





Languages
Pages
Legal


Dr Isabel Skypala
Consultant Allergy Dietitian
Royal Brompton & Harefield NHS Foundation Trust
Honorary Senior Clinical Lecturer
Imperial College
Food allergy versus intolerance –
understanding free-from dietary needs

Adverse Food Reactions
Immune-mediated
(Food Allergy and Coeliac
Disease)
Non Immune-mediated
(primarily food Intolerance)
IgE-mediated
Metabolic
Pharmacological Non IgE-
mediated
Toxic
Other
Idiopathic
Mixed
IgE and
Non IgE-
mediated
Cell-mediated
Adapted from:
Guidelines for the Diagnosis and Management of Food
Allergy in the United States (Boyce et al 2010)

Food-induced Allergic Disorders
IgE-mediated
Pollen
Food
Allergy
Syndrome
Urticaria
Angioedema
Mixed IgE and Non
IgE-mediated
Cell-mediated
Adapted from:
EAACI Food Allergy and Anaphylaxis
Guidelines: diagnosis and
management of food allergy (Muraro et
al 2014)
Rhinoconjunctivitis
Asthma
Gastrointestinal
Anaphylaxis
Food-dependent
Anaphylaxis
Atopic eczema
Dermatitis
Eosinophilic
Gastrointestinal
Disorders
Dietary protein
-induced
Proctitis &
Proctocolitis
Food
Protein-
Induced
Enterocolitis
Syndrome
(FPIES)

Perception of Food Allergy 20% of the population alters their diet because they
believe they have an adverse reaction to a food or food
component (Sicherer and Sampson 2006)
Children 12 months – reported rate 7.2%, actual rate 4%
3 years – reported rate 37%, actual rate 6%
Teenage – reported rate 18.7%, actual rate 1%
(Venter, Pierera and colleagues)

Adults Study authors Date Country Reported
rate
Actual or
estimated rate
Young et al 1994 UK 19.9% 1.4%
Jansen et al 1994 Netherlands 12.4% 2.4%
Zuberbier et al 2004 Germany 34% 3.6%
Vierk et al 2007 USA 9.1% 5.3%
Osterballe et al 2009 Denmark 19.6% 1.7%
Skypala et al 2013 UK 15.5% 5.3%
Burney et al 2014 Europe 21% 4.4%
Lifetime prevalence of self-reported food
allergy was 17.3% (95%CI: 17.0-17.6)
Point prevalence for challenged verified FA
was 0.9%
Incidence stable but prevalence increasing
Who is at risk? Children
• Parental atopy
• Eczema -33% of children with moderate/severe eczema may present
with a food allergy (NICE 2007)
• Relationship between asthma, allergic rhinitis and food allergy in
school age children (Penard-Morand et al 2005)
• Food allergy associated with severe asthma in children (Roberts et al
2003)
Adults
• Associated with urticaria, eczema, asthma and hayfever (Schafer
2001, Skypala 2013)
• Asthma - 90% of people who suffered fatal food anaphylaxis had
daily asthma treatment (Pumphrey and Gowland 2007)
• Female sex, rhinitis, eczema and sensitisation to aeroallergens
independently associated with new-onset food allergy (Patelis 2014)

IgE v Non IgE FA v Food Intolerance IgE Non-IgE Intolerance
Onset Rapid Delayed Rapid/delayed
Symptoms Itch, rash, flushing,
swelling, hives,
angiooedema, wheeze,
sneeze, anaphylaxis
Eczema, vomiting,
diarrhoea,
constipation, food
impaction
Rash, flushing,
nausea and
vomiting, rapid
heart beat,
diarrhoea,
constipation,
wheeze, sneeze
Typical
Foods
Milk, egg, wheat,
seafood, nuts, seeds,
legumes, fruits
Not clear but often
wheat, milk, soy
?? seafood
Composite foods,
unrelated foods
Diagnosis History, validated tests,
oral food challenge
History, exclusion
diet, oral food
challenge
History, few
validated tests,
exclusion diet, oral
food challenge

• Bioresonance, kinesiology, irridology, hair analysis,
cytotoxic test, IgG and IgG4, are not currently validated
and cannot be recommended for the diagnosis of food
allergy
• Food-specific IgG4 levels indicate repeated exposure to
high doses of a particular food

