




Languages
Pages
Legal


International Journal of Reproductive BioMedicineVolume 17, Issue no. 12, https://doi.org/10.18502/ijrm.v17i12.5789Production and Hosting by Knowledge E
Review Article
The role of melatonin in polycystic ovarysyndrome: A reviewSina Mojaverrostami1 D.V.M., Narjes Asghari2 M.Sc., Mahsa Khamisabadi3
D.V.M., Heidar Heidari Khoei4, 5 D.V.M.1Department of Anatomy, School of Medicine, Tehran University of Medical Sciences, Tehran,Iran.2Department of Molecular Medicine, Faculty of Medical Biotechnology, National Institute ofGenetic Engineering and Biotechnology, Tehran, Iran.3Faculty of Veterinary Medicine, Urmia University, Urmia, Iran.4Student Research Committee, School of Medicine, Shahid Beheshti University of MedicalSciences, Tehran, Iran.5Department of Biology and Anatomical Sciences, School of Medicine, Shahid BeheshtiUniversity of Medical Sciences, Tehran, Iran.
AbstractBackground: Polycystic ovary syndrome (PCOS) is a widespread endocrine disorder,affecting approximately 20% of women within reproductive age. It is associatedwith hyperandrogenism, obesity, menstrual irregularity, and anovulatory infertility.Melatonin is the main pineal gland hormone involved in the regulation of the circadianrhythm. In recent years, it has been observed that a reduction in melatonin levelsof follicular fluid exists in PCOS patients. Melatonin receptors in the ovary and intra-follicular fluid adjust sex steroid secretion at different phases of ovarian follicularmaturation. Moreover, melatonin is a strong antioxidant and an effective free radicalscavenger, which protects ovarian follicles during follicular maturation.Objective: In this paper, we conducted a literature review and the summary of thecurrent research on the role of melatonin in PCOS.Materials and Methods: Electronic databases including PubMed/MEDLINE, Web ofScience, Scopus, and Reaxyswere searched from their inception toOctober 2018 usingthe keywords “Melatonin” AND “Polycystic ovary syndrome” OR “PCOS.”Results: Based on the data included in our review, it was found that the administrationof melatonin can improve the oocyte and embryo quality in PCOS patients. It may alsohave beneficial effects in correcting the hormonal alterations in PCOS patients.Conclusion: Since metabolic dysfunction is the major finding contributing to theinitiation of PCOS, melatonin can hinder this process via its improving effects onmetabolic functions.
Key words: Hyperandrogenism, Infertility, Melatonin, PCOS.
How to cite this article: Mojaverrostami S, Asghari N, Khamisabadi M, Heidari Khoei H. “The role of melatonin in polycystic ovary syndrome:A review,” Int J Reprod BioMed 2019; 17: 865–882. https://doi.org/10.18502/ijrm.v17i12.5789 Page 865
Corresponding Author:
Sina Mojaverrostami;
Department of Anatomical
Sciences, School of Medicine,
Tehran University of Medical
Sciences, 16 Azar St., Poursina
St., Tehran, Iran.Postal Code: 1417933791
Tel: (+98) 21 64432348
Email:
Received 12 February 2019
Revised 16 May 2019
Accepted 20 July 2019
Production and Hosting by
Knowledge E
Mojaverrostami et al. This
article is distributed under the
terms of the Creative
Commons Attribution License,
which permits unrestricted
use and redistribution
provided that the original
author and source are
credited.
Editor-in-Chief:
Aflatoonian Abbas M.D.

International Journal of Reproductive BioMedicine Mojaverrostami et al.
1. Introduction
Polycystic ovary syndrome (PCOS) is a complexdisorder arising from the interaction of geneticand environmental reasons that affects up to 20%of women at reproductive age (1). According tothe ESHRE/ASRM consensus, at least two of thefollowing three features should be present forproper PCOS diagnosis: 1) ovulatory dysfunction(oligoanovulation and/or anovulation); 2) hyperan-drogenemia (the biochemical feature of androgenexcess) or hyperandrogenism (the clinical featureof androgen excess); 3) polycystic appearance ofovaries in ultrasonography (2), together with theexclusion of other etiologies (3). In addition toreproductive and cosmetic sequelae, PCOS syn-drome is associated with a higher risk of metabolicdisorders including insulin resistance, increasedoxidative stress (4), cardiovascular disease, type 2diabetes mellitus, liver disease, and endometrialcancer (5, 6).
Women with PCOS often seek treatment dueto their complaints of infertility and menstrualcycle irregularities which are the results of chronicoligo/anovulation (7). Changing lifestyles, such asnutritional counseling and weight loss are thenecessary step of all treatment plans (8). Despitethe many advances in the understanding of thePathobiology and treatment strategies of PCOSover the past decades, many questions remain tobe answered and the treatment of the syndromeremains empirical.
Melatonin (N-acetyl-5-methoxytrypamine) is anindolamine hormone that was firstly recognizedin the 1950s (9). Melatonin levels are regulatedby photoperiod as its production and secretionare promoted at night in response to darknesssince light can suppress its secretion (9). Melatoninis also produced in other organs such as thegastrointestinal tract, skin, retina, bone marrow,and lymphocytes (10, 11). It seems that mitochondriaare the site of melatonin synthesis within cells.
Moreover, the female reproductive organ, includingthe follicular cells, oocytes, and cytotrophoblastsare also among the melatonin production sites(12). Several studies have shown the involvementof melatonin in the pathogenesis of diabetes,cancer, Alzheimer’s disease, immune and cardiacdiseases (13-15). Melatonin has been identified tohave different pharmacological properties such asantioxidant, immunomodulatory, anti-angiogenic,and oncostatic effects (16). Melatonin acts asan inhibitory factor on the hypothalamic pituitarygonadal axis (17). Melatonin receptors are trans-membrane G-protein-coupled receptors includingmelatonin receptor 1 (MT1; MTNR1A) and melatoninreceptor 2 (MT2; MTNR1B) (18).
The effects of melatonin on female reproduc-tive physiology are mediated via its receptorsin hypothalamic, pituitary, and ovarian sites (19).Melatonin is also a potent free radical scavengerthat exerts protective effects in female reproductiveorgans; for instance, it is involved in the protectionof the oocyte against oxidative stress, particularlyat the time of ovulation. It can also be used toprotect the developing fetus from oxidative stresscan be happened by melatonin (20). The levels ofmelatonin in follicular fluid are higher than its levelsin the blood (21). The concentration of melatoninin follicular fluid significantly rises as the folliclesbecome mature (22).
In this paper, we have made an effort to reviewthe possible roles of melatonin in the pathogen-esis of PCOS as well as the potential melatonin-centered therapeutic measures, which can berecruited herein.
2. Materials and Methods
2.1. Search strategy
Related published articles were searched in thefollowing electronic databases: PubMed/MEDLINE,
Page 866 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
Web of Science, Scopus and Reaxys. All thesources were searched from their inception toOctober 2018 using the keywords “Melatonin” AND“Polycystic ovary syndrome” OR “PCOS.”
2.2. Study selection
Titles and abstracts from the electronicdatabases were scrutinized following the searchfor the keywords, and the full-text papers whichwere expected to match with our inclusioncriteria were obtained. The following specifiedinclusion criteria were used: (1) studies thatused melatonin in context of PCOS or those inwhich melatonin was somehow shown to be
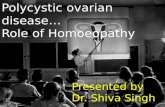
related to any of the mechanisms involved in thepathogenesis of PCOS; (2) papers with availablefull texts; (3) Papers in English language only.There was no limitation regarding the inclusionof any human or animal models for PCOS orcell lines researches. Furthermore, the followingexclusion criteria were applied: (1) no reporton the treatment with melatonin; (2) no reportwith the PCOS disease; (3) no report on theuse of melatonin for treating PCOS in clinicalor animal models or cell lines researches; (4)no report on the melatonin level alternation inthe different body biological fluids; (5) reviewarticles; and (6) non-English language articles(Figure 1).
Figure 1. Flow diagram of the search strategy.
