







Languages
Pages
Legal


1
Topic 8 – Motor Neuron Disorders & Spinal Cord Injury
1. Terminology
2. "Upper motor neuron" injury
3. Mechanisms of damage
4. Some disorders
Motor System Disorders -Terminology
• Muscle Strength• Paralysis / Paresis • hemi-, para- , or tetra (quad)-
plegia
• Muscle Bulk• atrophy – disuse or neurogenic
Motor System Disorders -Terminology
• Upper motor neurons• Originate in "higher" regions of
brain such as motor cortex• Corticospinal tract
• Lower motor neurons• Directly innervate skeletal
muscles
• Hypotonia - abnormally low resistance to stretch
• cerebellar disorders• LMN lesions• acute UMN lesions
• Hypertonia - abnormally strong resistance to stretch
• chronic UMN lesions• 2 types = spastic and rigid
Motor System Disorders -Terminology
• Spastic Hypertonia• resistance to passive movement
is velocity sensitive
• Rigidity • resistance to passive movement
remains constant regardless of velocity
• Decorticate / Decerebrate
Motor System Disorders -Terminology
Decerebrate Rigidity
2
Source: Haines, Fundamental Neuroscience, Churchill-Livingstone, 2002
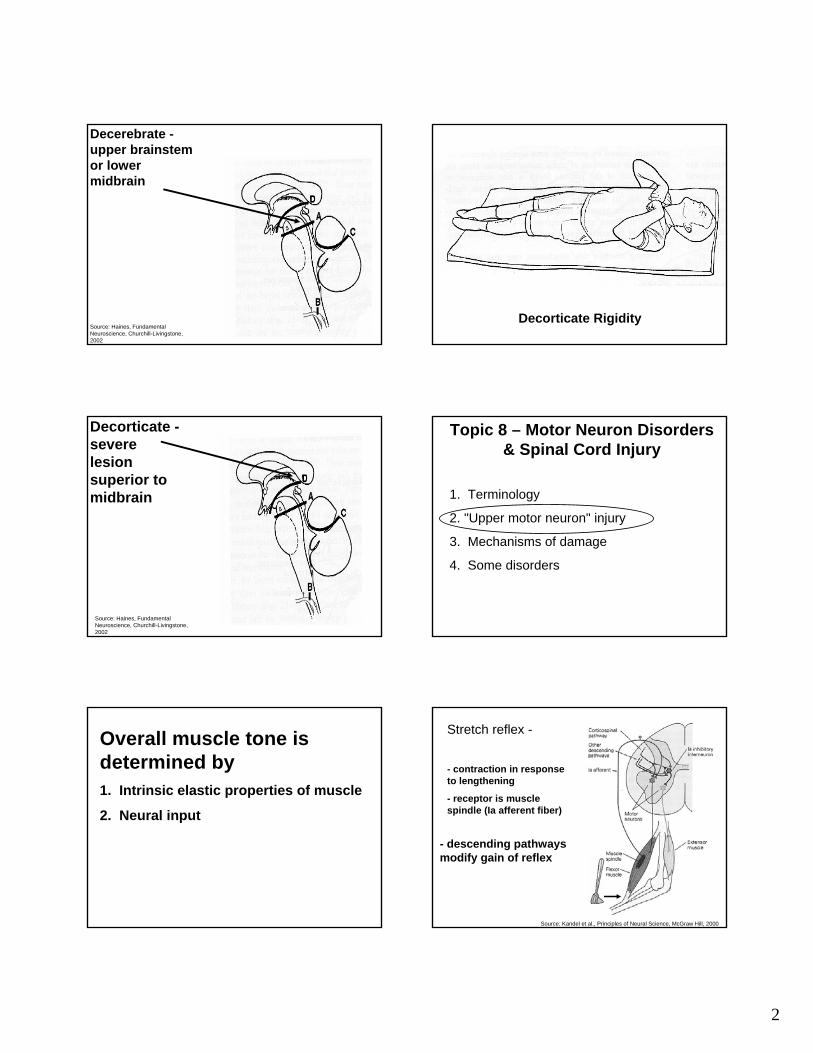
Decerebrate -upper brainstem or lower midbrain
Decorticate Rigidity
Source: Haines, Fundamental Neuroscience, Churchill-Livingstone, 2002
Decorticate -severe lesion superior to midbrain
Topic 8 – Motor Neuron Disorders & Spinal Cord Injury
1. Terminology
2. "Upper motor neuron" injury
3. Mechanisms of damage
4. Some disorders
Overall muscle tone is determined by1. Intrinsic elastic properties of muscle
2. Neural input
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
- contraction in response to lengthening
- receptor is muscle spindle (Ia afferent fiber)
- descending pathways modify gain of reflex
Stretch reflex -
3
Hoffmann Reflex
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
- stimulate Ia afferents (and motor neurons)
- measure "M-wave" and "H-wave" using EMG
"Spinal shock" -• Complete absence of reflexes• Maybe from sudden withdrawal of
descending input
• Reflexes recover (weeks – months) and become oversensitive…
"Hyperactive" reflexes
Source: Latash, Neurophysiological Basis of Movement, Human Kinetics, 1998.
• ‘spasm-like' muscle bursts in response to mild stimuli
• loss of descending inhibition
tactile stim. foot
Increased resistance to stretch -• Velocity-dependent
hypertonia
Treatment -
- administration of baclofen to spinal cord
- GABA B receptor agonist
- inhibition of synapse between Ia fibers and motor neurons
Babinski’s Sign• stroking across plantar
surface of foot normally causes flexion of toes
• Upper motor neuron damage can reverse this response
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Summary of "UMN" Injury Effects
Source: Latash, Neurophysiological Basis of Movement, Human Kinetics, 1998.

4
Topic 8 – Motor Neuron Disorders & Spinal Cord Injury
1. Terminology
2. "Upper motor neuron" injury
3. Mechanisms of damage
4. Some disorders
Primary Injury –mechanical damage to neuronal apparatus
Secondary Injury –occurs over hours post-injury
Glutamate - Excitotoxicity
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
NMDA Receptor - GLU binds to R and opens Na+ channels
- ↑ Na+, draws water into the cell = edema
- ↑ Ca++ , activates proteases, lipases that degrade components of cell, may initiate apoptosis
Neuroprotective strategies
- block glutamate receptors
- antioxidants
- block Na+ channels
Na+ Channel Blockers
Adapted from: Schwartz and Fehlings, J. Neurosurg., 2001, 94(Suppl 2):245-256.
Weeks Post-Injury
Riluzole
Control
BBB = measure of locomotor function
Na+ Channel Blockers
Adapted from: Schwartz and Fehlings, J. Neurosurg., 2001, 94(Suppl 2):245-256.
• effects on integrity of descending spinal tracts

5
Na+ Channel Blockers – Tissue Loss
Source: Schwartz and Fehlings, J. Neurosurg., 2001, 94(Suppl 2):245-256.
Riluzole
Control
Wallerian Degeneration
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Axotomy - transection of the axon by cutting or crushing
Can result in degeneration of pre- / post-synaptic cells and glia.
Wallerian Degeneration
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Possible Therapies• Regeneration of damaged axons
• Remyelination – Schwann cell transplants
• Cell replacement – stem cells
Topic 8 – Motor Neuron Disorders & Spinal Cord Injury
1. Terminology
2. "Upper motor neuron" injury
3. Mechanisms of damage
4. Some disorders
Poliomyelitis
• poliovirus• acute infection of ventral horn of spinal cord• Selectively destroys lower motor neurons –
denervates muscleSource: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Loss of lower motor neuron cell bodies

6
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Poliomyelitis Amyotrophic Lateral Sclerosis (ALS)
- degeneration of "upper" and "lower" motor neurons
- neurogenic atrophy of muscles
- correlated with mutation in chromosome 21
Multiple Sclerosis
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Axonal Conduction Block• normally, voltage gated K+ channels
are present in the internodes and v-g Na+ channels are densely packed in region of node
• after demyelination, electrical properties of axon change
• Conduction slows or may become blocked
End of topic 8Topic 9 - Parietal Association Cortex
1. Sensory-to-motor transformations
2. Activity in parietal association cortex and the effects of damage

