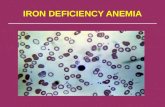
11. Iron Deficiency Anemia 2012
41
Iron Deficiency Anemia FACULTY OF MEDICINE UNIVERSITY OF BRAWIJAYA MALANG
description
Iron Deficiency Anemia
Transcript of 11. Iron Deficiency Anemia 2012

Iron Deficiency Anemia
FACULTY OF MEDICINE UNIVERSITY OF BRAWIJAYA MALANG

Faculty of Medicine University of Brawijaya
Clinical Competencies
Be able to describe: - the causes of iron deficiency anemia - the pathogenesis and pathophysiology of iron deficiency anemia - the stages in development of iron deficiency anemia - the principal management of iron deficiency anemia
Be able to diagnose iron deficiency anemia based on clinical features and laboratory findings

Introduction
Iron deficiency is defined as a decreased total iron body content.
Iron deficiency is the most prevalent single deficiency state on a worldwide.
If iron deficiency is sufficiently severe to diminish erythropoiesis of anemia iron deficiency anemia.
Diminished the capability of individuals: to perform physical labor, growth and development, academic achievement of children.
Faculty of Medicine University of Brawijaya

Iron deficiency anemia 2001underfives children in Indonesia
Household Survey, 2001
Untoro R. Peningkatan Kualitas Hidup Anak Melalui Pencegahan Anemia Gizi Besi. Disajikan pada Kampanye Anti Anemia 2006-2008. Depkes, Jakarta, 1 Maret 2007

Etiologic factors in iron deficiency anemia :1. Negative iron balance
a. Decreased iron intake- Inadequate diet- Impaired absorption
b. Increased iron loss blood loss- Gastrointestinal blood loss : epistaxis, varices,
gastritis, ulcer, etc- Genitourinary blood loss : menorrhagia,
chronic infections, cancer
- Other blood loss : trauma, excessive phlebotomy, etc.c. Increased requirements
- Infancy- Pregnancy- Lactation

Etiologic factors in iron deficiency anemia (cont’d……) :
2. Inadequate presentation to erythroid precursorsa. Atransferrinemiab. Antitransferrin receptor antibodies
3. Abnormal iron balancea. Aceruloplasminemiab. Autosomal-dominant hemochromatosis due to mutations in ferroportin

Iron metabolisms
Body iron distribution and transport
Iron absorption
Iron requirement
Andrew NC. Medical Progress: Disorders of Iron Metabolism. N Engl J Med 1999; 341: 1986-95
Hoffbrand AV, et al. Essential Hematology. 4th. London:Blackwell Science.2001

Body iron distribution

Iron transport across the intestinal epithelium
Andrew NC. Medical Progress: Disorders of Iron Metabolism. N Engl J Med 1999; 341: 1986-95

The transferrin cycles
Andrew NC. Medical Progress: Disorders of Iron Metabolism. N Engl J Med 1999; 341: 1986-95

Iron absorption
Hoffbrand AV, et al. Essential Hematology. 4th. London:Blackwell Science.2001
Factors favouring absorption Factors reducing absorption
Hem ironFerrous form (Fe2+)Acids (HCl, vit. C)Solubilizing agents (sugars, aminoacids)Iron deficiencyIncreased erythropoiesisPregnancyHereditary hemochromatosisIncreased expression of DMT-1 & ferroportin in duodenal enterocytes
Inorganic ironFerric form (Fe3+)Alkalis – antacids, pancreatic secretionsPrecipitating agents – phytates, phosphatesIron excessDecreased erythropoiesisInfectionsTea Decreased expression of DMT-1 & ferroportin in duodenal enterocytes

Iron requirements
Estimated daily iron requirements In children (average):- Urine, sweat, feces : 0.5 mg/day- Growth : 0.6 mg/day- Total : 1.1 mg/day
In female (age 12-15 yrs): - Urine, sweat, feces : 0.5-1 mg/day - Menses : 0.5-1 mg/day - Growth : 0.6 mg/day - Total : 1.6-2.6 mg/day
Hoffbrand AV, et al. Essential Hematology. 4th. London:Blackwell Science.2001

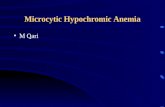
PATHOGENESIS OF IDA
Three pathogenetic and pathophysiologic factors are implicated in the anemia of iron deficiency :
1. Impaired hemoglobin synthesis, a concequence of reduced iron supply.
2. A generalized defect in cellular proliferation. 3. Reduced erythrocyte survival, particularly
when the anemia is severe.

