapeutic intervention
Patient does not respond optimally
Refer to psychiatric consultantAdapted from American Family Physician March 15, 1999 Michael F. Gliatto, M.D., Anil K. Rai, M.D. Page 6Adapted from American Family Physician March 15, 1999 Michael F. Gliatto, M.D., Anil K. Rai, M.D. Page 6
BryanLGH Medical Center and BryanLGH Medical Center and Lincoln/Lancaster County Crisis Lincoln/Lancaster County Crisis
CenterCenterTwo separate facilitiesTwo separate facilities
BryanLGH Medical Center Mental BryanLGH Medical Center Mental Health is not related to the Crisis Health is not related to the Crisis CenterCenter
When EPC happens individual When EPC happens individual transported to Crisis Center transported to Crisis Center unless Medical Condition requires unless Medical Condition requires Hospital TreatmentHospital Treatment
BryanLGH has 24 hour mental BryanLGH has 24 hour mental health assessment nurse health assessment nurse available in ED for those patients available in ED for those patients voluntarily seeking treatmentvoluntarily seeking treatment

Voluntary TreatmentVoluntary Treatment 83-1001 83-1001
State of Nebraska public policy declares State of Nebraska public policy declares that mentally ill dangerous persons be that mentally ill dangerous persons be encouraged to obtain voluntary treatment encouraged to obtain voluntary treatment
It is when voluntary treatment is refused It is when voluntary treatment is refused that the individual can be subjected to that the individual can be subjected to emergency protective custodyemergency protective custody
The majority of mentally ill dangerous The majority of mentally ill dangerous persons do obtain voluntary treatmentpersons do obtain voluntary treatment
Emergency Protective CustodyEmergency Protective CustodyCriteriaCriteria
Criteria 83-1009 Criteria 83-1009Mentally Ill and/or Mentally Ill and/or chemically dependentchemically dependent
Danger to self or Danger to self or othersothers
Inability to care for Inability to care for selfself
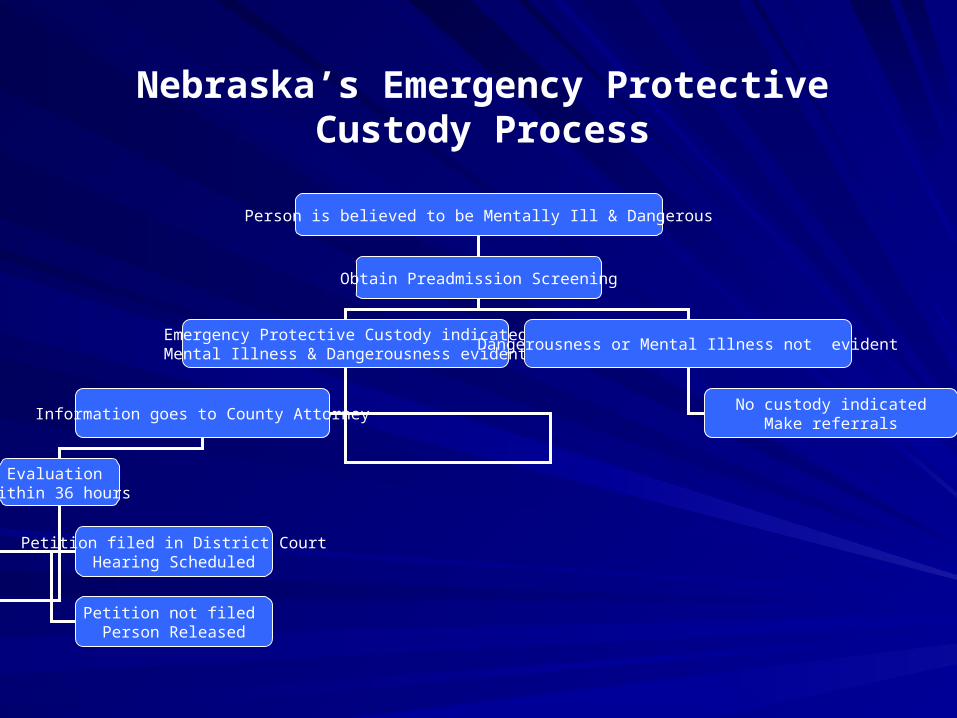
Person is believed to be Mentally Ill & Dangerous
Obtain Preadmission Screening
Emergency Protective Custody indicatedMental Illness & Dangerousness evident
Information goes to County Attorney
Evaluation within 36 hours
Dangerousness or Mental Illness not evident
No custody indicatedMake referrals
Petition filed in District CourtHearing Scheduled
Petition not filed Person Released
Nebraska’s Emergency Protective Custody Process
EPC ProcessEPC Process
Law enforcement Law enforcement initiatesinitiates
M.D. or LMHP have M.D. or LMHP have option to complete option to complete form that provides form that provides more information for more information for law enforcement about law enforcement about the individual and will the individual and will most likely need to most likely need to testify at the BMH testify at the BMH hearinghearing
EPC Process ContinuedEPC Process Continued
