






Languages
Pages
Legal


By DR OWADOKUN A.O. MB;BS (Ibadan).
PROBLEMS IN THE PUERPERIUM

IntroductionOverview of some Physiological &Anatomical
changes in the puerperium.Puerperal infections.Secondary post partum haemorrhage.Difficulties in breastfeedingPsychological problems in the puerperium.Conclusion.
Outline.

Puerperium is the postpartum period that lasts from the delivery of the placenta and its membranes until about six weeks after delivery during which anatomical and physiological changes of pregnancy,labour and delivery are reversed to an almost prepregnancy level.
Puerperium is easily overlooked by obstetricians due to the sense of achievement felt after the delivery of a live infant by a healthy mother .
Introduction.

Puerperium is divided into three periods;-Immediate puerperium: up to 24hrs after
delivery-Early puerperium:between second to seventh
day after delivery.-Late puerperium :from second week to sixth
week after delivery.

Uterine involution-By autolysis the uterus is markedly reduced in
size and wgt from the immediate postpartum wght of abt 1000g (abt 20wk size)to <100g over 6 wks.
-changes are dramatic within the 1st wk.Abt 500g at end of 1st wk.By end of 2nd wk ,no longer palpable above the symphysis pubis.
-observed changes in total area of uterus ,due to changes in uterine length as transverse diameter remains relatively constant.
Physiological and Anatomical Changes In The Puerperium

By the end of 1st wk,there is evidence of endometrial regeneration and completion within 3wks,however regeneration of placenta site progresses slowly and may extend to 8th wk
Rate of endometrial regeneration is influenced by feeding option.
Involution is faster in the breastfeeding and uterus is smaller than in the non breastfeeding.
Uterine involution(contd).

Lochia:-Normal postpartum discharge,alkaline,consists
of ;erythrocytes,decidua shreds,epithelia cells,cervical mucus,vaginal transudate and bacteria.

-Lochia rubra(red);consists mainly of blood and decidua ,tapers in amount,gradually changes to reddish brown color ,usu lasts 3-4 days.
-Lochia serosa(pale);serous to mucopurulent,often malodourous,there’s relative decrease in RBCs wt predominance of leucocytes,has a mean duration of abt 22-27 days.

10-15% of women have lochia serosa for at least 6wks
-Lochia alba(white);lochia is thicker,yellowish white,there’s predominance of leucocytes,degenerated decidua cells and mucus.
-usu by 5-6th wk lochia secretion ceases.-persistent red lochia suggests delayed
involution,usu associated wt infxn or RPC.

Elevated prolactin in breastfeeding women inhibits GnRH,FSH and LH wt resultant amenorrhoea.
In lactating women menses b/4 6mnths is mostly anovulatory,incidence of ovulation is as low as 1-5%.
Mean post delivery ovulation time in the non lactating is 70-75 days can occur as early as 27 days.Menses return in 7-9wks.
Mean ovulation time in lactating women is abt 190 days and menses may not occur for as long as 36 mnths.
Ovarian function.

Approximately 10-13kg is gained in pregnancy.There’s immediate loss of 4-6kg postpartum due to
delivery of fetus,placenta amniotic fluid and bld loss.By 6wks most women have lost abt 4kg due to
excretion of fluids and electrolytes.Loss of water is greater in preecclamptics and
ecclamptics.Women who did not have excessive wght gain in
pregnancy(>15kg) should have returned to their normal prepregnancy level by 6mnths,while women wt excessive gain may still have abt 5kg excess and this may persist indefinitely.
Weight loss,Fluid balance and Electrolytes

During pregnancy abt 35% increse in bld volume (plasma volume expands abt 1200mls,rbc volume ,abt 250 mls).
Post delivery,there is decrease in plasma vol partly due to bleeding.
Average blood loss in vaginal delivery is abt 500mls and abt 1000mls in C.S.
On 3rd DPP there’s shift from ECF to intravascular compartment wt 900-1200mls increase in intravascular volume.
Within 8wks PP RBC level returns to normal.
Haemodynamic and Haematological changes.

Several clotting factors remain elevated in the early puerperium and return to normal level by 3wks.
Fibrinogen rises in the first week and returns to normal within 6wks.
Platelet count falls in the early puerperium and rises to normal by the 6th wk.
Haemodynamic and Haematological changes(contd).

