




![Pneumonia (Ventilator-associated [VAP] and non-ventilator ...](https://static.fdocuments.net/doc/165x107/61c3dfa934191a172140c0d5/pneumonia-ventilator-associated-vap-and-non-ventilator-.jpg)

Languages
Pages
Legal

Ventilator Associated Pneumonia (VAP) Practice Alert
Ventilator Associated Pneumonia Ventilator Associated Pneumonia (VAP) (VAP)
Issued 01/2008Issued 01/2008
Author: Author: Marianne Chulay, Marianne Chulay, RN, DNSc, FAAN
Consultant, Clinical Research and Critical Care Nursing
Reviewers: Suzi Burns, Mary Jo Grap,Reviewers: Suzi Burns, Mary Jo Grap,Judy Verger, and Lori JacksonJudy Verger, and Lori Jackson
Ventilator Associated Pneumonia (VAP) Practice Alert
Prevention of Ventilator Prevention of Ventilator Associated Pneumonia (VAP)Associated Pneumonia (VAP)
2
Ventilator Associated Pneumonia (VAP) Practice Alert3
Lecture Content
Epidemiology of VAP Prevention strategies
HOB elevation Ventilator equipment changes Continuous removal of subglottic secretions Handwashing
Ventilator Associated Pneumonia (VAP) Practice Alert
