Multicentre study to determine the Etest epidemiological ...
Upload
tyrone-powellCategory
view
217download
1
A PROSPECTIVE MULTICENTRE REGISTRY FOR THE ASSESSMENT OF SAFETY AND EFFICACY OF BIODEGRADABLE
POLYMER COATED, PACLITAXEL ELUTING STENT LUC TM*
*(BALTON, POLAND)
9 th month study
P. Buszman1,2, R. Gil3, J. Rzezniczak4, T. Przewlocki5, M. Kosmider6, J. Wojcik7, J. Janczak8, S. Trznadel2, L. Kinasz2, M. Kondys2,
M. Krol2, K. Milewski1,2
1. Silesian Medical School, Katowice
2. American Heart of Poland, Ustron
3. Central Hospital of the Ministry of Internal Affairs, Warsaw
4. Department of Cardiology, District Hospital, Poznan
5. Institute of Cardiology, CM, JU, Kraków
6. Department of Cardiology and Cardiac Surgery, Medical School, Lodz
7. Division of Cardiology, Lublin
8. Department of Cardiology, Central Military Hospital, Warsaw
LIMITATIONS OF POLYMER COATED DES’s
Although polymers can ensure predictable release of different drugs, in some cases they cause exaggerated inflammatory response, neointimal hyperplasia and thrombosis.Biodegradable polymer – drug eluting stents (BP-DES) are to resolve the problem of chronic vascular inflammation and late thrombosis.
A new concept: after the drug and polymer are eluted, only neutral stainless steel is left in the vessel wall.
CHARACTERISTIC OF LUC STENT
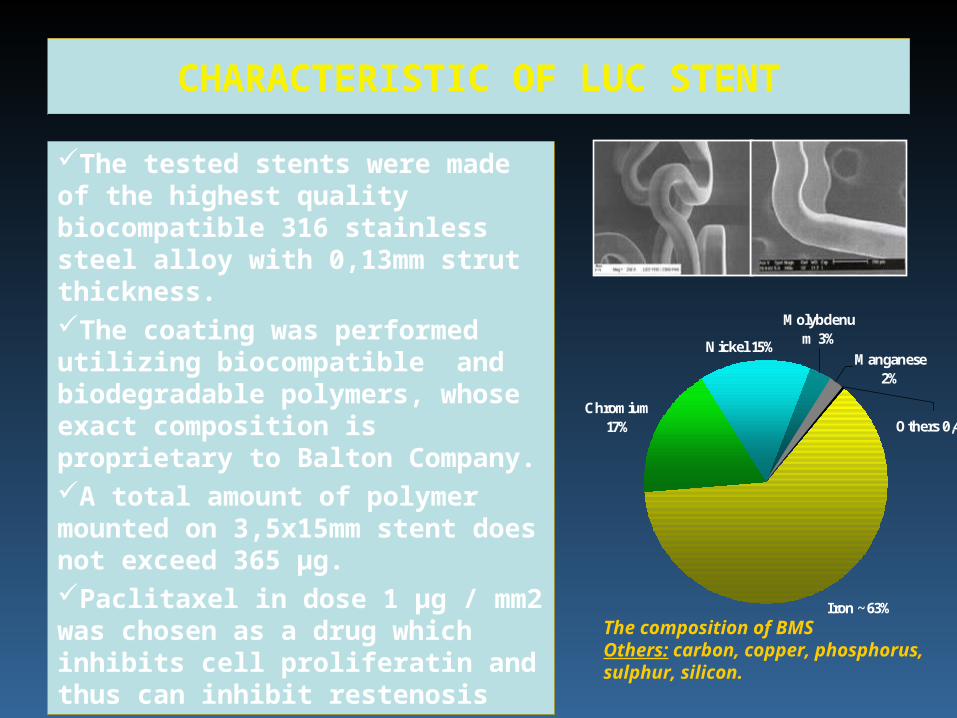
The tested stents were made of the highest quality biocompatible 316 stainless steel alloy with 0,13mm strut thickness.The coating was performed utilizing biocompatible and biodegradable polymers, whose exact composition is proprietary to Balton Company.A total amount of polymer mounted on 3,5x15mm stent does not exceed 365 µg. Paclitaxel in dose 1 μg / mm2 was chosen as a drug which inhibits cell proliferatin and thus can inhibit restenosis
Manganese 2%
Others 0,4%
Molybdenum 3%
Iron ~63%
Chromium 17%
Nickel 15%
The composition of BMSOthers: carbon, copper, phosphorus, sulphur, silicon.