Patient needs to be evaluated within 36 hours by a Patient needs to be evaluated within 36 hours by a psychiatrist or psychologistpsychiatrist or psychologistEvaluation and recommendations are submitted to Evaluation and recommendations are submitted to County Attorney to determine whether or not to file the County Attorney to determine whether or not to file the papers for a Board of Mental Health Hearingpapers for a Board of Mental Health HearingCounty Attorney Timelines: County Attorney Timelines: – If deemed committable – intent to file must be given and hearing If deemed committable – intent to file must be given and hearing
scheduled with 7 days of the date of the EPCscheduled with 7 days of the date of the EPC– If deemed NOT committable – County Attorney must decide If deemed NOT committable – County Attorney must decide
within 24 hours of receiving the information whether to file within 24 hours of receiving the information whether to file petition petition
Mental Health Board hearing will be held to determine Mental Health Board hearing will be held to determine treatment needs and/or placement needs of the patienttreatment needs and/or placement needs of the patient
EPC Process ContinuedEPC Process Continued
Physicians who would like to drop EPC will Physicians who would like to drop EPC will need to submit a recommendation to the need to submit a recommendation to the County AttorneyCounty Attorney
County Attorney will make a decision County Attorney will make a decision whether or not to drop EPC or file papers whether or not to drop EPC or file papers for Board of Mental Healthfor Board of Mental Health
EPC Process for YouthEPC Process for Youth(LAST RESORT)(LAST RESORT)
Same criteria (mentally ill/dangerous) Same criteria (mentally ill/dangerous) Physical assessment needed prior to placement Physical assessment needed prior to placement EPC youth are placed at BryanLGH Medical EPC youth are placed at BryanLGH Medical Center West or the Lincoln Regional Center Center West or the Lincoln Regional Center (LRC)(LRC)BryanLGH Medical Center and LRC BryanLGH Medical Center and LRC communicate daily regarding bed availability and communicate daily regarding bed availability and will decide the most appropriate placement for will decide the most appropriate placement for the youththe youth
Alternative to Youth EPCAlternative to Youth EPC
A responsible adult may authorize A responsible adult may authorize admission for treatment without initiating admission for treatment without initiating EPC processEPC process
Temporary Immediate Custody may be Temporary Immediate Custody may be initiated by Law Enforcement if neededinitiated by Law Enforcement if needed

Survivor IssuesSurvivor Issues
Normalize expression of feelings such as shock, Normalize expression of feelings such as shock, fear, sadness, guilt, anger at others or at the fear, sadness, guilt, anger at others or at the victim – Assure feelings will become less intense victim – Assure feelings will become less intense after talking, counselingafter talking, counseling
Assure no right way to feel after a suicide-Each Assure no right way to feel after a suicide-Each person will need to go through individual griefperson will need to go through individual grief
Clarify the factsClarify the facts
Acknowledge “why” questions-Victims choice-Acknowledge “why” questions-Victims choice-Only victim knows “why”Only victim knows “why”