Faculty of Medicine University of BrawijayaFaculty of Medicine University of Brawijaya
Staging I Iron depletion (without anemia)
Staging II Iron deficiency (without anemia)
Staging III Iron deficiency (with anemia)
“Iron deficiency anemia”
Staging of Iron Deficiency
Raspati H dkk. Buku Ajar Hemato-onkologi anak 2005.

CLINICAL STAGES IN DEVELOPMENT OF IRON DEFICIENCY ANEMIA
Stage IPrelatent/Iron Depletion
Stage IILatent/Iron Deficiency
Stage IIIIron Deficiency Anemia
Symptoms Fatique, malaise in some patients Pallor, pica, epithelial changes
Hemoglobin levels Normal Normal DecreasedMean corpuscular volume Normal Normal Decreased
Reticulocyte Hb content Normal Decreased DecreasedSerum iron Normal < 60 ug/dl < 40 g/dlTotal iron binding capacity 360-390 g/dl > 390 g/dl > 410 d/dl
Transferrin saturation Normal < 16% < 16%Serum ferritin < 20 g/L < 12 g/L < 12 g/LFree erythrocyte protoporphyrin, zinc protoporphyrin
Normal Increased Increased
Bone marrow iron Decreased Absent Absent


Diagnosis• History findings :
- onset & severity of anemia, age - parasitism, blood loss (acute or chronic)- inadequate diet (quantity & quality)- poor absorption- increased requirements
• Clinical features : symptoms & signs (general & specific)
• Laboratory findings : hematologic & biochemical markers

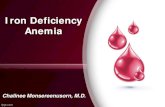
CLINICAL FEATURES OF IDA
Patients with anemia may present with fatique, pallor, vertigo, dyspnea, cold intolerance & lethargySymptoms unique to the IDA patient are :
- pica (an abnormal craving for unusual substances such as dirt, ice, or clay)- cheilitis (inflammation around the lips)- koilonychias (spooning of the nail beds)
IDA in infants may result in developmental delays and behavioral disturbances.
IDA in the 1st two trimesters pregnant women may lead to an increase in preterm delivery and an increase in delivering a low-birth-weight baby.

LABORATORY FINDINGS OF IDA
Hb level < normal varies by sex and ageMCV and MCHC will be markedly < normal RDW may be mildly The reticulocyte count will be lowPeripheral blood smear : hypochromic microcyticTest to assess a patient’s iron status include : - serum iron (SI) normal 50-150 g/L - TIBC normal 250-540 g/L
- transferrin saturation normal 20-50% - serum ferritin normal : ♂ 20-250 g/L
♀ 10-120 g/L

LABORATORY FINDINGS OF IDA…..(cont’d)
Tests are useful to establish the etiology of IDA - stool examination - test to detect blood loss : Benzidin test,
radiolabelled - test to assess hemoglobinuria & hemosiderinuria - Hb electrophoresis to establish thalassemia

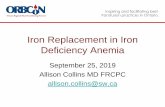
MANAGEMENT OF IDA
TREATMENT1. Medication : elemental iron
In adult : 325 mg (60 mg Fe) orally 3x/day In child : 3-6 mg/kg/day orally divided in 1-3 dosis
2. Dietetic therapy3. Surgical treatment : to stop bleeding and correct
the underlying defect either neoplastic or non-neoplastic disease of GIT, GUT, uterus, and lungs
4. Consultation : department of surgery, GE, etc5. Activity : restriction of activity is usually not
required; patients with moderately severe IDA and significant cardiopulmonary disease should limit their activities

TreatmentElemental Fe
- Do: 3-6 mg/kgBW/d (2-3 dosages)- It may take up to 2 mo after hemoglobin has
been corrected- Adverse effects : GI tract upset
to reduce the adverse reactions :- take the medicine after meal- slow released preparation- take a dosage then increase gradually
Treat the etiologyLanzkowsky P. 1995. p. 35-50.
Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p. 1614-6.Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38.
Killip S, et al. Am Fam Physician 2007;75:671-8.Segel GB, et al. Pediatr Rev 2002;23:75-84.
Grantham-McGregor S & Ani C. J Nutr 2001;131:649S-68S.