BIODEGRADATION OF TESTED POLYMER
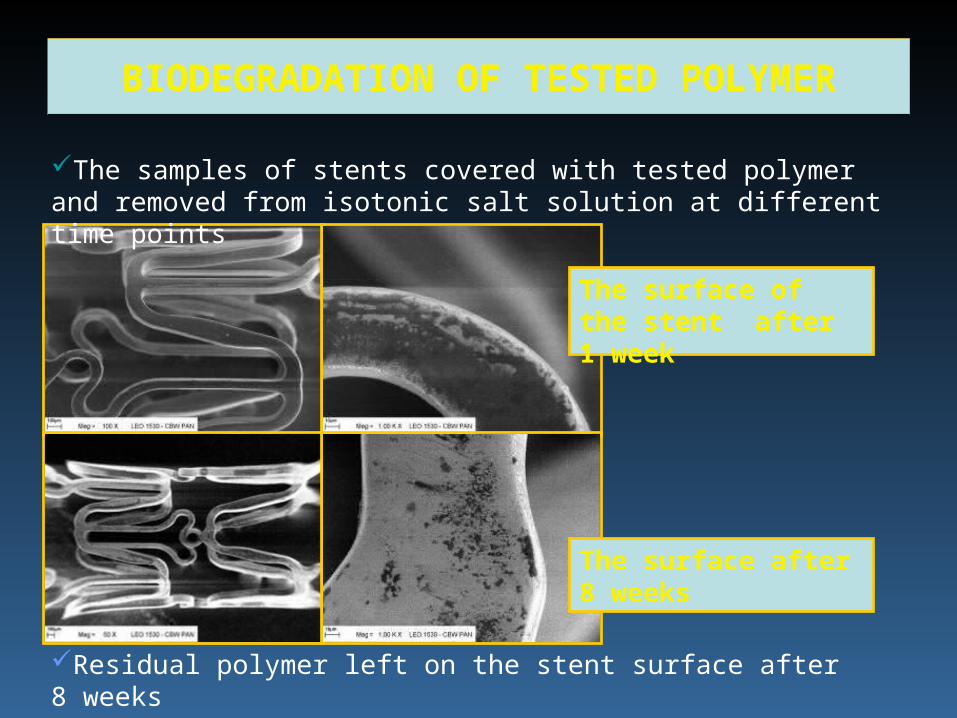
The surface of the stent after 1 week
The surface after 8 weeks
Residual polymer left on the stent surface after 8 weeks
The samples of stents covered with tested polymer and removed from isotonic salt solution at different time points
ANIMAL STUDY
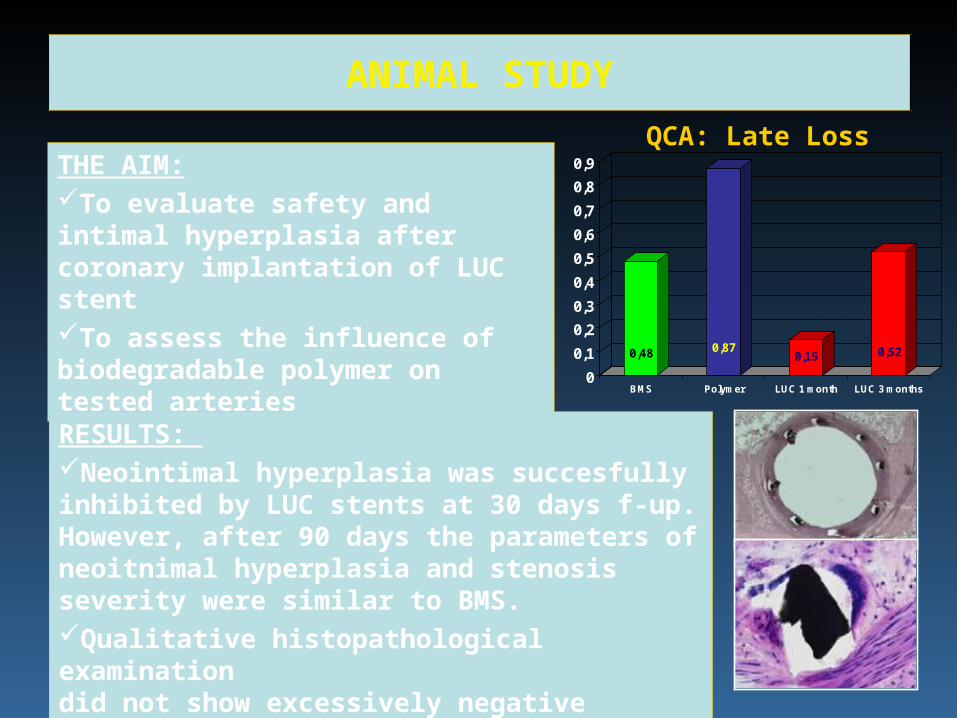
THE AIM:To evaluate safety and intimal hyperplasia after coronary implantation of LUC stentTo assess the influence of biodegradable polymer on tested arteries
RESULTS: Neointimal hyperplasia was succesfully inhibited by LUC stents at 30 days f-up. However, after 90 days the parameters of neoitnimal hyperplasia and stenosis severity were similar to BMS.Qualitative histopathological examination did not show excessively negative influence of polymer on tested artery.