Which foods in kids? • Milk, egg, wheat and soy
• IgE and non IgE-mediated
• Usually resolve by teenage years
• Peanut and tree nuts
• Usually start in childhood
• 80% continue into adulthood
• Fish – usually lifelong
IgE-mediated food allergy in adults
• Seafood – especially shellfish (Kamdar et al 2014)
• Tree nuts and peanuts – mainly as cross-reactive
allergies
• Seeds and legumes - sesame, mustard, sunflower
seed, soy, lupin, chick pea
• Fruit and vegetables – usually cause problems due to
cross-reactions between plant foods and pollen (Patelis
2014)
• Cross-reactive food allergy due to pollen common
• Cross-reactions between house dust mite/shellfish,
latex/fruit, cat/pork/beef, meat/tick bites can also occur
Wheat, rye, barley - Coeliac disease
Milk and milk products - Lactose intolerance
Milk, wheat, fruits and vegetables - Fermentable carbohydrates
Additives – preservatives and flavour enhancers
Sulphites - May affect up to 5% of asthmatics
Benzoates – may affect up to 2% of people with urticaria
Naturally occurring ‘food chemicals’
Biogenic Amines
- Headache, hay fever symptoms, flushing, itching, rashes, asthma,
arrhythmia, low blood pressure, abdominal cramping, brochospasm
- Scombroid poisoning
Non-IgE or non-immune mediated food allergy

Co-factors • Cause food allergy only when the food and the co-
factor are co-located
• Exercise most common co-factor –FDEIA – usually
involving wheat but also seafood and tomatoes
- Blood flow redistribution (Morita et al. 2007)
- Uptake of incompletely digested food proteins (Cheng
et al 2007)
- Suppression of gastric acid (Chen et al 2013 )
• Aspirin, NSAID, alcohol and food additives can
also act as co-factors (Cardona et al 2012)

Dietary Management Current Diet
• Food preferences
• Other dietary restrictions
(e.g. for cultural or ethical
reasons)
• Social factors (e.g.
cooking facilities, time)
• Changing nutritional
requirements e.g. growth
in children/pregnancy in
adults
• Nutritional adequacy
Proposed Diet
• What foods/nutrients are
being removed from the
diet?
• Will food substitutes be
required?
• How many foods are being
removed?
• How long will foods be
eliminated – weeks/months?
• Level of avoidance and
other routes of exposure

Other routes of exposure
• Inhalation of aerosolized allergens
• Transfer of allergens during cooking
• Touch and absorption through the skin
• 5-12% of accidental exposures causing
reaction are due to kissing

Level of avoidance IgE mediated food allergy
• Most often need to completely avoid the food and even trace amounts of the food
• Some people can tolerate baked milk or egg
Non-IgE mediated food allergy
• May tolerate small amounts of the trigger food
• Severe cases of non-IgE mediated allergy requires complete avoidance
Food Intolerance
• Reactions are often dose dependent

Nutritional Deficiency in Children • Infants presenting with food allergy have low weight for age
and low height for age Z scores (Viera et al 2010, Flammarion et al 2012)
• The avoidance of 3 or more food groups significantly impacts on weight for age scores (Flammarion et al 2012, Meyer R et al. 2014)
• Red flags are:
Growth faltering or static weight
Poor motor skills and other developmental milestones
Choice and tolerance of formula
Feed volume
Avoidance of multiple foods
Dietary restrictions not associated with food allergy
Presence of another chronic condition

Nutritional deficiency- adults • Diets of adults on milk and wheat free diets low in iron, B
vitamins, Vitamin D, calcium and energy
• Deficiencies in zinc, iron and vitamin D may contribute to
the development of allergies in the elderly (Diesner et al.
2011)
• Vitamin C - could be sub optimal if multiple fruits and
vegetables being avoided (des Roches et al 2006)
• A greater number of food allergies linked to increasing
number of nutritional deficiencies (Kim et al 2013)
• Full nutritional dietary and serum screen essential where
multiple foods have been avoided for some time
• Bone densitometry in those with asthma avoiding milk

Milk
Milk - Heat treatment
reduces allergenicity of β-
lactoglobulin but not α-
casein
Milk –90% cross-reactivity
to goat’s milk
mare and camel milk 4%
cross-reactivity
75% of milk allergic children tolerated baked milk – (Nowak et al JACI 2008)
Fraction Protein Allergen
Casein
80%
αs1-casein
Bos d 8
αs2-casein
ϐ-casein
ϒ1-casein
ϒ2-casein
ϒ3-casein
κ-casein
Whey or
serum
proteins
20%
α-lactalbumin Bos d 4
ϐ-lactoglobulin Bos d 5
Immunoglobulin Bos d 7
BSA Bos d 6
Lactoferrin