2.3. Data extraction
The papers, meeting all the aforementionedcriteria were reviewed separately to confirmthe reliability of the extracted data. Allcharacteristics of the articles such as author
name, year, study location, study population,study period, treatment method, dose oftreatment, and outcomes were extractedfrom the papers. The extracted data ofthe selected studies are shown in Tables Iand II.
https://doi.org/10.18502/ijrm.v17i12.5789 Page 867

International Journal of Reproductive BioMedicine Mojaverrostami et al.Ta
bleI.Cha
nges
inMelaton
inleve
lsof
PCOSpa
tients
Autho
r,ye
ar(ref)
Cou
ntry
Partic
ipan
tsMea
nag
e(yea
r)Sam
ple
Melaton
inor
itsmetab
olite
leve
ls𝛼M
T6sin
urine(μg/24h)
Melaton
inin
saliv
a,bloo
d,an
dfollicu
larflu
id(pg/ml)
Hormon
alleve
lsin
serum
LH,F
SH
(mIU
/ml)
Testos
terone
(ng/ml)8-O
HdG
(ng/ml)
Res
ult
Patie
nts
Control
LH/FSH
ratio
Patie
nts
Control
Lubo
shitzky
etal.,20
03an
d20
04(33,
34)
Israel
12wom
enwith
PCOS
20.3±4.8
Urin
eαM
T6s:
52.6±20
.330
.5±6.5
LH FSH
T
13.5±2.9
5.3±2.1
0.58
±0.28
4.6±2.2
6.5±1.4
0.3±0.1
Theleve
lofLH,
testosterone
,and
αMT6
sweresign
ificantlyhigh
erin
PCOSpa
tients
Lubo
shitzky
etal.,20
01(35)
Israel
22wom
enwith
PCOS
22.9±5.2
Urin
eαM
T6s:
54.0±20
.330
.1±6.6
LH/FSH
2.04
±1.2
40.74±0.39
PCOSpa
tientsha
dhigh
erleve
lsof
aMT6
s,testosterone
,LH/FSH
ratio
,an
dinsulin
than
control
wom
en.Testosteron
ewas
ago
odindicatorfor
aMT6
sco
ncen
tratio
ninPC
OS
patie
ntswhich
inve
rsely
relatedto
aMT6
s
Shreeve
etal.,20
13(42)
UK
15wom
enwith
PCOS
29.8+3
.7Urin
eαM
T6s:
60.3±30
.637.7±21.5
FSH
LH T8-OHdG
6.9±0.6
8.1±
1.22.3±0.2
120.5±42
.184
.0±40
.8
Night-timemelaton
inan
d8-OHdG
concen
tratio
nsweresign
ificantlyhigh
erin
PCOSwom
enco
mpa
red
tohe
althywom
en
Jain
etal.,
2013
(40)
India
50wom
enwith
PCOS
24.87±4.43
Bloo
dplasma
Melaton
in:
63.27±10.9
32.51±
7.5
FSH
LH TLH
/FSH
5.43
±1.5
316.13
±7.9
51.2
.84±6.96
3.10±1.6
9
6.60
±2.86
7.18±1.9
70.84
±12.75
1.15±0.25
Melaton
inleve
linc
reasein
allthe
casesof
PCOS
wom
enbu
ttestosteron
eleve
lrisein72
%of
patie
nts.Melaton
inleve
lpo
sitivelyrelatedto
increa
sedtestosterone
concen
tratio
n
Terzieva
etal.,20
13(49)
Bulgaria
30wom
enwith
PCOS
25.07±
1.10
Bloo
dserum
Melaton
in:
49.37±3.79
42.91±
9.38
FSH
LH TLH
/FSH
6.83
±1.0
412.43±3.83
0.60
±0.05
1.64±0.33
5.57
±0.32
4.08
±0.35
0.32
±0.03
0.73
±0.03
InPC
OSwom
en,serum
melaton
inco
ncen
tratio
nwas
sign
ificantlyhigh
erthan
thehe
althywom
en
Zang
eneh
etal.,20
14(50)
Iran
77wom
enwith
PCOS
26.6±4.7
Bloo
dserum
Melaton
in:2
5.48
±24
.27
32.45±24
.27
––
–
Melaton
inco
ncen
tratio
nin
serum
ofPC
OSwom
enwas
sign
ificantlylower
than
theco
ntrolw
omen
Kim
etal.,
2013
(72)
South
Korea
13wom
enwith
PCOS
31.1±0.8
FFMelaton
in:
20.9±3.6
136.8±26
.1–
––
Inwom
enwith
PCOS,
melaton
inco
ncen
tratio
nin
follicu
larfl
uidwas
sign
ificantlylower
than
the
controlg
roup
Page 868 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOSTa
bleII.
Protec
tiveeffectsof
exog
enou
sMelaton
ininPC
OS
Autho
r,ye
ar(ref)
Cou
ntry
Stud
yde
sign
PCOSmod
elSam
ple
size
Trea
tmen
t(do
sage
)Rou
teof
administration
Duration
Res
ults
Lemos
etal.,
2016
(68)
Brazil
In-vivo
PCOSrats
(indu
cedby
constant
light
stimulation)
50
Combina
tionof
melaton
in(200
μg/10
0gb.w.)and
metform
inhydroc
hloride(50
mg/100gb.w.)
Melaton
in(sub
cutane
ous
injections)and
Metform
inhydroc
hloride
(gavag
e)
20da
ys
Redu
cedthetim
ene
eded
for
preg
nanc
yan
dredu
ced
plasmaestro
genleve
lsinthe
treated
grou
p,increa
sedthe
plasmaprog
esterone
leve
lsan
dthenu
mbe
rand
weigh
tof
offspring,
beside
simprov
ingfetald
evelop
men
t
Kim
etal.,
2013
(72)
South
Korea
In-vitro
PCOSwom
en13
IVM
med
ium
containing
800µl
IVM
med
ium
with
10µm
ol/lmelaton
in
–2da
ys
Additio
nof
melaton
inlead
sto
improveinthecytoplasmic
maturationof
immature
oocytesan
dalso
implan
tatio
nratesan
dpreg
nanc
yrates
wereen
hanced
Pacchiarotti
etal.,20
15(64)
Italy
In-vivo
PCOSwom
en165
Combina
tionof
myo
-inosito
l(40
00mg),folicacid
(400
mcg
)and
melaton
in(3
mg)
Orally
administered
14da
ys
Increa
sing
thenu
mbe
rof
matureoo
cytesinthetre
ated
grou
pwas
show
edan
dintra
-follicu
larc
once
ntratio
nof
melaton
inwas
four
times
high
erthan
intheco
ntrol
grou
p
Lemos
etal.,
(2014)
(83)
Brazil
In-vivo
PCOSrats
(indu
cedwith
constant
Illum
ination)
15
Combina
tionof
melaton
in(200
μg/10
0gb.w.)and
metform
inhydroc
hloride(50
mg/100gb.w.)
Melaton
in(sub
cutane
ous
injections)and
Metform
inhydroc
hloride
(gavag
e)
20da
ys
Combina
tionof
twodrug
swas
morehe
lpfulinthe
declineof
plasmaticleve
lsof
liver
enzyme,
nitricox
ide,
and
totalg
lutathione
.Also,inthe
treated
grou
p,inflammatory
respon
sean
dhistop
atho
logicald
amag
ewerede
crea
sed
Limaet
al.,
2004
(79)
Brazil
In-vivo
PCOSrats
(Indu
cedwith
pine
alec
tomyor
continuo
uslight)
113
Melaton
in(200
μg/10
0gbo
dyweigh
t)
Injected
intra
-muscu
larly
4mon
ths
Melaton
in-trea
tedgrou
psshow
edasign
ificant
redu
ctioninthenu
mbe
rof
cystsan
dan
tigon
adotroph
iceffects
https://doi.org/10.18502/ijrm.v17i12.5789 Page 869

International Journal of Reproductive BioMedicine Mojaverrostami et al.Ta
bleII.
Continue
d
Autho
r,ye
ar(ref)
Cou
ntry
Stud
yde
sign
PCOSmod
elSam
ple
size
Trea
tmen
t(do
sage
)Rou
teof
administration
Duration
Res
ults
Nikmard
etal.,20
16(73)
Iran
In-vivo/In-
vitro
PCOSmice
(indu
cedby
the
injectionof
dehydro-
epiand
roster-
one)
16
10−5,10−
6 ,an
d10
−7
mol/L
ofmelaton
inweread
dedinto
the
med
ium
cultu
re.