0,48 0,870,15 0,52
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
BMS Polymer LUC 1 month LUC 3 months
QCA: Late Loss
FIRST IN MAN STUDY
Prospective, multi-center registry
•Warszawa
•Lodz
•Ustron
•Lublin
•Poznan
•Katowice
•KrakowBielsko
Biała
FIRST IN MAN STUDY
Silesian Medical School, Katowice P. Buszman Katowice
American Heart of Poland M. Kondys Ustron
Central Hospital of the Ministry of Internal Affairs R. Gil Warszawa
Department of Cardiology, District Hospital J. Rzezniczak Poznan
American Heart of Poland L. Kinasz Bielsko
Institute of Cardiology, CM, JU, Kraków T. Przewlocki Krakow
Department of Cardiology and Cardiac Surgery M. Kosmider Lodz
Division of Cardiology J. Wojcik Lublin
Department of Cardiology, Central Military Hospital J. Janczak Warszawa
Silesian Medical School, Katowice P. Buszman Katowice
American Heart of Poland M. Kondys Ustron
Central Hospital of the Ministry of Internal Affairs R. Gil Warszawa
Department of Cardiology, District Hospital J. Rzezniczak Poznan
American Heart of Poland L. Kinasz Bielsko
Institute of Cardiology, CM, JU, Kraków T. Przewlocki Krakow
Department of Cardiology and Cardiac Surgery M. Kosmider Lodz
Division of Cardiology J. Wojcik Lublin
Department of Cardiology, Central Military Hospital J. Janczak Warszawa
FIRST IN MAN STUDY
Principle Investigator:
Pawel Buszman, MD, FESC, FSCAI
Clinical Events Committee:
Mariusz Gasior
Ciecwierz Leszek
Angiographic Core Lab:
Core Imaging Analysis Laboratory
Krakow Cardiovascular Research Institute
FIRST IN MAN STUDY
Material and method:
Enrollment of 113 patients with:de-novo lesion in native coronary arteryvessel diameter 2.8 – 4.0 mmlesion length 18 mmstenosis ≥ 50% and ≤100% Dual antiplatelet therapy required for 9months
Period of implantation: 07/2005 – 11/2005
FIRST IN MAN STUDY
Clinical endpoints:
MACE after 30 days, 6 and 9 months
Angiographic endpoints:
Late loss
Restenosis rate
F-up visits after 30 days, then subsequently after 3 and 6 months to define MACE rate. 9-months control coronarography
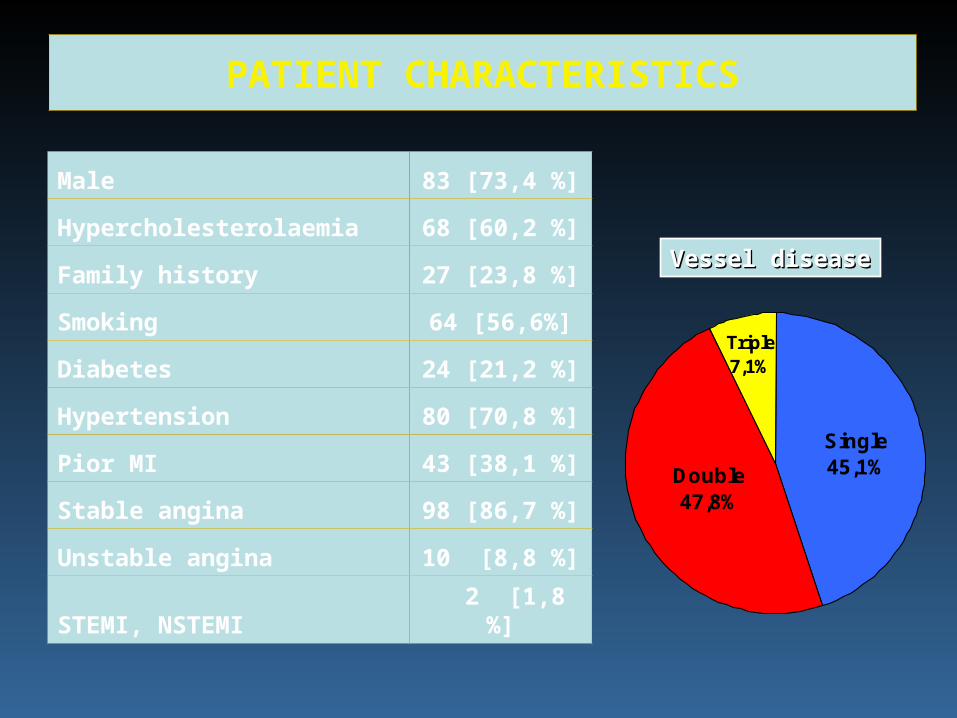
PATIENT CHARACTERISTICS
Male 83 [73,4 %]
Hypercholesterolaemia 68 [60,2 %]
Family history 27 [23,8 %]
Smoking 64 [56,6%]
Diabetes 24 [21,2 %]
Hypertension 80 [70,8 %]
Pior MI 43 [38,1 %]
Stable angina 98 [86,7 %]
Unstable angina 10 [8,8 %]
STEMI, NSTEMI 2 [1,8 %]
Vessel diseaseVessel disease
Single45,1%
Triple7,1%
Double47,8%