7
Sensory to Motor TransformationSensory information (visual, somatosensationetc.) is integrated and used to generate an appropriate motor output.
Culham and Kanwisher, (2001) Cur. Opinion in Neurobiol. 11: 157-163
Superior parietal lobule (SPL)
Inferior parietal lobule (IPL)
Intraparietal sulcus (IPS)
Posterior Parietal Cortex (PPC) association area
Anterior Posterior
- PPC is neither purely sensory nor purely motor ("association cortex")
- important for integration of sensory information
- sends information to motor areas (e.g. premotor and M1)
- important for "sensory-to-motor" transformation
PPC association area Topic 9 - Parietal Association Cortex
1. Sensory-to-motor transformations
2. Activity in parietal association cortex and the effects of damage
Parietal Association Cortex
Source: MacKay, Neuro 101, Sefalotek Ltd., 1999
- integrates information from several sensory modalities (e.g. V1 and S1)
Superior parietal lobule (SPL)
Scott, Sergio & Kalaska (1997) J. Neurophysiol. 78: 2413-2426
Cells have "preferred postures"
Natural position
Elbow raised
- Provides info about how body segments are positioned
8
Source: MacKay, Neuro 101, Sefalotek Ltd., 1999 Graziano et al. (2000) Science. 290: 1792.
Visual information is also important
General Take-Home Message!
PPC is involved in transforming sensory cues into info regarding- the locations of objects in the environment
- the location of our limbs in the environment
- relative location of body segments
helps provide a "reference frame" for the world around us.
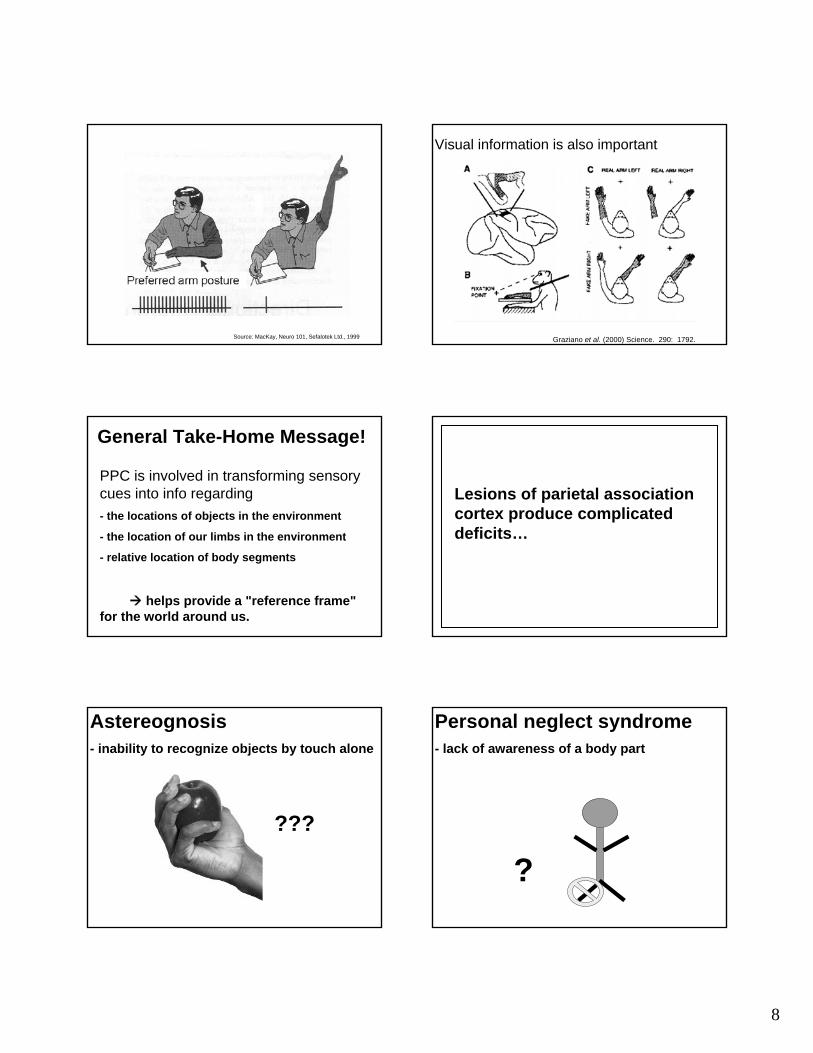
Lesions of parietal association cortex produce complicated deficits…
Astereognosis- inability to recognize objects by touch alone
???
Personal neglect syndrome - lack of awareness of a body part
?

9
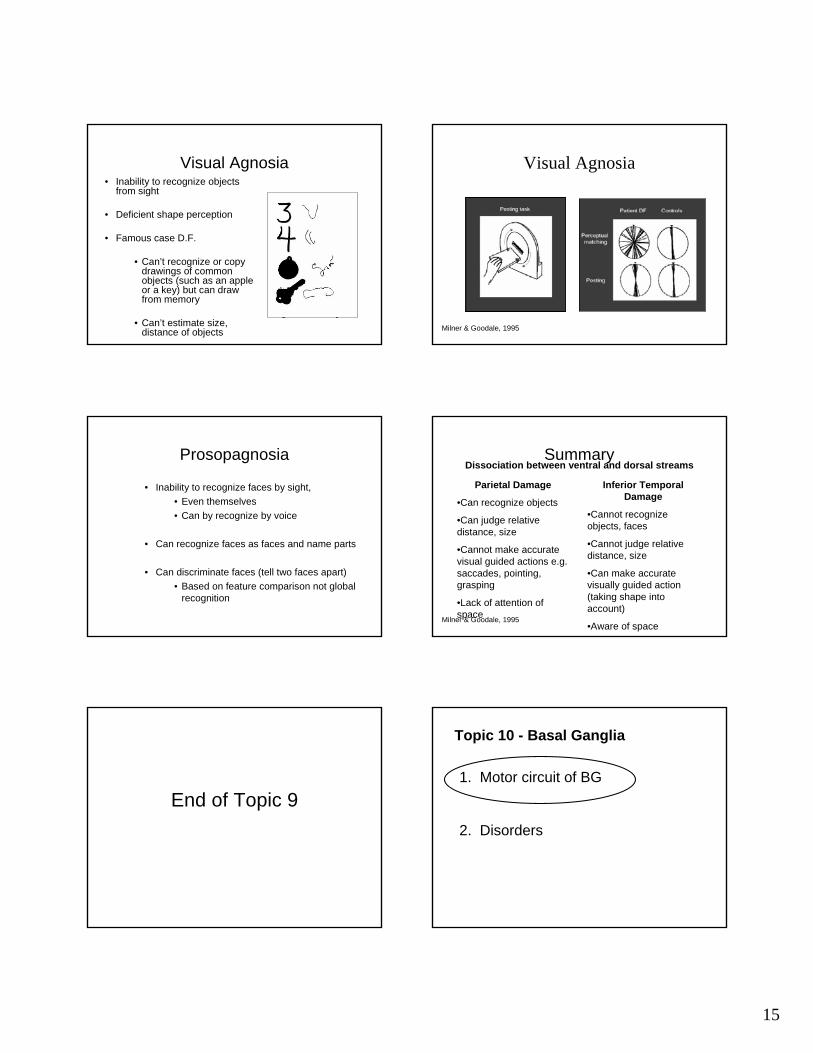
Optic Ataxia"dorsal" and "ventral" streams
Dorsal stream
Ventral stream
Primary visual area (V1)
Parietal lobe
Temporal lobe
Optic Ataxia
From: Perenin & Vighetto (1988) Brain. 111: 643-674
Optic Ataxia The inability to accurately reach for visible objects
Ideomotor Apraxia
Dorsal stream
Ventral stream
Primary visual area (V1)
Parietal lobe
Temporal lobe
?
Loss of ability to perform previously learned motor tasks
Disorders in Action and Perception
Dorsal vs. Ventral Streams
Milner & Goodale, 1995
Dorsal vs. Ventral Streams
10
•Visual control of motor output
•Absolute metrics
•Moment-to-moment computations
•‘Unconscious’
•Object identification
•Relational metrics
•Long term representation
•‘Conscious’
Goodale, MA & Humphrey, GK. (1998). Cognition
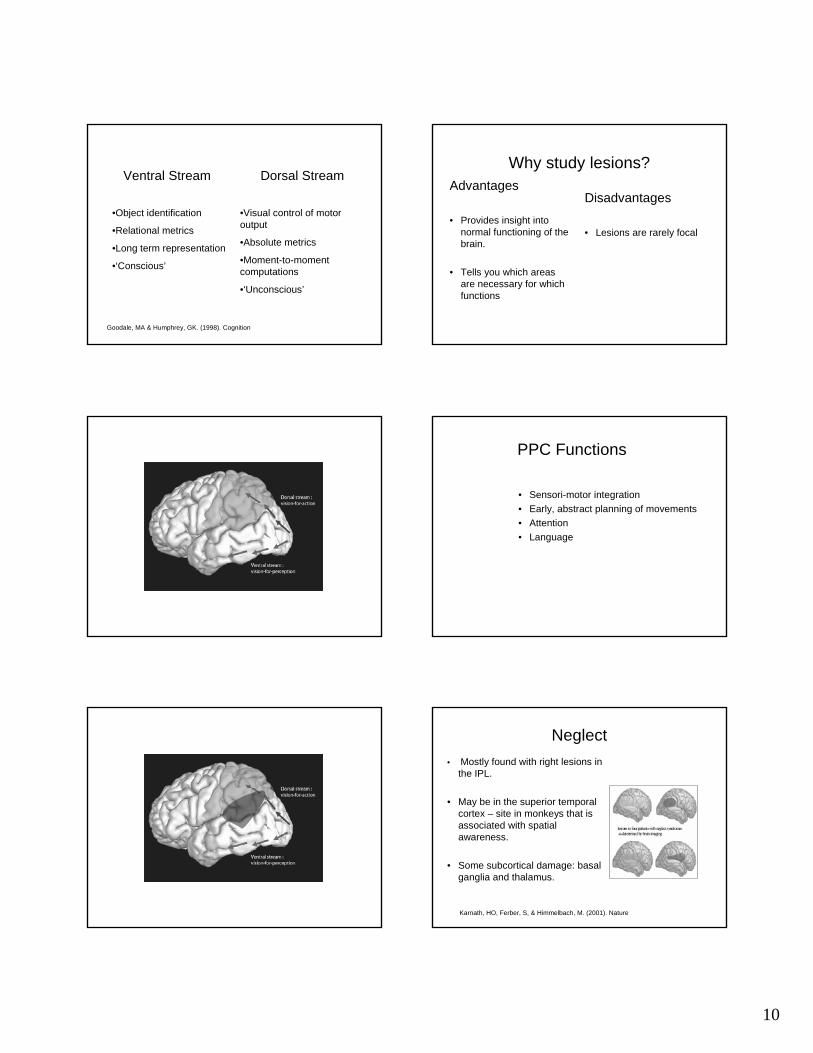
Ventral Stream Dorsal StreamWhy study lesions?
Disadvantages
• Lesions are rarely focal
Advantages
• Provides insight into normal functioning of the brain.
• Tells you which areas are necessary for which functions
PPC Functions
• Sensori-motor integration• Early, abstract planning of movements• Attention• Language
Neglect• Mostly found with right lesions in
the IPL.
• May be in the superior temporal cortex – site in monkeys that is associated with spatial awareness.
• Some subcortical damage: basal ganglia and thalamus.
Karnath, HO, Ferber, S, & Himmelbach, M. (2001). Nature

