Clinical Spectrum of Motor Neuron Disorders.8

of 21
-
Upload
anonymous-vnv6qf -
Category
Documents
-
view
216 -
download
0
Transcript of Clinical Spectrum of Motor Neuron Disorders.8
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
1/21
CLINICAL SPECTRUM
OF MOTOR NEURONDISORDERSRichard J. Barohn
ABSTRACT
The differential diagnosis of amyotrophic lateral sclerosis (ALS) includes a number ofacquired or inherited disorders causing degeneration of lower and/or upper motorneurons. It is important to consider these diagnoses in the appropriate clinicalcontext because the prognosis is often better, and, in certain situations, specifictreatments may be available. Many of the inherited motor neuron syndromes havecharacteristic clinical presentations that facilitate their recognition. Alternatively,features of the clinical presentation may be atypical for ALS, which should lead toinvestigation of alternative diagnoses. This chapter will review the clinical features ofmotor neuron syndromes that comprise the differential diagnosis of ALS and willprovide guidelines for their diagnostic investigation.
Continuum Lifelong Learning Neurol 2009;15(1):111131.
Less common motor neuron syn-dromes that may present clinically withprogressive dysfunction of motor neu-
rons are included in the differentialdiagnosis of sporadic amyotrophiclateral sclerosis (ALS). In many cases,diagnostic confirmation of these disor-ders requires specific electrophysiologic,serologic, or genetic tests that are notnecessarily routine, so the possibility ofthe disorder must be suspected by theclinician, primarily based on the clinicalpresentation. The recognition of a some-
what atypical presentation for ALS, or,
in some cases, characteristic clinicalfeatures of a distinct motor neuron syn-drome will guide the astute clinician inpursuing an alternative diagnosis to ALSin the appropriate clinical setting.
DEFINITION/TERMINOLOGY OFMOTOR NEURON DISORDERS
The terms amyotrophic lateral sclero-sis (ALS) and motor neuron disease
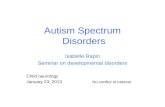
(MND) often are used interchangeably,but MND includes a spectrum of clinicalsyndromes that result from degenera-
tion of upper motor neurons (UMNs),lower motor neurons (LMNs), or both(Figure 5-1). ALS, in which patientsdemonstrate evidence of both anteriorhorn cell and corticospinal tract dys-function, is the most common formof MND.
Progressive muscular atrophy (PMA),or Aran-Duchenne syndrome, is an ex-ample of an MND in which there isexclusively LMN involvement. This dis-
order, which constitutes approximately8% to 10% of patients with MND, isslightly more common in men, with anearlier mean age of onset than ALS.Patients with PMA tend to have a muchbetter prognosis than patients with ALS,and bulbar involvement is rare.
Primary lateral sclerosis (PLS), inwhich only UMN degeneration occurs,occupies the other extreme of the
Copyright # 2009, American Academy of Neurology. All rights reserved.
111
Relationship Disclosure: Dr Barohn has nothing to disclose.Unlabeled Use of Products/Investigational Use Disclosure: Dr Barohn has nothing to disclose.
KEY POINTS
A Motor neuron
disease is
characterized
by degenerationof upper
motor neurons
(UMNs)
(corticospinal
tract), lower
motor neurons
(LMNs) (anterior
horn cells and
cranial nerve
motor nuclei), or
both. ALS, in
which patients
have both
anterior horn cell
and corticospinal
tract dysfunction,
is the most
common form
of motor neuron
disease.
A Progressive
muscular atrophy,
primary lateral
sclerosis (PLS), and
progressive bulbarpalsy are motor
neuron disorders
in which the
degeneration is
limited to the
LMNs, UMNs,
and bulbar
musculature,
respectively.
The differential
diagnosis, clinical
course, andprognosis are
distinct for these
motor neuron
disease syndromes
compared with
ALS, making
their recognition
clinically important.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
2/21
MND spectrum. PLS is a rare disorderand, like PMA, is associated with aprolonged course, with patients some-
times surviving for decades.Progressive bulbar palsy (PBP) re-fers to a form of MND in which theinitial symptoms result exclusively frombulbar dysfunction, which may be relatedto either UMN or LMN degeneration orboth. Although the disease may remainin this form for many years, it can prog-ress rapidly to cause more generalizedsigns and symptoms of ALS. For thosepatients in whom the disease is confinedto the bulbar muscles for many years,
the term isolated bulbar ALS (IBALS)(Dumitru et al, 2007) has been used.
The differential diagnosis, clinicalcourse, and prognosis are distinct forPMA, PLS, and PBP compared with ALS,making recognition of these clinical syn-dromes clinically important. The follow-ing sections will review the evaluationand differential diagnosis for typical ALS,PLS, and the pure LMN syndromes.
EVALUATION AND DIFFERENTIAL
DIAGNOSIS OF ALSAs discussed in the chapter Approachto the Patient With Suspected Myas-thenia Gravis or ALS: a CliniciansGuide, the El Escorial criteria(Brooks, 1994; Brooks et al, 2000)classify ALS into definite, probable,clinically possible, and clinically prob-able categories based on the numberof body regions with findings of UMNand LMN dysfunction. Clinically defi-
nite ALS is defined on clinical evidencealone and requires both UMN andLMN findings in the bulbar region and
at least two spinal regions (cervical,thoracic, lumbosacral) or UMN andLMN signs in three spinal regions.Clinically probable ALS is diagnosedon clinical evidence and has UMN andLMN signs in at least two regions, withsome UMN findings rostral to at leastone LMN finding. Clinically probablelaboratory-supported ALS is the pres-ence of clinical signs of UMN and LMNdysfunction in only one region, orUMN signs alone in one region, and
LMN signs defined by EMG criteriapresent in at least two regions, withother causes excluded by neuroimag-ing and other laboratory tests. Clini-cally possible ALS consists of UMN andLMN findings in one region or UMNfindings in two or more regions or LMNsigns rostral to UMN signs and insuffi-cient electrodiagnostic, neuroimaging,or clinical laboratory studies to sup-port the diagnosis of clinically probablelaboratory-supported ALS. Other diag-noses must have been excluded to ac-cept a diagnosis of clinically possible ALS.
In most patients, ALS does notpresent as a diagnostic dilemma. Inpatients with prominent UMN andLMN findings and a progressive course
without significant sensory or sphincterabnormalities, further laboratory studiesare unlikely to yield an alternativediagnosis. Patients typically present withbulbar or asymmetric limb weakness,
more prominent in distal than in proxi-mal muscles. Atypical clinical featuresshould prompt the clinician to searchfor alternative diagnoses (Table 5-1).
Laboratory Studies
For the patient with suspected ALS, aclinical presentation consisting of bothUMN and LMN findings in a wide-spread distribution, no laboratory testeither proves or disproves the diagno-sis. Experienced neurologists differ in
Continuum Lifelong Learning Neurol 2009;15(1)
112
FIGURE 5-1 Spectrum of motor neuron disorders.
KEY POINTS
A The El Escorial
criteria classify
ALS into definite,
probable,clinicallypossible, and
clinically probable
categories based
on the number of
body regions with
clinical findings of
UMN and LMN
dysfunction.