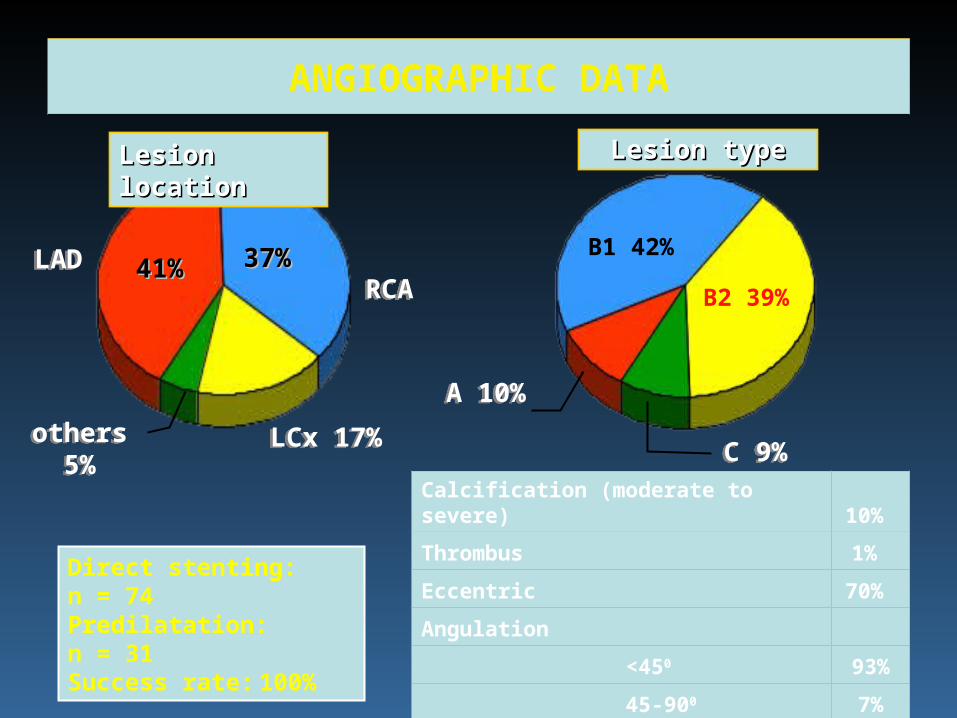
ANGIOGRAPHIC DATA
LADLADRCARCA
3737%%4411%%
LCx 17%LCx 17%others 5%others 5%
Lesion typeLesion type
C 9%C 9%
B2 39%
A 10%A 10%
Direct stenting: n = 74Predilatation: n = 31Success rate: 100%
B1 42%
Calcification (moderate to severe) 10%
Thrombus 1%
Eccentric 70%
Angulation
<450 93%
45-900 7%
Lesion locationLesion location
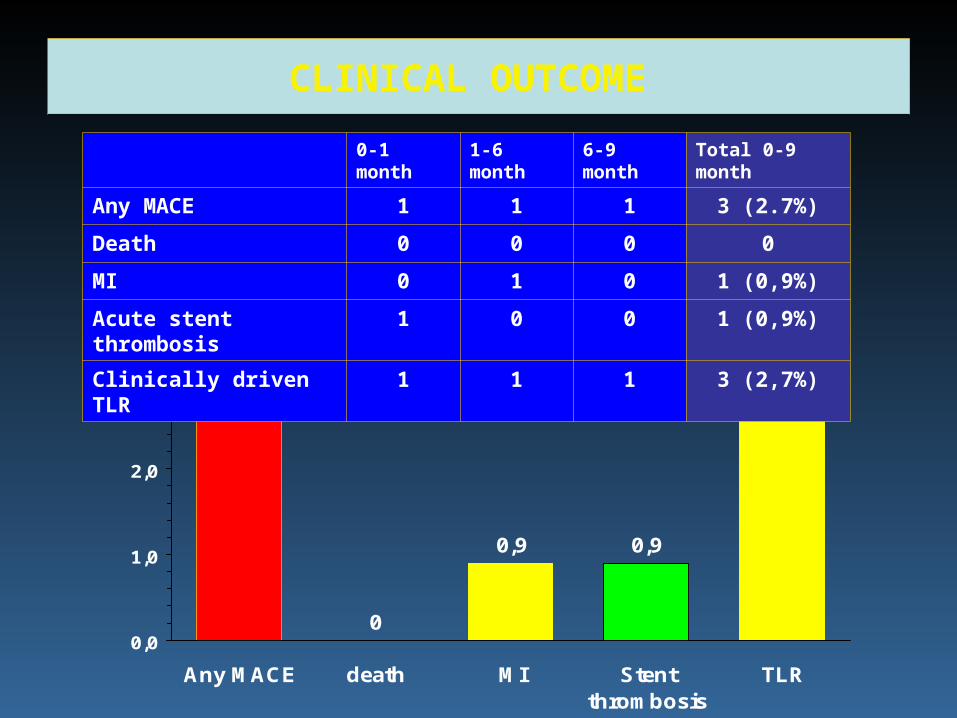
CLINICAL OUTCOME
0
0,9
2,7
0,9
2,7
0,0
1,0
2,0
3,0
Any MACE death MI Stentthrombosis
TLR
0-1 month 1-6 month 6-9 month Total 0-9 month
Any MACE 1 1 1 3 (2.7%)
Death 0 0 0 0
MI 0 1 0 1 (0,9%)
Acute stent thrombosis 1 0 0 1 (0,9%)
Clinically driven TLR 1 1 1 3 (2,7%)
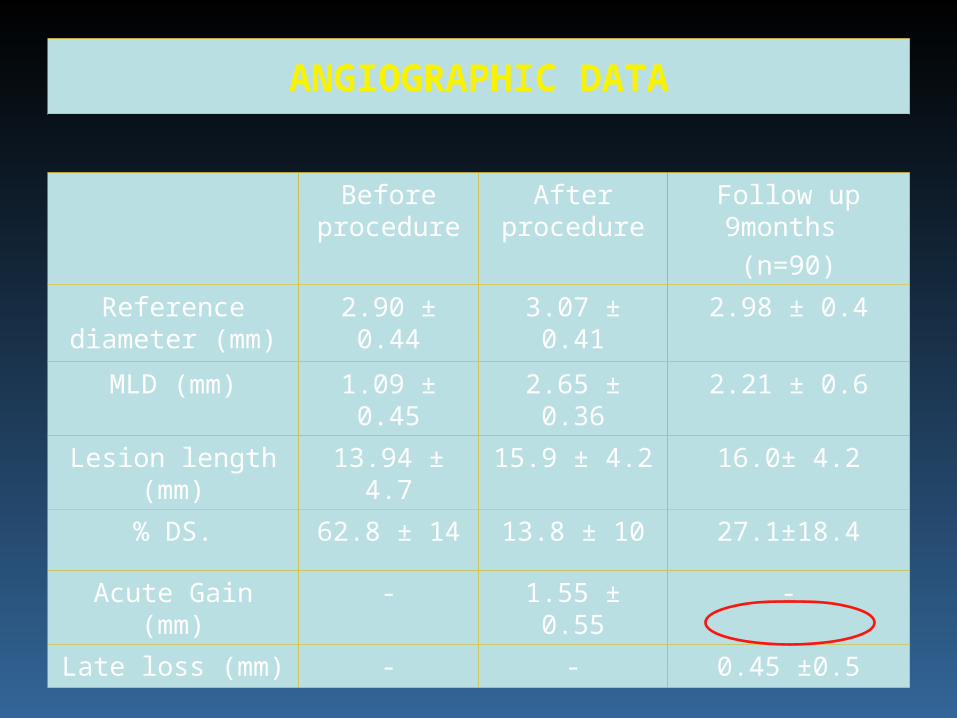
ANGIOGRAPHIC DATA
Before procedure
After procedure
Follow up 9months
(n=90)
Reference diameter (mm)