11
• Lack of awareness of personal and extra-personal space contralateral to lesioned hemisphere, e.g.
• patient may believe the left side of body is someone else’s.
• patient eats only the food in the right half of plate.• patient may only dress or shave on side.
Neglect Neglect
• Attention Deficits
Yves Rossetti, INSERM 534, France
Neglect
Yves Rossetti, INSERM 534, France
Neglect
Yves Rossetti, INSERM 534, France
• Visuo-motor deficits.
Neglect
Mattingley et al., Brain, 1992
• Visuo-motor deficits.
Neglect
Yves Rossetti, INSERM 534, France
12
Neglect
• Extinction• Anosognosia- The loss of recognition or awareness
of a disease.
• Most people with neglect are also unaware that they have the disorder.
Neglect
Balint’s syndrome
• Visuomotor and visuospatial disorders
• Bilateral damage to posterior parietal lobes
• Simultanagnosia – inability to interpret the visual field as a whole
• Ocular apraxia – deficit of visual scanning• Optic ataxia – inability to reach accurately under
visual guidance
Simultanagnosia
• Difficulty copying/drawing/writing because they can’t see the end of the pen and what is on the paper at the same time.
• Spatial disorientation: unable to discern spatial properties of objects e.g. distance and size.
• Difficulty describing complex scenes (eg. Boston cookie theft)
Simultanagnosia

13
Ocular Apraxia
• Impaired visual scanning (moving the eyes voluntarily)
• Not an oculomotor deficit
• Reflexive movements are spared
• Eye movements toward auditory stimuli are spared
• Gaze restricted to narrow band, right of midline (similar to neglect)
Ocular Apraxia
Apraxic eye movementsNormal eye movements
Optic Ataxia
• Visuomotor deficits - errors in visually-guided movements
• No other perceptual or motor deficits
• Two types of optic ataxia patients
Unilateral Optic Ataxia Bilateral Optic AtaxiaOptic Ataxia
Unilateral Optic AtaxiaOptic Ataxia
Vighetto, 1980
Ataxic Hand
Healthy Hand
Healthy Field Ataxic Field
Unilateral Optic Ataxia

14
Revol et al., 2003
Unilateral Optic AtaxiaBilateral Optic AtaxiaOptic Ataxia
Jeannerod, 1986. Neuropsychologia.
Bilateral Optic Ataxia
Milner et al., 1999; 2001; 2003
0 60 120 180 2400
60
120
180
240
300
0 60 120 180 2400
60
120
180
240
300
Optic Ataxia PatientControl
Immediate
0 60 120 180 2400
60
120
180
240
300
0 60 120 180 2400
60
120
180
240
300
Delayed
Bilateral Optic Ataxia
IT Functions
• Object perception, recognition, memory
• Face perception
15
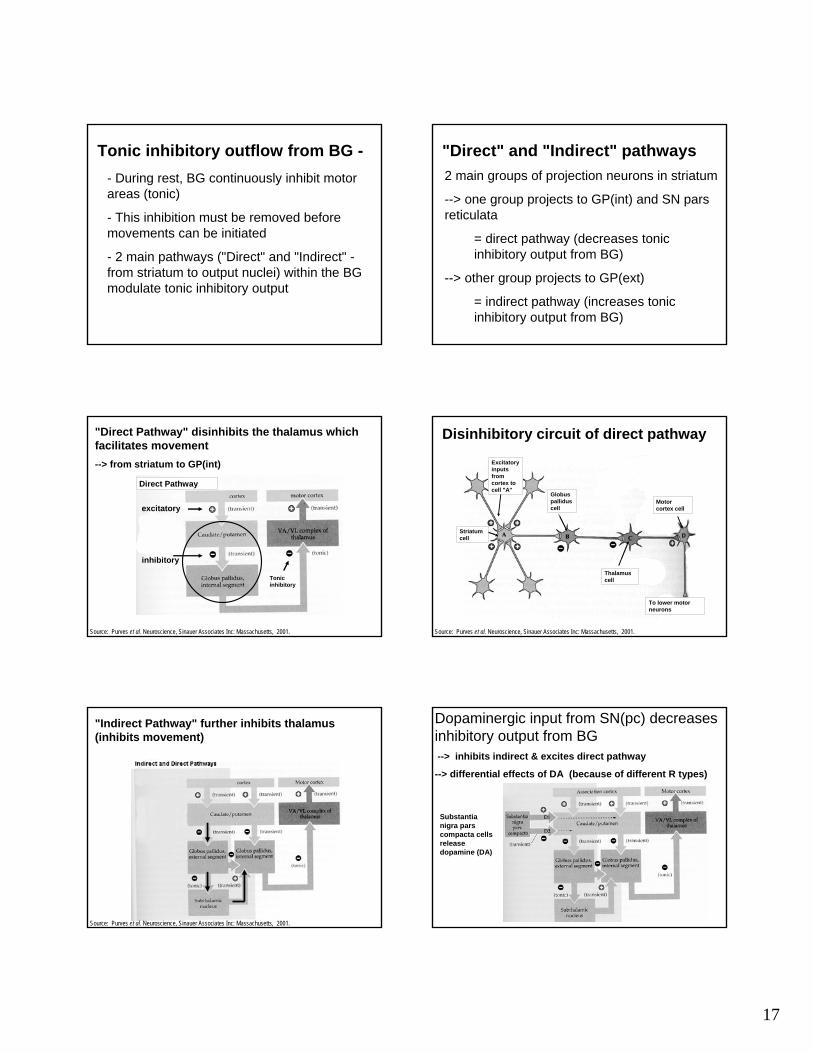
Visual Agnosia• Inability to recognize objects
from sight
• Deficient shape perception
• Famous case D.F.
• Can’t recognize or copy drawings of common objects (such as an apple or a key) but can draw from memory
• Can’t estimate size, distance of objects Milner & Goodale, 1995
Visual Agnosia
Prosopagnosia
• Inability to recognize faces by sight,• Even themselves• Can by recognize by voice
• Can recognize faces as faces and name parts
• Can discriminate faces (tell two faces apart)• Based on feature comparison not global
recognition
SummaryDissociation between ventral and dorsal streams
Inferior Temporal Damage
•Cannot recognize objects, faces
•Cannot judge relative distance, size
•Can make accurate visually guided action (taking shape into account)
•Aware of space
Parietal Damage
•Can recognize objects
•Can judge relative distance, size
•Cannot make accurate visual guided actions e.g. saccades, pointing, grasping
•Lack of attention of spaceMilner & Goodale, 1995
End of Topic 9
Topic 10 - Basal Ganglia
1. Motor circuit of BG
2. Disorders

16
The Basal Ganglia- group of subcortical nuclei (4 main parts)
- influence movement by modulating activity in "upper motor neurons"
Source:http://cti.itc.virginia.edu/~psyc220
(partially cut-away to reveal underlying structures)
1. Striatum(caudate and putamen),
2. GlobusPallidus (external and internal segments),
3. Substantianigra (pars compacta and pars reticulata),
4. Subthalamicnucleus
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Input to Basal Ganglia -From most of cerebral cortex (and other regions)--> to striatum - i.e caudate and putamen (main input areas)
Output from Basal GangliaTo motor areas via the thalamus--> from GlobusPallidus (int.) and
To eye mvtareas of brainstem--> from substantia nigra(pars reticulata)
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Motor cortex
Caudate
Thalamus
Subthalamicnucleus
Substantia nigrapars reticulata
GP -intGP -ext
Putamen Superior colliculus
• Multiple loops between cortex and basal ganglia -
1. Motor - voluntary movements1. 2. Limbic - "emotional behaviour"2. 3. Executive - "cognitive processes"
BG Circuits
• Involved in initiation of voluntary movements
• motor circuit has a general somatotopic organization throughout projections
Motor Circuit
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
SMA – supplementary motor area; PMC – premotor cortex; MC – motor cortex GPe/GPi – globus pallidusexternal/internal segmentsSTN – subthalamic nucleusVLo/VApc/CM – thalamic nuclei
Tonic inhibitory outflow from BG -- During rest, BG continuously inhibit motor areas (tonic)
Motor cortex
Caudate
Thalamus
Subthalamicnucleus
Substantia nigrapars reticulata
GP -intGP -ext
Putamen Superior colliculus
17
Tonic inhibitory outflow from BG -- During rest, BG continuously inhibit motor areas (tonic)
- This inhibition must be removed before movements can be initiated
- 2 main pathways ("Direct" and "Indirect" -from striatum to output nuclei) within the BG modulate tonic inhibitory output
"Direct" and "Indirect" pathways2 main groups of projection neurons in striatum
--> one group projects to GP(int) and SN pars reticulata
= direct pathway (decreases tonic inhibitory output from BG)
--> other group projects to GP(ext)
= indirect pathway (increases tonic inhibitory output from BG)
Direct Pathway
"Direct Pathway" disinhibits the thalamus which facilitates movement--> from striatum to GP(int)
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
inhibitory
excitatory
Tonic inhibitory
Excitatory inputs from cortex to cell "A"
Striatum cell
Globuspalliduscell
Thalamus cell
Motor cortex cell
To lower motor neurons
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Disinhibitory circuit of direct pathway
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
"Indirect Pathway" further inhibits thalamus (inhibits movement)
Dopaminergic input from SN(pc) decreases inhibitory output from BG--> inhibits indirect & excites direct pathway
--> differential effects of DA (because of different R types)
Substantianigra pars compacta cells release dopamine (DA)