A In patients with
suspected ALS
who have
multisegmentalUMN and LMN
findings and
a progressive
course, without
significant
sensory or
sphincter
abnormalities,
further
laboratory
studies are
unlikely to yield
an alternativediagnosis.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
3/21
Continuum Lifelong Learning Neurol 2009;15(1)
113
TABLE 5-1 Differential Diagnosis for Motor Neuron Disorders
Combined Upper and LowerMotor Neuron Disorder
Pure Upper MotorNeuron Disorder
Pure Lower MotorNeuron Disorder
" Sporadic Motor Neuron Disease
Amyotrophic lateral sclerosis Primary lateral sclerosis Progressive muscular atrophy
Juvenile monomelic atrophy
Brachial amyotrophic diplegia
Leg amyotrophic diplegia
" Metabolic, Nutritional, and Toxic Disorders
Hyperthyroidism Cobalamin (B12) deficiencya Heavy metal exposure
Hyperparathyroidism Vitamin E deficiencya
Cobalamin (B12) deficiencya Copper deficiencya
Copper deficiencya
" Structural Lesions
Brain stem tumor/massa Cervical spondylotic myelopathya Polyradiculopathy/plexopathya
Spinal cord tumor/mass/vascularmalformations, disc herniationa
Spinal cord tumor/mass/vascularmalformations, disc herniationa
Plexopathya
Cervical spondyloticmyelopathya
Foramen magnum tumor
Polyradiculopathy/plexopathyaArnold-Chiari malformation
SyringomyeliaaSyringomyelia
a
" Degenerative and Hereditary Diseases
Polyglucosan body disease Hereditary spastic paraparesis Spinal muscular atrophy
Leukodystrophies(adrenoleukodystrophy,
adrenomyeloneuropathy,metachromatic leukodystrophy)a
Leukodystrophies(adrenoleukodystrophy,
adrenomyeloneuropathy,metachromatic leukodystrophy)a
Kennedy bulbospinalmuscular atrophy
Hereditary ALS Hereditary ALS Hereditary motor neuropathy(distal spinal muscular atrophy)
Spinocerebellar ataxiasHereditary ALS
Diffuse Lewy body disease
" Infection
HIV myelopathya HIV myelopathya
Lyme diseasea Tropical spastic paraparesis(human T-lymphotropicvirus type 1 infection)
Neurosyphilisa
Lyme diseasecontinued on next page
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
4/21
their choice of studies routinely or-dered when the clinical diagnosis of
ALS is suggested. In general, very fewlaboratory studies need to be donebefore a diagnosis of ALS is rendered.The purpose of laboratory studies is toexclude other diagnostic possibilities,and, in most cases, the testing requiredis usually very limited. For patients
with a classic presentation as notedabove, routine chemistries, complete
blood count (CBC), serum creatinekinase (CK), electrophysiologic testing,and imaging studies of the spine/braincommonly are performed. More exten-sive laboratory testing should be re-served for more atypical presentations(pure UMN or LMN syndromes, diseaseof early onset or prolonged duration,evidence of a coexistent systemic ill-ness, or the presence of sensory orurinary symptoms).
Continuum Lifelong Learning Neurol 2009;15(1)
114
TABLE 5-1 Continued
Combined Upper and LowerMotor Neuron Disorder
Pure Upper MotorNeuron Disorder
Pure Lower MotorNeuron Disorder
" Dysimmune Diseases
Multiple sclerosis Multifocal motor neuropathy
Stiff person syndrome Mononeuropathy multiplex
Hexosaminidase A deficiency
Chronic inflammatory
demyelinating polyneuropathya
" Vascular
Multiple cerebral infarcts
" Malignant/Paraneoplastic
Lymphoma Lymphoma
" Other
Postradiation plexopathyor motor neuron disease
Postradiation plexopathyor motor neuron disease
" Myopathic and Neuromuscular Junction Disorders
Inclusion body myositisb Myasthenia gravis
Myasthenia gravisb Lambert-Eaton syndrome
Lambert-Eaton syndromeb Polymyositis
Polymyositisb Inclusion body myositis
Limb-girdle dystrophyb Limb-girdle dystrophy
Isolated neck or trunkextensor myopathyb
Isolated neck or trunkextensor myopathy
Distal myopathyb Distal myopathy
aUsually has sensory symptoms or signs.bWith other causes for upper motor neuron signs, such as cervical spondylotic myelopathy or old stroke.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
5/21
CBC and chemistry profiles generallyare performed as a screen for a systemicillness but are rarely revealing in typical
ALS cases. Thyroid function tests oftenare obtained to exclude hyperthyroid-ism because it can manifest rarely with
weakness, fasciculations, and hyperre-flexia. Serum cobalamin (vitamin B12)and copper levels are performed toexclude combined systems degenera-tion, but these patients almost invari-ably have sensory symptoms and signs(Case 5-1). If absolutely no sensorysymptoms or signs are present, it isprobably not necessary to obtain B12or
copper serum levels. It may be helpfulto obtain a serum CK, which is usuallymildly increased in ALS but may benormal. A CK level greater than 10 timesthe upper limit of normal is suggestiveof a myopathy, such as polymyositis orinclusion body myositis, rather than
ALS. Hypercalcemia, hypophosphate-mia, and elevated parathyroid hormonelevels may suggest primary hyperpara-thyroidism. Rarely, patients with hyper-parathyroidism can present with muscle
weakness. After removal of a parathy-roid adenoma, some patients with
weakness have improved clinically butother patients have had a progressivelyfatal course, suggesting the coinciden-tal occurrence of the two disorders(Jackson et al, 1998). Based on thisexperience, it is not necessary to ob-tain routine parathyroid hormone levelsin patients with suspected ALS unlessthe serum calcium is elevated.
Laboratory studies also may includeserum protein electrophoresis withimmunofixation to screen for a mono-clonal gammopathy because occasion-ally motor neuropathy occurs in patients
with lymphoma.The presence of a monoclonal
gammopathy should prompt a hema-tology consultation for possible bonemarrow examination and considerationof CSF examination for cytology. Iflymphoma presents with a motor neu-
ropathy presentation, however, an LMNpresentation usually predominates.
It is not recommended to perform a
lumbar puncture routinely for CSFexamination in typical ALS cases be-cause the yield is low. For now, CSFevaluation is reserved for patients in
whom meningeal inflammatory or in-filtrative disease is suspected clinically.In most cases, these patients will havesensory symptoms, pain, and/or signsof systemic illness. In the future, diag-nostic CSF biomarkers may allow forimproved diagnosis of ALS, perhapsleading to the ability to make a diag-
nosis definitively in early cases. Rou-tine testing for heavy metals in theserum or urine is not indicated unlessthere is a high index of suspicion forexposure.
In young-onset patients, particu-larly those under 40 years of age,testing for a familial ALS syndromeshould be considered, even in theabsence of a family history (see thechapter ALS Update: Signs of Prog-ress, Reasons for Hope). In youngerpatients with symmetric (proximalgreater than distal) weakness and noUMN findings, serum hexosaminidase
A levels often are obtained to lookfor late-onset GM2 gangliosidosis. Inpatients with distal amyotrophy andassociated ataxia or dystonia, adult-onset spinocerebellar ataxia shouldbe considered.
All patients with MND should un-dergo EMG and nerve conduction
studies (NCS). The purpose of elec-trophysiologic testing is to confirm thepresence of a multisegmental motoraxonopathy consistent with the clini-cal impression of ALS and to search forevidence of an alternative diagnosis.To support the diagnosis of ALS,results of the NCS should be normalor suggest degeneration of motoraxons without sensory involvement.The EMG can be used to documentLMN involvement in a particular body
Continuum Lifelong Learning Neurol 2009;15(1)
115
KEY POINTS
A In patients
with suspected
ALSand a typical
clinicalpresentation,
laboratory
studies to
exclude other
diagnostic
possibilities may
be very limited.
More extensive
laboratory
testing should
be reserved for
more atypical
presentations
pure UMN
or LMN
syndromes,
disease of early
onset or
prolonged
duration,
evidence of
a coexistent
systemic illness,
or the presence
of sensoryor urinary
symptoms.
A In typical ALS
presentations,
the yield of a
lumbar puncture
for CSF
examination
is low. CSF
evaluation
is reserved
for patientsin whom
meningeal
inflammatory
or infiltrative
disease is
suspected
clinically.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
6/21
region. The electrophysiologic findingsof motor conduction block or otherdemyelinating features suggest the pres-ence of a demyelinating neuropathy.
Accordingly, the NCS should evaluate
proximal segments of the nerve formotor conduction block, which wouldbe suggestive of a demyelinating disor-der such as multifocal motor neuropa-thy. Multifocal motor neuropathy is
Continuum Lifelong Learning Neurol 2009;15(1)
116
Case 5-1A 54-year-old woman presented with a 2-year history of progressive gaitdysfunction and lower limb weakness and stiffness. She initially noted
bilateral foot numbness and gait unsteadiness. Whereas the numbnesspersisted for several months and then resolved, her gait unsteadinessworsened and she noted stiffness in her legs. During the ensuing months,she developed leg weakness and muscle thinning, developing a rightfootdrop 10 months from onset of symptoms followed by a leftfootdrop 12 months later. She required the use of a walker. She had notedleft-hand weakness for the past 3 months. She had no bowel or bladderdifficulties and had only intermittent sensory complaints (transientparesthesias in the hands and feet).
Examination showed prominent atrophy of the anterior and posteriorleg compartments bilaterally. The patient had a completely flail right footand severe weakness of dorsiflexion and plantar flexion of the left foot
(2/5). Proximal muscle strength was normal, but muscle tone was increased.There was moderate atrophy of the intrinsic muscles of the left hand,with grade 4- strength. The right hand was normal. Muscle stretch reflexeswere very brisk with spread but absent at the ankles bilaterally. Shehad bilateral Babinski signs. Sensory examination showed impaired lighttouch, pain, and vibration in a stocking-glove distribution (to midcalfand wrists).