Optional SlidesOptional Slides
Lancaster County Crisis CenterLancaster County Crisis Center
Once EPC’d adult individuals may be Once EPC’d adult individuals may be taken to the Crisis Center operated by taken to the Crisis Center operated by Lancaster CountyLancaster CountyWhile at Crisis Center individual will be While at Crisis Center individual will be preparing for Board of Mental Health preparing for Board of Mental Health hearinghearingPlease call the Crisis Center prior to Please call the Crisis Center prior to leavingleaving
Lancaster County Crisis Center Lancaster County Crisis Center ContinuedContinued
Once making call to Crisis Center they will:Once making call to Crisis Center they will:
-Be able to inform you of bed availability-Be able to inform you of bed availability
-If bed is available:-If bed is available:
-Individual needs to be medically stable (No IV’s, -Individual needs to be medically stable (No IV’s, and O2)and O2)
Individual needs to be mobileIndividual needs to be mobile
Only staffed with 1 RN for 15 bedsOnly staffed with 1 RN for 15 beds
Lancaster County Crisis Center Lancaster County Crisis Center ContinuedContinued
If beds are full at Crisis If beds are full at Crisis Center the next alternative Center the next alternative would be BryanLGH would be BryanLGH Medical Center WestMedical Center WestIf this happens, please call If this happens, please call the Administrative the Administrative Supervisor 475-1011 at Supervisor 475-1011 at BryanLGH Medical Center BryanLGH Medical Center West and indicate you West and indicate you have an EPC and the have an EPC and the Crisis Center is full and Crisis Center is full and inquire about bed inquire about bed availabilityavailability
EPC BryanLGH Medical CenterEPC BryanLGH Medical Center
Contact the administrative supervisor:Contact the administrative supervisor:• They will make determination on capability They will make determination on capability
and capacity to receive patientand capacity to receive patient• If able to receive patient, they will If able to receive patient, they will
coordinate receiving patient through the coordinate receiving patient through the Emergency Department or as a direct Emergency Department or as a direct admit to unit/physicianadmit to unit/physician
EPC Process ContinuedEPC Process Continued
If medically unstable If medically unstable (OD, intoxication BAC (OD, intoxication BAC > 200) :> 200) :
Individual will need to Individual will need to be admitted to be admitted to BryanLGH Medical BryanLGH Medical Center West and not Center West and not Crisis Center Crisis Center
EPC Process ContinuedEPC Process Continued
If BAC is < 200:If BAC is < 200:
Patient will need to be stable for transfer Patient will need to be stable for transfer prior to leaving hospitalprior to leaving hospital
EPC DocumentationEPC Documentation(83-1021)(83-1021)
– Observed Behavior of Observed Behavior of subjectsubject
– Witness description of Witness description of subject’s behaviorsubject’s behavior
– Environmental Description Environmental Description Historical InformationHistorical Information
What do you see?
What do you hear?
Trust your intuition….