18
Topic 10 - Basal Ganglia
1. Motor circuit of BG
2. Disorders
Hypokinesia- decrease in the amount and speed of movements
Hyperkinesia- unwanted movements
Normal
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehab. Saunders, 2002
Parkinson's Disease
PD
- Cell death in substantia nigra(unknown cause)
- Loss of dopamine
- Disrupts normal modulations of BG output
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Parkinson's Disease
Parkinson Disease
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• Loss of dopamine-producing cells in SNc
– - Akinesia – difficulty initiating movement voluntarily
– - Bradykinesia – once started, movements very slow
– - Resting tremor in distal limbs (4-6 Hz) from oscillator properties of pallidal cells
• Loss of acetylcholine-producing cells in pedunculopontine nucleus
– - Rigidity - unable to inhibit reticulospinal and vestibulospinal tracts
PD Treatments - Pallidotomy
19
PD Treatments - STN lesion PD Treatments - L-DOPA (Dopamine precursor)
Increase DA levels
Source: http://web.sfn.org/content/Publications/BrainBriefings/
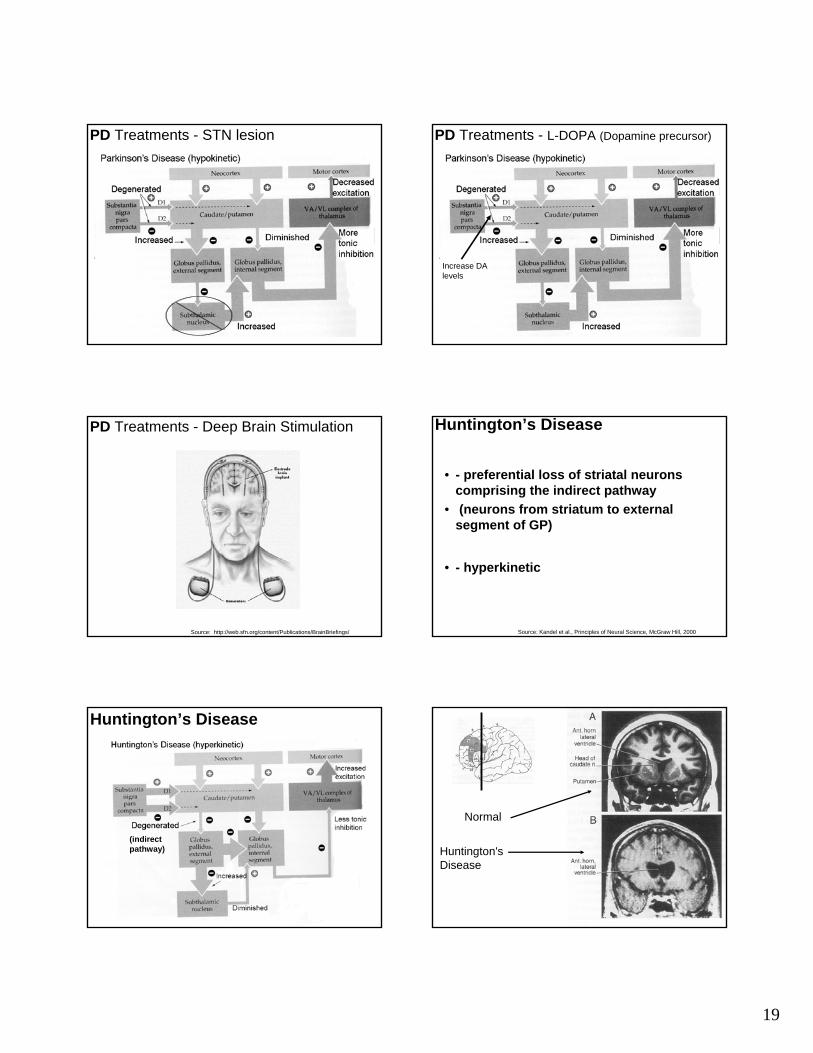
PD Treatments - Deep Brain Stimulation Huntington’s Disease
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• - preferential loss of striatal neurons comprising the indirect pathway
• (neurons from striatum to external segment of GP)
• - hyperkinetic
(indirect pathway)
Huntington’s Disease
Normal
Huntington's Disease

20
Hemiballism
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• uncontrolled, involuntary flinging of limbs on side contralateral to lesion
• STN lesion - stroke
• ↓ output of Gpi
End of Topic 10
1. Theories of Function
2. Neuroanatomy
3. Basic circuitry and dysfunction
Topic 11 – Cerebellum
Cerebellum
Cerebellum - Introduction
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Cerebellum - Introduction
• Approx 10% of total brain volume– But contains about half of brain's neurons!
• Can remove cerebellum without loss of perception or muscle weakness.
• Regulates movement indirectly by adjusting output of major descending motor systems
Cerebellum - Multiple Roles in Voluntary Movement
- Timing and spatial accuracy of movements
- Motor learning•– acquisition new motor skills
- "Comparator" •– compares sensory feedback with intended movement (receives a copy of the intended "motor plan" in the form of "efferencecopy").