There’s a transient rise in blood pressure in the first 5 days PP which reflects an increased uterine vascular resistance and a transient increase in plasma volume,wt progressive fall in BP reaching prepregnancy level in most women by 6th wk.
There’s Abt 28% reduction C.O within 2wks.
Haemodynamic and Haematological Changes (contd).

H.R and S.V return to prepregnancy levels by 2nd wk.
Pregnancy induced ventricular hypertrophy resolves within 1yr.
Limited data support slow return of cardiac haemodynamics to prepregnancy level over 1yr.
Resolution in haemodynamics are not affected by lactation
Haemodynamic and Haematological Changes (contd).

Infections are among the most prominent puerperal complications.
Infections may occur in several sites and each need to be investigated in the presence of elevated temperature.
PUERPERAL PYREXIA: - A rise in temperature to 38*C or more on at
least two occasion 4-6hrs apart within 10 days of delivery,exclusive of the 1st 24hrs.
Puerperal pyrexia includes all cases of significant pyrexia in the puerperium.
Puerperal Infections.

A slightly elevated temperature is not uncommon after delivery especially after a difficult labour and delivery or instrumental or abdominal delivery but usually falls to normal within 24hrs.
In abt 80% of women who develop fever in the first 24hrs of delivery,no evidence of infection can be identified.However any pyrexia associated wt tachycardia merits investigation.
Puerperal infections(contd).

Puerperal uterine infections.Perineal infections. Post surgical wound infections.Urinary tract infections.
Common causes of puerperal pyrexia.

Breast infections.Thrombophlebitis.Respiratory tract infections.esp after general
anaesthesia with endotracheal intubation.Other non obstetric causes;malaria,chest
infexn,HIV/AIDS.
Common causes of puerperal pyrexia.

Full clinical investigation.MSU mcsECS&HVS mcsBld culture.Sputum culture(if possible).
Investigations.

The following measures can be taken to minimise puerperal infections;
-shorter labours,-better labour ward techniques,-administration of potent antibiotics.

This is the infection of the genital tract that occurs between delivery of the fetus and 6 wks after delivery.
Aetiology:-Occurs as a result of ascending
infection(vagina to endometrium).-Colonization of the endometrium ,involvement
of the myometrium,tubes and ovaries
Puerperal sepsis.

Infexns are mainly polymicrobial.Examples are streptococci,staphylococci,colliforms,bacteroides,mixe-d anaerobes,pseudomonas and chlamydia .
Anaerobic organisms account for abt 80% of cases.
Complications include,Disseminated intravascular coagulation,septic shock,subsequent infertility and Death.


Predisposing factors;General:-Anaemia-malnutrition-unbooked pts -low socioeconomic status-coitus near term Labour events:-Prolonged rupture of membranes(>24hrs)-chorioamnionitis-Repeated V.Es-IU fetal monitoring

Predisposing factors(contd).Delivery:-haemorrhage-manual placenta removal-episiotomy-genital tract lacerationsOperative risks:-C-section-operative techniques-instrumental deliveries-emergency operations.-poor surgical techniques

Infxn of the endometrial lining.Commonest infxn following
delivery,commoner following CS than vaginal delivery(incidence abt 1-3% ffng vaginal delivery &5-15% ffng CS,can be as high as 30-35% in CS performed for prolonged labour,rupture of membranes wtout a-biotcs.
In high risk pts(DM,anemic,obese etc rates are doubled).
Endometritis

Predisposing factors :-prolonged labour -prolonged rupture of membranes-repeated vaginal examinations during labour-application of internal monitorig devices-retained products of conception-traumatic operative vaginal delivery-APH and PPH

Organisms commonly implicated include;-haemolytic strept(grp B)-gram –ve bacilli(E.coli,klebsiella,proteus,pseudomonas)-gram +ve anaerobes(peptostreptococci and
peptococci)-thrive in the medium of necrotic decidua and RPCs
-staphylococci (not common) and clostridia(occur in EC culture in abt 5% of asymptomatic women,also rare )
- Others;Mycoplasma, ureaplasma urealyticum and chlamydia(causes late indolent metritis cos of its long latent period)