–24
hours
Additio
nof
melaton
into
med
ium
cultu
reincrea
sed
maturationrate
andclea
vage
rate.H
ighe
stmaturationrate
was
observed
at10
−6mol/L
concen
tratio
nof
melaton
in
Paie
tal.,
2014
(56)
India
In-vivo
PCOSrats
(indu
cedby
administra
tion
oftestosterone
)
16Melaton
in(1mg/kg
and2mg/kg
)
Intra
-pe
riton
eally
injected
35da
ys
Both
dosesof
melaton
inmea
ning
fully
redu
cedthe
numbe
rofc
ystic
follicles,
neop
lasticen
dometria
lglan
dsan
dde
crea
sed
adipoc
ytehype
rtrop
hy
Ahmad
iet
al.,20
17(74)
Iran
In-vivo
PCOSmice
(indu
cedby
injections
ofDHEA
)
12Melaton
in(10
mg/kg
body
weigh
t)
Intra
-pe
riton
eally
injected
5da
ys
Administra
tionof
melaton
inlead
sto
asign
ificant
increa
seinthethickn
essof
the
gran
ulos
alaye
rbut
the
redu
ctioninthethickn
essof
thethec
alaye
r
Tagliaferri
etal.,20
17(91)
Italy
In-vivo
PCOSwom
en40
Melaton
in(Arm
onia
Fast1m
g;2tabletsa
day)
Orally
administra
ted
6mon
ths
Melaton
intre
atmen
tde
crea
sedan
drog
ensleve
ls,
butF
SHleve
lsignifican
tlyraised
andan
ti-Mulleria
nho
rmon
eleve
lsignifican
tlydrop
ped
Bashee
ret
al.,20
18(80)
India
In-vivo
PCOSrats
(indu
cedby
Letro
zole)
–Melaton
in(200
μg/10
0gbo
dyweigh
t)
Intra
-pe
riton
eally
injected
–
Melaton
intre
atmen
tinPC
OS
ratsrestored
theMT1
and
MT2
rece
ptorsintheov
arian
tissue
Al-Q
adhi,
2018
(60)
Iraq
In-vivo
PCOSwom
en50
Melaton
in3mg/da
yOrally
administra
ted
2mon
ths
Melaton
intre
atmen
tde
crea
sedLH
leve
land
BMI
inPC
OSpa
tients
Page 870 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
3. Results
3.1. Study characteristics
After searching the aforementioned databaseswith considered keywords, the papers werereviewed by two authors. In the first step, titlesand abstracts were screened and 121 papersthat had enough connectivity with our keywordswere included. In the second step, full textswere reviewed for the eligibility and relevanceof their findings, and 99 articles were excludeddue to duplicate data, non-English languages,review articles, and insufficient relevance. Finally,22 studies were selected, including studiesthat have used melatonin administration fortreating PCOS in clinical and animal models ofPCOS and also the studies that have shownalternation of melatonin levels involved in thepathogenesis and diagnosis of PCOS; 22 articleswere included in the current review, including15 clinical human studies and 7 animal studies.Table I is related to the studies that indicatethe alternation of melatonin levels in differentbiological fluids such as blood, serum, urine,saliva, and follicular fluid in PCOS patients. Table IIis related to the studies that have used exogenousmelatonin as a drug for curing PCOS in sickwomen, animal models, or cell lines researches.And, the remaining studies are related to themelatonin receptor gene polymorphisms in PCOSpatients.
3.2. PCOS pathogenesis
PCOS may be initiated by some specific abnor-malities in the hypothalamus-pituitary compart-ment, ovaries, adrenal gland, and the peripheralcompartment like adipose tissue (23). In PCOSpatients, an increase in gonadotropin-releasinghormone (GnRH) pulse frequency enhances the
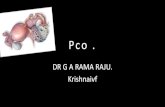
luteinizing hormone (LH) pulse frequency andamplitude (24). In spite of elevated LH secretion,follicle-stimulating hormone (FSH) levels remainin the lower follicular range due to the negativefeedback of enhanced estrogen levels and follic-ular inhibition (24). As a result of altered LH:FSHratio in PCOS women, the androgen productionby the theca cells in the ovaries is increased;however, due to the low FSH levels, the follic-ular maturation is dramatically impaired (25). Inaddition, ovarian dysregulation of cytochrome-17,defects in the aromatase activity of the ovariangranulosa cells (GC), as well as the stimulationof the ovarian theca cells by high levels ofinsulin-like growth factor 1 (IGF-1) are among othermechanisms involved in androgen overproduction(26). Excessive adrenocortical secretion of dehy-droepiandrosterone is observed in approximately50-70% of PCOS patients (27). Increased peripheral5 alpha-reductase activity and enhanced periph-eral aromatization of androgens to estrogens thatinduces the reversal of estrone to estradiol ratioand a chronic hyperestrogenic state are also seenin PCOS patients (28). There is general agree-ment that insulin resistance and hyperinsuline-mia play a major part in the pathogenesis ofPCOS (29). Hyperinsulinemia stimulates ovariantheca cells and leads to androgen overproduc-tion. Hyperinsulinemia along with hyperandrogen-emia and enhanced levels of IGF-1 inhibit sexhormone-binding globulin secretion, which surgesthe levels of bioactive androgens and worsensthe clinical manifestations of androgen excess inPCOS patients (29). Also, it has been discoveredthat insulin resistance and hyperandrogenism canaffect normal function of adipocytes (30). Previousresearchers have found that adipose tissue dys-function are associated to metabolic and reproduc-tive dysfunction including insulin resistance andandrogen excess secretion in most PCOS patients(31) (Figure 2).
https://doi.org/10.18502/ijrm.v17i12.5789 Page 871

International Journal of Reproductive BioMedicine Mojaverrostami et al.
3.3. Alternation of melatonin levels indifferent body fluids of PCOS patients
Melatonin synthetic enzymes such as arylalky-lamine N-acetyl-transferase and hydroxyindole-O-methyltransferase have been identified in mosttissues including ovaries (10). Measurable levels ofmelatonin have been identified in most biologicalfluids, interestingly in the follicular fluid. The con-centration of melatonin in preovulatory follicles ishigher than that of plasma suggesting its possibledirect effects on ovarian function (32).
In several studies, melatonin levels in PCOSwomen have been measured to find its role inthe PCOS pathogenesis (Table I) (33, 34). Themost important metabolite of melatonin, urinary 6-sulfatoxymelatonin (aMT6s), is considered to be agood marker for melatonin production in the body(35). The plasma concentrations of aMT6s in hyper-androgenic and PCOS women were significantlyhigher than healthy women possibly due to highermelatonin production (35). It has been demon-strated that testosterone and estrogen can regu-late melatonin secretion. Melatonin secretion hasbeen shown to decrease in castrated rats due tothe reduction of testosterone levels (36). Ovariec-tomized rats exposed to 17β-estradiol had reducednumbers of α/β-adrenoreceptors, responsible forthe stimulation of melatonin production, in theirpinealocytes (37). Sex hormones can adjust thehuman biological clock by affecting the hypotha-lamic suprachiasmatic nucleus and pinealocytes(38). In a study by Luboshitzky and colleagues,PCOS women had higher levels of αMT6s, LH,and testosterone than patients with idiopathichirsutism or the control groups. The results ofthis study showed that αMT6s level inverselyrelated to testosterone level in PCOS disease.However, this result seems contradictory becauseother studies in PCOS introduced the direct rela-tionship between αMT6s and testosterone (33).
Treatment with estradiol-cyproterone acetate nor-malized the αMT6s levels in PCOS patients byinhibiting androgens and gonadotropins (33). Inanother study by the same group, women withPCOS had higher aMT6s, testosterone, LH/FSHratio, and insulin values than women in the controlgroups. Higher aMT6s levels were due to the ampli-fication of melatonin production. In some studies,testosterone was introduced as a determinant ofaMT6s level in PCOS patients (35). Melatonin hasbeen found to increase the secretion of proges-terone and androgen in pre-antral follicles afterincubation for two weeks and in antral folliclesafter a 30-hr incubation (39). In other studies,the elevated melatonin levels in serum of PCOSpatients was found to be positively associatedwith testosterone levels (40). Results from studiesshow that melatonin levels in blood and salivaalong with the level of 6-sulfatoxymelatonin inurine were significantly higher in PCOS patientscompared to the healthy women (41). The levelsof 6-sulfatoximelatonin in urine, nocturnal mela-tonin levels in saliva (at 3:00 am), and melatoninin the blood had a significant correlation withthe degree of sleep disorders (41). 8-hydroxy-2’-deoxyguanosine (8-OHdG) is a marker of oxidativedamage to DNA that can be detected in urine(42). In one study, the daytime urinary aMT6sand 8-OHdG levels were similar in PCOS patientsand the control group, while the night-time levelsof these molecules were significantly higher inPCOS patients than those of the control group(42). During the night, PCOS women with raisedoxidative stress markers had higher levels of8-OHdG and aMT6s. The production of higheramounts of melatonin was probably for neutralizingreactive oxygen species (ROS) at the night time.Melatonin level in PCOS cases was shown to havea significant correlation with the serum LH:FSHratio (40). In patients with higher LH:FSH ratios,melatonin levels were significantly lower than the
Page 872 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
patients with lower ratios, indicating the inversecorrelation of LH:FSH ratio andmelatonin secretion(40).