Cow’s milk substitutes
• Hydrolysed and elemental formula milks for infants
Partially hydrolysed formula
Extensively hydrolysed
Amino acid
• Soya milk – affects 7-14% of infants with IgE –mediated milk allergy
but up to 50% of non-IgE-mediated milk allergy
• Rice milk – not for children aged between 1 and 4.5 years
• Adults and older children
• Pea milk, almond milk, Oat milk, Coconut milk, Hemp milk
• Other milk substitutes – lacto-free milk

Eggs Allergen Common
name
Heat -
treated
Digestive
enzyme-
treated
Allergenic
activity
Gal d 1 Ovomucoid Stable Stable +++
Gal d 2 Ovalbumin Unstable Unstable ++
Gal d 3 Ovotransferrin
Conalbumin
Unstable
Unstable
+
Gal d 4 Lysozyme Unstable Unstable ++
Cross-reactivity with other birds eggs, birds
feathers and chicken

Egg Ladder
Well cooked egg Lightly cooked egg Raw egg
Cakes and biscuits
Egg pasta
Pancakes
Well-done Yorkshire
pudding
Sausages
Burgers
Quorn
Sponge cake
Milky Way or Mars bar
or Crème egg
Some soft-centred
chocolates
Waffles
Commercial marzipan
Scrambled, boiled, fried,
poached egg
Omelette
Egg fried rice
Meringues
Some marshmallows
Lemon curd
Quiche
Egg in batter or breadcrumbs
Hollandaise sauce
Quiche and flans (fruity and
savoury)
Egg custard, Crème caramel
Crème Brulée and ‘real’ custard
Runny Yorkshire pudding
Tempura batter
Mayonnaise or salad
cream
Mousse
Ice cream
Sorbet
Royal icing
Home-made marzipan
Cake mix
Egg glaze on pastry
Horseradish sauce
Tartar sauce
Cheese containing egg
white in the form of
lysozyme

Seafood Pan allergens –βParvalbumin in vertebrate fish and
invertebrate tropomyosin in crustaceans and molluscs
Allergens are heat-stable, water-soluble
Shrimp allergens detected in oil used to cook shrimp
and reported to cause problems in cooking vapours (Lehrer et al 2007, Carrillo et al 1992)
Species-specific reactions
Contamination
Differential diagnosis

Peanuts and Tree nuts
• Peanut
• Ground nuts
• Monkey nuts
• Earth nuts
• Goober peas
• Brazil
• Walnut
• Hazelnut
• Almond
• Cashew
• Pistachio
• Pecans
• Macadamia
Nutmeg, Coconut, pine nut
and palm nut are not
classified as nuts
• Cold-pressed ‘gourmet’
oils
• Marzipan
• Frangipan
• Amaretto products
• Macaroons
• Bakewell tarts
• Praline
• Noisette
• Marron e.g. marron glace
• Satay sauce
• Korma sauce
• Pesto sauce
• Cakes, biscuits and
pastries
• Ice cream, desserts
and dessert toppings
• Chocolate bars
• Cereal bars and
confectionery
• Savoury snack foods
• Breakfast cereals,
especially muesli or
nut mixtures

Peanuts and Tree nuts
• Cross-reactivity and cross-contamination
• Avoidance of all nuts or just specific nuts?
• May contain traces nut warnings
• Lifelong abstinence – is resolution
important to challenge for?
• Non-food sources of nuts and seeds

Soy Whole bean
products
Soy sprouts, Edamame, soy milk, tofu, Miso, Natto, Yuba, Tempeh,
Soy sauce, soy nuts, soynut butter, soy cereals, soy cheese, soy milk,
soy ice cream/yoghurt/desserts
Hull Products Bread, bakery products , snack bars
Protein
products
Soy flour, protein concentrate, protein isolate, textured soy
Baby foods, infant formulae, bread, biscuits, pancakes, pastry,
crackers, snack foods, noodles, pizza, breakfast cereals, soy milk, ice
cream, soy yoghurt and cheese, sausages, tinned meat and fish, soups
and gravy, beef burgers, salad dressing, stock cubes, sauces
Oil Products Refined oil, lecith in
Cooking oil, salad oil, margarine, salad dressing, mayonnaise, coffee
whiteners, chocolate, sweets, pastry filling, cheese dips, emulsifying
agents, dietary supplements and body building agents