EPC CERTIFICATES
EPC DocumentationEPC Documentation
What the County Attorney and Mental What the County Attorney and Mental Health Professionals Need to know . . . Health Professionals Need to know . . . – Current InformationCurrent Information
risk factors and behaviorsrisk factors and behaviorsCurrent mental health diagnosis / treatmentCurrent mental health diagnosis / treatmentCurrent medical factorsCurrent medical factors
– Historical InformationHistorical Information Including information about past behavior is Including information about past behavior is appropriateappropriate
– Mental Health history; contacts with law enforcement; Mental Health history; contacts with law enforcement; incidents of violence or crisisincidents of violence or crisis
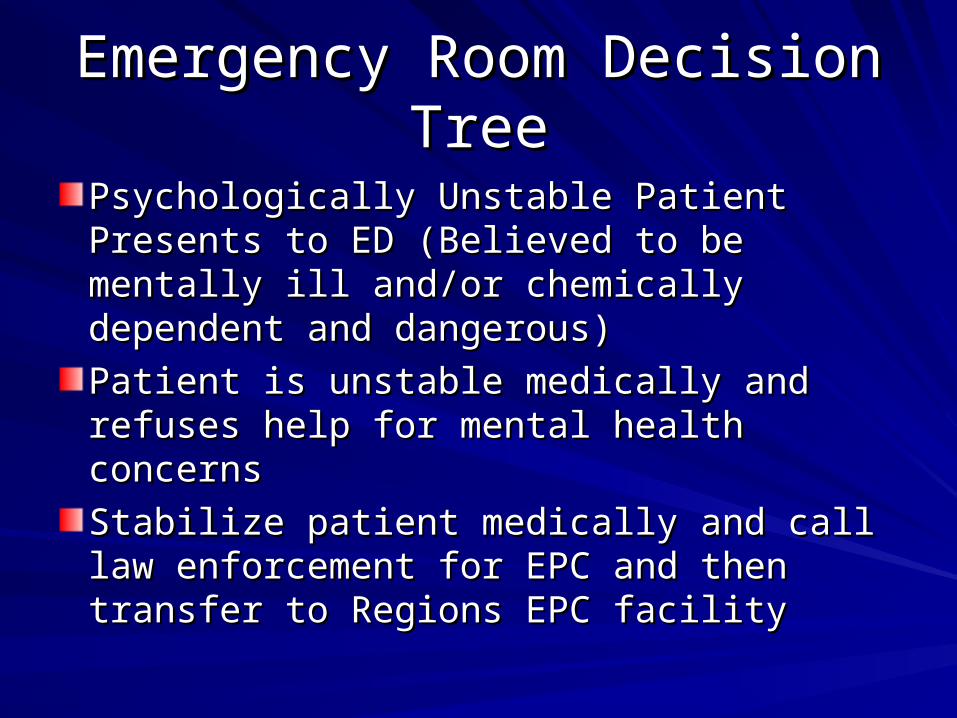
Emergency Room Decision Emergency Room Decision TreeTree
Psychologically Unstable Patient Presents Psychologically Unstable Patient Presents to ED (Believed to be mentally ill and/or to ED (Believed to be mentally ill and/or chemically dependent and dangerous)chemically dependent and dangerous)
Patient is unstable medically and refuses Patient is unstable medically and refuses help for mental health concernshelp for mental health concerns
Stabilize patient medically and call law Stabilize patient medically and call law enforcement for EPC and then transfer to enforcement for EPC and then transfer to Regions EPC facilityRegions EPC facility