Different studies have indicated that PCOSpatients have higher serum levels of melatonin(35, 40), therefore melatonin could be used asa valuable marker for the prediction of PCOS.It was suggested that the elevation of serummelatonin in PCOS patients is due to the reductionin its follicular fluid concentration (32) The roleof melatonin in oocyte maturation has been alsoapproved. Concentration of melatonin in the pre-ovulatory follicles is higher than smaller immaturefollicles, resulting in higher antioxidant capacity oflarger follicles (43). In PCOS patients, the declinein the follicular concentration of melatonin is dueto the reduction in the uptake of melatonin fromcirculation and an increase in the numbers of atreticfollicles (32). Follicular atresia could be seen inPCOS patients due to increased oxidative stressand follicular damage which occurs as a resultof the reduction in intra-follicular melatonin levels(32). A great deal of research has shown that ROSgeneration and lipid peroxidation are meaning-fully higher in PCOS cases (44, 45). Along withthese changes, levels of superoxide dismutase,catalase, and glutathione peroxidase are reduced,which causes intense oxidative stress in ovarianfollicles (46). Melatonin is shown to be capableof regulating the gene expression of antioxidantenzymes, in addition to preventing apoptosis byincreasing Bcl2 and reducing Caspase 3 (47,48). Terzieva and colleagues reported that mela-tonin levels in women with PCOS in the morningwere significantly higher than at night time, andthe night-day difference of melatonin levels inPCOS cases was lower than that of the healthygroup (49). However, a study reported conflictingresults stating that the total serum melatonin levelswere significantly lower in women with PCOS(50).
3.4. Association of melatonin receptorgene polymorphisms in PCOS patients
The positive effects of melatonin on differenttissues of the body are mediated by the melatoninreceptors 1A and 1B (18). The earliest study on theassociation between common genetic variations ofmelatonin receptors and the prevalence of PCOSwas conducted by Wang and colleagues (51). Inthis study, four single nucleotide polymorphisms(SNPs) (rs4753426, rs10830963, rs1562444, andrs1279265) in MTNR1B gene were determinedand no differences in genotype and allelotypefrequencies for these SNPs were found neitherin the PCOS nor in the healthy women. In addi-tion, they found a significant association betweenthe rs10830963 SNP and the concentration oftestosterone in PCOS patients. The amount oftestosterone, glucose, and insulin in the serums ofwomen with cytosine/guanine allele (CG) and gua-nine/guanine allele (GG) genotypes were consider-ably higher than the cytosine/cytosine allele (CC)genotypes, which describes the possible effectsof DNA sequence variations of melatonin receptorgenes on the occurrence of PCOS. In subsequentresearch that was performed on Chinese women,the relationship between the pathogenesis ofPCOS and rs2119882 SNP, which is located in theMTNR1A gene was evaluated. Genotype and allelefrequencies of rs2119882 were significantly differ-ent between the PCOS cases and the controls;the C allele frequency in the PCOS patients wassignificantly higher than the control group whichconfirms the association of SNP rs2119882 withPCOS (52). In another study, an association oftwo SNPs, rs10830963 and rs10830962 locatedat the MTNR1B gene with PCOS, was examined.Both genotypes and allelotypes occurrences ofthe rs10830963 SNP in PCOS women were sig-nificantly different compared to healthy women.In addition, the occurrences of GG and GC were
https://doi.org/10.18502/ijrm.v17i12.5789 Page 873

International Journal of Reproductive BioMedicine Mojaverrostami et al.
higher among PCOS women. According to theresults of the mentioned study, rs10830963SNPis associated with the predisposition of women toPCOS. No suggestive differences were observedin the genotypes and allele distributions of theother SNPs (rs10830962) between the PCOS andthe healthy women (53). Recently, Song and col-leagues reported that there is a significant asso-ciation between rs2119882 and the prevalence ofPCOS, although no association was found betweenrs10830963 and PCOS (54). They reported that theclinical and metabolic features of PCOS manifestlargely in CC genotype carriers than the TC andTT genotypes. They also showed that there existsa considerable difference in the transmission ofallele C of rs2119882 between obese and non-obese PCOS patients.
3.5. Protective effects of exogenousmelatonin administration in PCOS
3.5.1. Metabolic function improvement bymelatonin
An improvement of metabolic function in PCOSpatients may enhance ovarian function. There hasbeen growing evidence suggesting the relation ofmelatonin with glucose homeostasis and insulinsecretion. Peschke and colleagues have showna negative correlation between melatonin andinsulin levels in patients with type 2 diabetes(55). Furthermore, several studies have shownthat melatonin administration can improve glucosehemostasis, exert antihyperglycemic effects, andimprove endothelial vascular function in experi-mental models of metabolic syndrome and type 2diabetes (56). Faria and colleagues showed thatmelatonin, through melatonin receptors 1 and 2,activates a brain-liver communication and sup-presses hepatic gluconeogenesis via peripheralmuscarinic receptors in rats (57). Evidence from
in-vitro studies have shown that glucose uptakein adipocytes and skeletal muscle cells can beincreased by melatonin (58).
Letrozole is an aromatase inhibitor which islargely used for treatment of breast cancer (34). In2001, Letrozole, for the first time, was described asan ovulation-inducting agent (35). Letrozole inhibitsandrogens-to-estrogens conversion at the GC,resulting in the reduction of estrogen levels, whichconsequently releases the hypothalamus-pituitaryaxis from its negative feedback and increasesthe FSH secretion by pituitary stimulation (35). Inaddition, an inhibition of aromatase activity at theovarian level increases intraovarian androgens thatimprove follicular sensitivity (36). A meta-analysisincluding 26 randomized controlled trials (5,560women) concluded that letrozole therapy appearsto improve live birth and pregnancy rates in anovu-latory PCOS patients compared with clomiphenecitrate (37, 38). Chottanapund and colleagues (59)have evaluated the aromatase suppressive effectsof melatonin on hormonal positive breast cancercells and have shown that melatonin was as potentas letrozole in inhibiting aromatization of androgento estrogen. Furthermore, in several studies, it hasbeen demonstrated that melatonin behaves as aselective estrogen enzyme modulator (SEEM) anda selective estrogen receptor modulator (SERM)(40). Moreover, the aromatase-suppressive effectof melatonin has been also shown in various cells,such as breast cancer, glioma, and endothelialcells (42). Several studies have demonstrated thatmelatonin reduces obesity and restores adipokinepatterns and ameliorates the proinflammatorystate, which underlies the development of insulinresistance (60). These findings all together showthat the use of melatonin due to its aromatase-modulating activity, as well as its reducing effectson hepatic gluconeogenesis, ameliorating the pro-inflammatory state present in PCOS, improvementof glucose uptake by peripheral tissues, and the
Page 874 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
subsequent reduction in insulin levels, may beeffective in the management of PCOS patients(Table II).
3.6. Melatonin in PCOS patientsundergoing assisted reproductivetechnology (ART) treatment
PCOS affects ART outcomes and controlledovarian hyperstimulation (COH) with conventionalprotocols leads to a higher risk of ovarian hyper-stimulation syndrome (OHSS) (61). Several studieshave demonstrated that the poor fertilization, lowoocyte, and embryo quality adversely influencethe clinical outcomes in PCOS patients undergoingART treatment (62). Insulin resistance of ovarianGC and overexpression of vascular endothelialgrowth factor (VEGF) due to insulin stimulationare proposed to be the underlying mechanisms ofpoor clinical outcomes (63). Melatonin may affectovarian microenvironment by improving insulinresistance. In a randomized double-blind trial ofPCOS patients, the administration of melatoninwithmyo-inositol enhanced the oocyte and embryoquality (64). The main goal in COH of PCOSpatients is to prevent OHSS. The only way toprevent all type of OHSS in ART treatment is in-vitromaturation (IVM) followed by in-vitro fertilization(IVF) since this approach avoids the activation ofVEGF-mediated processes (65). However, despitethe extensive research conducted so far, IVM isstill a suboptimal procedure and the applicationof IVM in infertility treatment remains immature(66). The IVM involves additional procedures thatincrease oxidative stress in oocytes and embryosand reduce the developmental competence ofoocytes, in comparison to the conventional IVF (67).The effects of melatonin on oocyte and embryoquality and ART outcomes are discussed in thefollowing sections of this review.