Fruits & Vegetables • Pollen-food syndrome (PFS) or Oral Allergy Syndrome occurs in
people whose pollen antibodies recognise and cross-link with
homologous plant food proteins
• Main Birch pollen allergen Bet v 1 has 35-60% sequence identity
with many PR10 proteins in plant foods
• Immediate oral symptoms on contact with plant food
• 66% (50 to 93%) birch pollen allergic patients may have PFS
• Other pollens which can cross-react include grass, ragweed and
mugwort
• Only raw foods cause symptoms
• Typical foods include apples, peaches, cherries, kiwi fruit, tree nuts,
but can also involve tomatoes, carrots, celery, peeling potatoes,
melon, oranges and peanuts
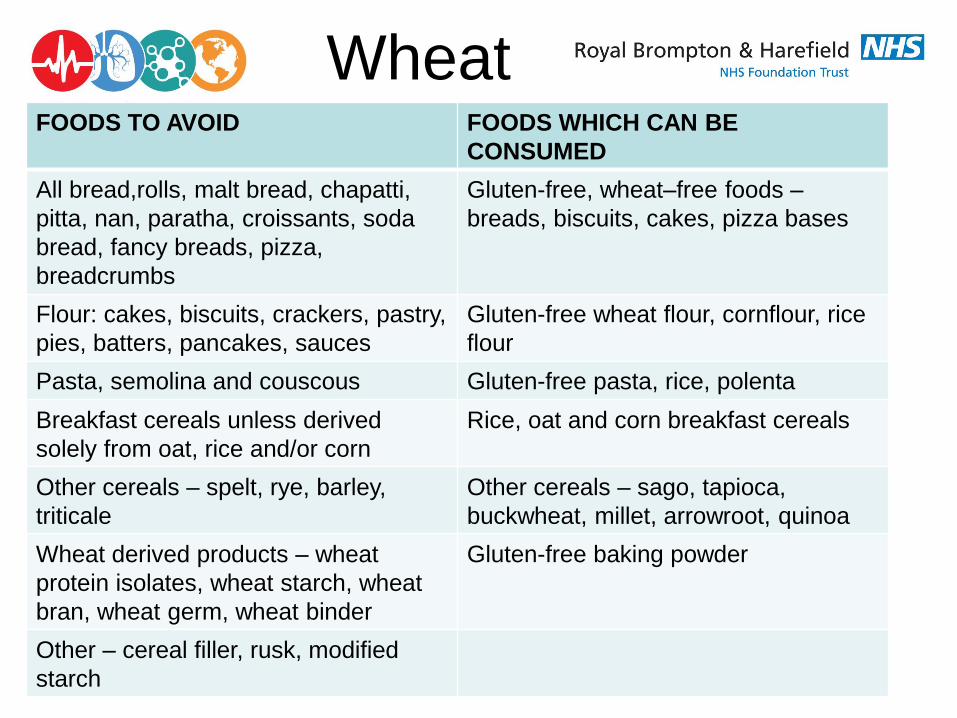
FOODS TO AVOID FOODS WHICH CAN BE
CONSUMED
All bread,rolls, malt bread, chapatti,
pitta, nan, paratha, croissants, soda
bread, fancy breads, pizza,
breadcrumbs
Gluten-free, wheat–free foods –
breads, biscuits, cakes, pizza bases
Flour: cakes, biscuits, crackers, pastry,
pies, batters, pancakes, sauces
Gluten-free wheat flour, cornflour, rice
flour
Pasta, semolina and couscous Gluten-free pasta, rice, polenta
Breakfast cereals unless derived
solely from oat, rice and/or corn
Rice, oat and corn breakfast cereals
Other cereals – spelt, rye, barley,
triticale
Other cereals – sago, tapioca,
buckwheat, millet, arrowroot, quinoa
Wheat derived products – wheat
protein isolates, wheat starch, wheat
bran, wheat germ, wheat binder
Gluten-free baking powder
Other – cereal filler, rusk, modified
starch
Wheat

Semolina
Couscous Pearl barley
Spelt
Quinoa Potato flour Buckwheat
Tapioca Cornflour Polenta

Pizza – soy, celery,
mustard, wheat
protein isolate
Asian food – prawns,
sesame, peanuts,
buckwheat noodles,
Indian food – almonds,
pistachio, cashew,
peanuts, celery, mustard,
seafood
Bakery products – lupin, soy, other legumes,
buckwheat, barley, cochineal
Hidden allergens