Preparation Available strength Elemental FeTablets/capsulesFerrous fumarate 300 mg/cap 99 mg/capFerrous gluconate 300 mg/tab 35 mg/tabFerrous sulphate 300-325 mg/tab 60-65 mg/tabFerrous sulphate, slow released 160 mg/tab 65 mg/tabPolysaccharide-iron complex 150 mg/tab 150 mg/capOral liquid suspensionsFerrous fumarate 60 mg/ml 20 mg/mlFerrous sulphate Drops : 75 mg/ml
Syrup : 30 mg/mlDrops : 15 mg/mlSyrup : 6 mg/ml
ParenteralIron dextran -- 50 mg/mlSodium ferric gluconate -- 12.5 mg/mlIron sucrose -- 20 mg/ml
Iron preparation
http://www.freece.com/FreeCe/Article.asp?dbArticleID=105.

Lanzkowsky P. 1995. p. 35-50.Glader B. In: Nelson Textbook of pediatrics. 17th ed.; 2004. p.
1614-6.Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38.
Killip S, et al. Am Fam Physician 2007;75:671-8.Segel GB, et al. Pediatr Rev 2002;23:75-84.
Response to iron therapy in iron-deficiency anemia

Indication : If hemoglobin levels < 4 g/dL
Transfusion
Lanzkowsky P. 1995. p. 35-50.Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p.
1614-6.
Dept. of Child Health Dr. Saiful Anwar Hospital:Hb < 7 /dL g/dLHb > 7 g/dL, with cardiorespiratory disturbances, severe infection, dehydration, surgical procedures

Diet
Milk : 24 oz/day Iron rich food (fish, liver, meat) rather than rice,
spinach, wheat, soybean ↓ absorption: tanin, calsium, phytates ↑ absorption: vitamin C, HCl, amino acid, fructosa,
meat
Lanzkowsky P. 1995. p. 35-50.Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p.
1614-6.Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-
38.

Parenteral iron therapy
If not successful with oral iron preparation parenteral therapy
Indication:- Severe bowel disease- Genuine intolerance of oral iron- Chronic hemorrhage
Adverse reaction :- Mild : fever, headache, pruritus, nausea- Life threatening : anaphylaxis shock
Lanzkowsky P. 1995. p. 35-50.Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p.
1614-6.Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-
38.Killip S, et al. Am Fam Physician 2007;75:671-8.

Prevention
Primary prevention Exclusive breastfeeding
- The absorption of iron from breast milk is higher than that from whole cow’s milk (50%
vs 10%)- Iron-fortified cow’s milk : 4%
Milk consumption : 24 oz/day (other: 16 oz/day)Lanzkowsky P. 1995. p. 35-50
Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p. 1614-6
Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38Killip S, et al. Am Fam Physician 2007;75:671-8
Segel GB, et al. Pediatr Rev 2002;23:75-84Oski FA. N Engl J Med 1993;329:190-3

Primary prevention…..
Allen LH. J Nutr 2002;132:813S-9SLanzkowsky P. 1995. p. 35-50
Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38Oski FA. N Engl J Med 1993;329:190-3

Secondary prevention First year of life
Diet : - Cow’s milk consumption - Low iron-fortified formula - Exclusive breastfeeding without Fe supplement
Prenatal/perinatal - Anemia during pregnancy - Low birth weight - Prematurity - Gemelli
Socioeconomic - Low socioeconomic - Imigrant from the developing countries - High growth rate
Aterm: age 9-12 moPrematur/LBW or gemelli: age 6 mo
SCREENINGCBC, serum ferritin and transferrin
saturation

Secondary prevention…….Age 1-3 years
History of iron deficiency anemia (+) Milk consumption > 24 oz/day Poor intake of iron and vitamin C Imigrant from the developing countries
age 15-18 months and 24 months
Sandoval et al. Hematol Oncol Clin N Am 2004;18:1423-38.Killip et al. Am Fam Physician 2007;75:671-8.
Brugnara. Clin Chemistry 2003;49:1573-8.

