
Combination and Sequential Therapy for the …
16
Combination and Sequential Therapy for the Treatment of Osteoporosis Felicia Cosman 1 The screen versions of these slides have full details of copyright and acknowledgements 1 Combination and Sequential Therapy for the Treatment of Osteoporosis Prof. Felicia Cosman Professor of Medicine, Columbia University, New York, NY Medical Director, Clinical Research Center Helen Hayes Hospital, West Haverstraw, NY 2 Disclosures/acknowledgements • Speakers Bureaus: Eli Lilly, Amgen • Advisory Boards: Amgen, Merck, Eli Lilly, Radius • Consultant: Eli Lilly, Amgen, Merck, Novartis, Radius, GSK, Unigene, Tarsa, Zosano, Enteris • Research Grants/Research Medication: Amgen, Novartis, Eli Lilly, Merck 3 Current pharmacologic management of osteoporosis • Anabolic agents: Parathyroid hormone analogs – PTH 1-84 – Teriparatide (PTH 1-34) • Antiresorptive agents: Hormone/estrogen therapy Selective estrogen receptor modulators Conjugated estrogen/ bazedoxifene complex Oral bisphosphonates – Alendronate, risedronate, ibandronate Intravenous zoledronic acid Subcutaneous denosumab
Transcript of Combination and Sequential Therapy for the …

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
1The screen versions of these slides have full details of copyright and acknowledgements
1
Combination and Sequential Therapy for the Treatment of Osteoporosis
Prof. Felicia Cosman
Professor of Medicine, Columbia University, New York, NY
Medical Director, Clinical Research Center
Helen Hayes Hospital, West Haverstraw, NY
2
Disclosures/acknowledgements
• Speakers Bureaus: Eli Lilly, Amgen
• Advisory Boards: Amgen, Merck, Eli Lilly, Radius
• Consultant: Eli Lilly, Amgen, Merck, Novartis, Radius,
GSK, Unigene, Tarsa, Zosano, Enteris
• Research Grants/Research Medication:
Amgen, Novartis, Eli Lilly, Merck
3
Current pharmacologic management of osteoporosis
• Anabolic agents:
Parathyroid hormone analogs
– PTH 1-84
– Teriparatide (PTH 1-34)
• Antiresorptive agents:
Hormone/estrogen therapy
Selective estrogen
receptor modulators
Conjugated estrogen/
bazedoxifene complex
Oral bisphosphonates
– Alendronate, risedronate, ibandronate
Intravenous zoledronic acid
Subcutaneous denosumab

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
2The screen versions of these slides have full details of copyright and acknowledgements
4
Choosing anabolic vs. antiresorptive therapy
• As first-line therapy
No consensus or guidelines
Use in highest risk patients:
– Patient with recent fracture (within the year)
– Patients with history of multiple fractures
• As second-line therapy
Sometimes mandated by reimbursement
Response to anabolic medication different in patients
who have already been treated with potent antiresorptive therapy
(bisphosphonates and denosumab)
No fracture data in this group
5
Combination therapy rarely used
• Cost and potential for additional side effects/adverse events
• Belief that combination therapy provides no benefit
and might even be inferior to TPTD monotherapy
In part based on results of the PaTH trial1
– Women randomized to receive PTH monotherapy, alendronate
monotherapy or PTH plus alendronate combination therapy
1 Black et al., NEJM 2003; 349: 1207-1215
6
PaTH 12 month changes with PTH1-84 in DXA BMD
Black et al., NEJM 2003; 349: 1207-15
• PTH-alendronate combination group showed no greater
improvement in spine BMD – a disappointment
• The combination therapy did produce a superior effect
on hip and radius BMD