3.7. Fertility and pregnancy
Recently, several studies evaluated the effectsof melatonin in the treatment of PCOS to improvefertility and hormonal alterations. Lemos and col-leagues have shown that rat models of PCOShave lower weight gain during pregnancy andshow reduced numbers of implantation sites whichresult in a decreased number of offspring. Also,rat models of PCOS have higher collagen contentin the uterine horns which hinders the blastocyst-endometrial interactions and reduces the implan-tation rate (68). Co-treatment of melatonin andmetformin can reverse the reduced weight gainand the high collagen fiber content of uterine hornsin the PCOS group, compared to the control group.Moreover, the number and weights of the offspring,the blastocyst-endometrium interactions, and thefetal development were increased while the timerequired for pregnancy was decreased (68). Insome recent studies, it has been reported thatoral administration of melatonin has no significanteffects on clinical pregnancy rate or oocyte andembryo qualities (69).
3.8. Oocyte maturation
Follicular fluid melatonin produced by theluteinizing GC in the late folliculogenesis periodhas a substantial function in the growth and mat-uration of mammalian oocytes (47). In the ovary,melatonin receptors in granulosa-lutein cells canregulate the function of this organ by controllingprogesterone secretion in addition to LH andGnRH receptors gene expression via pathwayssuch as mitogen-activated protein kinase andactivation of Elk-1 (22). Melatonin concentrationsare significantly higher in larger follicles, particu-larly in preovulatory follicles, due to participationin the secretion of progesterone and maturationof oocyte along with subsequent ovulation and
https://doi.org/10.18502/ijrm.v17i12.5789 Page 875

International Journal of Reproductive BioMedicine Mojaverrostami et al.
luteinization events (70). Interestingly, intrafollicularmelatonin level is considerably lower in PCOSwomen than the healthy women which may be thereason for the anovulation and low oocyte quality(32).
The supplementation of culture medium withdifferent substances can increase oocyte mat-uration and IVF, as a remedy for reproductiveproblems (71). Based on these findings, a numberof studies were designed, using supplementationof culture media by melatonin to enhance oocytematuration and embryonic development. In a studyby Kim and colleagues, melatonin concentrationgradually increased in the culture media of GCdue to its production by GC. Also, the addition ofmelatonin to IVM media improved the cytoplasmicmaturation of immature oocytes and increasedthe rates of implantation (72). The amplification ofmRNA expression of the enzymes that participatein melatonin production in cultured GC includingacetylserotonin O-methyltransferase (ASMT) andaralkylamine N-acetyltransferase (AANAT) has alsobeen shown. PCOS results in anovulation andis considered an important cause of IVF failure.Melatonin along with other substances such asmyo-inositol was identified as a good predictor forIVF outcomes, and their high concentrations werean indicator of appropriate quality of oocytes (32).Oral administration of melatonin in combinationwith myo-inositol in PCOS patients enhanced thequality of the oocyte and embryo, increased thenumber of mature oocytes, and finally resultedin an increased concentration of follicular fluidmelatonin (64). In another study, the beneficialeffect of melatonin on the quality of oocytes inPCOS patients during IVM with different melatoninconcentrations was investigated. Also, melatoninproved to be effective in the stimulation of nuclearmaturation of oocytes as well as in increasingthe cleavage rate via regulating free radicals to acertain level required for increasing maturation rate
(73). This effect of melatonin on oocyte maturationhad a dose-dependent pattern in a manner thatlower doses were more effective on maturationrate.
3.9. Histological changes in the ovary
In one study, the histopathological inspectionof the ovary and uterus showed reductions inneoplastic endometrial glands and cystic folliclesin PCOS rats following melatonin treatment (56).In another study, the administration of melatoninreduced cystic follicles and thickness of the thecalayer and increased the number of corpus luteumand the granulosa layer thickness (74). The reduc-tion in the thickness of theca interna is due to theaction of melatonin on the reduction of androgenproduction in the ovary (75). Melatonin showedprotective effects on corpus luteum against ROSvia its antioxidant effects (76). The absence ofmelatonin in pinealectomized animals causes thedevelopment of ovarian cysts due to the modifica-tion of the synthesis of LH and FSH. Increase in theLH levels is a major abnormality detected in PCOS(77). Similarly, constant illumination, an inductionmodel of PCOS in rats, have shown permanentestrous condition and polycystic ovaries aspect(78). In one study, pinealectomy and continuouslight were used separately in female rats to inducePCOS. In both of these methods, the productionof melatonin was diminished and PCOS conditionwas observed. In the group treated with melatonin,a significant reduction in the number and sizeof cysts were observed, probably as a result ofthe antigonadotrophic effects of melatonin (79).Melatonin has shown protective effects againstmetabolic and reproductive abnormalities in animalmodels of PCOS (56, 80). Melatonin treatment inPCOS patients significantly affects body character-istics including reduced body weight, body massindex, and intra-abdominal fat (56).
Page 876 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
3.10. Antioxidant effects
Several studies revealed that oxidative stress isone of the main reasons for female reproductivesystem disorders such as infertility, endometrio-sis, and PCOS (81). This has been supported bythe fact that PCOS patients have higher levelsof oxidative stress compared to healthy women(45, 82). It has been demonstrated that PCOSpatients are at risk of cardiovascular diseases dueto their higher exposure to oxidative stress andthe following undesirable effects such as bloodpressure and insulin resistance (45). Lemos andcolleagues showed that animal models of PCOSinduced by constant illumination had higher levelsof lipid peroxidation, which leads to increases inoxidative stress, pro-oxidant enzymes, and pro-inflammatory cytokines (83). Treatment with a com-bination of metformin hydrochloride and melatoninwas shown to be advantageous in the PCOSgroup by regulating plasmatic variables of oxidativestress, for example, reduction of nitric oxide andtotal glutathione levels. Furthermore, treatmentwith melatonin apparently reduced liver toxicity,pro-inflammatory cytokines, TNF-α and IL-1 and thepro-inflammatory enzymes iNOS (83). Similarly, indifferent studies, the antioxidant effect of melatoninalong with its inhibitory effects on pro-oxidantenzymes and pro-inflammatory cytokines werereported (84).
Melatonin supplementation to the culturemedium has been shown to increase the oocytematuration rate and reduce ROS production (85).It can promote the expression of superoxidedismutase and glutathione peroxidase (86); also,melatonin is able to quench ROS and reactivenitrogen species (RNS) (76). Scavenging action ofmelatonin plays a valuable role during ovulation,because ovulation is an inflammatory process,and reactive species are generated and releasedin the follicular fluid (87). Therefore, melatonin
quenches ROS and RNS and protects GC andoocyte during ovulation (32). Studies have alsodisplayed that oxidative stress is detrimental tooocyte maturation, since the activation of oxidativestress pathway in follicular and IVM medium isunavoidable due to cellular metabolism and lackof antioxidant mechanisms, melatonin is a suitablecandidate to be added to the IVM medium (73,88).
3.11. Melatonin and menstrual cyclicityin PCOS
Menstrual cycle irregularities are among themajor complications of PCOS that affect the qualityof life of patients leading to infertility (89). Thealtered steroid sex hormones in PCOS patientsaffect the hypothalamic-pituitary-ovarian axis andlead to the failure of follicular maturation andovulation (89). Furthermore, hyperinsulinemia andinsulin resistance cause ovarian dysfunction (90).These events result in anovulation and inadequatehormonal levels leading to irregularities in men-strual cycle.
Melatonin seems to promote follicular matu-ration and ovulation through the protection offollicles against oxidative stress and their rescueform atresia (40). After six months of melatonintherapy in 40 normal-weight PCOS patients, men-strual irregularities and hyperandrogenism wereimproved. The lack of significant alterations in thesecretion of insulin and insulin sensitivity suggeststhat melatonin may act on the ovary throughan independent mechanism (91). However, theeffect of long-term melatonin therapy with the aimof menstrual cyclicity improvement needs to beevaluated in large-scale prospective randomizedstudies.
Thanks to the highly selective effects of mela-tonin on its receptors and therefore an excellent
https://doi.org/10.18502/ijrm.v17i12.5789 Page 877

International Journal of Reproductive BioMedicine Mojaverrostami et al.
safety profile, it is well tolerated (92). However,more studies are required to be carried out in order
to shed light on the possibility of its application inthe context of PCOS.
Figure 2. The role of melatonin in the pathogenesis of PCOS.