Electrodiagnostic testing revealed unobtainable motor responses in theperoneal and tibial nerves and normal motor responses in the upperextremity. Sensory responses were normal in the upper limb, but the suralsensory nerve action potential was low amplitude. EMG showed acute andchronic neurogenic changes in a multisegmental distribution in the upperand lower limbs.
MRI studies of the cervical, thoracic, and lumbosacral spine were normal.CSF evaluation was normal. Extensive laboratory evaluation showed anormal vitamin B12 level and moderate anemia (hemoglobin 9.2). Thepatient had an undetectable serum copper level (less than 0.10 mg/mL),low serum ceruloplasmin (7.8 mg/dL), and elevated serum zinc level(2.5 mg/mL). She was placed on oral copper gluconate (3 mg/d). Sixmonths later, her neurologic symptoms had stabilized with some mildimprovement in left-hand function.
Comment. Most reports of the neurologic manifestations of copperdeficiency describe a myeloneuropathy with prominent sensory symptoms,sensory ataxia, and varying degrees of spastic paraparesis. This patient hadclear evidence of LMN dysfunction both clinically and on electrodiagnostic
studies. Although her sensory symptoms were never persistent, they wereassociated with some degree of sensory dysfunction on examination andmildly abnormal sensory nerve action potentials on electrodiagnostictesting. This was correctly judged to be atypical for sporadic ALS, and amore extensive laboratory workup revealed the correct diagnosis.
KEY POINT
A All patients with
MND should
undergo EMG
and nerveconduction
studies. The
purpose of
electrophysiologic
testing is to
confirm the
presence of a
multisegmental
motor
axonopathy and
to search for
evidence of an
alternative
diagnosis.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
7/21
characterizedbyslowlyprogressiveasym-metric weakness, conduction block inmotor NCS, and occasionally elevated
GM1ganglioside titers. This demyelinat-ing neuropathy can superficially resem-ble ALS but has no UMN signs. Becausemultifocal motor neuropathy patientsrespond to IV immunoglobulin as ther-apy, appropriate diagnosis is critical.
Abnormal sensory NCS would suggestan alternative diagnosis of a polyneurop-athy, mononeuritis multiplex, or, rarely,
X-linked bulbospinal neuronopathy (seediscussion later in this chapter).
The needle examination is essential
to confirm the diagnosis of ALS butseldom suggests an alternative di-agnosis. Rarely, the needle EMG willsuggest a myopathic process such aspolymyositis or inclusion body myosi-tis. In typical ALS, spontaneous activityis found at rest in affected regions andincludes fibrillations, positive sharp
waves, and fasciculations. Evaluationof voluntary motor units usually re-
veals decreased recruitment of motorunits and increased motor unit firingrates, greater than 10 Hz. With rein-nervation of motor units, patients willhave large-amplitude, long-duration, andsometimes polyphasic motor units. Se-lection of muscles for needle examina-tion is an important component of theEMG. Evaluation of thoracic paraspinalmuscles is particularly useful becausedenervation in thoracic paraspinals ar-gues against the alternative diagnosis ofcombined cervical and lumber spondy-
losis mimicking MND. Needle examina-tion of the tongue documents involve-ment of the disease above the neck,thereby excluding the possibility of acervical cord mass or compression as thecause of the patients concerns. How-ever, it is often difficult to get goodrelaxation of the tongue, and the in-experienced electromyographer maymistake the small motor units of thetongue for fibrillation potentials. Needleexamination of facial muscles also may
be used to document the disease ofthe bulbar region.
Most ALS specialists require evi-
dence of denervation (LMN dysfunc-tion) on the needle examination in atleast two of the following regions:brainstem (bulbar/cranial motor neu-rons) or cervical, thoracic, or lumbo-sacral spinal cord. For the cervical andlumbosacral regions, it is suggestedthat at least two muscles with differentnerve root and different peripheralnerve innervations must show EMGchanges. For the brainstem and tho-racic region, it is sufficient to demon-
strate the EMG change in only onemuscle (tongue, facial, jaw muscles forthe brainstem; paraspinal or abdomi-nal for the thoracic) (Brooks et al,2000; Ross et al, 1998).
Other laboratory studies that maysupport the diagnosis of ALS includeMRI and muscle biopsy. Many patientshave an imaging procedure, usually anMRI scan of the brain, cervical spinalcord, or both, to look for evidence of atumor, syrinx, herniated cervical spinaldisk, cervical spondylosis with spinalcord compression, or some other de-generative disease. Cervical MRI isparticularly important if the patienthas no bulbar symptoms or signs. In apatient with bulbar and spinal symp-toms and signs as well as EMG abnor-malities in these regions, an MRI isprobably not needed. Although MRIscans of the brain and spinal cord areoften normal in ALS, they rarely may
show degeneration of corticospinaltracts. MRI scans are primarily impor-tant to exclude alternative etiologies forthe patients clinical presentation.
A muscle biopsy may be useful ifthere is suspicion of a myopathy basedon clinical or EMG findings, but it is notnecessary in most cases of ALS. If mini-mal evidence for LMN involvement ispresent, a muscle biopsy that indicatesactive denervation, with darkly stained,small, angular fibers on oxidative and
Continuum Lifelong Learning Neurol 2009;15(1)
117
KEY POINTS
A A clinical
diagnosis of
ALS is supported
by evidenceof denervation
(LMN
dysfunction) on
needle EMG
in at least two
of the following
regions:
brainstem
(bulbar/cranial
motor neurons),
cervical,
thoracic, or
lumbosacral
spinal cord.
A MRI of the brain
and/or spinal
cord is done to
look for
evidence of a
tumor, syrinx,
herniated
cervical spinal
disk, or cervical
spondylosis with
spinal cordcompression.
Cervical MRI is
particularly
important in
patients with
limb disease and
no bulbar
findings to
exclude cervical
radiculomyelopathy.
A Muscle biopsy is
rarely necessaryin most cases of
ALS but may
be considered
if there is a
suspicion of
myopathy
based on
clinical or
EMG findings.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
8/21
esterase stains and chronic denerva-tion with reinnervation, with fiber typegrouping and grouped atrophy, sup-
ports the diagnosis of LMN disease in aregion. This information, however, usu-ally can be obtained through the EMG,and muscle biopsy is not needed.
Rarely, inclusion body myositis(IBM) can be misdiagnosed initially as
ALS because of the asymmetric onset.The needle EMG can have both neuro-genic and myopathic motor units inIBM. Usually the pattern of weaknessin IBM is so typical, with wrist andfinger flexor and knee extensor in-
volvement, that there should be noconfusion with ALS. However, occa-sionally it may be difficult at thebedside and with the EMG to differen-tiate patients with IBM from patients
with ALS, particularly if the IBM patienthas another cause for UMN findings,such as cervical spondylotic myelopa-thy. In this setting, a muscle biopsy isuseful. The biopsy in IBM should showa chronic myopathy with endomysialinflammation and rimmed vacuoles inmuscle fibers.
PRIMARY LATERAL SCLEROSIS
Jean-Martin Charcot first reported PLSin 1874, calling it primary sclerosis ofthe lateral columns (Rowland, 2001).He noted the paucity of pathologicevidence and the inability to knowconclusively that LMN signs would notappear over time. These concerns,
which made it difficult to categorize
PLS as a distinct disease entity, stillapply in the modern era. As he statedin a public lecture, pathological in-
vestigations have not yet furnished anyproof, and hence the solution to theproblem remains in suspense. Mean-
while, the clinical description deservesto exist alone (Charcot, 1883).
The caution voiced by Charcot as towhether PLS is a distinct entity wasreiterated by Kinnier Wilson (1940) inhis authoritative textbook of neurology:
Divergent views are still held in regardto so-called primary lateral sclerosis,the spastic spinal paralysis of Erb.