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
3The screen versions of these slides have full details of copyright and acknowledgements
7
Caveats in generalizability of PaTH trial
• Daily not weekly alendronate
Small uptake into osteoblasts with each dose
• Alendronate is different from other bisphosphonates
and other antiresorptives
• PaTH utilized PTH 1-84 (not 1-34)
Possible differences in skeletal response1
• Study performed in treatment naïve women
Results may not apply to treatment experienced women,
particularly those on the most potent antiresorptive therapies
1Hansen S et al., JBMR 2013
8
Response to TPTD different in treatment naïve and treatment experienced
• Much larger active bone surface in treatment naïve individuals
• In treatment naïve, with acute administration
of potent antiresoptive agents
Increase in endogenous PTH for up to 12 months
Might produce a different response
to exogenously administered PTH
• Perhaps unique effects on osteoclasts and/or osteoblasts
in treatment experienced individuals
9
Alendronate treated Treatment naive
Inactive osteoclast Normal osteoclast
50 μm 50 μm
< 22 nuclei/cell profile < 8 nuclei/cell profile
Images used with permission by Dr. Dempster 31 May 2013
Dempster, et al., ASBMR 2007

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
4The screen versions of these slides have full details of copyright and acknowledgements
10
Re-evaluating the potential role for combination and sequential therapy
• In treatment naïve women
Concomitant treatment with intravenous zoledronic acid
and TPTD1
Concomitant treatment with subcutaneous denosumab
and TPTD2-3
1. Cosman, et al., JBMR 2011; 26(3): 503–511
2. Tsai et al., Lancet 2013
3. Leder et al., JCEM 2014
11
Treatment naïve: IV zoledronic acidand daily TPTD study overview
• 412 treatment-naïve postmenopausal women
T score ≤−2.5 at any site or T score ≤−2.0 plus ≥1 op-related fracture
Age range 45-87 years, mean 65
Mean spine T-score spine -2.9, Hip -1.9
• Randomized to one of 3 active treatment groups
IV ZOL 5 mg
IV ZOL 5 mg + Subcut TPTD 20 μg/day
IV PBO + TPTD 20 μg/day
• One-year follow-up
Cosman, et al., JBMR 2011; 26(3): 503–511
12
ZOL + TPTD
TPTD alone
ZOL alone
Treatment naïve women: IV Zol and daily TPTD changes in serum β–CTx and PINP
Weeks
Seru
m β
-CTx
(n
g/m
L)
Serum β-CTx
0 4 8 12 16 20 24 28 32 36 40 44 48 520
0.2
0.8
1
0.4
0.6
Weeks
Seru
m P
INP
(n
g/m
L)
Serum PINP
0 4 8 12 16 20 24 28 32 36 40 44 48 520
50
100
150
200
Cosman, et al., JBMR 2011; 26(3): 503–511

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
5The screen versions of these slides have full details of copyright and acknowledgements
13
Treatment naïve women: IV Zol and daily TPTDpercent changes in lumbar spine BMD
Weeks
‡Least-squares mean (LSM) % changes
0 13 26 39 52
Me
an %
ch
ange
in B
MD
‡
0
1
3
4
6
7
9
2
5
8
*
*
†
*P<0.001 vs. TPTD alone and vs. ZOL alone
†P<0.001 vs. ZOL alone
†
Cosman, et al., JBMR 2011; 26(3): 503–511
ZOL + TPTD
TPTD alone
ZOL alone
14
0
0.5
1
1.5
2
2.5
3
0 13 26 39 52
Weeks
Me
an %
ch
ange
in B
MD
‡
Total hip BMD
0 13 26 52
Weeks
Me
an %
ch
ange
in B
MD
‡
Femoral neck BMD
-1
0
2
3
1
39
*
*†*
**
*P<0.05 vs. TPTD alone
†P<0.05 vs. ZOL alone
*
*
*
*
**
*
ZOL + TPTD
TPTD alone
ZOL aloneCosman, et al., JBMR 2011; 26(3): 503–511
‡Least-squares mean (LSM) % changes
Treatment naïve women: IV Zol and daily TPTD percent changes in lumbar spine BMD (2)
15
Treatment naïve women: IV Zol and daily TPTD - summary
.
• With combination (ZOL+TPTD) therapy:
Spine BMD increase similar to TPTD alone
– Combination >ZOL alone but not greater than TPTD alone
Hip BMD increase similar to ZOL alone
– Combination >TPTD alone
• Considering hip and spine BMD outcomes together,
combination therapy provided the overall largest
and fastest BMD outcome
Cosman, et al., JBMR 2011; 26(3): 503–511