4. Discussion
The current review summarizes the role of mela-tonin in the pathogenesis of PCOS and the protec-tive effects of exogenous melatonin administrationin the regulation of reproductive function in thecontext of PCOS. Melatonin levels in serum andfollicular fluid of PCOS patients are different fromhealthy women. In PCOS patients, melatonin level
in serum is usually higher than in healthy women,which is considered as a sign of diagnosing PCOS(32). But a reverse condition occurs in melatoninlevel of follicular fluid. Due to fewer uptakes ofmelatonin in ovarian follicle in PCOS patientsagainst healthy women, follicular fluid containslesser melatonin level compared to the healthycondition (32). Melatonin seems to promote follicu-lar maturation and ovulation through the protection
Page 878 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
of follicles against oxidative stress and their rescueform atresia (40). Furthermore, melatonin showedprotective effects on corpus luteum against ROSvia its antioxidant effects (76). Melatonin levelin follicular fluid of PCOS women is notablylower than in healthy women, which is relatedto the ovulation problems. It has been reportedthat melatonin administration can compensate thereduction of this hormone in follicular fluid andcan halt ovulation problems (32). Melatonin treat-ment indicated protective effects against metabolicand reproductive abnormalities in PCOS patients.Melatonin administration in PCOS patients sig-nificantly affects body characteristics includingreduced body weight, body mass index and intra-abdominal fat (56). During the ovulatory process,ROS are produced within the follicles; for this rea-son, the scavenging activity of melatonin plays animportant role during ovulation. Melatonin reducesoxidative stress and causes oocyte maturation andluteinization of GC making it as an effective treat-ment for PCOS patients. Intra-follicular melatoninconcentration was considerably lower in PCOSpatients giving rise to anovulation and poor oocytequality in these patients. The administration ofmelatonin alone or in combination with other drugsin PCOS women has been shown to increase theintrafollicular melatonin concentration, reduce theintrafollicular oxidative stress, and also increasesthe fertilization and pregnancy rates. Melatoninalso improves the production of progesterone fromcorpus luteum in PCOS patients. The deficiency ofmelatonin alters gonadotrophin secretion, reducesthe synthesis of FSH, and increases the synthesisof LH, the latter being the major change detectedin PCOS patients (77). Melatonin can adjust thehypothalamic axis by inhibiting the release of hor-mones such as FSH, which leads to the reductionof cystic follicles. Melatonin can also regulate thesynthesis of GnRH through its receptors in thegranulosa-luteal cells via inhibiting GnRH receptor
expression and sustaining the corpus luteumwhichmaintains progesterone secretion (93).
5. Conclusion
In summary, metabolic dysfunction is the majorfinding contributing to the initiation of PCOS, mela-tonin can hinder this process via its improvingeffects on metabolic functions. Melatonin treat-ment in PCOS patients can enhance the qualityof the oocyte and embryo, increase the numberof mature oocytes, reduce obesity, and amelioratethe proinflammatory state, which underlies thedevelopment of insulin resistance.
Conflict of Interest
All authors declare no conflicts of interest.
References
[1] Shaikh N, Dadachanji R, Mukherjee S. Genetic Markersof Polycystic Ovary Syndrome: Emphasis on Insulin Resis-tance. International Journal of Medical Genetics 2014;2014:1–10.
[2] Rotterdam ESHRE/ASRM-Sponsored PCOS consensusworkshop group. Revised 2003 consensus on diagnosticcriteria and long-term health risks related to polycysticovary syndrome (PCOS). Hum Reprod 2004;19: 41–47.
[3] Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E,Escobar-Morreale HF, Futterweit W, et al. The Androgenexcess and PCOS society criteria for the polycystic ovarysyndrome: the complete task force report. Fertil Steril2009; 91: 456–488.
[4] DeUgarte CM, Bartolucci AA, Azziz R. Prevalence of insulinresistance in the polycystic ovary syndrome using thehomeostasis model assessment. Fertil Steril 2005; 83:1454–1460.
[5] Dunaif A. Perspectives in polycystic ovary syndrome: fromhair to eternity. J Clin Endocrinol Metab 2016; 101: 759–768.
[6] Heidari Khoei H, Dehdehi L, Moloudizargari M, BaninamehZ, Rezaie-Chamani S, Gea Conti O, et al. Female obesityand clinical outcomes of assisted reproductive technolo-gies (ART): An updated systematic review and Meta-Analysis. Int J Med Res Health Sci 2016; 5: 157–170.
[7] Morgante G, Massaro MG, Di Sabatino A, Cappelli V, DeLeo V. Therapeutic approach for metabolic disorders andinfertility in women with PCOS. Gynecol Endocrinol 2018;34: 4–9.
https://doi.org/10.18502/ijrm.v17i12.5789 Page 879

International Journal of Reproductive BioMedicine Mojaverrostami et al.
[8] Sirmans SM, Pate KA. Epidemiology, diagnosis, and man-agement of polycystic ovary syndrome. Clin Epidemiol2013; 6: 1–13.
[9] Asghari MH, Moloudizargari M, Bahadar H, Abdollahi M. Areview of the protective effect of melatonin in pesticide-induced toxicity. Expert Opin Drug Metab Toxicol 2017; 13:545–554.
[10] Asghari MH, Moloudizargari M, Ghobadi E, Fallah M,Abdollahi M. Melatonin as a multifunctional anti-cancermolecule: Implications in gastric cancer. Life Sci 2017; 185:38–45.
[11] Asghari MH, Moloudizargari M, Baeeri M, Baghaei A,Rahimifard M, Solgi R, et al. On the mechanisms of mela-tonin in protection of aluminum phosphide cardiotoxicity.Arch Toxicol 2017; 91: 3109–3120.
[12] Reiter RJ, Tan DX, Tamura H, Cruz MH, Fuentes-Broto L.Clinical relevance of melatonin in ovarian and placentalphysiology: a review.Gynecol Endocrinol 2014; 30: 83–89.
[13] Asghari MH, Abdollahi M, Oliveira MR, Nabavi SM.A review of the protective role of melatonin duringphosphine−induced cardiotoxicity: focus onmitochondrialdysfunction, oxidative stress and apoptosis. J PharmPharmacol 2017; 69: 236–243.
[14] Moradkhani F, Moloudizargari M, Fallah M, Asghari N,Heidari Khoei H, Asghari MH. Immunoregulatory roleof melatonin in cancer. J Cell Physiol 2019; 4: doi:10.1002/jcp.29036.
[15] Moloudizargari M, Moradkhani F, Asghari N, Fallah M,Asghari MH, Moghadamnia AA, et al. NLRP inflammasomeas a key role player in the pathogenesis of environmentaltoxicants. Life Sci 2019; 231: 116585.
[16] Goradel NH, Asghari MH, Moloudizargari M, NegahdariB, Haghi-Aminjan H, Abdollahi M. Melatonin as an angio-genesis inhibitor to combat cancer: Mechanistic evidence.Toxicol Appl Pharmacol 2017; 335: 56–63.
[17] Berson DM, Dunn FA, Takao M. Phototransduction byretinal ganglion cells that set the circadian clock. Science2002; 295: 1070–1073.
[18] Kohsaka A, Bass J. A sense of time: how molecular clocksorganize metabolism. Trends Endocrinol Metab 2007; 18:4–11.
[19] Reiter RJ, Tan DX, Manchester LC, Paredes SD, MayoJC, Sainz RM. Melatonin and reproduction revisited. BiolReprod 2009; 81: 445–456.
[20] Tan DX, Manchester LC, Hardeland R, Lopez−Burillo S,Mayo JC, Sainz RM, et al. Melatonin: a hormone, a tissuefactor, an autocoid, a paracoid, and an antioxidant vitamin.J Pineal Res 2003; 34: 75–78.
[21] ItohMT, Ishizuka B, Kudo Y, Fusama S, Amemiya A, Sumi Y.Detection of melatonin and serotonin N-acetyltransferaseand hydroxyindole-O-methyltransferase activities in ratovary. Mol Cell Endocrinol 1997; 136: 7–13.
[22] Reiter RJ, Tamura H, Tan DX, Xu XY. Melatonin andthe circadian system: contributions to successful femalereproduction. Fertil Steril 2014; 102: 321–328.
[23] Majumdar A, Sharma MN. Anovulatory Infertility. In: KaminiAR. Principles & Practice of Assisted Reproductive Tech-nology. New Delhi, India: Jaypee Brothers Medical Pub-lishers LTD., 2014.
[24] McCartney CR, Eagleson CA, Marshall JC. Regulation ofgonadotropin secretion: implications for polycystic ovary
syndrome. Seminars in reproductive medicine. SeminReprod Med 2002; 20: 317–326.
[25] Johansson J, Stener-Victorin E. Polycystic ovary syn-drome: effect and mechanisms of acupuncture for ovu-lation induction. Evid Based Complement Alternat Med2013; 2013: 762615.