Epidemiology of Epidemiology of Ventilator Associated Pneumonia Ventilator Associated Pneumonia
(VAP)(VAP)
4
Ventilator Associated Pneumonia (VAP) Practice Alert5
Nosocomial Pneumonias
Account for 15% of all hospital associated infections
Account for 27% of all MICU acquired infections
Primary risk factor is mechanical ventilation (risk 6 to 21 times the rate for nonventilated patients)
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004Craven, Chest 2000; 117:186S-187S.
Ventilator Associated Pneumonia (VAP) Practice Alert6
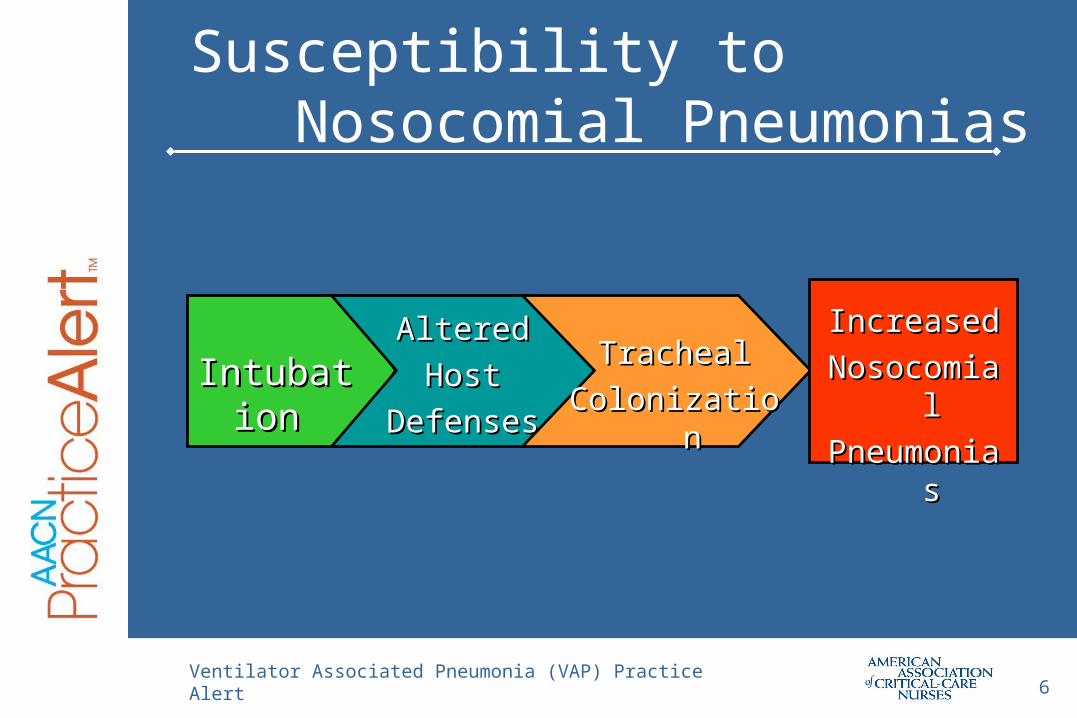
Susceptibility to Nosocomial Pneumonias
IntubationIntubationAlteredAltered
HostHost
DefensesDefenses
TrachealTracheal
ColonizationColonization
IncreasedIncreased
NosocomialNosocomial
PneumoniasPneumonias
Ventilator Associated Pneumonia (VAP) Practice Alert7
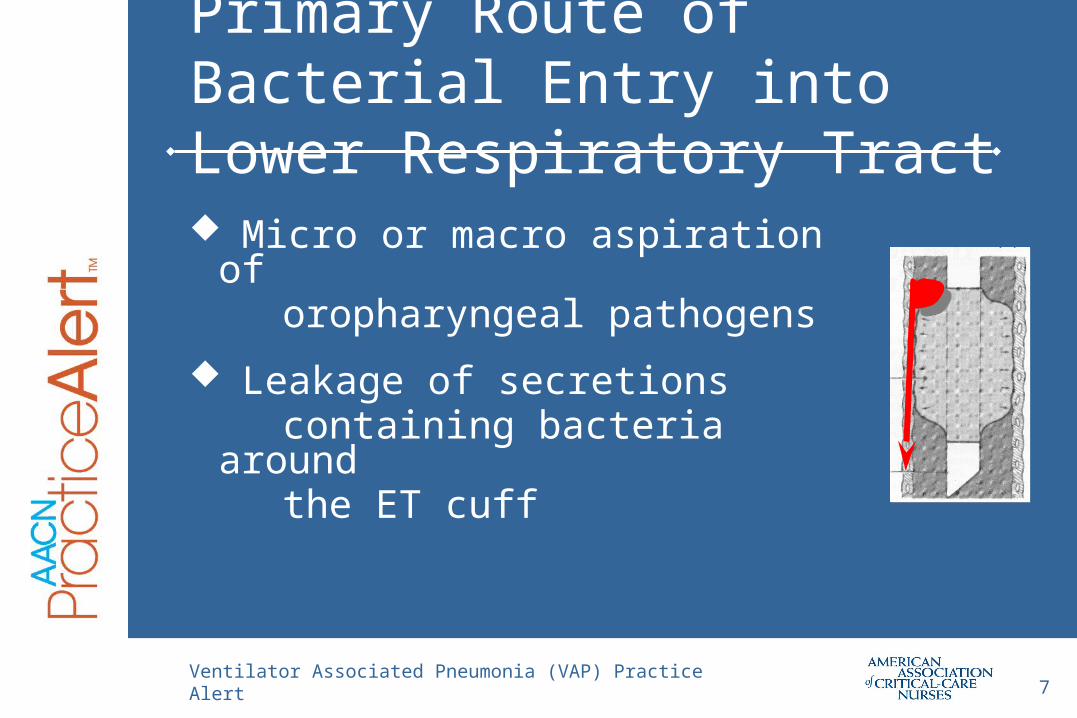
Primary Route of Bacterial Entry into Lower Respiratory Tract
Micro or macro aspiration of
oropharyngeal pathogens
Leakage of secretions containing bacteria around the ET cuff