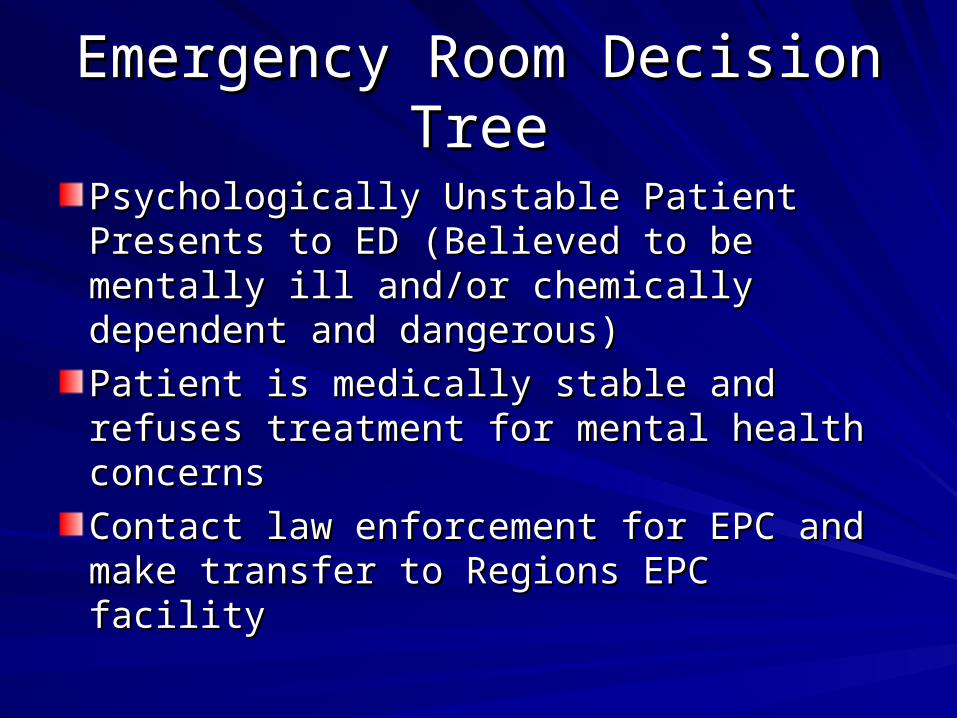
Emergency Room Decision Emergency Room Decision TreeTree
Psychologically Unstable Patient Presents Psychologically Unstable Patient Presents to ED (Believed to be mentally ill and/or to ED (Believed to be mentally ill and/or chemically dependent and dangerous)chemically dependent and dangerous)
Patient is medically stable and refuses Patient is medically stable and refuses treatment for mental health concernstreatment for mental health concerns
Contact law enforcement for EPC and Contact law enforcement for EPC and make transfer to Regions EPC facilitymake transfer to Regions EPC facility
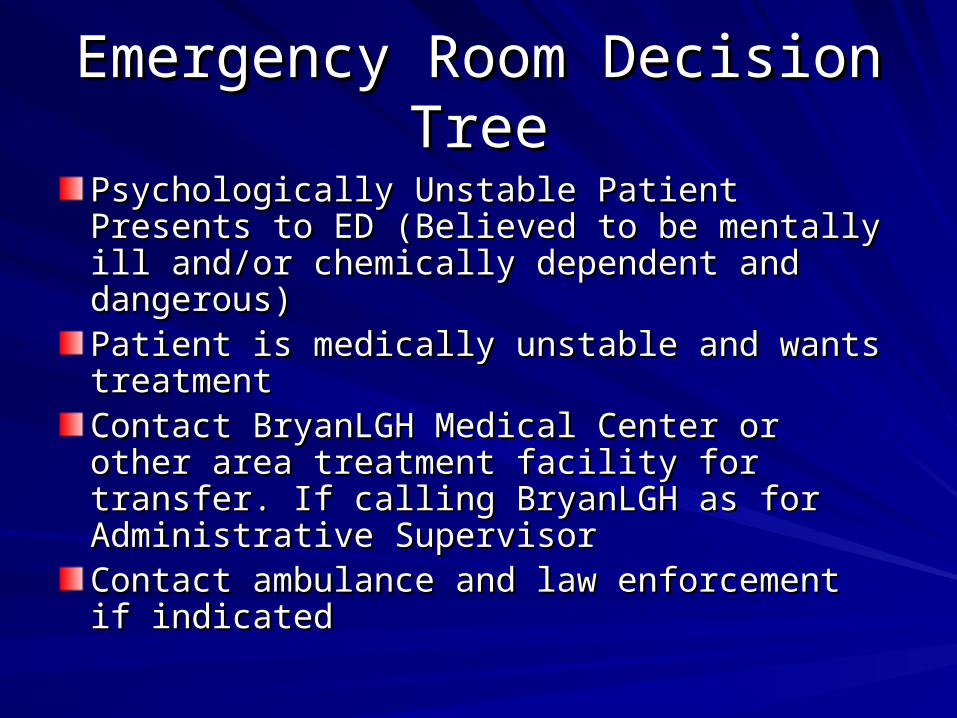
Emergency Room Decision Emergency Room Decision TreeTree
Psychologically Unstable Patient Presents to ED Psychologically Unstable Patient Presents to ED (Believed to be mentally ill and/or chemically (Believed to be mentally ill and/or chemically dependent and dangerous)dependent and dangerous)Patient is medically unstable and wants Patient is medically unstable and wants treatmenttreatmentContact BryanLGH Medical Center or other area Contact BryanLGH Medical Center or other area treatment facility for transfer. If calling BryanLGH treatment facility for transfer. If calling BryanLGH as for Administrative Supervisor as for Administrative Supervisor Contact ambulance and law enforcement if Contact ambulance and law enforcement if indicatedindicated