Lack of response to iron therapy
Inappropriate dosage Ineffective iron preparation Did not solve the etiology (e.g. ongoing blood loss) Incorrect diagnosis Poor compliance
Lanzkowsky P. 1995. p. 35-50Glader B. Nelson Textbook of pediatrics. 17th ed.; 2004. p.
1614-6Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38
Killip S, et al. Am Fam Physician 2007;75:671-8Segel GB, et al. Pediatr Rev 2002;23:75-84



Etiology of iron deficiency Less 1 year• Low iron storage (LBW or gemelli)• Lack of iron supplements in exclusively breast-
fed infants beyond 6 months of age• Unfortified milk formulaAge 1-2 year• ”Milkaholics”• Increased iron needs due to chronic infection• Malabsorption• Blood loss >> eg. parasitic infection and
Meckel’s diverticulum

Etiology………Age 2-5 year• Poor intake of iron-rich food• Increased iron needs due to chronic infection• Blood loss >> eg. Parasitic infection and
Meckel’s diverticulumAge 5 year – adolescence• Blood loss >> eg. Parasitic infection or
polyposisAdolescence – adult• Woman : eg. menorrhagia
Lanzkowsky P. 1995. p. 35-50.Glader B. In: Nelson Textbook of pediatrics. 17th ed.; 2004. p. 1614-6.
Sandoval C, et al. Hematol Oncol Clin N Am 2004;18:1423-38.Killip S, et al. Am Fam Physician 2007;75:671-8.
Segel GB, et al. Pediatr Rev 2002;23:75-84.

Figure 5. The Underlying and Immediate Causes of Iron Deficiency
UNDERLYING CAUSES IMMEDIATE CAUSESLow food supplyErroneous feeding
practicesLow socio-economic status
Low intake of available ironUnsuitable meal
compositionexcess of inhibitors
Growth Pregnancy & Lactation
Acute bleeding Chronic blood lossPoor sanitation &
parasitism
Inadequate health services
Inadequate diet
Poor absorption
Increased requirements
Blood loss
Infection
Iron deficiency
Source : Florentina RF, et al (1984)

For infants (0 to 12 months) and children (1 to 5 years) • Encourage breastfeeding or • Iron-fortified formula • Serve one serving of fruits, vegetables, juice by 6 months • Screen children for anemia every 6 monthsSchool-age children (5 to 12 years) and adolescent boys (12 to 18 years) • Screen only those with history of IDA or low iron intake groupsAdolescent girls (12 to 18 years) and nonpregnant women of childbearing age • Encourage intake of iron-rich food and foods that increase iron absorption • Screen nonpregnant women every 5 to 10 years through childbearing yearsPregnant women • Start oral doses of iron at first prenatal visit • Screen for anemia at first prenatal visit • If hemoglobin is _9 g/dL, provide further medical attentionPostpartum women • Risk factors include continued anemia, excessive blood loss & multiple birthsMales older than 18 years/postmenopausal women • No routine screening is recommended
Table 4. Recommendations to Prevent and Control Iron Deficiency in the US

Controversies A single vs 3-times-daily dose iron supplementation
resulted in a similar rate of successful treatment of anemia (Hb & ferritin) (p= 0,25 and p=0,99)
Sungthong et al. J Nutr 2004;134:2349-54 Siddiqui et al. J Trop Pediatr 2004;50:276-8Awasthi et al. J Trop Pediatr 2005;51:67-71
Zlotkin et al. Pediatrics 2001;108:613-6
Iron supplementation 1-2 weekly vs daily- The increases in Hb concentration were comparable- Improvement of cognitive function- Cost effective- No or fewer side-effect

Controversies…..
Several micronutrients can improve the hemoglobin response to iron.
Iron absorption may be inhibited by nutrients such calsium, magnesium and zinc.
Geltzman et al. Pediatrics 2004;114:86 93.
Allen LH. J Nutr 2002;132:813S-9S
Multivitamins with iron was not effective in preventing iron deficiency