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
6The screen versions of these slides have full details of copyright and acknowledgements
16
DATA trial: teriparatide or Dmab monotherapy vs. combination
• 94 postmenopausal women at high risk of fracture
(age 51-91)
• 12 month open label randomized controlled trial
with three treatment groups:
Teriparatide (TPTD) 20 μg SC daily (n=31)
Denosumab (DMAB) 60 mg SC Q6 mo (n=33)
Both medications (n=30)
Tsai JN Lancet 2013
17
Teriparatide or Denosumab monotherapy vs. combination therapy
Tsai JN Lancet 2013
18Tsai Lancet 2013
Teriparatide or Denosumab monotherapy vs. combination therapy (2)

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
7The screen versions of these slides have full details of copyright and acknowledgements
19
Gray bars: BMD gain year 1
Yellow bars: BMD gain year 2
Leder et al., JCEM 2014
Teriparatide or Denosumab monotherapy vs. combination therapy (3)
20
Summary: combination therapyin treatment naïve women
• Combination therapy: all studies consistent with superior
BMD gain in the hip compared to TPTD/PTH monotherapy
Teriparatide with zoledronic acid
Teriparatide with denosumab
PTH with alendronate
• Combination therapy superior for BOTH spine
and hip BMD gain
Teriparatide with denosumab
21
Teriparatide in the treatment experienced woman: teriparatide monotherapy or combination therapy?

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
8The screen versions of these slides have full details of copyright and acknowledgements
22
Teriparatide after prior bisphosphonate treatment
• ADD vs. Switch Studies
Spine BMD may not be affected substantially when switching
to teriparatide monotherapy compared to adding teriparatide
to ongoing antiresorptive
Hip BMD routinely declines in Switch Studies over 6-12 months1-3
Hip BMD does not decline when TPTD is added to ongoing BP4
References:
1.Ettinger JBMR 2004; 19(5): 745–751
2.Miller, et al., JCEM 2008; 93: 3785–3793
3.Boonen, et al., JCEM 2008; 93: 852-860
4.Cosman, et al., NEJM 2005; 353: 566-75
23
0 3 6 12 18
-2
0
2
4
6
8
10
12
*
TPTD after raloxifene or alendronate:effect on total hip BMD
Mean %change
Months
*P<0.05 vs. from baseline
†P<0.05 between groups
Raloxifene-TPTD
Alendronate-TPTD
0.3
1.8
*†
Ettinger JBMR 2004; 19(5): 745–751
24
Total hip BMD percent changes from baselineCompleter population
Miller, et al. JCEM 2008; 93: 3785–3793
• Hip bone density declined substantially within the first
six months, and was still below baseline at the end
of the year-long study (residronate or alendronate
switch to PTH monotherapy)

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
9The screen versions of these slides have full details of copyright and acknowledgements
25
Adjusted mean BMD changes from baselineTotal hip
Boonen, et al., JCEM 2008; 93: 852-860
• When women were switched to teriparatide:
hip bone density declined significantly in both groups
within the first six months
It remained below baseline for the entire first whole year
of treatment
26
Total hip BMD
Tota
l Hip
% C
han
ge in
BM
D
Cosman, et al., NEJM 2005; 353: 566-75
u ALN Only
l
n Daily PTH+ALN
Cyclic PTH+ALN
n
nn
nn
n
l l
ll
u
u uu
u
u
0 3 6 9 12 15-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
Time (months)
l
l
27
Switch to teriparatide in patients experienced on prior denosumab treatment
• Patients randomized to denosumab arm in DATA trial
After 2 years of denosumab alone, switched to teriparatide
Leder et al., ASBMR 2014