21
Cerebellum- basic connectivity
Premotor, motor, somatosensory, PPC
1. Theories of Function
2. Neuroanatomy
3. Basic circuitry and dysfunction
Topic 11 – Cerebellum
Anatomy
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• 2 hemispheres divided by vermis• 3 lobes – anterior, posterior, flocculonodular• Cerebellar cortex over white matter
Vermis
Anterior
Posterior
Cerebellar hemisphere
• Superior – output to cortex via thalamus
• Middle – input / output via pons
• Inferior – input / output with brain stem / spinal cord
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
AnatomyConnected to brain stem through 3 peduncles
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Anatomy3 pairs of deep cerebellar nuclei
1. Fastigial
2. Interposed (globose and emboliform)
3. Dentate
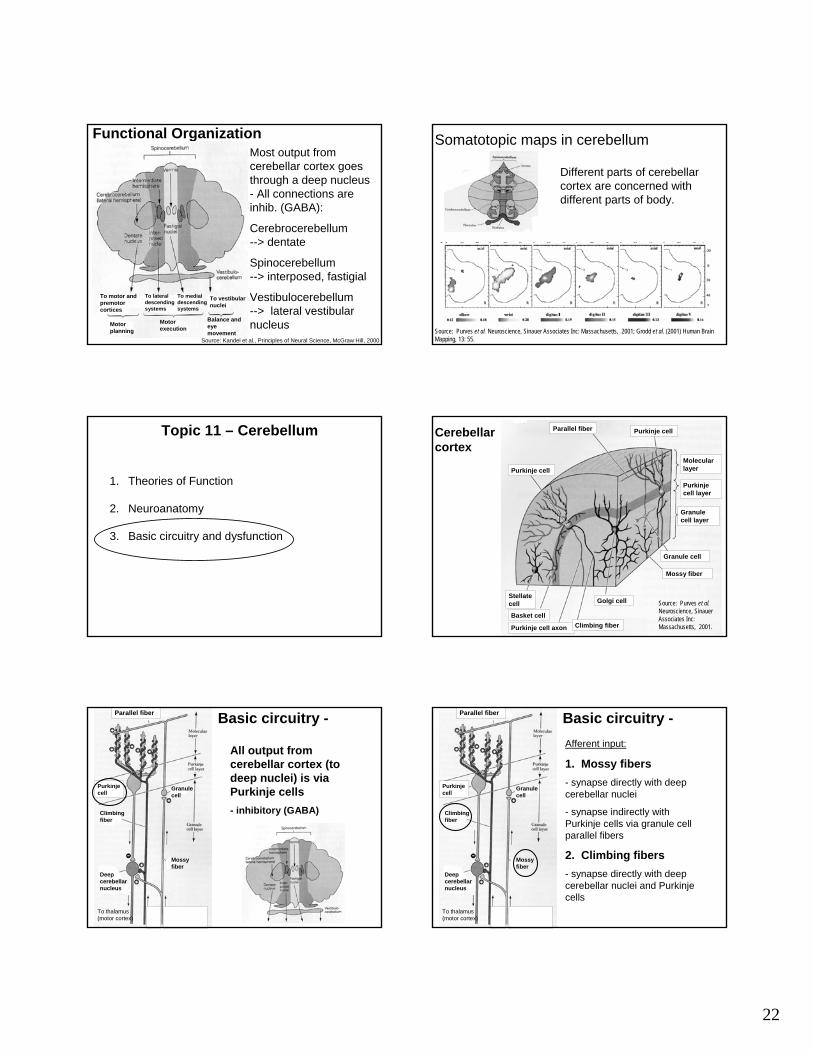
Functional Organization
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Spinocerebellum (vermis and intermediate)
Cerebrocerebellum(lateral hemisphere)
Vestibulocerebellum(flocculonodular lobe)
22
Functional OrganizationMost output from cerebellar cortex goes through a deep nucleus - All connections are inhib. (GABA):
Cerebrocerebellum --> dentate
Spinocerebellum --> interposed, fastigial
Vestibulocerebellum --> lateral vestibular nucleus
To motor and premotor cortices
To lateral descending systems
To medial descending systems
To vestibular nuclei
Balance and eye movement
Motor execution
Motor planning
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
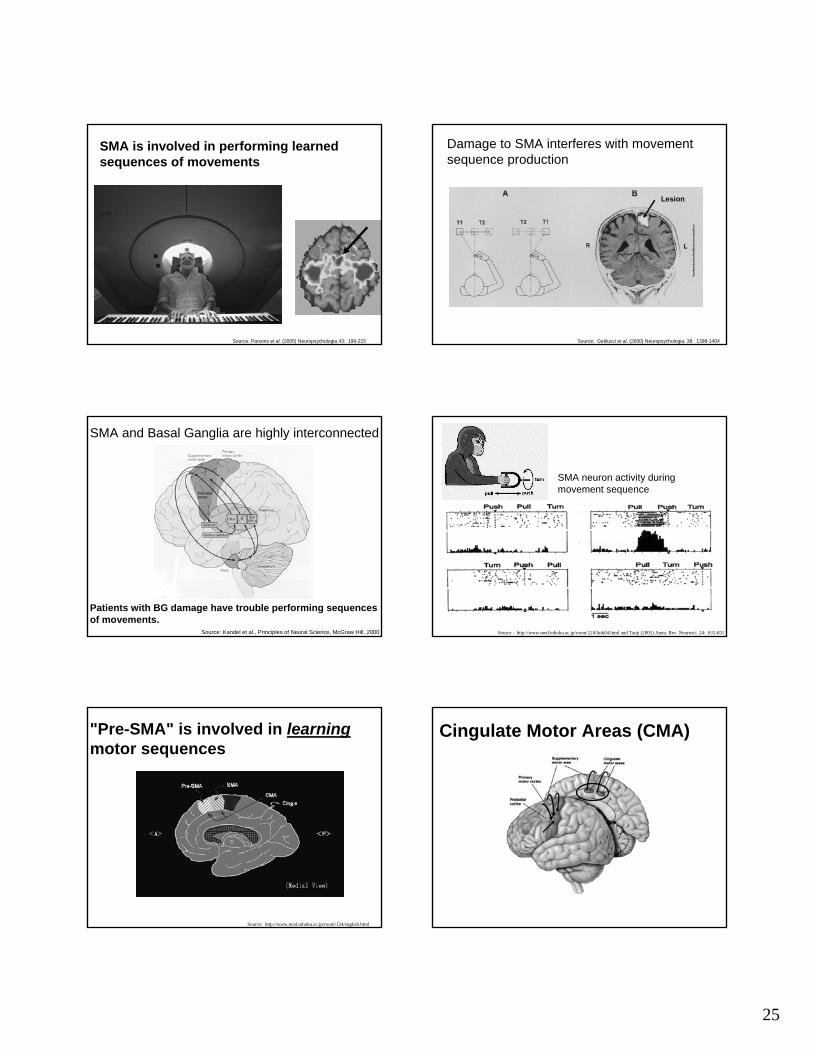
Somatotopic maps in cerebellum
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001; Grodd et al. (2001) Human Brain Mapping, 13: 55.
Different parts of cerebellar cortex are concerned with different parts of body.
1. Theories of Function
2. Neuroanatomy
3. Basic circuitry and dysfunction
Topic 11 – Cerebellum
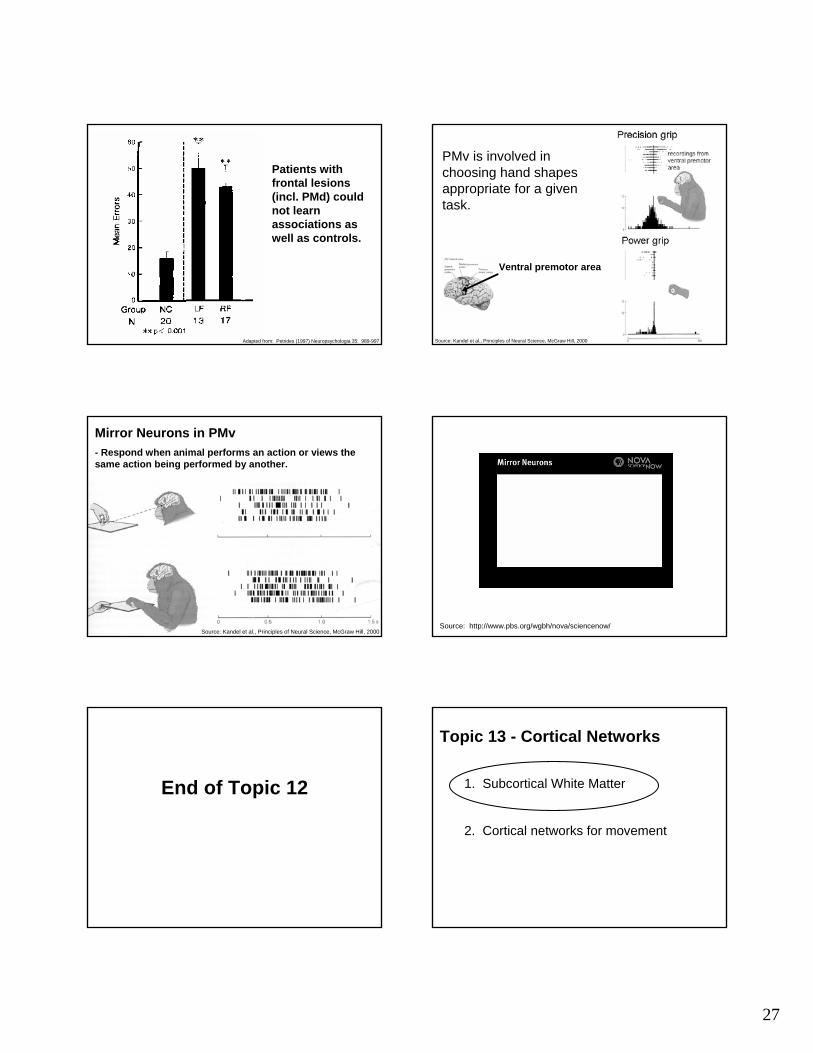
Stellate cell
Basket cell
Purkinje cell axon Climbing fiber
Golgi cell
Mossy fiber
Granule cell
Granule cell layer
Purkinje cell layer
Molecular layer
Purkinje cellParallel fiber
Purkinje cell
Source: Purves et al.Neuroscience, SinauerAssociates Inc: Massachusetts, 2001.
Cerebellar cortex
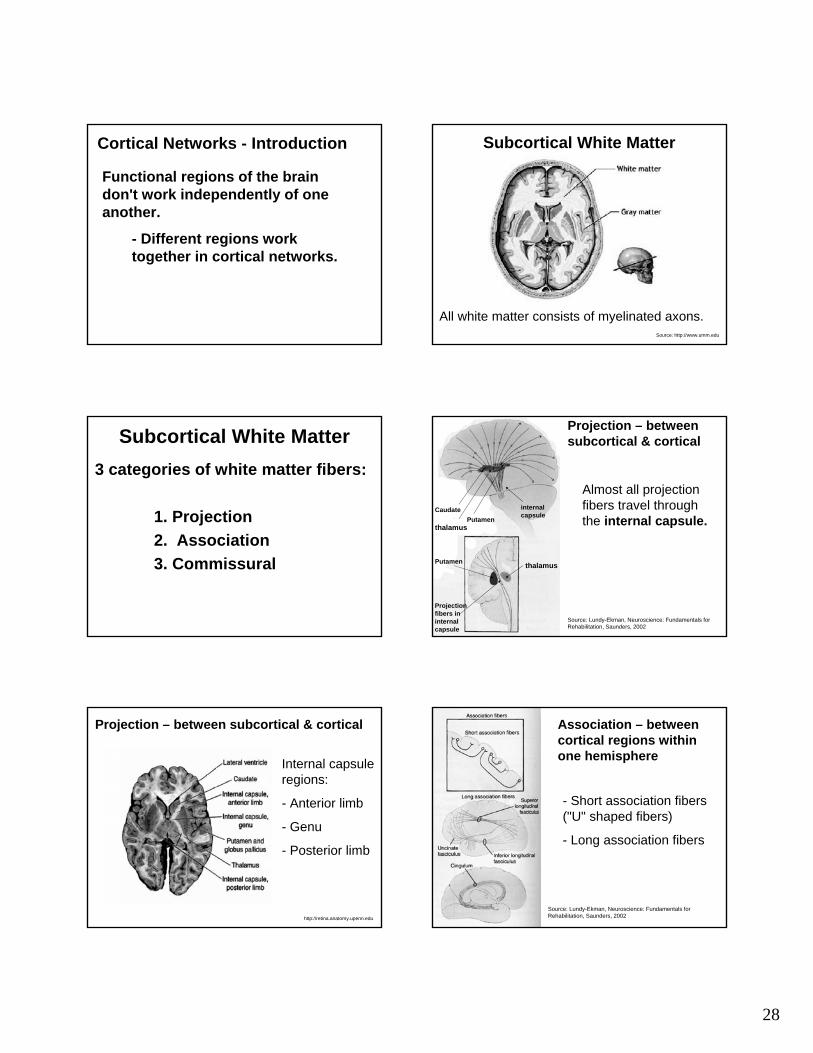
Basic circuitry -Parallel fiber
Purkinje cell
Granule cell
Mossy fiber
Climbing fiber
Deep cerebellar nucleus
To thalamus (motor cortex)
All output from cerebellar cortex (to deep nuclei) is via Purkinje cells- inhibitory (GABA)
Basic circuitry -Parallel fiber
Purkinje cell
Granule cell
Mossy fiber
Climbing fiber
Deep cerebellar nucleus
To thalamus (motor cortex)
Afferent input:
1. Mossy fibers - synapse directly with deep cerebellar nuclei
- synapse indirectly with Purkinje cells via granule cell parallel fibers
2. Climbing fibers- synapse directly with deep cerebellar nuclei and Purkinje cells

23
Complex / Simple Spikes
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• Mossy Fibers –result in simple spikes
• Climbing Fibers –result in complex spikes
(Intracellular recordings from Purkinje cells)
Interneurons modulate inhibitory activity of P-cells
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
- Golgi cells - stellate cells - basket cells
This "Basic circuit" is repeated throughout the cerebellum.
Purkinje Cells as "Relaxation Couplers"
Circuitry enables temporal control of output(i.e. Coordination) Source: MacKay, Neuro 101, Sefalotek Ltd., 1999 Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000 Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
• lack of coordination among limb / body segments
Cerebellar Ataxia

24
End of Topic 11
Topic 12 - Premotor Cortex
1. General
2. Medial regions
3. Lateral regions
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
- a set of interconnected areas in the frontal lobe (rostral to M1)
- divided into "lateral" and "medial" regions
Premotor CortexPremotor areas - Introduction
- Concerned with planning movements
- active during preparation of movement
- uses info from other regions to select movements appropriate to context of a required action
- extensive connections with M1 and direct projections to spinal cord
Topic 12 - Premotor Cortex
1. General
2. Medial regions
3. Lateral regions
Medial premotor areas- Supplementary motor area (SMA) - Cingulate motor areas (CMA)
Source: http://www.driesen.com/secondary_motor_cortex.htm
25
Source: Parsons et al. (2005) Neuropsychologia 43: 199-215
SMA is involved in performing learned sequences of movements
Damage to SMA interferes with movement sequence production
Source: Getilucci et al. (2000) Neuropsychologia. 38: 1398-1404
Lesion
SMA and Basal Ganglia are highly interconnected
Patients with BG damage have trouble performing sequences of movements.
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000 Source : http://www.med.tohoku.ac.jp/room/124/link04.html and Tanji (2001) Annu. Rev. Neurosci. 24: 631-651
SMA neuron activity during movement sequence
"Pre-SMA" is involved in learning motor sequences
Source: http://www.med.tohoku.ac.jp/room/124/english.html
Cingulate Motor Areas (CMA)