Presentation;-ill pt in the puerperium-c/o fever,lower abdominal pain and offensive
lochia.o/e;-febrile,pale,jaundiced-lower abdominal tenderness,larger for date soft
and tender uterus-offensive lochia-open cervical os in the prescence of RPCs-CET may be elicited,POD may be full and tender

Mgt;-Investigations:FBC,bld culture,platelet
count,HVS/ECS mcs-bld culture-platelet count,HVS/ECS mcs-bld film for MP-Urine mcs-USS

Treatment;-Correct anaemia and malnutrition if present- Empirical Intravenous broad spectrum
antibiotics wt good coverage for anaerobes- Modify a-biotics wt mcs result- Anticoagulation- Wt appropriate a-biotics pt should improve
within 48hrs- Evacuation of RCPs.

Prevention:-preventing and treating anaemia at ANC-preventing prolonged labour-avoiding unnecessary VEs-aseptic techniques in the labour room-use of prophylactic antibiotics at CS may be
helpful

Urinary tract infection;-second only to to genital tract infection as a
cause of puerperal pyrexia.-following delivery bladder and lower genital
tract remain hypotonic wt resultant residual urine and reflux.
-frequent pelvic examination,frequent or prolonged catheterization during labour are risk factors.

-occurs in 3-7% of pt wt asymptomatic bacteriuria in pregnancy
-common organisms:E.coli,s.sapprophyticus,E.fecalis,Proteus,
-sulphonamides,quinolones,amoxycillins ,nitrofurantoin based on MSU mcs are drugs of choice
- liberal fluid intake is encouraged

Wound infections;-General condition of pts prior to
CS,episiotomies or perineal lacerations is paramount to incidence.
-anemia,DM,obesity place pts at risk.-episiotomy infection is generally not common-emergency CS,Prolonged ROM,prolonged
labour,chorioamnionitis poor surgical tecniques,lengthy procedures are risk factors
-Wound mcs, appropriate antibiotics,removal of some or all stitches
- Wound dressing as appropriate.

Abnormal bleeding from the genital tract between 24hrs and 6wks and delivery.
Causes ;-retained placental tissues-intrauterine infection wt or wtout RPCs-subinvolution of the uterus-vulva haematoma-CS incision dehiscence
Secondary postpartum Haemorrhage

Mgt-resuscitate pt,-blood transfusion as needed-uss to detect retained products-antibiotics(broad spectrum+antianaerobes e.g.
metronidazole)-evacuation of the uterus if products of conception
are seen.specimen should be sent for histology-life threatening bleeding may persist after
evacuation.uterine artery embolization,uterine tamponade or hysterectomy may be the last resort.
Secondary postpartum haemorrhage(contd).

-Results from increased coagulation and impaired fibrinolytic activities in pregnancy.
-occur in abt 0.5-1% of pregnancies but commoner in the puerperium
-includes thrombophlebitis,DVT and P.E.
Thromboembolic disorders.

-Inflammation of a vein wt thrombosis-may occur in superficial veins of hand and
forearm following prolonged iv cannulation-overlying skin is inflamed and tender-self limiting and rarely life threatening-inflammatory process may extend to deep
veins if not treated promptly.
Thrombophlebitis

-Now uncommon because of antibiotics use-rarely complicates puerperal pelvic infections-incidence is abt 1% of puerperal endometritis-common form is acute thrombosis of one,usu
right or both ovarian veins-color doppler,CT or MRI are diagnostic tools.
Septic pelvic thrombosis

-antibiotics and heparin are mainstay of treatment.-heparin serum level should be around 0.2-0.7iu/ml-activated partial thrombin time is kept to 2 times
the normal and treatment is for 7-10 days-symptoms should start regressing within 48-72
hrs,otherwise consider ligation of affected vessel(s)or embolectomy.
-excision of infected vessels and adnexa wt or wtout the uterus in the prescence of well defined abscess is considered according to severity
Septic pelvic thrombosis(contd).

-Usually follow operative deliveries when it though other risk factors play
-risk factors include;>35yrs,immobility,obesity,preeclampsia,parity>4,previous DVT and SCA,trauma to legs from stirrup
-clinical features;leg pain and swelling,warmth,lower abdominal pain may be present.Homan’s sign is positive
Deep venous thrombosis

-investigations;doppler uss, x-ray venography,CT
Rx:anticoagulation is the mainstay of treatment. SC low molecular wt heparin has gained acceptance.
-SC heparin prophylaxis in high risk pts ,early mobilization after surgery is preventive,
Deep venous thrombosis(contd).