Some consider it belongs to a sepa-rate class from Charcots disease[ALS], taking presence or absence ofmuscular atrophy for the criterion;but since pure atonic atrophy oftenco-exists with slight pyramidal le-sions only disclosed after death,spasticity without wasting might wellrepresent the opposite extreme ofthe same condition.Renewed interest in PLS was stimu-
lated by Fishers 1977 report of six cases
of chronic progressive quadriparesis.In 1992, Pringle and colleagues de-scribed eight cases with one autopsyand proposeddiagnostic criteria, broad-ened to include patients with limitedelectrophysiologic evidence of denerva-tion. A number of relatively large seriesfollowed. In 2001, Le Forestier andcolleagues reported 20 patients fromthe ALS Center at the SalpetriereHospital; they contended that mostpatients with a diagnosis of PLS showmild signs of LMN denervation onfollow-up. Cohorts of 25 patients weredescribed by Zhai and colleagues (2003)at the NIH and by Singer and colleagues(2005) from the University of Texas.Singer and colleagues (2007) recentlysummarized their experience in a re-
view article and proposed new diagnos-tic criteria.
Clinical Features
The most common manifestations ofPLS are leg weakness and spasticity andspastic bulbar weakness. As with ALS,sensory symptoms and signs shouldprompt continued investigation for analternative diagnosis. Although upperextremity symptoms frequently developover time, they are uncommon as aninitial manifestation. Rarely, patientsexperience progressive hemiparesisbefore spread to the opposite sidebecomes clinically apparent.
Continuum Lifelong Learning Neurol 2009;15(1)
118
KEY POINT
A The clinical
manifestations
of PLS include
adult onset,progressive leg
weakness
and spasticity,
spastic bulbar
palsy, and
hyperreflexia
without sensory
signs. Spastic
weakness
may progress
asymmetrically.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
9/21
With lower-limb onset, symptomsusually begin unilaterally. Spasticity pro-duces most of the limb dysfunction in
the early stages, unlike ALS, in whichweakness usually predominates. Pa-tients with PLS typically report stiffness,clumsiness, or poor coordination asthe initial limb symptom; when limb
weakness occurs, it generally followsa UMN pattern. Bulbar symptoms usu-ally manifest first as dysarthria, followedby dysphagia, and may evolve to emo-tional lability and inappropriate laugh-ing or crying (pseudobulbar affect).Dysarthria can progress to anarthria.
Worsening dysarthria may necessitatefeeding-tube placement, even in theabsence of significant limb involvement.Emotional lability (pseudobulbar affect)is common, occurring in more than 50%of patients.
Although Erbs triad of spasticity,hyperreflexia, and mild weakness re-mains the most prominent manifesta-tion of PLS, several other features havebeen noted consistently in patients withPLS. These features include eye move-ment abnormalities, urinary dysfunc-tion, and cognitive impairment. Patientsdo not report visual symptoms, butabnormalities of eye movements, par-ticularly saccadic breakdown of smoothpursuits, may be noted on examination.
Urinary concerns initially were con-sidered to indicate a different diseaseprocess. However, most clinical seriesnow have reported urinary urgency orincontinence as a frequent symptom,
usually developing several years afterinitial presentation. Such symptomsappear more commonly in PLS thanin ALS.
In most early studies, cognition wasreported as normal in patients withPLS. However, in recent years, a fron-tal lobe dementia syndrome has beenreported in PLS patients. These obser-
vations, consistent with the finding offrontal lobe dementia in 10% to 20%of patients with ALS, have contributed
to the increasing awareness noted ear-lier that MND may reflect one fea-ture of a more general neurodegen-
erative process.As illustrated byCase 5-2, PLS tendsto follow a very slowly progressivecourse, a key distinctive clinical fea-ture compared with ALS. Most recentreports indicate that patients were stillalive, with average duration at the timeof follow-up of 8 years. Whereas theaverage life expectancy for patients
with ALS is about 3 years, longevitydata for PLS are incomplete. AmongPLS patients with reported deaths,
survival reports range from 1 to 15years after onset.
EMG Findings
Although in pure PLS needle EMGshould be normal, the recently re-ported series and criteria allow forelectrophysiologic evidence of milddenervation manifested as occasionalfibrillation and increased insertionalactivity in a few muscles, but notenough or to the degree seen in ALS.For this reason, the presence of activedenervation (increased insertional ac-tivity, grade 1+ fibrillations, or posi-tive sharp waves) or fasciculations ordecreased recruitment of motor unitsin a few muscles does not necessarilyrule out PLS. However, this is a con-troversial issue for which clear con-sensus is lacking.
There are reports of patients ini-
tially thought to have PLS but sub-sequently diagnosed with ALS after7 to 27 years of UMN involvement.Gordon and colleagues (2006) identi-fied a group of 29 patients with iso-lated UMN signs and no evidence ofLMN involvement clinically or on EMG.Of that group, 13 went on to developEMG evidence of denervation as wellas clinical signs of LMN dysfunction.
Patients with a diagnosis of PLS andminimal EMG changes seem to have
Continuum Lifelong Learning Neurol 2009;15(1)
119
KEY POINTS
A Bulbar symptoms
in PLS usually
manifest first as
dysarthria,followed by
dysphagia,
and may evolve
to emotional
lability and
inappropriate
laughing or
crying
(pseudobulbar
affect).
Dysarthria can
progress to
anarthria.
A Other reported
clinical features
in patients with
PLS include eye
movement
abnormalities,
urinary
dysfunction,
and cognitive
impairment.
A PLS tends
to follow
a very slowly
progressive
course, a key
distinguishing
it from ALS.
Whereas the
average life
expectancy for
patients with
ALS is about
3 years,
longevity datafor PLS are
incomplete.
Among PLS
patients with
reported
deaths, survival
reports range
from 1 to
15 years
after onset.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
10/21
more disability compared with PLS pa-
tients without EMG changes. Singerand colleagues (2005) reported asignificantly decreased ability to am-bulate independently in their patients
with PLS with minimal EMG changes,even after controlling for increasedduration of illness in that group.Gordon and colleagues (2006) notedsignificant differences in scores on the
ALS Functional Rating Scale betweentheir clinically pure PLS group and theUMN-dominant ALS group, with a
trend toward lower forced vital capac-
ity and reduced time to disability inthe UMN-dominant ALS group.
Differential Diagnosis
The differential diagnosis for progres-sive corticospinal spasticity, alone ortogether with corticobulbar spasticity,is broad (Table 5-1). Many disorders,such as inherited illnesses or condi-tions with sensory symptoms or moregeneralized neurologic impairment,could be eliminated readily after a
Continuum Lifelong Learning Neurol 2009;15(1)
120
Case 5-2A 55-year-old woman initially developed lower extremity stiffnessbeginning with the right leg 10 years ago, which gradually progressed
to the point that she became wheelchair bound 6 years later.Approximately 3 years ago, she noted the onset of a speech problem,which worsened to the point that, 18 months later, her speech waspractically incomprehensible. She had difficulty with swallowing for thepast 2 years and ate mainly soft, pureed food. She denied bladderincontinence but had significant constipation for years. She had nofamily history of neurologic disease.
On examination, the patient had a severe spastic dysarthria. Tongueprotrusion appeared normal in strength, but tongue movements weremarkedly slowed. No tongue atrophy or fasciculations were present.There was bilateral weakness of upper and lower facial muscles. Mildsymmetric weakness of the distal upper extremity muscles with associated
spasticity and a severe spastic paraparesis were present. She was thin,but no clear muscle wasting or fasciculations were present. Muscle stretchreflexes were diffusely brisk (3+), and she had prominent finger flexor,pectoralis, and jaw jerk reflexes. Sensation was normal.
MRI of the brain showed only deep white matter signal changes.MRI of the cervical and thoracic spine was normal. NCS and EMG doneon three occasions were normal. Spinal fluid analysis was normal.Human T-lymphotropic virus antibodies were not present in the serumor CSF. Hematology, serum chemistries, genetic hereditary spasticparaparesis, B12, and serum immunofixation electrophoresis studieswere all normal.
Comment. This patient initially presented with lower limb spasticitywith a slowly progressive course and subsequently developed a progressive
spastic dysarthria. Clinically, she had predominant UMN dysfunction,with three previous electrodiagnostic studies failing to reveal LMNinvolvement. The absence of significant muscle atrophy also indicatedthat this patient most likely had PLS. It has been suggested that patientswith MND presenting with spasticity who do not develop limb wastingwithin 3 years do not have the classic profile of sporadic ALS and mostprobably have PLS. These patients likely will progress more slowly and livelonger than those with typical ALS.
KEY POINT
A Needle EMG
findings in
PLS should
show noevidence
of LMN
dysfunction.