2.90 ± 0.44 3.07 ± 0.41 2.98 ± 0.4
MLD (mm) 1.09 ± 0.45 2.65 ± 0.36 2.21 ± 0.6
Lesion length (mm) 13.94 ± 4.7 15.9 ± 4.2 16.0± 4.2
% DS. 62.8 ± 14 13.8 ± 10 27.1±18.4
Acute Gain (mm) - 1.55 ± 0.55 -
Late loss (mm) - - 0.45 ±0.5
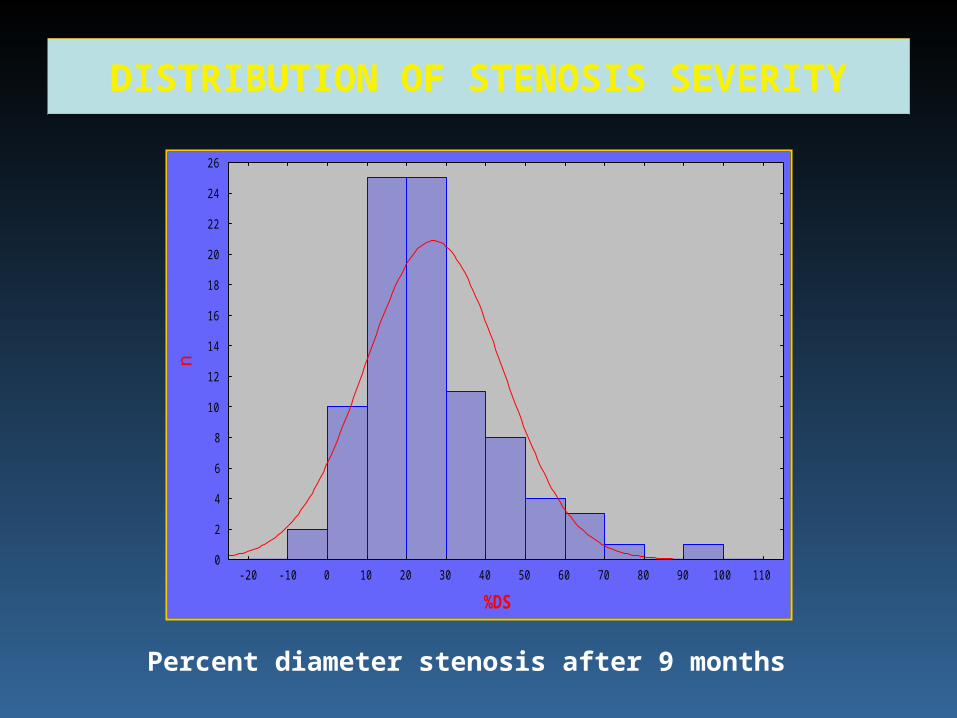
DISTRIBUTION OF STENOSIS SEVERITY
-20 -10 0 10 20 30 40 50 60 70 80 90 100 110
%DS
0
2
4
6
8
10
12
14
16
18
20
22
24
26
n
Percent diameter stenosis after 9 months
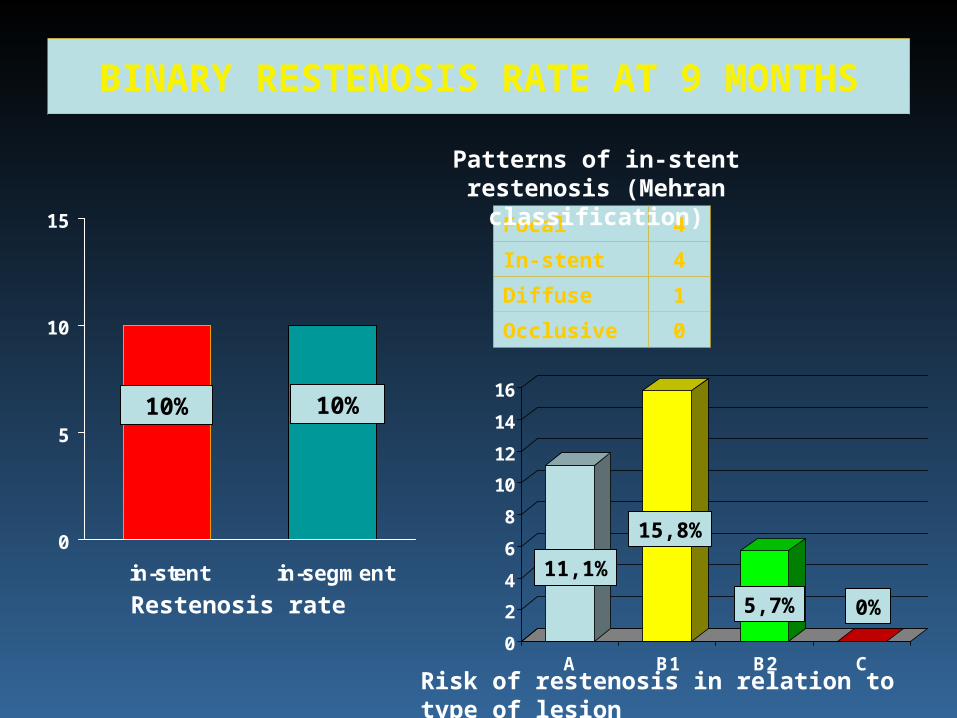
BINARY RESTENOSIS RATE AT 9 MONTHS
0
5
10
15
in-stent in-segment
10%10%
Focal 4
In-stent 4
Diffuse 1
Occlusive 0
Patterns of in-stent restenosis (Mehran classification)
0
2
4
6
8
10
12
14
16
A B1 B2 CRisk of restenosis in relation to type of lesion
11,1%
15,8%
5,7% 0%Restenosis rate
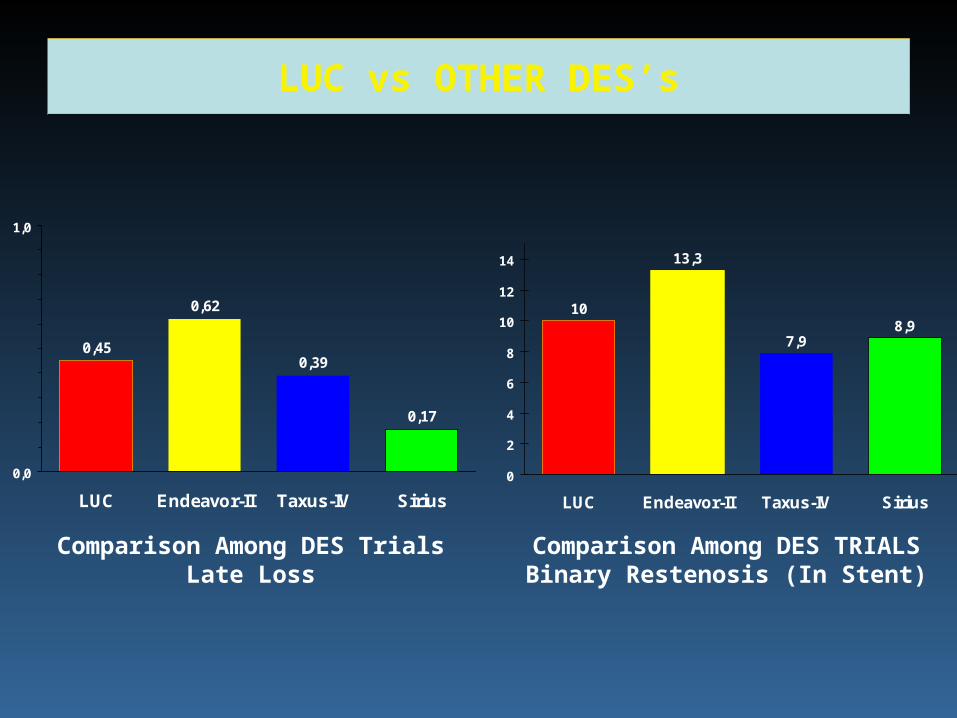