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
10The screen versions of these slides have full details of copyright and acknowledgements
28
Data trial 1 year extension
Leder et al., ASBMR 2014
PA Spine
29
Switch to teriparatide in patients experienced on prior antiresorptive treatment
• Hip BMD declines consistently in all studies in patients
on potent antiresorptive agents (alendronate,
risedronate, denosumab)
Magnitude of BMD decline might be related to potency
of antiresorptive effect
• No fracture data available to determine if this decline
is associated with a detrimental effect on fracture occurrence
Studies small
An approach to prevent this BMD decline would be preferable
in patients at high risk for hip and other cortical bone fractures
30
Teriparatide in treatment experienced: monotherapy vs. combination therapy
• Objective: to compare the effect of adding vs. switching
to TPTD in women on prior aln or rlx in a randomized trial
• Subjects: postmenopausal women ≥ 50 years of age
on weekly aln (n=102) or daily rlx (n=96) for > 18 months
Average treatment duration >4 years
Mean age 68
• Protocol: randomize to
Continue Aln/Rlx and add TPTD (combination therapy)
Stop Aln/Rlx and switch to TPTD (monotherapy)
Cosman F, et al., JCEM 2009; 94: 3772–3780

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
11The screen versions of these slides have full details of copyright and acknowledgements
31
Switch
Add
TPTD in treatment experienced switch vs. add: bone turnover markers: PINP
P < 0.05; §, P < 0.01; and †, P < 0.001 for percentage change difference
between groups within the alendronate or raloxifene stratum
Cosman F, et al., JCEM 2009; 94: 3772–3780
32
TPTD in treatment experienced switch vs. add: bone turnover markers: CTX
P < 0.05; §, P < 0.01; and †, P < 0.001 for percentage change difference
between groups within the alendronate or raloxifene stratum
Switch
Add
Cosman F, et al., JCEM 2009; 94: 3772–3780
33
Teriparatide in treatment experienced switch vs. add: BMD at 6 months
*P<0.05 within group from baseline
+P<0.05 between treatment groups within each treatment stratum
ALN RLX
(Switch) (Switch)(Add) (Add)
Cosman F, et al., JCEM 2009; 94: 3772–3780

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
12The screen versions of these slides have full details of copyright and acknowledgements
34
Teriparatide in treatment experienced switch vs. add: BMD at 18 months
***P < 0.001, **P < 0.01 within group from baseline
++P < 0.01, +P< 0.05 between treatment groups within each treatment stratum
ALN RLX
Cosman F, et al., JCEM 2009; 94: 3772–3780
35
Spine volumetric BMD
*P<0.01 vs. baseline
p values for differences between add vs. switch groups are shown above each pair of bars
Add group
Switch group
Values are medians
(IQ range)
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
36
Estimated spine strength
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
*P<0.01 vs. baseline
p values for differences between add vs. switch groups are shown above each pair of bars
Add group
Switch group
Values are medians
(IQ range)

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
13The screen versions of these slides have full details of copyright and acknowledgements
37
Hip volumetric BMD
Add group
Switch group
Values are medians
(IQ range)
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
*P<0.01 vs. baseline
p values for differences between add vs. switch groups are shown above each pair of bars
38
Estimated hip strength
*P<0.01 vs. baseline; †P<0.05 vs. baseline
p values for differences between add vs .switch groups are shown above each pair of bars
Add group
Switch group
Values are medians
(IQ range)
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
39
Alendronate stratumHip volumetric BMD, month 18
*P<0.01 vs. baseline
p values for differences between add vs. switch groups are shown above each pair of bars
ALN Add
ALN Switch
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
Values are medians
(IQ range)

