







Languages
Pages
Legal


Jai Radhakrishnan, MDJai Radhakrishnan, MDColumbia University
1. The Patient-Centered Medical Home2. CKD Clinic as the paradigm for PCMH?3. Outcome data 4. The Columbia model5. Limitations6. Financial considerations

Scheduled appointment: (FU 99213: 15 mins) 75 year old patient with diabetes, R leg
amputation, CKD (eGFR 22ml.min)Hi BP i 200/100 3 d His BP is 200/100, 3+ edema
He has run out of medications, (does not remember nothing in the computer)remember, nothing in the computer)
You peep out in the waiting room You give him samples and call him back in 1 You give him samples and call him back in 1
month

RenalRenal OfficeOffice

Planned follow up visit for CKD Arrives with home attendant with BP and
blood sugar readings taken by VNSVi l i h l d b k d Vital signs have already been taken, meds updated by health tech.
CKD CDSS can be accessed online CKD-CDSS can be accessed online Epo and Influenza vaccine is prescribed-given
by NP in Room 2by NP in Room 2 Total visit 30 mins


Frequently, the acute symptoms and concerns of the patient crowd out the less urgent need to bring chronic illness under optimal managementmanagement
Bodenheimer..JAMA. 2002;288:1775-1779.

A physician-directed practice that provides care that is accessible, continuous,comprehensive and coordinated and delivered in the context of family anddelivered in the context of family and community.
The PCMH is a model of comprehensive health care delivery and payment reform that
emphasizes a central role for primary careemphasizes a central role for primary care
Health Aff (Millwood) 27 : 1219 –1230, 2008

Coordinated care by incorporation primary care model and disease management model:◦ reduced emergency department visits◦ fewer hospitalizations◦ fewer hospitalizations◦ less duplication and by incorporating increased use
of the electronic medical record with the chronic d l i l fcare model onto a primary care platform
Receive additional remuneration for coordinating allReceive additional remuneration for coordinating all of the patient's care, from diet to mental health to preventive measures.

Health Care O i ti Community
ResourcesOrganization
Self-management S pport
Delivery System Design SupportSystem Design
D i i S tDecision SupportClinical Information
S tSystemsBodenheimer..JAMA. 2002;288:1775-1779.

Primary care physician (PCP) societies American Medical Association American Association of Retired Persons Labor and consumer organizations Corporations, including IBM and Merck

Blue Cross/Blue Shield United Healthcare Aetna Centers for Medicare and Medicaid Services
(CMS) under Tax Relief and Health Care Act of 2006 to conduct a PCMH demonstrationof 2006 to conduct a PCMH demonstration project beginning in January 2010

1. CKD / ESRD is a growing problem 2. Late referral to nephrology is not goodate e e a to ep o ogy s ot good 3. Nephrologists might do a better job 4. CKD/ ESRD is expensivep

USRDS 2004

*
Adapted from Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. Nov. 7, 2007;298:17.
>20 years old*

16

17

Medicare: period prevalent general Medicare patients age 65 & older, with Medicare as primary payor, & not enrolled in Medicare Advantage Medstat: period prevalent patients age 50 64 enrolled in a fee fornot enrolled in Medicare Advantage. Medstat: period prevalent patients age 50–64, enrolled in a fee-for-service plan. CHF, diabetes, & CKD determined from claims.

Early: > 12 months Intermediate: 4-12 months Late: <4 months
Kinchen KS….Ann Intern Med 2002 Sep 17;137(6):479-86


Effectiveness of a chronic kidney disease clinic in achieving K/DOQI guideline targets at initiation of dialysis--a single-
centre experience
Lee, W. et al. Nephrol. Dial. Transplant. 2006 0:gfl701v1-6; doi:10.1093/ndt/gfl701
Copyright restrictions may apply.
Lee, W. et al. Nephrol. Dial. Transplant. 2006 0:gfl701v1 6; doi:10.1093/ndt/gfl701

Effectiveness of a chronic kidney disease clinic in achieving K/DOQI guideline targets at initiation of dialysis--a single-
centre experience

PHYSICIANN C lt•New Consults
•Follow up consults with active issues•Return from NP if active
NURSE PRACTITIONERS
FELLOWS3 SECRETARIES1 BILLER
PRACTITIONERS•Straight CKD•Chronic Stable GN•Chronic Stable
Patient Volunteer
Dedicated Vascular Surgeon•Transplant
•Hypertension
Surgeon
Dedicated Interventional Nephrologist

Extensive use of online and paper diet sheets Extensive use of online and paper diet sheets Patient helpline for drug assistance programs Patient volunteer and front desk staff are very Patient volunteer and front desk staff are very
efficient.

43%50%
Column1
23%20%30%40%
7%2%
0%10%20%
AVF PLACED AVF REFERRED PD FAILED ACCESS

Health Care O i ti Community
ResourcesOrganization
Self-management S pport
Delivery System Design SupportSystem Design
D i i S tDecision SupportClinical Information
S tSystemsBodenheimer..JAMA. 2002;288:1775-1779.