Lactose Intolerance • Congenital -rare -poor growth + diarrhoea from first
exposure to breast milk
• Primary - 70% of humans from early childhood onwards
– can often tolerate foods that have lower lactose
content
• Secondary/transient - reversible loss of lactase activity
due to damage to brush border of small intestine e.g.
due to gastroenteritis or giardia
• Main foods - milk, soft cheese, ice cream, butter
30

Wheat, milk and IBS
Fermentable Oligo-Di-Monosaccharides and Polyols (FODMAP™)
• Fructo-oligosaccharides - wheat, rye, onions, garlic and artichokes
• Galacto-oligosaccharides – legumes
• Fructose - honey, apples, pears, watermelon and mango - affects
45%
• Lactose - affects 25%
• Sorbitol - peaches, plums, cherries, nectarines, sugar free mints and
gum
• Mannitol - mushrooms, cauliflower
Barrett et al. Aliment Pharmacol Ther. 2009;30:165-74
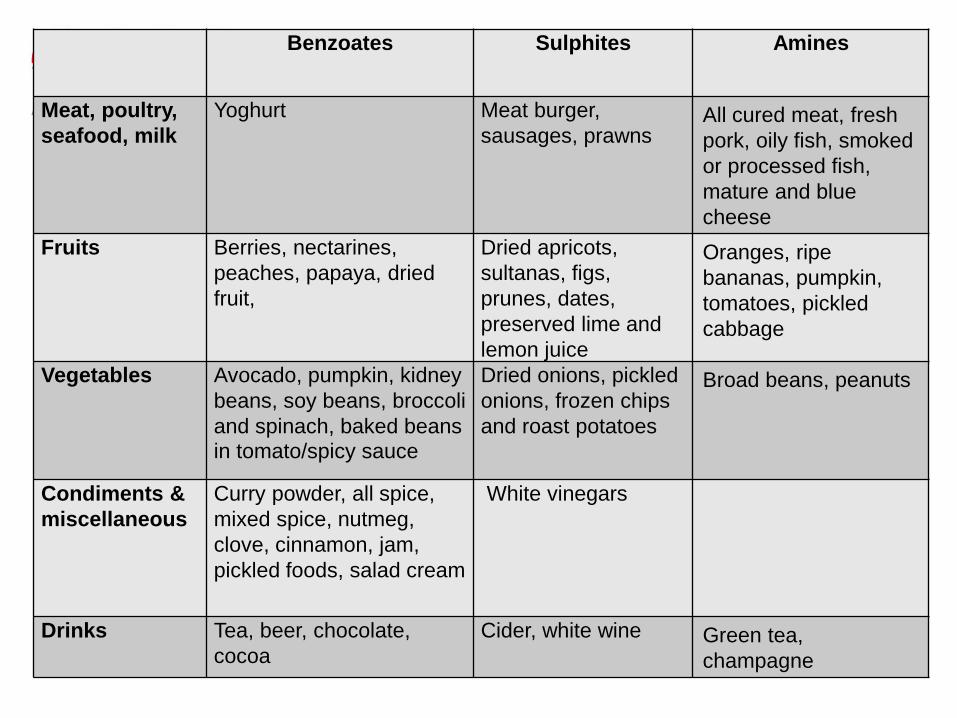
Benzoates Sulphites Amines
Meat, poultry,
seafood, milk
Yoghurt Meat burger,
sausages, prawns All cured meat, fresh
pork, oily fish, smoked
or processed fish,
mature and blue
cheese
Fruits Berries, nectarines,
peaches, papaya, dried
fruit,
Dried apricots,
sultanas, figs,
prunes, dates,
preserved lime and
lemon juice
Oranges, ripe
bananas, pumpkin,
tomatoes, pickled
cabbage
Vegetables Avocado, pumpkin, kidney
beans, soy beans, broccoli
and spinach, baked beans
in tomato/spicy sauce
Dried onions, pickled
onions, frozen chips
and roast potatoes
Broad beans, peanuts
Condiments &
miscellaneous
Curry powder, all spice,
mixed spice, nutmeg,
clove, cinnamon, jam,
pickled foods, salad cream
White vinegars
Drinks Tea, beer, chocolate,
cocoa
Cider, white wine Green tea,
champagne

Summary
• Many different presentations of food allergy and
intolerance
• Diagnosis not straightforward
• Food avoidance can depend on the type of food
allergy or intolerance experienced
• Dietary exclusion can be difficult and nutritional
problems are common, especially in children

THANK YOU FOR LISTENING
Top Related