[26] Kelly CJ, Stenton SR, Lashen H. Insulin-like growth factorbinding protein-1 in PCOS: a systematic review and meta-analysis. Hum Reprod Update 2011; 17: 4–16.
[27] Azziz R, Black VY, Knochenhauer ES, Hines GA, BootsLR. Ovulation after glucocorticoid suppression of adrenalandrogens in the polycystic ovary syndrome is not pre-dicted by the basal dehydroepiandrosterone sulfate level.J Clin Endocrinol Metab 1999; 84: 946–950.
[28] Fassnacht M, Schlenz N, Schneider SB, Wudy SA, Allolio B,Arlt W. Beyond adrenal and ovarian androgen generation:increased peripheral 5α-reductase activity in women withpolycystic ovary syndrome. J Clin Endocrinol Metab 2003;88: 2760–2766.
[29] Polak K, Czyzyk A, Simoncini T, Meczekalski B. Newmarkers of insulin resistance in polycystic ovary syndrome.J Endocrinol Invest 2017; 40: 1–8.
[30] Corbould A. Chronic testosterone treatment inducesselective insulin resistance in subcutaneous adipocytes ofwomen. J Endocrinol 2007; 192: 585–594.
[31] Diamanti-Kandarakis E. Role of obesity and adiposity inpolycystic ovary syndrome. Int J Obes 2007; 31 (Suppl.):S8–S13.
[32] Tamura H, Nakamura Y, Korkmaz A, Manchester LC, TanDX, Sugino N, et al. Melatonin and the ovary: physiologicaland pathophysiological implications. Fertil Steril 2009; 92:328–343.
[33] Luboshitzky R, Shen-Orr Z, Herer P, Nave R. Uri-nary 6-sulfatoxymelatonin excretion in hyperandrogenicwomen with polycystic ovary syndrome: the effect ofethinyl estradiol-cyproterone acetate treatment. GynecolEndocrinol 2003; 17: 441–447.
[34] Luboshitzky R, Herer P, Shen-Orr Z. Urinary 6-sulfatoxymelatonin excretion in hyperandrogenic women:the effect of cyproterone acetate-ethinyl estradioltreatment. Exp Clin Endocrinol Diabetes 2004; 112:102–107.
[35] Luboshitzky R, Qupti G, Ishay A, Shen-Orr Z, FutermanB, Linn S. Increased 6-sulfatoxymelatonin excretion inwomen with polycystic ovary syndrome. Fertil Steril 2001;76: 506–510.
[36] Daya S, Potgieter B. The effect of castration, testosteroneand estradiol on14C-serotonin metabolism by organ cul-tures of male rat pineal glands. Experientia 1985; 41: 275–276.
[37] Hayashi K, Okatani Y. Mechanisms underlying the effectsof estrogen on nocturnal melatonin synthesis in peripuber-tal female rats: relation to norepinephrine and adenylatecyclase. J Pineal Res 1999; 26: 178–183.
[38] Kruijver FP, Swaab DF. Sex hormone receptors are presentin the human suprachiasmatic nucleus. Neuroendocrinol-ogy 2002; 75: 296–305.
[39] Tanavde VS, Maitra A. In vitro modulation of steroidogene-sis and gene expression bymelatonin: a studywith porcineantral follicles. Endocr Res 2003; 29: 399–410.
Page 880 https://doi.org/10.18502/ijrm.v17i12.5789

International Journal of Reproductive BioMedicine Melatonin in PCOS
[40] Jain P, Jain M, Haldar C, Singh TB, Jain S. Melatoninand its correlation with testosterone in polycystic ovariansyndrome. J Hum Reprod Sci 2013; 6: 253–258.
[41] Andreeva E, Absatarova Y, Sheremetyeva E, Derkatch D,Ponomareva T, Tiulpakov A, et al. Analysis of the infor-mativeness of melatonin evaluation in polycystic ovarysyndrome. Obesity and Metabolism 2016; 13: 15–20.
[42] ShreeveN, Cagampang F, Sadek K, Tolhurst M, Houldey A,Hill CM, et al. Poor sleep in PCOS; is melatonin the culprit?Hum Reprod 2013; 28: 1348–1353.
[43] Basheer M, Rai S. Melatonin vs. phytomelatonin: Thera-peutic uses with special reference to polycystic ovariansyndrome (PCOS). Cogent Biol 2016; 2: 1136257.
[44] González F, Rote NS, Minium J, Kirwan JP. Reactive oxy-gen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndrome. J Clin Endocrinol Metab 2006;91:336–340.
[45] Sabuncu T, Vural H, HarmaM, HarmaM.Oxidative stress inpolycystic ovary syndrome and its contribution to the riskof cardiovascular disease. Clin Biochem 2001; 34: 407–413.
[46] Gupta RK, Miller KP, Babus JK, Flaws JA. Methoxychlorinhibits growth and induces atresia of antral folliclesthrough an oxidative stress pathway. Toxicol Sci 2006; 93:382–389.
[47] Reiter RJ, Tan DX, Maldonado MD. Melatonin as anantioxidant: physiology versus pharmacology. J Pineal Res2005; 39: 215–216.
[48] Tan DX, Reiter RJ, Manchester LC, Yan MT, El-Sawi M,Sainz RM, et al. Chemical and physical properties andpotential mechanisms: melatonin as a broad spectrumantioxidant and free radical scavenger. Curr Top MedChem 2002; 2: 181–197.
[49] Terzieva DD, Orbetzova MM, Mitkov MD, Mateva NG.Serum melatonin in women with polycystic ovary syn-drome. Folia Med 2013; 55: 10–15.
[50] Zafari Zangeneh F, Naghizadeh MM, Abdollahi A, BagheriM. Synchrony between ovarian function & sleep in polycys-tic ovary syndrome patients. Open Journal of Obstetricsand Gynecology 2014; 4: 725–731.
[51] Wang L, Wang Y, Zhang X, Shi J, Wang M, Wei Z,et al. Common genetic variation in MTNR1B is associatedwith serum testosterone, glucose tolerance, and insulinsecretion in polycystic ovary syndrome patients. FertilSteril 2010; 94: 2486–2489.
[52] Li C, Shi Y, You L, Wang L, Chen ZJ. Melatonin receptor1A gene polymorphism associated with polycystic ovarysyndrome. Gynecol Obstet Invest 2011; 72: 130–134.
[53] Li C, Shi Y, You L, Wang L, Chen ZJ. Association ofrs10830963 and rs10830962 SNPs in themelatonin recep-tor (MTNR1B) gene among Han Chinese women withpolycystic ovary syndrome.Mol Hum Reprod 2011; 17: 193–198.
[54] Song X, Sun X, Ma G, Sun Y, Shi Y, Du Y, et al. Fam-ily association study between melatonin receptor genepolymorphisms and polycystic ovary syndrome in HanChinese. Eur JObstet Gynecol ReprodBiol 2015; 195: 108–112.
[55] Peschke E, Frese T, Chankiewitz E, Peschke D, PreissU, Schneyer U, et al. Diabetic Goto Kakizaki rats as
well as type 2 diabetic patients show a decreased diur-nal serum melatonin level and an increased pancreaticmelatonin−receptor status. J Pineal Res 2006; 40: 135–143.
[56] Pai SA, Majumdar AS. Protective effects of melatoninagainst metabolic and reproductive disturbances in poly-cystic ovary syndrome in rats. J Pharm Pharmacol 2014;66: 1710–1721.
[57] Faria JA, Kinote A, Ignacio-Souza LM, de Araújo TM, RazolliDS, Doneda DL, et al. Melatonin acts through MT1/MT2receptors to activate hypothalamic Akt and suppresshepatic gluconeogenesis in rats. Am J Physiol EndocrinolMetab 2013; 305: E230–E242.
[58] Ha E, Yim SV, Chung JH, Yoon KS, Kang I, Cho YH, et al.Melatonin stimulates glucose transport via insulin recep-tor substrate−1/phosphatidylinositol 3−kinase pathway inC2C12 murine skeletal muscle cells. J Pineal Res 2006; 41:67–72.
[59] Chottanapund S, Van DuursenMB, Navasumrit P, HunsontiP, Timtavorn S, Ruchirawat M, et al. Anti-aromatase effectof resveratrol and melatonin on hormonal positive breastcancer cells co-cultured with breast adipose fibroblasts.Toxicol In Vitro 2014; 28: 1215–1221.