26
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002Source: Morecraft & Van Hoesen (1998) Brain Res. Bulletin. 45: 209-232
CMA may be involved in the "emotional" aspects of movements
Topic 12 - Premotor Cortex
1. General
2. Medial regions
3. Lateral regions
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Dorsal premotor (PMd)
Ventral premotor (PMv)
Lateral Premotor Cortex
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Medial areas - internally initiated movementsLateral areas - externally cued movements
Dorsal premotor area (PMd) - Involved in learning associations between a particular sensory input and a specific motor output. - Role in selection of action based on learned associations.
e.g. red = stop
Source: Petrides (1997) Neuropsychologia 35: 989-997
Subjects had to learn correct associations between different colour cues and hand postures.
27
Patients with frontal lesions (incl. PMd) could not learn associations as well as controls.
Adapted from: Petrides (1997) Neuropsychologia 35: 989-997
PMv is involved in choosing hand shapes appropriate for a given task.
Ventral premotor area
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Mirror Neurons in PMv- Respond when animal performs an action or views the same action being performed by another.
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000Source: http://www.pbs.org/wgbh/nova/sciencenow/
End of Topic 12
Topic 13 - Cortical Networks
1. Subcortical White Matter
2. Cortical networks for movement
28
Functional regions of the brain don't work independently of one another.
- Different regions work together in cortical networks.
Cortical Networks - Introduction
Source: http://www.umm.edu
Subcortical White Matter
All white matter consists of myelinated axons.
Subcortical White Matter3 categories of white matter fibers:
1. Projection 2. Association3. Commissural
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Projection – between subcortical & cortical
thalamusPutamen
Projection fibers in internal capsule
thalamusPutamen
Caudate
Almost all projection fibers travel through the internal capsule.
internal capsule
Projection – between subcortical & cortical
http://retina.anatomy.upenn.edu
Internal capsule regions:
- Anterior limb
- Genu
- Posterior limb
Association – between cortical regions within one hemisphere
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
- Short association fibers ("U" shaped fibers)
- Long association fibers
29
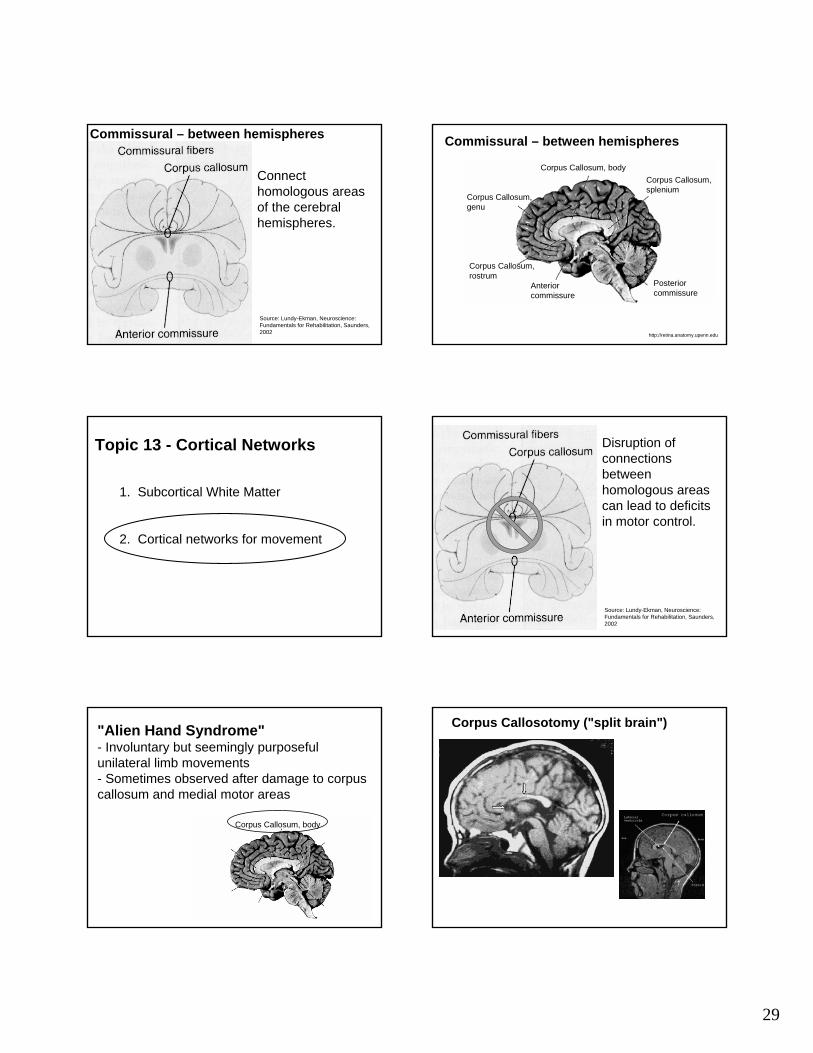
Commissural – between hemispheres
Connect homologous areas of the cerebral hemispheres.
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002 http://retina.anatomy.upenn.edu
Commissural – between hemispheres
Corpus Callosum, body
Corpus Callosum, genu
Corpus Callosum, splenium
Posterior commissure
Anterior commissure
Corpus Callosum, rostrum
Topic 13 - Cortical Networks
1. Subcortical White Matter
2. Cortical networks for movement
Disruption of connections between homologous areas can lead to deficits in motor control.
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
"Alien Hand Syndrome"- Involuntary but seemingly purposeful unilateral limb movements - Sometimes observed after damage to corpus callosum and medial motor areas
Corpus Callosum, body
Corpus Callosotomy ("split brain")

30
Source: Giovannetti et al. (2005) Neuropsychologia. 43: 75-88
leftright
6 months post-stroke: - left medial frontal lesion extending into corpus callosum
The "Dual Premotor systems" Hypothesis:
Source: Goldberg & Bloom (1990) Am. J. Phys. Med. Rehabil. 69: 228-238.
Lateral Premotor regions
- externally cued movements
Medial Premotor regions
- internally-generated movementsAlien Hand Syndrome may result from
imbalance between lateral and medial premotor systems
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Medial areas - internally initiated movementsLateral areas - externally cued movements
(Slide from "Topic 12" lecture)
"Left hand apraxia" after CC lesion
- Can't pantomime object use from verbal command or visual presentation of object.
Lateralization of function (ie. localization of a function to the left or right side of brain) could be a factor in production of this deficit.
Evidence of Lateralization in Motor Areas
Left M1 Right M1
Amount of activity (pixels)
C = contralateral (I.e. hand on opposite side of body)
I = ipsilateral (I.e. hand on same side of body)
= left-handed
= right-handed
e.g. M1
Adapted from: Kim et al. (1993) Science. 261: 615-617.
Lateralization of function in M1 -
- Right M1 is mainly activated during movement of left hand
- Left M1 is activated during movement of either hand
(regardless of handedness)

31
Other examples of lateralization in motor regions -
- Left-brain dominance for motor planning?
- Lateralization during performance of complex sequences in premotor and parietal regions?
Sources: Sabate et al. (2004) Neuropsychologia. 42: 1041-1049; Haaland et al. (2004) J. Cogn. Neurosci. 16: 621-636 Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Parieto-Frontal Connections
Importance of Parieto-Frontal Connections
• Premotor regions select behaviours and muscle synergies based on information supplied by posterior half of the brain
– this info is used by premotor regions to relate target to body position in order to act on it
premotor regions also integrate cognitive information (last lecture), rules for movement
Adapted from: Cavada (2001) NeuroImage. 14: S21-S26.
Regions within the Intraparietal Sulcus (IPS)
VIP = ventral intraparietal area
MIP = medial intraparietal area
AIP = anterior intraparietal area
LIP = lateral intraparietal area
Parietal lobe
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Anterior Intraparietal region -
Source: Murata et al (2000) J. Neurophysiol. 83: 2580-2601.
AIP neuron activity varies depending on object grasped.- Neurons "prefer" some shapes to others.

32
Anterior Intraparietal region -
Source: Murata et al (2000) J. Neurophysiol. 83: 2580-2601.
Some AIP neurons respond to purely visual info.
Anterior Intraparietal region -
Source: Murata et al (2000) J. Neurophysiol. 83: 2580-2601.
Examples of highly selective "object-type visual-dominant" AIP neurons during visual fixation of different objects.
PMv might use info about size, shape and orientation of objects from AIP to choose hand shapes appropriate for a given task.
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Areas active in human brain during object manipulation.
Source: Binkofski et al. (1999) Exp. Brain Res. 128: 210-213 .
PMv
Anterior region of IPS
Human Anterior Intraparietal region also responds to pictures of "graspable" objects
(hammer, house, lion, face)
Source: Chao & Martin (2000) NeuroImage. 12: 478-484.Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000