Breast disorders can be due to poor techniques of breastfeeding
Cracked nipples:-sores on the nipples,usu due to incorrect
positioning and attachment as baby sucks directly from the nipple instead of the areola.
-increased risk of mastitis-candidiasis may also cause soreness-Rx: Rest affected nipple,express milk manually
and reintroduce breastfeeding gradually, application of emollients,use of nipple shields
Problems in Breastfeeding.

Lactation mastitis ;-commoner in primigravidas than in multiparas -can be infective or non infectiveInfective mastitis: -usu affect part of one breast,one quadrant or
one lobule -causative org usu staph aureus,Strept spp
and E.coli are occasionally isolated.-organisms can be introduced from infant’s
nostril to mother’s breast

Two major types;-Cellulitis: connective tissues inbtwn breast
lobes become inflammed and infected. There is fever and general malaise .Breast is tense and tender. No pus can be expressed from the duct.
- Adenitis: the lactiferous sysytem is infected wt pus formation which may be expressed wt milk. Symptoms are similar to cellulitis.

Rx:-Teach correct techniques-Antibiotcs: antistaphs or a cephalosporin-Antiinflammatory-antipyretic analgesics-Local heat and breast support to reduce pain-Suspend breastfeeding in affected breast and
express .Not necessary in cellulitis.

Breast abscess:-usu develop as a complication of untreated
mastitis.-large collection of pus within breast tissues-a segment of the breast is tender and fluctuant -pt often appear toxic-Rx:I&D under G.A.-Antibiotics,usu antistaph-Cessation of breastfeeding.

Breast abscess.

Non infective(congestive)mastitis:-usu occur from 2nd or 3rd DPP-commoner in primigravidas than in multiparas-usu due to inadequate suckling-affect whole of one or both breasts-breasts are swollen and tender,tense and
warm

Rx:-Frequent emptying of breast by frequent
expression,frequent breastfeeding should be encouraged
-For the non breastfeeding,tight breast binding,cold compress,restriction of breast stimulation
-Analgesics to relieve pain-Drug induced supression of lactation may not
be helpful.

Breast Engorgement.

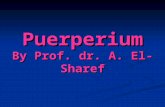
Right Technique of breastfeeding.

ConstitutionalMalnutrition and bad general conditionInfrequent or irregular sucklingSheehan’s syndromeRx;-regular breastfeeding -good diet plenty of fluids
Defficient lactation

-Experience of labour and delivery may be followed by psychological reactions
-3 main types of puerperal psychological disorders exist;
-postpartum blues -postpartum depression -puerperal psychosis
Psychological problems in the puerperium

-mild and transient -incidence abt 50-70%-occurs on any day within 1st wk usu resolve by
10th day-tearful,sad,sleep is
disturbed,restlessness,headaches,poor concentration
-Rx: sympathetic support and understanding,
Postpartum blues

-incidence is abt 10-15%-pks in 3rd-4th wk-2/3rd are selflimiting’1/3rd sustained and severe-50% recurrence in subsequent pregnancy-risk factors include; -age<20yrs
Postpartum depression

-unmarried -low self esteem -poor relationship wt partner and family -financial problems etc-pt is irritable,tired,feels guilty,unable to
cope,undue anxiety-Rx:psychotherapy,support and antidepressant
Postpartum depression

-Incidence is 0.14-0.26%-Usu begins abt 3rd DPP pks in abt2wks PP and
lasts abt 2-3mnths-suicide thoughts and tendencies,can kill their
babies-symptoms;suspicious,deny pregnancy and
babies,delusions,hallucination,confused,cognitive impairment
Puerperal psychosis

-risk factors;previous psychosis,unmarried,CS,infections,perinatal death
-20%in next pregnancy-50%psychotic again later in life-outcome is generally more favourable than
non puerperal psychosis.
Puerperal psychosis

Compared with the dramatic and climatic events of labour and delivery,puerperium may seem uneventful,however,there is need for vigillance during this period as death occuring during this period also qualifies as maternal death.
CONCLUSION

THANK YOU FOR LISTENING!
Top Related