Ventilator Associated Pneumonia (VAP) Practice Alert8
VAP Etiology Most are bacterial pathogens, with Gram negative
bacilli common
Pseudomonas aeruginosa Proteus spp Acinetobacter spp
Staphlococcus aureus
Early VAP associated with non-multi-antibiotic- resistant organisms
Late VAP associated with antibiotic-resistant organism
Ventilator Associated Pneumonia (VAP) Practice Alert9
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004Heyland et al, Am J Respir Crit Care Med 1999; 159:1249Bercault et al, Crit Care Med 2001; 29:2303
Mortality ranges from 20 to 41%, depending on infecting organism, antecedent antimicrobial therapy, and underlying disease(s)
Leading cause of mortality from nosocomial infections in hospitals
Significance of Nosocomial Pneumonias
Ventilator Associated Pneumonia (VAP) Practice Alert10
Significance of Nosocomial Pneumonias Increases ventilatory support requirements and ICU stay
by 4.3 days
Increases hospital LOS by 4 to 9 days
Increases cost - > $11,000 per episode
Estimates of VAP cost / year for nation > $ 1.2 billion
Heyland et al, Am J Respir Crit Care Med 1999;159:1249Craven, Chest 2000;117:186-187SRello et al, Chest 2002;122:2115Safdar et al, Critical Care Medicine 2005;33:2184-93
Ventilator Associated Pneumonia (VAP) Practice Alert
VAP PreventionVAP Prevention
11
Ventilator Associated Pneumonia (VAP) Practice Alert12
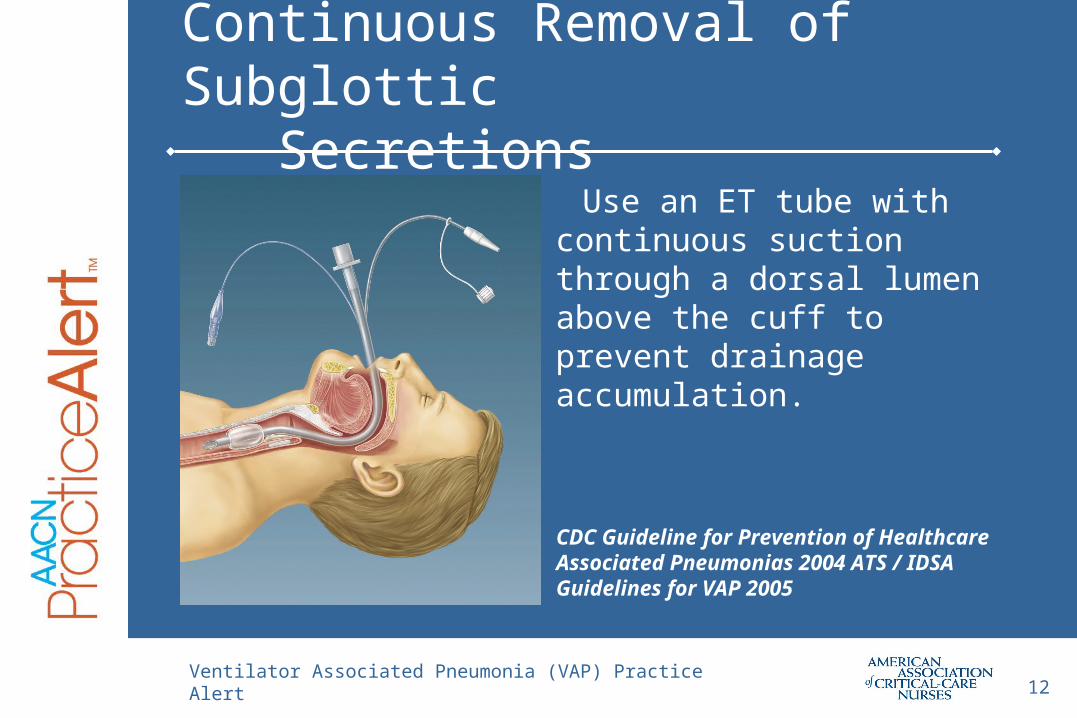
Continuous Removal of Subglottic Secretions
Use an ET tube with continuous suction through a dorsal lumen above the cuff to prevent drainage accumulation.
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004 ATS / IDSA Guidelines for VAP 2005
Ventilator Associated Pneumonia (VAP) Practice Alert13
Continuous Removal of Subglottic Secretions Mahul et al. Int Care Med 1992;18:20-25
Valles et al. Ann Int Med 1995;122:179-186
Kollef et al. Chest 1999;116:1339-1346
Smulders et al. Chest 2002;121:858-862
Dezfulian et al. Am J Med 2005;118:11-18 (meta-analysis)
Ventilator Associated Pneumonia (VAP) Practice Alert14
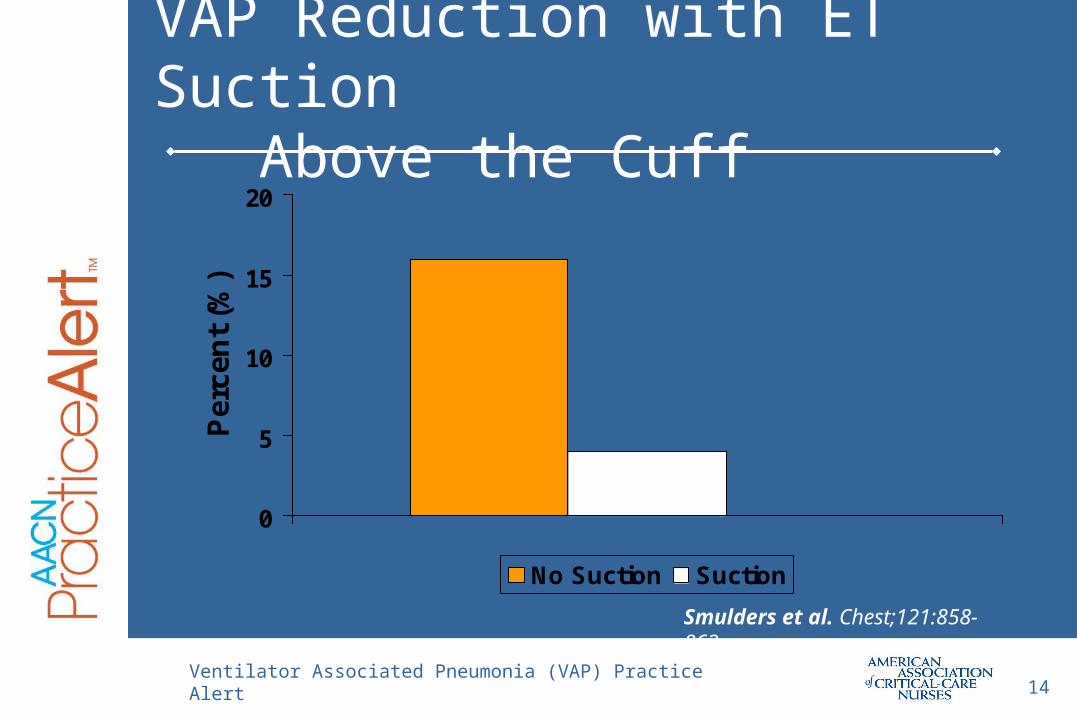