33
Scott, Sergio & Kalaska (1997) J. Neurophysiol. 78: 2413-2426 Scott, Sergio & Kalaska (1997) J. Neurophysiol. 78: 2413-2426
- MIP / area 5 provides info about how body segments are positioned (cells have "preferred postures")
- PMd might use info about current posture from MIP neurons to plan movements
The nervous system must also deal with ‘higher order’ relationships
PMd cells are active during the delay period when the rules are needed to make the appropriate
movement to a given cue (discussed last lecture)
Biomechanical / kinetic information provided in primary motor area
Complex force/emg profile
34
Parietal (area 5) cells vs. MI
cells
Sergio, L. E. et al. J Neurophysiol 94: 2353-2378 2005
Reflects emg/force profiles
Doesn’t reflect emg/force profiles
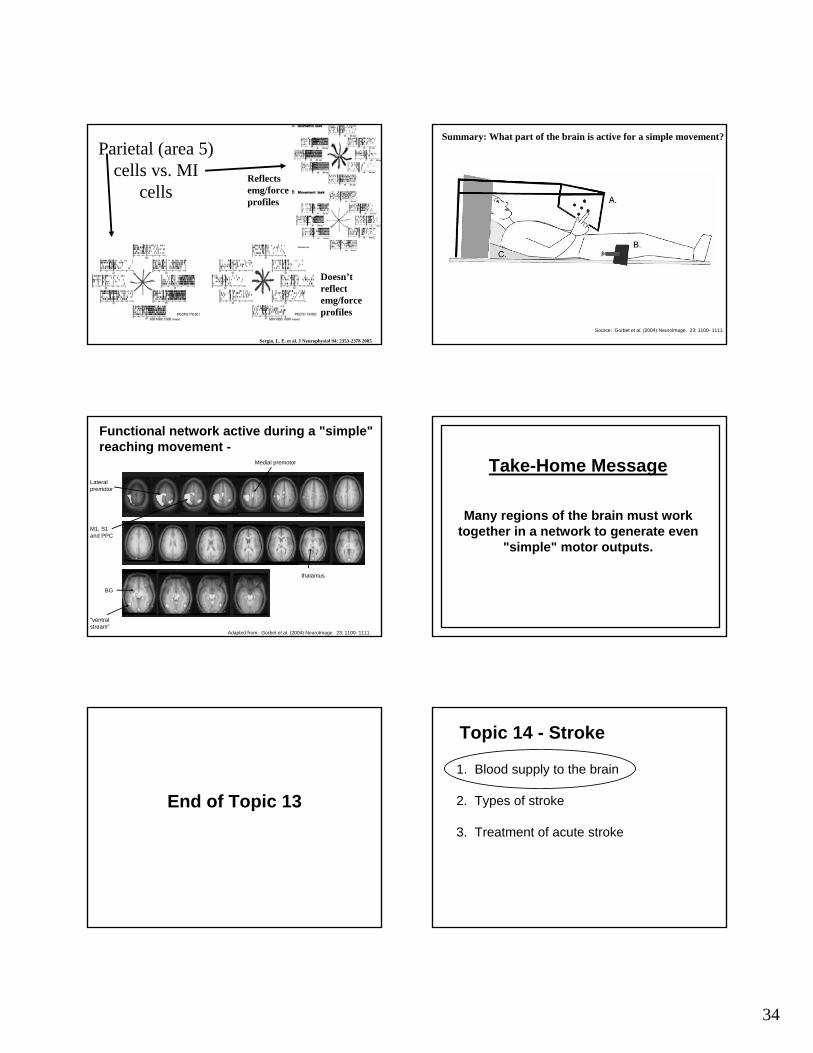
Source: Gorbet et al. (2004) NeuroImage. 23: 1100- 1111.
Summary: What part of the brain is active for a simple movement?
Functional network active during a "simple" reaching movement -
"ventral stream"
BG
thalamus
Lateral premotor
Medial premotor
M1, S1 and PPC
Adapted from: Gorbet et al. (2004) NeuroImage. 23: 1100- 1111.
Take-Home Message
Many regions of the brain must work together in a network to generate even
"simple" motor outputs.
End of Topic 13
Topic 14 - Stroke
1. Blood supply to the brain
2. Types of stroke
3. Treatment of acute stroke
35
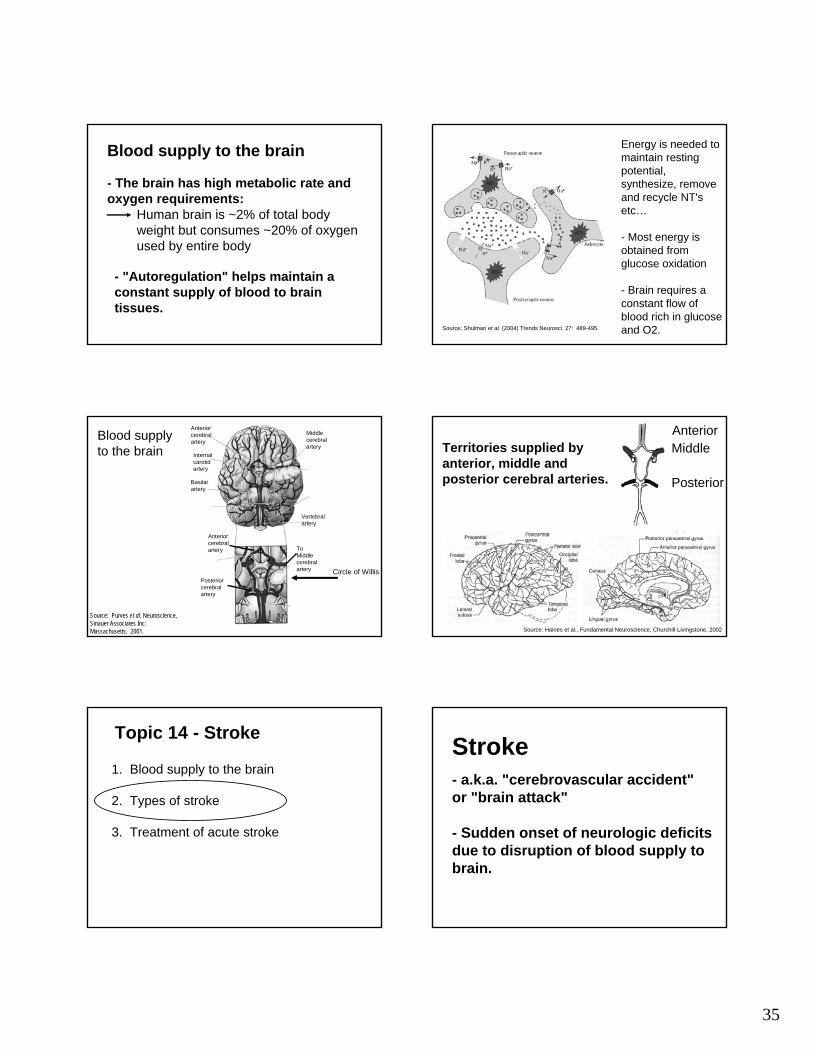
Blood supply to the brain
- The brain has high metabolic rate and oxygen requirements:
Human brain is ~2% of total body weight but consumes ~20% of oxygen used by entire body
- "Autoregulation" helps maintain a constant supply of blood to brain tissues.
Source: Shulman et al. (2004) Trends Neurosci. 27: 489-495.
Energy is needed to maintain resting potential, synthesize, remove and recycle NT's etc…
- Most energy is obtained from glucose oxidation
- Brain requires a constant flow of blood rich in glucose and O2.
Anterior cerebral artery
Internal carotid artery
Basilar artery
Middle cerebral artery
Vertebral artery
Anterior cerebral artery
Posterior cerebral artery
To Middle cerebral artery Circle of Willis
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
Blood supply to the brain
Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
AnteriorMiddle
Posterior
Territories supplied by anterior, middle andposterior cerebral arteries.
Topic 14 - Stroke
1. Blood supply to the brain
2. Types of stroke
3. Treatment of acute stroke
Stroke- a.k.a. "cerebrovascular accident" or "brain attack"
- Sudden onset of neurologic deficits due to disruption of blood supply to brain.

36
STROKE - StatisticsDeaths• 4th leading cause of death in Canada• approx. 16,000 Canadians die each
year
Prevalence• 40,000-50,000 strokes in Canada each
year (500,000 in US)• approx every 10-12 minutes
STROKE
1) Ischemic - Blockage of a blood
vessel caused by a blood clot
2 major causes of a stroke:
Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
Source: http://www.stjohn.org
Region of decreased blood flow
Interruption of blood supply (blood clot)
Ischemic Stroke
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Lacunar Infarcts
2) Hemorrhagic- rupture of a blood vessel
Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
STROKE 2 major causes of a stroke:
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002
Hemorrhagic Stroke

37
Watershed Lesions
Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
Source: Lundy-Ekman, Neuroscience: Fundamentals for Rehabilitation, Saunders, 2002Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
"Umbra" region (ischemic core)
"Penumbra" region (surrounding region)
Neural Effects1. Energy failure -
• Ischemia (deficiency in blood flow) results in hypoxia (deficiency in oxygen) and decreased glucose availability.
Source: Shulman et al. (2004) Trends Neurosci. 27: 489-495.
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
Na+/K+ pump requires ATP to maintain resting potential.
extracellularintracellular
Within 5 min of ischemia, extracellular glutamate ↑ ~8x.
Neural Effects
2) Excitotoxicity - excessive exposure to glutamate may kill neurons
Neural Effects
Transport of glutamate out of synaptic cleft
Astrocyte glutamine
glutamate
Source: MacKay, Neuro101, Sefalotek Ltd., 1999
Glutamate - Excitotoxicity
Source: Kandel et al., Principles of Neural Science, McGraw Hill, 2000
NMDA Receptor - ↑ Na+, draws water into the cell
- Changes in cell volume can lead to osmotic lysis(particularly in umbra region)
- ↑ Ca++ , activates proteases, lipases that degrade components of cell, may initiate apoptosis

38
Stroke outcome depends on regions effected -
Source: Haines et al., Fundamental Neuroscience, Churchill-Livingstone, 2002
Topic 14 - Stroke
1. Blood supply to the brain
2. Types of stroke
3. Treatment of acute stroke
Treatment of acute stroke
Decreased blood flow in areas supplied by posterior cerebral artery.
Intracranial hemorrhaging.
Thrombolytics – dissolve clots– Tissue Plasminogen Activator (t-PA)– ~ 3 hour time window– 33% more likely to recover from stroke with
little or no disability– Risks include hemorrhage
Acute Treatment for Ischemic Stroke
TIME IS BRAIN!!!!
Acute Treatment
Neuroprotective strategies -
- Glutamate antagonists
- Ca++ and Na+ blockers
- Antioxidants (scavengers of free radicals)
May extend time window for thrombolytics.
Hypothermia as a Neuroprotective strategy?
Source: Kammersgaard et al. (2000) Stroke. 31: 2251-2256.
- Lowered body temperature by 1.3 degrees Celsius during acute phase of stroke
- Patients who were cooled were 2x more likely to survive 6 months post-stroke

39
Hypothermia may decrease infarct volumeInfarct volume after thromboembolic stroke
Thrombolysis Hypothermia Thrombolysis and Hypothermia
Source: Kollmar et al. (2004) Exper. Neurol. 190: 204-212.
End of Topic 14 Topic 15 - Recovery from Stroke
Motor Recovery Post-Stroke - Spontaneous
Source: Duncan et al., Neuropharm., 39:835-841, 2000.