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
14The screen versions of these slides have full details of copyright and acknowledgements
40
Alendronate stratumEstimated hip strength, month 18
*P<0.01 vs. baseline
p values for differences between add vs. switch groups are shown above each pair of bars
Cosman, et al., JBMR 2013 Jun; 28(6): 1328-36
Values are medians
(IQ range)
ALN Add
ALN Switch
41
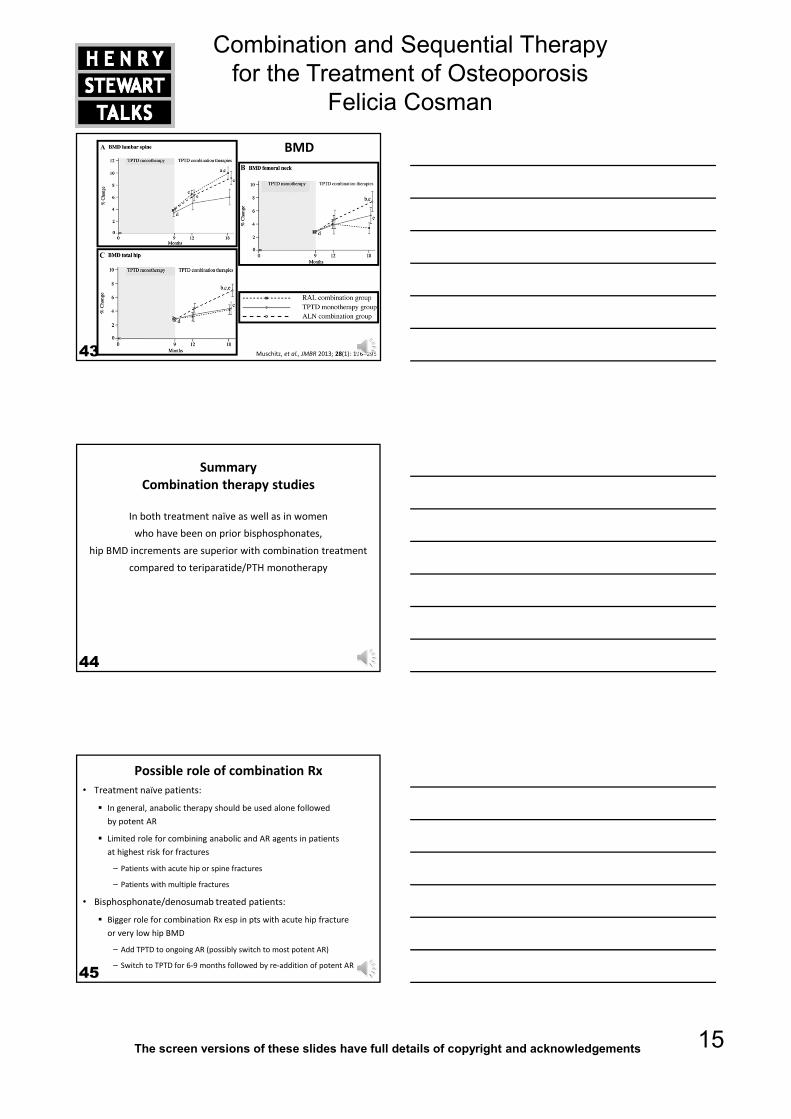
CONFORS trial: TPTD alone for 9 months followed by combination
• 125 women
90% had history of prior AR therapy
– 70% history of alendronate exposure
• All women received TPTD alone for 9 months
• After 9 months TPTD, randomized to:
Continued TPTD alone (n=47)
Continued TPTD + ALN 70 mg/wk (n=41)
Continued TPTD + RLX 60 mg/day (n=37)
for 9 additional months
Muschitz, et al., JMBR 2013; 28(1): 196–205
42
Bone turnover
Muschitz, et al., JMBR 2013; 28(1): 196–205
Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
15The screen versions of these slides have full details of copyright and acknowledgements
43
BMD
Muschitz, et al., JMBR 2013; 28(1): 196–205
44
Summary Combination therapy studies
In both treatment naïve as well as in women
who have been on prior bisphosphonates,
hip BMD increments are superior with combination treatment
compared to teriparatide/PTH monotherapy
45
Possible role of combination Rx
• Treatment naïve patients:
In general, anabolic therapy should be used alone followed
by potent AR
Limited role for combining anabolic and AR agents in patients
at highest risk for fractures
– Patients with acute hip or spine fractures
– Patients with multiple fractures
• Bisphosphonate/denosumab treated patients:
Bigger role for combination Rx esp in pts with acute hip fracture
or very low hip BMD
– Add TPTD to ongoing AR (possibly switch to most potent AR)
– Switch to TPTD for 6-9 months followed by re-addition of potent AR

Combination and Sequential Therapy for the Treatment of Osteoporosis
Felicia Cosman
16The screen versions of these slides have full details of copyright and acknowledgements
46








![[G] Combination therapy - NICE](https://static.fdocuments.net/doc/165x107/61c4f6f30b69943f787f9356/g-combination-therapy-nice.jpg)