However,
recently
reported series
and criteria
allow for
electrophysiologic
evidence of
mild denervation
manifest as
occasional
fibrillations
and increased
insertional activity
in a few muscles.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
11/21
careful history and examination. Al-though PLS generally has been adiagnosis of exclusion, the same con-
sideration applies to most sporadicdegenerative conditions for whichno diagnostic test is available. Studiesrecommended to exclude other diag-noses include serum chemistries, co-balamin (vitamin B12) and copper levels,as well as serum testing for syphilis,Lyme disease, and human T-cell lym-photropic virus type 1. Examination ofCSF and imaging of brain and spinalcord are obtained to exclude compres-sive lesions or hyperintense lesions sug-
gestive of multiple sclerosis. Imagingalso will exclude compressive lesionsdue to a mass or developmental disor-der. For patients with limb onset, test-ing for genetic mutations associated
with hereditary spastic paraparesisshould be considered and be mandatoryif other family members have a similardisorder. Determination of very long-chain fatty acids for adrenomyeloneur-opathy and HIV serologies are obtained
when clinically appropriate. All patientsshould undergo EMG and NCS. Furthertesting, such as evoked potentials andmuscle biopsy, should be performedaccording to the clinical situation. Se-rum CK results are not reported fre-quently in PLS (Singer et al, 2005) but,
when mildly elevated, support addi-tional LMN involvement.
The hereditary spastic paraplegias(HSPs) and familial ALS merit particu-lar consideration. The inherited forms
of spasticity originally were termedhereditary PLS by Erb and later referredto as Strumpell disease (an autosomaldominant form of HSP now designatedspastic paraplegia type 3) (Holmesand Shaywitz, 1977). The past decadehas witnessed rapid progress in clari-fying the genetic basis for several formsof HSP. HSP can be autosomal domi-nant, recessive, or X-linked. Twentygenetic loci (spastic gait loci [SPG])have been identified thus far (Fink,
2003; Fink and Ranier, 2004). The mostcommon form, accounting for 40% ofautosomal dominant cases, is asso-
ciated with mutation of the SPG4gene, which produces the proteinspastin. Other autosomal dominantforms are caused by mutations of thegenes encoding atlastin (SPG3), kinesinheavy chain (SPG10), nonimprintedin Prader-Willi/Angelman syndrome 1(NIPA1) (SPG6), and heat shock pro-tein 60 (SPG13). Autosomal recessiveinheritance has been linked to mu-tations in paraplegin (SPG7) and spar-tin (SPG20), and X-linked forms to
L1 cell adhesion molecule (SPG1)and proteolipid protein (SPG2). Cur-rently, genetic testing is available com-mercially for spastin, atlastin, andNIPA1mutations.
HSP usually presents before 20 to30 years of age, most commonly inadolescence. There is some range inthe age of onset of illness, includingpatients diagnosed in middle age withsymmetric leg spasticity. Although lowerextremity spasticity generally prog-resses in severity, arm involvement isuncommon and bulbar manifestationsare extremely rare (McDermott et al,2000).Interestingly, LMN dysfunctionhasbeen reported in a subgroup of patients
with mutation of SPG4 (McDermottet al, 2006). Bladder symptoms are com-mon, and some patients may exhibitmild sensory loss in the feet, suggestingposterior column involvement. It is cer-tainly possible that some reported pa-
tients with PLS actually had a form ofHSP, although the absence of familyhistory, typical onset in middle age orlater life, and bulbar involvement wouldmake this prospect less likely.
In familial ALS, patients usually displayovert UMN and LMN involvement. Rarecases of PLS have been reported, how-ever, in families with nonsuperoxidedismutase 1 autosomal dominant ALS(Brugman et al, 2005) and spinal mus-cular atrophy type IV (Appelbaum et al,
Continuum Lifelong Learning Neurol 2009;15(1)
121
KEY POINT
A The hereditary
spastic
paraplegias
merit particularconsideration in
the differential
diagnosis
of patients
presenting with
progressive
spastic limb
weakness. The
absence of
family history,
typical onset
in middle age
or later life,
and bulbar
involvement
would make
this possibility
less likely.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
12/21
1992). Autosomal recessive juvenile-onset forms of ALS have been identi-fied, related to mutations in the ALS2
gene, a gene coding for the GTPasealsin (Kress et al, 2005). Of considerableinterest, mutations in this same genehave been associated with autosomalrecessive cases of infantile ascendingHSP and juvenile PLS (Eymard-Pierreet al, 2006; McDermott et al, 2006). Itremains unclear how mutations in thesame gene can lead to three verydifferent phenotypes; the age of onset,however, is usually in the first 2 yearsof life, unlike typical PLS.
For patients with exclusive UMNsymptoms acquired in middle age orlater, the two main diseases to con-sider are ALS and PLS. ALS is morecommon and is usually the ultimatediagnosis. If there is no or verylimited evidence of LMN involvement,a tentative diagnosis of a PLS-spectrumdisorder can be made. In thissetting, patients can be informed thatthe prognosis is better compared
with ALS and that the progressionis slow. Such patients require closefollow-up to determine whether LMNsigns develop.
Diagnostic Criteria
Recently suggested diagnostic criteriafor PLS are given in Table 5-2 (Singeret al, 2007).
PURE LOWER MOTORNEURON SYNDROMES
The LMN syndromes are hetero-geneous and consist of idiopathicconditions similar to ALS, inheriteddisorders, andof most interestimmune-mediated disorders (Tables5-1 and 5-3). The difference in prog-nosis leads many clinicians to explorethe possibility of an immune-mediateddisorder in many patients with sus-pected ALS. The truth is that, in mostcases, the distinction between an im-mune neuropathy and MND can be
made readily on the basis of a thor-ough history and neurologic examina-tion. The main immune-mediated dis-
orders that are in the differentialdiagnosis for MND (Table 5-1) arechronic immune demyelinating poly-neuropathy (CIDP), mononeuritis mul-tiplex, and multifocal motor neuro-pathy. In CIDP and mononeuritismultiplex, patients almost invariablyhave sensory signs and symptoms. InCIDP, diffuse hyporeflexia is a charac-teristic feature, and profound muscle
weakness may be accompanied bylittle or no muscle atrophy (in contra-
distinction to MND). The latter alsomay be the case for multifocal motorneuropathy, particularly in the earlystages. Although patients with multi-focal motor neuropathy may haveasymmetric weakness and fascicula-tions, careful examination will revealthat the weakness is in the distribu-tion of individual peripheral nerves,rather than myotomal, as would beexpected for MND.
Patients with an idiopathic, purelyLMN disorder typically are referred toas having PMA. It is clear that a sig-nificant proportion of patients withPMA actually have ALS and just lackclinical evidence of UMN involvement.This is supported by autopsy seriesshowing UMN pathology in approxi-mately 50% of patients with PMA(Ince et al, 2003). Up to one-third ofpatients with MND lack UMN signsat presentation (Mortara et al, 1984).
A significant portion of patientswith PMA, if followed over time,will develop UMN findings and thencan be diagnosed with ALS. In somecases, UMN signs may have beenpresent before the patient is evaluatedbut subsequently became undetect-able because of progressive LMN loss.During the lifetime of a patient withPMA, evidence of UMN pathologymay be detected with MRI or trans-cranial magnetic stimulation (Sach et al,
Continuum Lifelong Learning Neurol 2009;15(1)
122
KEY POINTS
A For patients
with progressive
purely UMN
symptomsacquired in
middle age or
later, the two
main diseases
to consider are
ALS and PLS.
ALS is more
common and
is usually
the ultimate
diagnosis.
A The distinctionbetween
an immune-
mediated
neuropathy,
such as
multifocal motor
neuropathy,
and motor
neuron disease
can usually
be readily
made on the
basis of athorough history
and neurologic
examination and
supported by
electrophysiologic
studies.
A Patients with
an idiopathic
purely LMN
disorder are
typically referred
to as havingprogressive
muscular atrophy
(PMA). A
significant
proportion of
patients with
PMA actually
have ALS and
just lack clinical
evidence of UMN
involvement.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
13/21
Continuum Lifelong Learning Neurol 2009;15(1)
123
TABLE 5-2 Proposed Diagnostic Criteria for PrimaryLateral Sclerosis
" Clinical FeaturesPresence of:
Findings of UMN disorder on physical examination
Spasticity
Pathologic reflexes
Weakness, when present, in an UMN distribution
Regions of involvement
Limb (legs, arms, or both
Bulbar
Mixed limb and bulbar
Time course: 4 years or longer
Progressive
Age of onset: adult older than 20 years
Bladder symptoms due to UMN dysfunction may be present
Absence of:
LMN disorder on physical examination
Fasciculations
Atrophy
Sensory signs on physical examination
Family history of similar disorders
" Laboratory Features
Supportive of:
Transcranial magnetic stimulation
Increased central motor conduction time
Decreased cortical excitability (eg, motor evoked potential cannotbe obtained)
Magnetic resonance spectroscopy findings in the motor cortex
Decreased NAA/creatinine ratio
Decreased NAA/choline ratio
Diffusion-tensor imaging findings in the posterior limb of theinternal capsule
Decreased fractional anisotropy
Increased apparent diffusion coefficient
continued on next page
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
14/21
2004). Conventional MRI sequencesmay indicate UMN involvement, but
more specialized modalities, such asmagnetic resonance spectroscopy, areusually needed (Kalra and Arnold,2003).