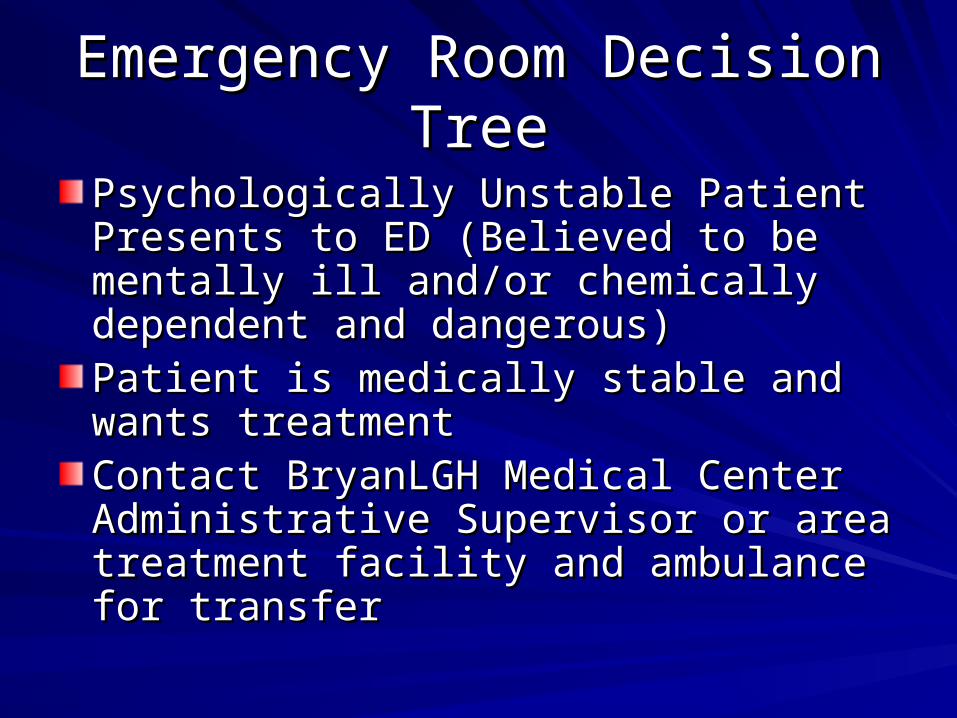
Emergency Room Decision Emergency Room Decision TreeTree
Psychologically Unstable Patient Presents Psychologically Unstable Patient Presents to ED (Believed to be mentally ill and/or to ED (Believed to be mentally ill and/or chemically dependent and dangerous)chemically dependent and dangerous)Patient is medically stable and wants Patient is medically stable and wants treatmenttreatmentContact BryanLGH Medical Center Contact BryanLGH Medical Center Administrative Supervisor or area Administrative Supervisor or area treatment facility and ambulance for treatment facility and ambulance for transfertransfer
Admission Criteria for EPC Admission Criteria for EPC FacilitiesFacilities
Identify the EPC facility in your areaIdentify the EPC facility in your area Know their admission criteria Know their admission criteria
1.1. Medical StabilityMedical Stability1.1. IntoxicationIntoxication2.2. Invasive procedures needed (IV’s? Feeding tubes?)Invasive procedures needed (IV’s? Feeding tubes?)3.3. AmbulatoryAmbulatory
2.2. Criminal Charges Criminal Charges 1.1. Degree of violence / Seriousness of chargesDegree of violence / Seriousness of charges2.2. Transfers from jailTransfers from jail
3.3. AgeAge1.1. Juvenile vs. AdultJuvenile vs. Adult