VAP Reduction with ET Suction Above the Cuff
0
5
10
15
20P
erce
nt
(%)
No Suction Suction
Smulders et al. Chest;121:858-862
Ventilator Associated Pneumonia (VAP) Practice Alert15
HOB Elevation
HOB at 30-45º
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004 ATS / IDSA Guidelines for VAP 2005
Ventilator Associated Pneumonia (VAP) Practice Alert16
HOB Elevation
HOB at 30-45º
Torres et al, Annals of Int Med 1992;116:540-543 Ibanez et al. JPEN 1992;16:419-422 Orozco-Levi et al. Am J Respir Crit Care Med
1995;152:1387-1390 Drakulovic et al. Lancet 1999;354:1851-1858 Davis et al. Crit Care 2001;5:81-87 Grap et al. Am J of Crit Care 2005 14:325-332
Ventilator Associated Pneumonia (VAP) Practice Alert17
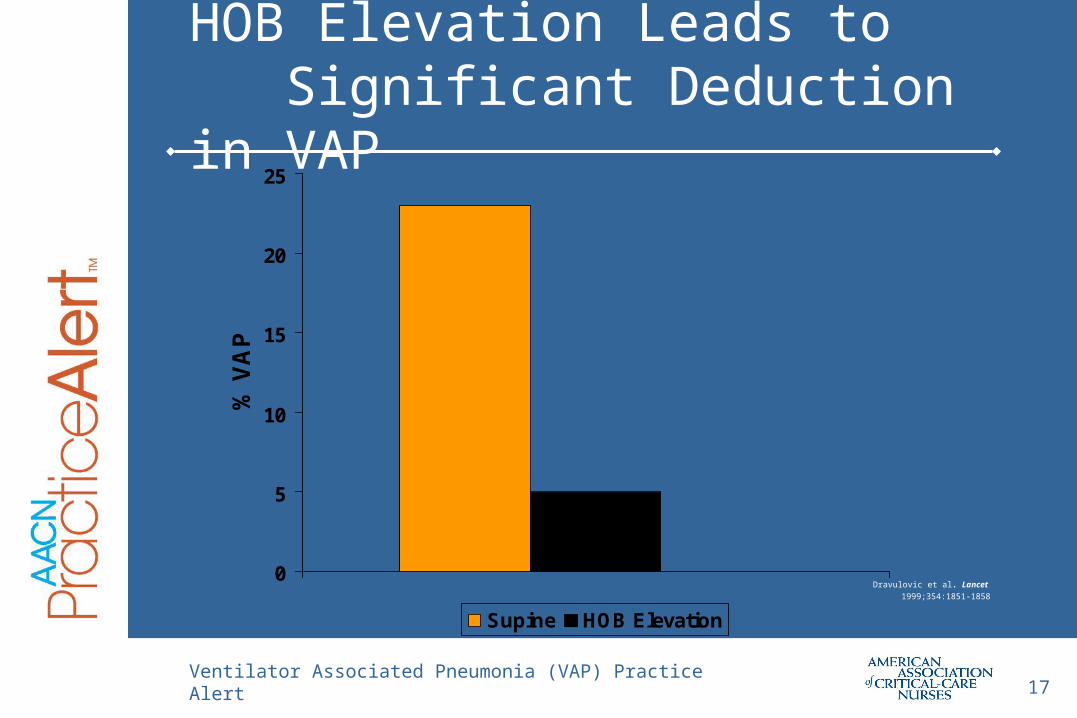
HOB Elevation Leads to Significant Deduction in VAP
0
5
10
15
20
25
% V
AP
Supine HOB Elevation
Dravulovic et al. Lancet
1999;354:1851-1858
Ventilator Associated Pneumonia (VAP) Practice Alert18
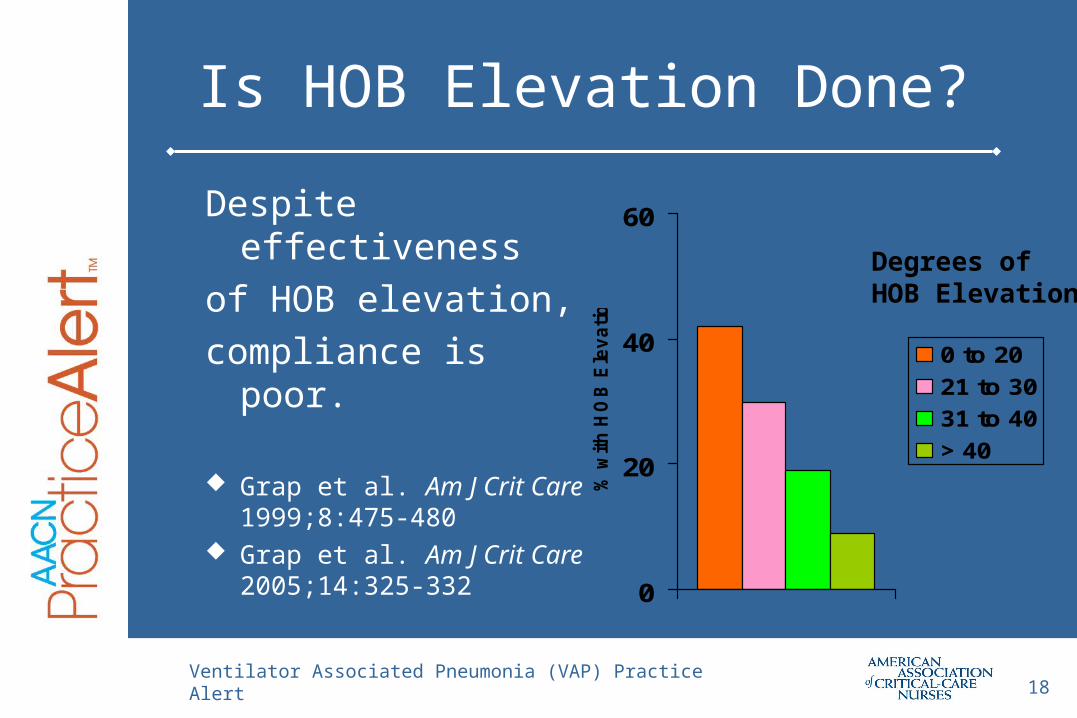
Is HOB Elevation Done?
Despite effectiveness
of HOB elevation,
compliance is poor.