Patient with CKD
Identify patients with CKD
CKD-CDSS
Provider
Note in EHR
CDSSMonitors notes for
CKD documentation
Informs provider of CKD ifInforms provider of CKD if documentation is lacking

JAMIA 2010 17: 588-594

EHREHR
This is the first admission for a 74 year
Date Test Value
“Structured” data “Unstructured” dataCDS
admission for a 74 year old man admitted with chronic renal insufficiency and shortness of breath…
1/23/09 Creatinine 1.6
12/2/09 Creatinine 1.7 CKD
29

CDSS Promoting Early Recognition and Optimal Management of CKD
Patient CKD Report
Provider CKD Report
Feedback [2]
CKD Diagnosis
pRenal Function
Anemia
Mineral Metabolism...A
Provider
CDSS
Patient CKD ReportRenal Function
Anemia
Mi l M t b li
Note in EHR [1]
Patient CKD ReportRenal Function
Anemia
CDSS
Notification [1]
Mineral Metabolism...
E
Anemia
Mineral Metabolism...
Guideline-based reportsRecommendations [2]
R
Guidelines
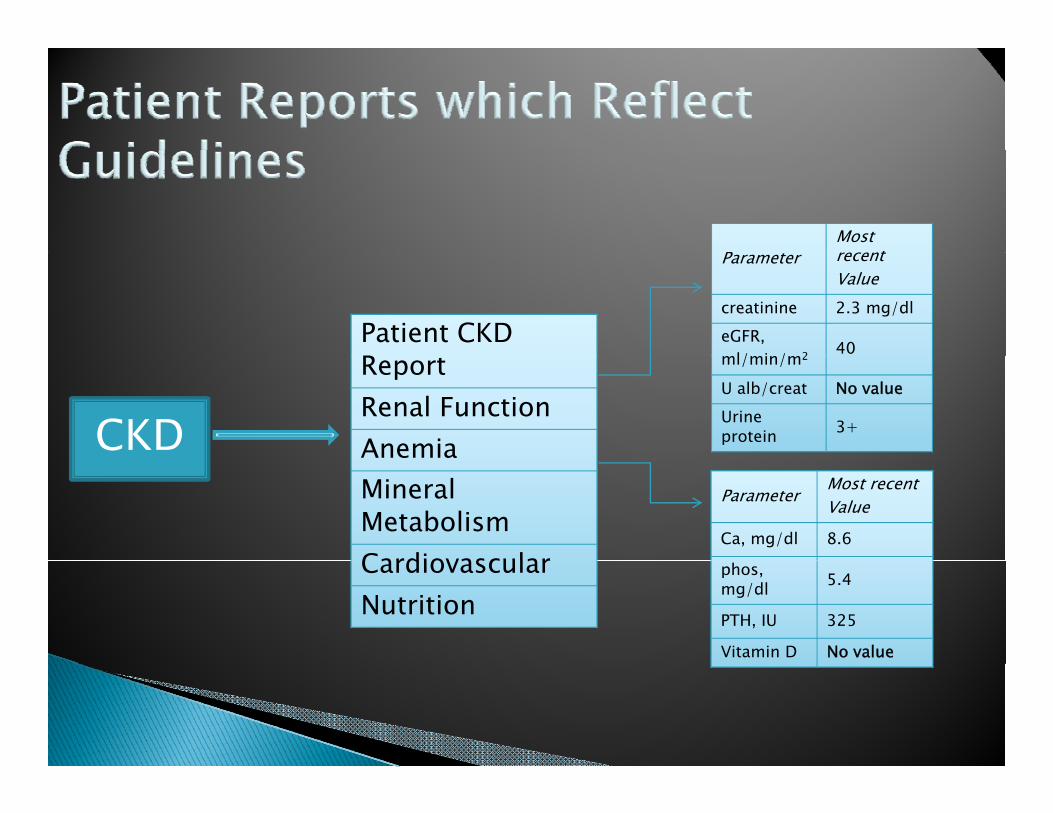
PMost recent
Patient CKD
Parameter recentValue
creatinine 2.3 mg/dleGFR,
l/ i / 2 40ReportRenal FunctionAnemia
ml/min/m2
U alb/creat No valueUrine protein 3+CKD e a
Mineral MetabolismCardiovascular
Parameter Most recentValue
Ca, mg/dl 8.6
CardiovascularNutrition
phos, mg/dl 5.4
PTH, IU 325
Vitamin D No value


ICD 9 Office Visit Billing Codes
CKD Stage 1 (GFR > 90) – 585.1 CKD Stage 2 (GFR 60 89) 585 2 CKD Stage 2 (GFR 60-89) – 585.2 CKD Stage 3 (GFR 30-59) – 585.3 CKD Stage 4 (GFR 15-29) – 585.4g ( ) CKD Stage 5 (GFR<15) – 585.5

Office Visit Reimbursement
Commercial Insurances reimburse NPs at f100% of MD charges
Medicare only reimburses NPs at 80% of MD hcharges
Medicare and a secondary insurance reimburses NPs at 100% of MD chargesreimburses NPs at 100% of MD charges

Office Visit Reimbursement
Commercial Insurances reimburse NPs at f100% of MD charges
Medicare only reimburses NPs at 80% of MD h if t i d d tlcharges if pt independently seen
Medicare and a secondary insurance reimburses NPs at 100% of MD chargesreimburses NPs at 100% of MD charges


CPT ESA Billing Codes
Epoetin alfa – J0885 (Standard unit 1,000 units)
Darbepoetin alfa - J0881 (Standard unit 1 )mcg)
Injection – 96372HemoCue Lab 85018QW HemoCue Lab – 85018QW

Multilingual communications Comprehensive electronic data systems Detailed case management Coordination of care Performance and satisfaction reporting
C t l i Cost analysis Proactive patient care self-initiatives Preventive care measures Preventive care measures Ongoing continuous quality improvement

Nephrologists would usually not wish to be designated as the medical homedesignated as the medical home.
Exceptions: dialysis or transplant recipients Exceptions: dialysis or transplant recipients.

The financial and logistic burden of CKD/ESRD patients continue to increase
CKD clinics with physician extenders are a logical next step.
The PCMH model is probably an optimal one but needs to be “customized”one, but needs to be customized .

Top Related