Opinions differ on how to refer topatients with an acquired LMN syn-drome. For patients presenting witha clinical picture resembling ALSasymmetric, progressive weaknessbut lacking UMN findings, many clini-cians will give a diagnosis of ALS. Thisis based on the high incidence of UMN
features that can be found in suchpatients on imaging, transcranial mag-
netic stimulation, or autopsy. Otherclinicians tell such patients that theydo not at that time meet criteria for ALSand are, instead, diagnosed with PMA.
Another semantic issue involves theterms PMA and spinal muscular atrophy(SMA). Some physicians use the termSMA synonymously with PMA. Manyclinicians reserve the term SMA forpatients with a genetic disorder ofLMN. It is occasionally difficult to know
with certainty the cause of a particular
Continuum Lifelong Learning Neurol 2009;15(1)
124
TABLE 5-2 Continued
" Laboratory Features
Exclusionary
Serologic evidence for etiology of myelopathy
Abnormal CSF
Evidence of structural abnormality or demyelinating disorder on
routine MRI of brain or spine
EMG
Abnormal motor or sensory nerve conduction studies
See classification section (below) for patients with EMG abnormalities
Any known HSP or alsin gene mutations
" Classification of Primary Lateral Sclerosis
Clinical primary lateral sclerosis
Fulfills above clinical and laboratory inclusionary and exclusionary features
Suspected primary lateral sclerosis
Fulfills above clinical and laboratory inclusionary and exclusionary
features with the following exceptions:
Four years duration or less
EMG evidence of minimal denervation that does not satisfy ElEscorial criteria for ALS
Complicated PLS (PLS plus)Patients who fulfill the criteria for clinical PLS or suspected PLS whoalso have evidence of dementia, parkinsonism, or sensory abnormalities(Note: consider multiple system atrophy)
CSF = cerebrospinal fluid; EMG = electromyography; LMN = lower motor neuron; NAA =N-acetylaspartate; PLS = primary lateral sclerosis; UMN = upper motor neuron.
Reprinted from Singer MA, Statland JM, Wolfe GI, Barohn RJ. Primary lateral sclerosis. Muscle Nerve2007;35(3):291302. Copyright# 2007, with permission from John Wiley & Sons, Inc.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
15/21
patients LMN syndrome. Although pa-tients may have a genetic cause fortheir weakness, if there is no familyhistory and no gene defect identified,
their diagnosis may be classified as PMA.However, certain clinical features, suchas symmetric and proximal weakness
with legs weaker than arms, would favorSMA over PMA.
Several different LMN syndromeshave been described. Although over-lap occurs, there are distinguishingaspects with regard to age of onset,etiology, site of involvement (regionalpredilections and restrictions), pro-gression, and mortality (Table 5-3).
Progressive Muscular Atrophy
PMA (also sometimes referred to asAran-Duchenne syndrome) comprisesapproximately 10% of patients with
MND (Van Den Berg-Vos, et al, 2003).It is slightly more common in men, withan earlier mean age of onset than ALS.Patients receiving the diagnosis of PMArepresent a mixed group, includingpatients who have ALS but lack clinicalfeatures of UMN involvement as well aspatients with a purely LMN disorder.Therefore, it is impossible to know forcertain the clinical course and prognosisof PMA. As a group, patients with PMAhave a much better prognosis than
Continuum Lifelong Learning Neurol 2009;15(1)
125
TABLE 5-3 Comparison of Lower Motor Neuron Disorders to ALS
ALS
ProgressiveMuscularAtrophy
SpinalMuscularAtrophy
KennedyDisease
MonomelicAmyotrophy
BrachialAmyotrophicDiplegia
Age of Onset(Years)
3060 3060 2050 3060 1535 3060
Duration Monthsto years
Years Decades Decades Progressionover 2 to3 years withsubsequentstabilization
Years
Distributionof Weakness
Asymmetric,distal
Asymmetric,distal
Symmetric,proximal
Symmetric,proximal
Asymmetric,restricted
to 1 to 2extremities
Symmetric,proximal upper
extremities
Upper MotorNeuron Signs
Present Absent Absent Absent Absent Absent
Lower MotorNeuron Signs
Present Present Present Present Present Present
Inheritance Sporadic (95%)Inherited (5%)
AD, AR, XR
Sporadic AR (SMNgene)
XR(CAG
repeats)
Sporadic Sporadic
Distinct
Features
Gynecomastia,
diabetes,impotence,infertility
Male
predominance
Preservation
of respiratoryand bulbarfunction
AD = autosomal dominant, AR = autosomal recessive, XR = X-linked recessive; CAG = cytosine-adenine-guaninenucleotidase.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
16/21
those with ALS. In one series, patientswith PMA showed a 5-year survival rateof 56% (Chio et al, 1985).
Spinal Muscular Atrophy
SMA is a diverse group of hereditaryMNDs, selectively involving LMNs, par-ticularly the anterior horn cells of thespinal cord. Adult-onset SMA, referredto as type IV, has several forms andusually begins after the age of 20. Theprevalence is estimated to be 0.32 per100,000 population and accounts forless than 10% of all SMA cases. Weak-ness is usually greater in the legs than in
the arms. The most common inheri-tance pattern (seen in approximatelytwo-thirds of patients) is autosomalrecessive, with a mean age of onset inthe fourth decade (Rudnik-Schonebornet al, 1994). The autosomal dominantform accounts for one-third of casesand shares a similar clinical phenotype(Pearn, 1978). The adult-onset diseaseis slowly progressive, with only asmall proportion of patients becoming
wheelchair dependent after 20 years.Patients typically present with symmet-ric proximal or generalized weaknessand fasciculations. SMA rarely affectsbulbar muscles, and respiratory musclesgenerally remain unaffected. UMN signsare absent. Other forms of SMA caninvolve predominantly distal muscles(so-called distal SMA) (Harding andThomas, 1980). Distal SMA also can beeither autosomal recessive (two-thirds)or autosomal dominant (one-third).
Most cases of SMA types I, II, III, and IVare caused by deletions in the sur-vival motor neuron gene on chromo-some 5, although the younger the ageof diagnosis, the more likely this muta-tion will be found (Brahe et al, 1995).
X-Linked SpinobulbarNeuronopathy(Kennedy Disease)
Kennedy disease is a form of MNDthat is associated with bulbar involve-
ment and X-linked recessive inheritance(Kennedy et al, 1968). The diseaseaffects only males, usually beginning
in the third or fourth decade of life.The initial symptoms include musclecramps, a limb-girdle distribution ofmuscle weakness, and bulbar symp-toms. Distinguishing clinical featuresinclude facial and, particularly, perioralfasciculations, which are present inmore than 90% of patients, hand tremor,and tongue atrophy associated with alongitudinal midline furrow. There isno evidence of UMN involvement. Al-though sensory examination is typically
normal, sensory NCS are frequently ab-normal. Other systemic manifestationsinclude gynecomastia in 60% to 90% ofpatients due to elevated gonadotropinlevels associated with testicular atrophy,feminization, impotence, and infertility.Diabetes mellitus is seen in 10% to 20%of patients. Genetic testing can beperformed to confirm the presence ofan abnormal trinucleotide-repeat expan-sion (CAG) in the androgen receptorgene on the X chromosome (La Spadaet al, 1991). In healthy individuals, therepeats range from 17 to 26 in thiscoding area, whereas, in Kennedy dis-ease, the number of repeats rangesfrom 40 to 65. The number of theenlarged CAG repeat is significantlycorrelated with the age of onset buthas no correlation with severity of
weakness, degree of sensory neuropa-thy, presence of gynecomastia, or im-potence (Case 5-3).