LUC vs OTHER DES’s
0,62
0,39
0,17
0,45
0,0
1,0
LUC Endeavor-II Taxus-IV Sirius
13,3
7,98,9
10
0
2
4
6
8
10
12
14
LUC Endeavor-II Taxus-IV Sirius
Comparison Among DES TrialsLate Loss
Comparison Among DES TRIALSBinary Restenosis (In Stent)
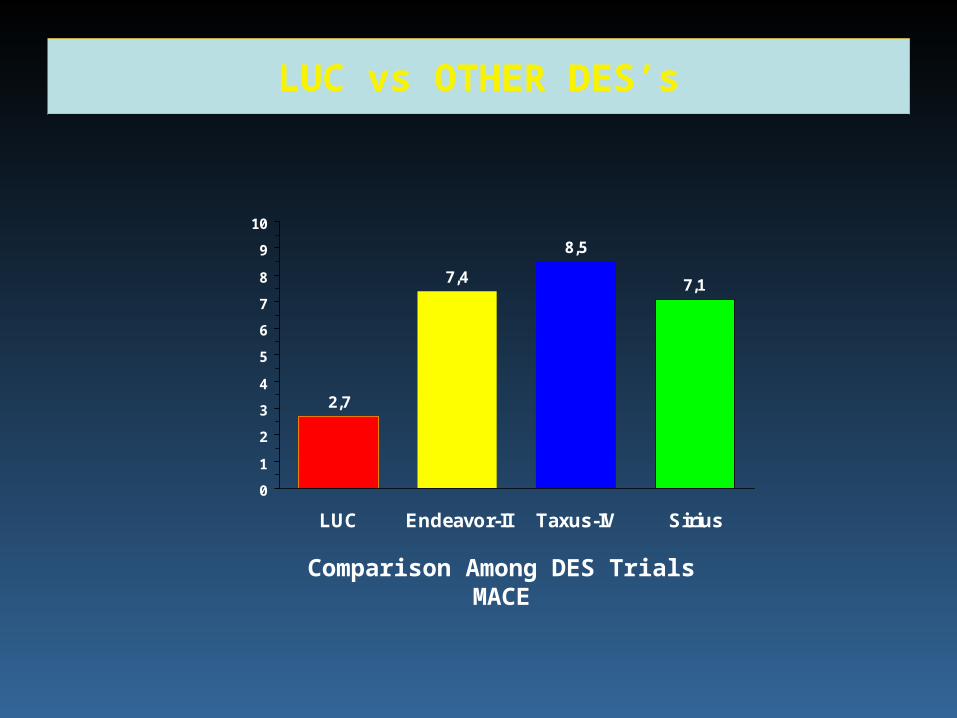
LUC vs OTHER DES’s
7,4
8,5
7,1
2,7
0
1
2
3
4
5
6
7
8
9
10
LUC Endeavor-II Taxus-IV Sirius
Comparison Among DES TrialsMACE
SUMMARY
EExcellent procedural outcomexcellent procedural outcome with with device device success 100%success 100%
Low MACE rate over 9 months after Low MACE rate over 9 months after implantation (2.7%)implantation (2.7%)
FFavorable late avorable late (9 months)(9 months) angiographic angiographic results:results:
- B- Binary restenosis 1inary restenosis 10,00,0%%
- L- Late loss 0.ate loss 0.4545 mm mm