Grap et al. Am J Crit Care 1999;8:475-480
Grap et al. Am J Crit Care 2005;14:325-332
0
20
40
60
% w
ith
HO
B E
lev
ati
on
0 to 20
21 to 30
31 to 40
> 40
Degrees ofHOB Elevation
Ventilator Associated Pneumonia (VAP) Practice Alert19
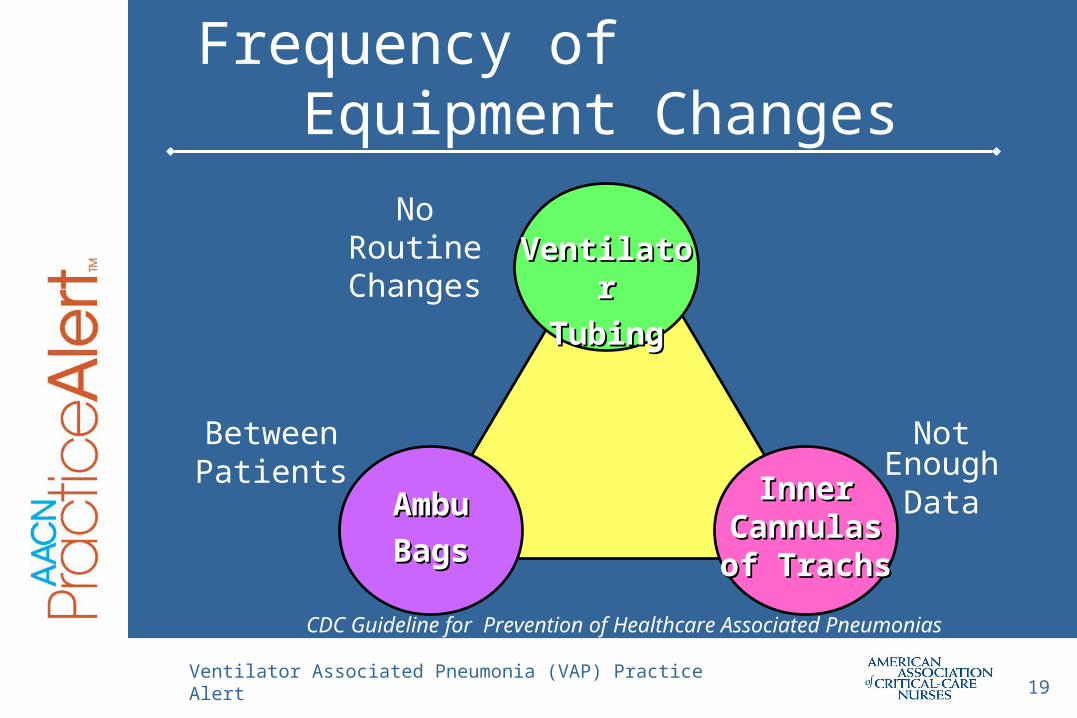
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004
Frequency of Equipment Changes
VentilatorVentilator
TubingTubing
AmbuAmbu
BagsBags
Inner Inner Cannulas Cannulas of Trachsof Trachs
No Routine Changes
BetweenPatients
Not EnoughData

Ventilator Associated Pneumonia (VAP) Practice Alert20
Handwashing
What role does handwashing playin nosocomial pneumonias?
Albert, NEJM 1981; Preston, AJM 1981; CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004
Ventilator Associated Pneumonia (VAP) Practice Alert21
VAP Prevention
Wash hands or use an alcohol-based waterless antiseptic agent before and after suctioning, touching ventilator equipment, and/or coming into contact with respiratory secretions.
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004AACN Practice Alert for VAP, 2007
Ventilator Associated Pneumonia (VAP) Practice Alert22
VAP Protection
Use a continuous subglottic suction ET tube for intubations expected to be > 24 hours
Keep the HOB elevated to at least 30 degrees unless medically contraindicated
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004AACN Practice Alert for VAP, 2007
Ventilator Associated Pneumonia (VAP) Practice Alert23
No Data to Support These Strategies
Use of small bore versus large bore gastric tubes
Continuous versus bolus feeding
Gastric versus small intestine tubes
Closed versus open suctioning methods
Kinetic beds
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004
Ventilator Associated Pneumonia (VAP) Practice Alert24
Oral Care
Role of oral care, colonization of the oropharynx, and VAP unclear – dental plaque may be involved as a reservoir
Limited research on impact of rigorous oral care to alter VAP rates
Surveys indicate most nurses use foam swabs rather than toothbrushes in intubated patients
CDC Guideline for Prevention of Healthcare Associated Pneumonias 2004Grap M. Amer J of Critical Care 2003;12:113-119.
Ventilator Associated Pneumonia (VAP) Practice Alert25
For more information or further assistance, please contact a clinical practice specialist with the AACN Practice Resource Network.
Need Further Assistance?
Email:[email protected]
Phone:
(800) 394-5995
Top Related