Monomelic Amyotrophy(Focal Motor Neuron Disease,Hirayama Disease)
Monomelic amyotrophy usually refersto an MND originally described asjuvenile muscular atrophy of the distalupper extremity by Hirayama in 1959in which muscle weakness remainslimited to several myotomes (usuallyC5 to T1) within a single extremity
Continuum Lifelong Learning Neurol 2009;15(1)
126
KEY POINTS
A PMA comprises
approximately
10% of
patients withmotor neuron
disease, being
slightly more
common in
men, with
an earlier
mean age of
onset. Patients
receiving the
diagnosis of
PMA represent
a mixed group:
patients who
have ALS
but lack
clinical features
of UMN
involvement as
well as patients
with a purely
LMN disorder
(more favorable
prognosis).
A In adult-onset
spinal muscularatrophy,
patients
typically present
with symmetric
proximal or
generalized
weakness and
fasciculations,
with sparing
of the bulbar
and respiratory
muscles.Inheritance
may be either
autosomal
dominant or
recessive.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
17/21
(Hirayama et al, 1987). The mean ageof onset is typically 20 to 35 years witha male predominance (2:1). Patientsdemonstrate preferential weakness inthe hand and forearm muscles, whichprogresses rapidly over a period of 2to 3 years and subsequently remainsstable. Approximately 75% of cases in-
volve the upper extremities, and theothers involve the lower extremities.Reflexes in the involved muscles are
invariably hypoactive or absent. Thereare no UMN signs, and sensory symp-toms are limited to hypesthesia topin and touch in approximately 20% ofpatients. In 50% of cases, the weak-ness remains localized to one limb;the other 50% of cases show clinicalevidence of involvement in the con-tralateral limb. Electrodiagnostic stud-ies often show evidence of bilateralinvolvement, although weakness may
Continuum Lifelong Learning Neurol 2009;15(1)
127
Case 5-3A 53-year-old man was referred for a second opinion regarding a diagnosisof ALS. He reported progressive symmetric lower extremity weakness with
onset 5 years ago. He noted a prominent fatigable component to hisweakness, with worsening associated with prolonged use of the muscles.More recently, he had noted shoulder weakness, difficulty swallowing, andfacial twitching. He reported significant recurrent muscle cramping sincehis early 20s. He denied a family history of neurologic illness.
Examination showed bifacial weakness with nearly continuous facialfasciculations, proximal greater than distal extremity weakness, areflexia,and normal sensation. There was also weakness and atrophy of thetongue, a mild nasal dysarthria, and significant axial weakness withan exaggerated lumbar lordosis. A postural tremor was noted in the upperextremities, and frequent fasciculations were observed in the arms andlegs. He had gynecomastia.
CBC and chemistries were normal. MRI of the brain and C-spinewere normal. Serum CK level was elevated at 2400 IU/L. EMG showedwidespread reinnervation changes and fasciculations in arms, legs, tongue,and thoracic paraspinals, with minimal fibrillation potentials. MotorNCS were normal, although somewhat borderline in amplitude, andsensory responses were absent in the upper and lower limbs.
Genetic studies were positive for an expanded allele in the CAG repeatregion of the androgen receptor gene (44 CAG repeats; normal is fewerthan 30), confirming the diagnosis of Kennedy disease. The patient wasprovided with genetic counseling because he had two adult daughterswho were potential carriers of the genetic mutation.
Comment. This patient presented with prominent weakness andfasciculations of the lower facial and oromandibular muscles and
proximal limb weakness, with onset of symptoms in his late 40s.The prominent fasciculations and the electrophysiologic findings ofmultisegmental neurogenic disease led to the initial diagnosis of ALS.However, the chronic course, symmetric weakness, sensory abnormalitieson electrophysiologic testing, and the excessively elevated serum CKlevel were clearly atypical findings. Further investigation led to therecognition of the prominent facial fasciculations, gynecomastia, andupper extremity tremor as characteristic of X-linked bulbospinalneuronopathy, or Kennedy disease, and appropriate genetic testingwas performed to confirm the diagnosis.
KEY POINTS
A X-linked
bulbospinal
neuronopathy
(Kennedydisease) presents
with a limb-girdle
distribution of
muscle weakness
and bulbar
symptoms with
onset typically
in the fourth
or fifth
decade of life.
Distinguishing
clinical features
include
facial/perioral
fasciculations,
gynecomastia,
hyporeflexia,
hand tremor,
and tongue
atrophy with a
characteristic
midline furrow.
A Monomelic
amyotrophy
is a rare disorderin which
motor neuron
degeneration is
limited to a
single or several
myotomes
(usually C5 to
T1) within a
single extremity.
Progression
usually occurs
for 1 to 3 yearsfollowed by
disease stability.
The mean age of
onset is typically
20 to 35 years
with a male
predominance.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
18/21
be clinically apparent in only one ex-tremity (Donofrio, 1994).
MRI may reveal a normal cervical
spinal cord, but bilateral or unilateralcord atrophy often is seen (Chen et al,2004). Hirayama and colleagues (2000)have suggested that this syndromemay be related to either local com-pression of the cervical cord or cir-culatory insufficiency caused by ananterior shift of the posterior duraduring neck flexion. Sometimes ab-normalities may be seen on MRI only
when images are acquired with theneck in a flexed position (forward
displacement of cervical dural sac)(Hirayama et al, 2000). Neck flexionalso may produce decreased abnor-malities on somatosensory evokedpotentials. A recent report from Tai-
wan describes a useful finding that canbe seen in cervical spine MRI scanstaken in a neutral, nonflexed position(Chen et al, 2004). These investigatorsfound that an increased separationbetween the posterior dural sac andadjacent lamina was a highly sensi-tive and specific finding in Hirayamapatients. They endorse a pathogenictheory involving imbalance betweenthe spinal cord and spinal column thatresults in a tight dural sac.
Flail Arm Syndrome
Flail arm syndrome is an MND regionalvariant consisting of weakness exclu-sively confined to the upper extremi-ties. Cases have also been described
under the names of hanging armsyndrome and neurogenic man inthe barrel. Patients with flail arm syn-drome have bilateral upper extrem-ity weakness and atrophy that affectspredominantly the proximal arms andshoulder girdle. The average age ofonset does not differ from that of ALS,but, in comparison with ALS, this syn-drome is significantly more commonin men (Hu et al, 1998; Katz et al,1999). Average survival is approxi-
mately 5 years, compared with 3 yearsfor patients with ALS. Although theoverall survival is longer than for ALS,
some patients presenting with a flailarm phenotype can go on to developa typical ALS course. A flail arm pat-tern is seen in approximately 10%of patients with MND, although itis much more common in those of
African descent (Tomik et al, 2000).Curiously, these patients do not showthe same prolonged survival as whitepatients with the flail arm phenotype(Tomik et al, 2000).
Within the flail arm clinical pheno-
type, another significant division can bemade. Among patients with this presen-tation, if weakness remains confined tothe arms for at least 18 months, noclinically significant progression outsideof the upper extremities occurs andsurvival is quite prolonged. In the seriesof Katz and colleagues (1999), after amean follow-up of 5.5 years, weaknessremained restricted to the upper ex-tremities in seven of 10 patients. Whenpresent, leg involvement was mild. Nopatient lost the ability to ambulateindependently, and none developedbulbar or respiratory involvement. Onepatient had restricted weakness forgreater than 10 years. This clinical pre-sentation has been named brachialamyotrophic diplegia (Katz et al, 1999).Patients with brachial amyotrophic di-plegia (showing no progression beyondarms by 18 months) represent approxi-mately 2% of all patients with MND.
There may be an analogous processin the legs, which has been termedleg amyotrophic diplegia (Rosenfeldet al, 2002).
SUMMARY AND CONCLUSIONS
The clinical spectrum of motor neurondisorders is relatively wide, and, depend-ing on the particular clinical phenotype,one or more of these disorders may beconsidered in the differential diagno-sis of sporadic ALS. The distribution of
Continuum Lifelong Learning Neurol 2009;15(1)
128
KEY POINTS
A Flail arm
syndrome
is an MND
regional variantconsisting of
weakness
exclusively
confined to
the upper
extremities.
Average
survival is
approximately
5 years,
compared with
3 years for
patients with
ALS.
A In the flail arm
syndrome
clinical
phenotype,
if weakness
remains
confined to
the arms
for at least
18 months,
usually noclinically
significant
progression
outside of
the upper
extremities
occurs and
survival is quite
prolonged.