40
Recovery Post-StrokeAt least 3 separate but interactive
processes associated with recovery
1) Resolution of diaschisis, inflammation etc..
2) Behavioural compensation
3) Neuroplasticity
Recovery Post-StrokeAt least 3 separate but interactive
processes associated with recovery
1) Resolution of diaschisis, inflammation etc..
2) Behavioural compensation
3) Neuroplasticity
- Loss of function in remote areas anatomically connected to region of lesion
Diaschisis
- Possibly from disruption of afferent excitatory input from lesioned area to other brain regions.
Diaschisis
Adapted from: Gold and Lauritzen (2002). Proc. Natl. Acad. Sci. 99: 7699-7704
Some initial improvement also likely corresponds to resolution of tissue inflammation.
- early stage inflammation starts a few hours after onset of ischemia
- microglia and leukocyte involvement
Motor Recovery Post-Stroke - Spontaneous
Source: Duncan et al., Neuropharm., 39:835-841, 2000.

41
Recovery Post-StrokeAt least 3 separate but interactive
processes associated with recovery
1) Resolution of diaschisis, inflammation etc..
2) Behavioural compensation
3) Neuroplasticity
Behavioural compensation
e.g. - Use unaffected arm
- Learn to walk with a cane
Recovery Post-StrokeAt least 3 separate but interactive
processes associated with recovery
1) Resolution of diaschisis, inflammation etc..
2) Behavioural compensation
3) Neuroplasticity
Mechanisms of NeuroplasticityImplicated in Stroke Recovery
1) Redundancy – alternate pathways take over lost function
2) Unmasking - activation of normally inhibited pathways
3) Long-term potentiation - increasing efficiency of synaptic connections and formation of new synapses.
1) Redundancy – alternate pathways take over lost function
Adapted from: Cramer et al. (1997). Stroke. 28: 2518-2527.
Cortical Activity During Index Finger Tapping
1) Redundancy – alternate pathways take over lost function
42
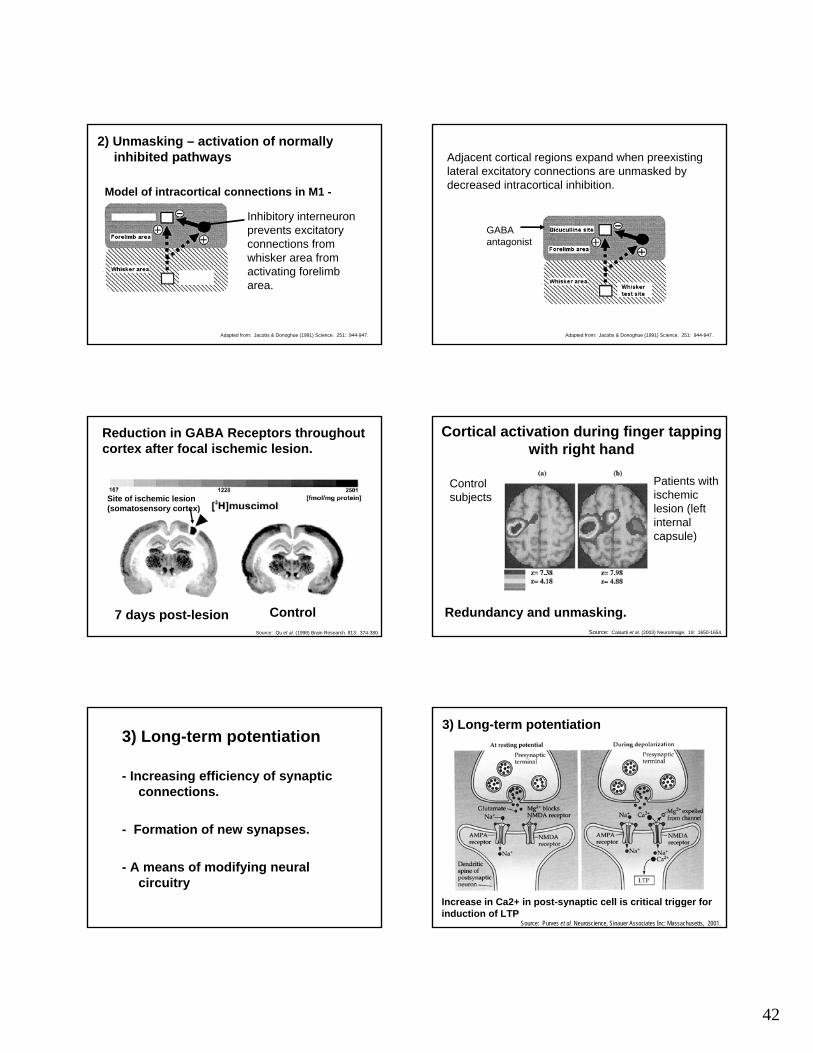
2) Unmasking – activation of normally inhibited pathways
Inhibitory interneuron prevents excitatory connections from whisker area from activating forelimb area.
Model of intracortical connections in M1 -
Adapted from: Jacobs & Donoghue (1991) Science. 251: 944-947.
Adjacent cortical regions expand when preexisting lateral excitatory connections are unmasked by decreased intracortical inhibition.
GABA antagonist
Adapted from: Jacobs & Donoghue (1991) Science. 251: 944-947.
Source: Qu et al. (1998) Brain Research. 813: 374-380.
Reduction in GABA Receptors throughout cortex after focal ischemic lesion.
Control7 days post-lesion
Site of ischemic lesion (somatosensory cortex)
Control subjects
Patients with ischemic lesion (left internal capsule)
Cortical activation during finger tapping with right hand
Source: Calautti et al. (2003) NeuroImage. 19: 1650-1654.
Redundancy and unmasking.
3) Long-term potentiation
- Increasing efficiency of synaptic connections.
- Formation of new synapses.
- A means of modifying neural circuitry
Increase in Ca2+ in post-synaptic cell is critical trigger for induction of LTP
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
3) Long-term potentiation

43
Source: Purves et al. Neuroscience, SinauerAssociates Inc: Massachusetts, 2001.
Ca2+ ions activate postsynaptic protein kinases
--> result is increased synaptic strength
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
LTP may arise from rapid insertion of AMPA receptors
Source: Luscher et al. (2000) Nature Neurosci. 3: 545
LTP may increase size and number of synaptic contacts
Source: Engert & Bonhoeffer (1999) Nature. 399: 66-70.
New dendritic spines begin to form approx 1 hour after induction of LTP
Long-term depression - weakening of a synaptic connection
Source: Purves et al. Neuroscience, Sinauer Associates Inc: Massachusetts, 2001.
End of Topic 15
44
Topic 16 - Rehabilitation After Stroke
1. Rehab techniques
2. Pharmacological approaches
Forced Use / Constraint-Induced Training
Patients practice using affected limb while other limb is restrained.
- ~6 hours/day for several weeks
- Can increase patient's ability to use affected limb.
Constraint-induced rehab training enhances cortical reorganization
The representation of the unconstrained limb increased.
Source: Kim et al. (2004) Yonsei Med. Journal. 45: 241-246.
- Induced lesion in part of hand representation area in M1.- Without post-stroke rehab digit representation in non-lesioned regions also diminished.
from Nudo, et al., Science, 272:1791-1794, 1996 from Nudo, et al., Science, 272:1791-1794, 1996
- Induced lesion in part of hand representation area in M1.- After rehab spared hand rep areas increased in size.

45
Rehabilitative Training
• Post-lesion training is important for optimizing plastic change.
• An absence of training can lead to a further reduction in representation of the affected limb.
Other approaches…
"Observation" therapy - patient observes someone else moving with intent to imitate movements
--> may involve "mirror neuron" system
"Mirror-box" therapy -movements of patient's unaffected arm appear to be made by patient's impaired limb.
Other approaches…
Source: Ramachandran & Rogers-Ramachandran (1996) Proc R Soc Lond B Biol Sci. 1369: 377-386.
Topic 16 - Rehabilitation After Stroke
1. Rehab techniques
2. Pharmacological approaches
Source: Walker-Batson et al. (1995) 26: 2254-2259.
Amphetamine Enhances Recovery ??
Source: Dam et al. (1996) Stroke. 27: 1211-1214.
Fluoxetine Enhances Recovery ??

46
Stem Cell Therapy
Stem cells are cells with the ability to divide indefinitely and, under the right conditions, give rise to many different cell types.
- potential to replace damaged tissues
http://stemcells.nih.gov/info/scireport(Photo Credit: Mr. J. Conaghan)
Human Blastocyst
Source: Sanai et al. (2004) Nature. 427: 740-744
Lateral ventricular walls of adult human brain contain stem cells.
"Activation" of these cells could allow the brain to heal itself.
Adapted from: Chu et al. (2004) Brain Res. 1016: 145-153.
• Acute treatment• Reperfusion and neuroprotection• Time window: hours• Target: ischemic core and penumbra• Limitations: time window, risks
• Recovery and Rehabilitation • Time window: days, weeks, months,
years• Target: the “rest” of the brain• Development of innovative rehabilitation
techniques and “stroke recovery drugs”
Summary - Stroke Management Strategies
End of Topic 16
(and lecture material!)
Top Related