[60] Al-Qadhi HI. Effect of melatonin supplementation onserum LH level and BMI in women with polycystic ovariansyndrome. J Pharm Sci Res 2018; 10: 1–4.
[61] Swanton A, Storey L, McVeigh E, Child T. IVF outcome inwomen with PCOS, PCO and normal ovarian morphology.Euro J Obstet Gynecol Reprod Biol 2010; 149: 68–71.
[62] Raju GA, Chavan R, Deenadayal M, Gunasheela D,Gutgutia R, Haripriya G, et al. Luteinizing hormone andfollicle stimulating hormone synergy: a review of role incontrolled ovarian hyper-stimulation. J Hum Reprod Sci2013; 6: 227–234.
[63] Doronzo G, Russo I, Mattiello L, Anfossi G, Bosia A, TrovatiM. Insulin activates vascular endothelial growth factor invascular smooth muscle cells: influence of nitric oxide andof insulin resistance. Eur J Clin Invest 2004; 34: 664–673.
[64] Pacchiarotti A, Carlomagno G, Antonini G, Pacchiarotti A.Effect of myo-inositol and melatonin versus myo-inositol,in a randomized controlled trial, for improving in vitrofertilization of patients with polycystic ovarian syndrome.Gynecol Endocrinol 2016; 32: 69–73.
[65] Rose BI. Avoidance of severe ovarian hyperstimulationwith IVM treatment. Development of In Vitro Maturation forHuman Oocytes: Springer; 2017.
[66] Virant-Klun I, Krijgsveld J, Huntriss J, Rodgers RJ. Newadvances in reproductive biomedicine. Biomed Res Int2014; 2014: 529170.
[67] Hao Y, Zhang Z, Han D, Cao Y, Zhou P, Wei Z, et al. Geneexpression profiling of human blastocysts from in vivo and‘rescue IVM’with or without melatonin treatment. Mol MedRep 2017; 16: 1278–1288.
[68] de Lemos AJJM, Costa FS, Peixoto CA, Teixeira ÁAC, daSilva SB, Ferreira CGM, et al. Combination of melatoninand metformin hydrochloride for treatment polycysticovarian in female rats. Acta Scientiae Veterinariae 2016;44: 1–10.
[69] Fernando S, Wallace EM, Vollenhoven B, Lolatgis N, HopeN, Wong M, et al. Melatonin in assisted reproductivetechnology: a pilot double-blind randomized placebo-controlled clinical trial. Front Endocrinol 2018; 9: 545.
https://doi.org/10.18502/ijrm.v17i12.5789 Page 881

International Journal of Reproductive BioMedicine Mojaverrostami et al.
[70] Tamura H, Takasaki A, Taketani T, Tanabe M, Kizuka F, LeeL, et al. Melatonin as a free radical scavenger in the ovarianfollicle. Endocr J 2013; 60: 1–13.
[71] Entezari Najafabadi M, Karimpour Malekshah A, Esmailne-jad Moghaddam A, Ghasemi Hamidabadi H, Heidari M.Effect of embryonic fibroblast cells conditioned mediumon in vitro maturation of immature mouse oocytes. JMazandaran Univ Med Sci 2014; 23: 107–114.
[72] Kim MK, Park EA, Kim HJ, Choi WY, Cho JH, Lee WS,et al. Does supplementation of in-vitro culture mediumwith melatonin improve IVF outcome in PCOS? ReprodBiomed Online 2013; 26: 22–29.
[73] Nikmard F, Hosseini E, Bakhtiyari M, Ashrafi M, Amidi F,Aflatoonian R. Effects of melatonin on oocyte maturationin PCOS mouse model. Anim Sci J 2017; 88: 586–592.
[74] Ahmadi M, Rostamzadeh A, Fathi F, Mohammadi M, RezaieMJ. The effect of Melatonin on histological changes ofovary in induced polycystic ovary syndromemodel inmice.Middle East Fertility Society Journal 2017; 22: 255–259.
[75] Rocha RM, Lima LF, Alves AM, Celestino JJ, MatosMH, Lima-Verde IB, et al. Interaction between mela-tonin and follicle-stimulating hormone promotes in vitrodevelopment of caprine preantral follicles. Domest AnimEndocrinol 2013; 44: 1–9.
[76] Galano A, Tan DX, Reiter RJ. Melatonin as a natural allyagainst oxidative stress: a physicochemical examination. JPineal Res 2011; 51: 1–16.
[77] Polson DW, Wadsworth J, Adams J, Franks S. Polycysticovaries-a common finding in normal women. The Lancet1988; 331: 870–872.
[78] Kang X, Jia L, Shen X. Manifestation of hyperandrogenismin the continuous light exposure-induced PCOS rat model.Biomed Res Int 2015; 2015: 943694.
[79] Prata Lima MF, Baracat EC, Simões MJ. Effects of mela-tonin on the ovarian response to pinealectomy or contin-uous light in female rats: similarity with polycystic ovarysyndrome. Braz J Med Biol Res 2004; 37: 987–995.
[80] Basheer M, Rai S, Ghosh H, Ahmad Hajam Y. Therapeuticefficacy of melatonin against polycystic ovary syndrome(pcos) induced by letrozole in wistar rat. Pak J Biol Sci2018; 21: 340–347.
[81] Giannetto A, Fernandes JM, Nagasawa K, Mauceri A,Maisano M, De Domenico E, et al. Influence of continuouslight treatment on expression of stress biomarkers inAtlantic cod. Dev Comp Immunol 2014; 44: 30–34.
[82] Fenkci V, Fenkci S, Yilmazer M, Serteser M. Decreasedtotal antioxidant status and increased oxidative stress inwomen with polycystic ovary syndrome may contribute to
the risk of cardiovascular disease. Fertil Steril 2003; 80:123–127.
[83] Lemos AJ, Peixoto CA, Teixeira ÁA, Luna RL, Rocha SW,Santos HM, et al. Effect of the combination of metforminhydrochloride and melatonin on oxidative stress beforeand during pregnancy, and biochemical and histopatho-logical analysis of the livers of rats after treatment forpolycystic ovary syndrome. Toxicol Appl Pharmacol 2014;280: 159–168.
[84] Kim JB, Jung JY, Ahn JC, Rhee CK, Hwang HJ. Antioxidantand anti-apoptotic effect of melatonin on the vestibularhair cells of rat utricles. Clin Exp Otorhinolaryngol 2009;2: 6–12.
[85] Kang JT, Koo OJ, Kwon DK, Park HJ, Jang G, KangSK, et al. Effects of melatonin on in vitro maturation ofporcine oocyte and expression of melatonin receptor RNAin cumulus and granulosa cells. J Pineal Res 2009; 46: 22–28.
[86] Korkmaz A, Rosales-Corral S, Reiter RJ. Gene regulationbymelatonin linked to epigenetic phenomena.Gene 2012;503: 1–11.
[87] Shkolnik K, Tadmor A, Ben-Dor S, Nevo N, Galiani D, DekelN. Reactive oxygen species are indispensable in ovulation.Proc Natl Acad Sci USA 2011; 108: 1462–1467.
[88] Shi JM, Tian XZ, Zhou GB, Wang L, Gao C, Zhu SE, et al.Melatonin exists in porcine follicular fluid and improvesin vitro maturation and parthenogenetic development ofporcine oocytes. J Pineal Res 2009; 47: 318–323.
[89] Van Hooff MH, Voorhorst FJ, Kaptein MB, Hirasing RA,Koppenaal C, Schoemaker J. Polycystic ovaries in adoles-cents and the relationship with menstrual cycle patterns,luteinizing hormone, androgens, and insulin. Fertil Steril2000; 74: 49–58.
[90] Dowdy D. Emotional needs of teens with polycystic ovarysyndrome. J Pediatr Nurs 2012; 27: 55–64.
[91] Tagliaferri V, Romualdi D, Scarinci E, Cicco S, Florio CD,Immediata V, et al. Melatonin treatment may be able torestore menstrual cyclicity in women with pcos: a pilotstudy. Reprod Sci 2018; 25: 269–275.
[92] Wilson SJ, Nutt DJ, Alford C, Argyropoulos SV, BaldwinDS, Bateson AN, et al. British association for psychophar-macology consensus statement on evidence-based treat-ment of insomnia, parasomnias and circadian rhythmdisorders. J Psychopharmacol 2010; 24: 1577–1601.
[93] Chan WY, Ng TB. Effects of pineal indoles on ovarianresponse to gonadotropin-induced ovulation in mice. JNeural Transm Gen Sect 1995; 100: 239–246.
Page 882 https://doi.org/10.18502/ijrm.v17i12.5789
Top Related