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
19/21
weakness, the degree of UMN versusLMN involvement, the rate of progres-sion, and the presence of associated
neurologic or systemic signs will deter-mine the differential diagnosis for each
individual patient. Recognition of theclinical MND phenotypes described inthis chapter is critical in light of the more
favorable prognosis of these disorderscompared with sporadic ALS.
REFERENCES
Appelbaum JS, Roos RP, Salazar-Grueso EF, et al. Intrafamilial heterogeneity in hereditarymotor neuron disease. Neurology 1992;42(8):14881492.
Brahe C, Servidei S, Zappata S, et al. Genetic homogeneity between childhood-onset andadult-onset autosomal recessive spinal muscular atrophy. Lancet 1995;346(8977):741742.
Brooks BR, Miller RG, Swash M, Munsat TL; World Federation of Neurology Research
Group on Motor Neuron Diseases. El Escorial revisited: revised criteria for the diagnosis ofamyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord2000;1(5):293299.
Brooks, BR; World Federation of Neurology Research Group on Neuromuscular Diseases.El Escorial World Federation of Neurology criteria for the diagnosis of amyotrophiclateral sclerosis. J Neurol Sci 1994;124(suppl):96107.
Brugman F, Wokke JH, Vianney de Jong JM, et al. Primary lateral sclerosis as a phenotypicmanifestation of familial ALS. Neurology 2005;64(10):17781779.
Charcot JM. Lecture XVI: transverse myelitis and spasmodic tabes dorsalis. In: Lectures onthe localization of cerebral and spinal diseases. London: The New Sydenham Society,1883:299300.
Chen CJ, Hsu HL, Tseng YC, et al. Hirayama flexion myelopathy: neutral-position MRimaging findingsimportance of loss of attachment. Radiology 2004;231(1):3944.
Chio A, Brignolio F, Leone M, et al. A survival analysis of 155 cases of progressive muscularatrophy. Acta Neurol Scand 1985;72(4):407413.
Donofrio PD. AAEM case report #28: monomelic amyotrophy. Muscle Nerve1994;17(10):11291134.
Dumitru D, Wang Y, Syed K, et al. Isolated bulbar ALS (IBALS): clinical andelectrophysiological features [Abstract]. J Clin Neuromusc Dis 2007;9(3):183.
Eymard-Pierre E, Yamanaka K, Haeussler M, et al. Novel missense mutation in
ALS2 gene results in infantile ascending hereditary spastic paralysis. Ann Neurol2006;59(6):976980.
Fink JK. The hereditary spastic paraplegias: nine genes and counting. Arch Neurol2003;60(8):10451049.
Fink JK, Ranier S. Hereditary spastic paraplegia: spastin phenotype and function.Arch Neurol 2004;61(6):830833.
Fisher CM. Pure spastic paralysis of corticospinal origin. Can J Neurol Sci1977;4(4):251258.
Continuum Lifelong Learning Neurol 2009;15(1)
129
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
20/21
Gordon PH, Cheng B, Katz IB, et al. The natural history of primary lateral sclerosis.Neurology 2006;66(5):647653.
Harding AE, Thomas PK. Hereditary distal spinal muscular atrophy: a report on
34 cases and a review of the literature. J Neurol Sci 1980;45(23):337348.
Hirayama K, Tokumaru Y. Cervical dural sac and spinal cord in juvenile muscularatrophy of distal upper extremity. Neurology 2000;54(10):19221926.
Hirayama K, Tomonaga M, Kitano K, et al. Focal cervical poliopathy causing juvenilemuscular atrophy of distal upper extremity: a pathological study. J Neurol NeurosurgPsychiatry 1987;50(3):285290.
Holmes GL, Shaywitz BA. Strumpells pure familial spastic paraplegia: case study andreview of the literature. J Neurol Neurosurg Psychiatry 1977;40(10):10031008.
Hu MT, Ellis CM, Al-Chalabi A, et al. Flail arm syndrome: a distinctive variant ofamyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry 1998;65(6):950951.
Ince PG, Evans J, Knopp M, et al. Corticospinal tract degeneration in the progressivemuscular atrophy variant of ALS. Neurology 2003;60(8):12521258.
Jackson CE, Amato AA, Bryan WW, et al. Primary hyperparathyroidism and ALS:
is there a relation? Neurology 1998;50(6):17951799.
Kalra S, Arnold D. Neuroimaging in amyotrophic lateral sclerosis. Amyotroph Lateral SclerOther Motor Neuron Disord 2003;4(4):243248.
Katz JS, Wolfe GI, Andersson PB, et al. Brachial amyotrophic diplegia: a slowly progressivemotor neuron disorder. Neurology 1999;53(5):10711076.
Kennedy WR, Alter M, Sung JH. Progressive proximal spinal and bulbar muscular atrophyof late onset. A sex-linked recessive trait. Neurology 1968;18(7):671680.
Kress JA, Kuhnlein P, Winter P, et al. Novel mutation in the ALS2 gene in juvenileamyotrophic lateral sclerosis. Ann Neurol 2005;58(5):800803.
La Spada AR, Wilson EM, Lubahn DB, et al. Androgen receptor gene mutationsin X-linked spinal and bulbar muscular atrophy. Nature 1991;352(6330):7779.
Le Forestier N, Maisonobe T, Spelle L, et al. Primary lateral sclerosis: furtherclarification. J Neurol Sci 2001;185(2):95100.
McDermott C, White K, Bushby K, Shaw P. Hereditary spastic paraparesis: a reviewof new developments. J Neurol Neurosurg Psychiatry 2000;69(2):150160.
McDermott CJ, Burness CE, Kirby J, et al; UK and Irish HSP Consortium. Clinical features ofhereditary spastic paraplegia due to spastin mutation. Neurology 2006;67(1):4551.
Mortara P, Chio A, Rosso MG, et al. Motor neuron disease in the province ofTurin, Italy, 19661980: survival analysis in an unselected population. J Neurol Sci1984;66(23):165173.
Pearn J. Autosomal dominant spinal muscular atrophy: a clinical and genetic study.J Neurol Sci 1978;38(2):263275.
Continuum Lifelong Learning Neurol 2009;15(1)
130
"MOTOR NEURON DISORDERS
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
7/24/2019 Clinical Spectrum of Motor Neuron Disorders.8
21/21
Pringle CE, Hudson AJ, Munoz DG, et al. Primary lateral sclerosis: clinical features,neuropathology and diagnostic criteria. Brain 1992;115(pt 2):495520.
Rosenfeld J, Chang SW, Jackson CE, et al. Lower extremity amyotrophic diplegia
(LAD): a new clinical entity in the spectrum of motor neuron disease. Neurology2002;58(suppl 3):411412.
Ross MA, Miller RG, Berchert L, et al; rhCNTF ALS Study Group. Toward earlier diagnosisof amyotrophic lateral sclerosis: revised criteria. Neurology 1998;50(3):768772.
Rowland LP. How amyotrophic lateral sclerosis got its name: the clinical-pathologicgenius of Jean-Martin Charcot. Arch Neurol 2001;58(3):512515.
Rudnik-Schoneborn S, Rohrig D, Morgan G, et al. Autosomal recessive proximalspinal muscular atrophy in 101 sibs out of 48 families: clinical picture, influence ofgender, and genetic implications. Am J Med Genet 1994;51(1):7076.
Sach M, Winkler G, Glauche V, et al. Diffusion tensor MRI of early upper motor
neuron involvement in amyotrophic lateral sclerosis. Brain 2004;127(pt 2):340350.
Singer MA, Kojan S, Barohn RJ, et al. Primary lateral sclerosis: clinical and laboratoryfeatures in 25 patients. J Clin Neuromusc Dis 2005;7(1):19.
Singer MA, Statland JM, Wolfe GI, Barohn RJ. Primary lateral sclerosis. Muscle Nerve2007;35(3):291302.
Tomik B, Nicotra A, Ellis CM, et al. Phenotypic differences between African andwhite patients with motor neuron disease: a case-control study. J Neurol NeurosurgPsychiatry 2000;69(2):251253.
Van Den Berg-Vos RM, Van Den Berg LH, Visser J, et al. The spectrum of lower motorneuron syndromes. J Neurol 2003;250(11):12791292.
Wilson SAK. Amyotrophic lateral sclerosis. In: Bruce AN, ed. Neurology. Baltimore:Williams & Wilkins, 1940:10151016.
Zhai P, Pagan F, Statland J, et al. Primary lateral sclerosis: a heterogeneous disordercomposed of different subtypes? Neurology 2003;60(8):12581265.
131