


Languages
Pages
Legal


Biloma formation without prior surgery or trauma is infrequent. Acute free GBP (Niemeier type I) typically presents with generalized chemical peritonitis. In our case, consistent with histological analysis an oligosymptomatic cholecystitis has to be assumed, succeeded by an unrecognized GBP with low-grade leakage and encapsulation of bile fluid thus preventing chemical peritonitis and leading to an unspecific clinical picture predominantly caused by mass effect of the biloma.
GBP in patients with cholecystitis has been reported in literature with a low incidence varying from 2% to 11% and has traditionally been classified in three types by Niemeier. The constellation of GBP with encapsulated biloma formation is an exceptional clinical entity classified as type IV in recent literature. This case highlights the diversity of GBP presentation and stresses the physician’s awareness of an uncommon pathogenesis and unspecific findings to successfully manage this rare entity.
b b
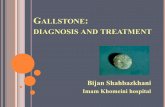
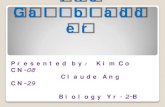
Fig. 1 a/b: Abdominal CT scan
CT examination revealed a fluid collection (11.3x5.8x5.3cm) between the left hepatic lobe and lesser curvature of the stomach – antibiotic treatment was initiated. In a second step diagnosis of a biloma was made by puncture material analysis. On endosonography and MRCP neither obvious signs of bile source nor communication with bile ducts could be demonstrated.
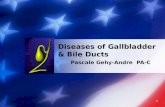
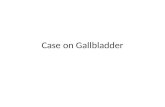
Fig. 2: CT-guided drainage
II. Our Patient
III. Intervention CT-guided drainage was followed by surgical revision through an upper midline laparotomy which evacuated two litres of bile fluid surrounded by a pseudocystic capsule. A 5mm leaking hole in the gallbladder was identified as bile source. Open retrograde cholecystectomy, abdominal lavage and drainage were performed followed by an uneventful postoperative course.
IV. Results
V. Conclusion
Niemeier classification Type 1 (acute): Associated with free perforation into the peritoneal cavity. Type 2 (subacute): Persisting perforation at the perforation site, pericholecystic abscess and localized peritonitis. Type 3 (chronic): Perforation consists of internal or external fistula formation Type 4 (chronic): Low-grade leakage from the bile resulting in a biloma without severe symptoms
A 76-year old man presented with a one week medical history of intermittent colicky right upper quadrant abdominal pain and fever. He reported abdominal distension, anorexia, weightloss and postprandial nausea and vomitus. Clinical and laboratory findings showed a severe systemic inflammation but normal serum bilirubin and liver transaminase levels.
a
b
References: 1 O. W. Niemeier, “Acute free perforation of the gall-bladder,” Ann. Surg., vol. 99, no. 6, pp. 922–924, 1934. 2 F. Ausania, S. Guzman Suarez, H. Alvarez Garcia, P. Senra Del Rio, and E. Casal Nuñez, “Gallbladder perforation: morbidity, mortality and preoperative risk prediction.,” Surg Endosc, Aug. 2014. 3 I. Başara and M. Seçil, “Spontaneous asymptomatic gallbladder perforation.,” Quant Imaging Med Surg, vol. 4, no. 3, pp. 212–213, Jun. 2014.
Encapsulated subhepatic biloma after gallbladder perforation Kreienbuehl A. , Frischknecht A., Melcher G. A. Department of Surgery, Hospital of Uster
We report a rare case of gallbladder perforation (GBP) with consecutive biloma formation presenting with an unspecific symptomatic.
I. Introduction
Biloma formation without prior surgery or trauma is infrequent. Acute free GBP (Niemeier type I) typically presents with generalized chemical peritonitis. In our case, consistent with histological analysis an oligosymptomatic cholecystitis has to be assumed, succeeded by an unrecognized GBP with low-grade leakage and encapsulation of bile fluid thus preventing chemical peritonitis and leading to an unspecific clinical picture predominantly caused by mass effect of the biloma.
GBP in patients with cholecystitis has been reported in literature with a low incidence varying from 2% to 11% and has traditionally been classified in three types by Niemeier. The constellation of GBP with encapsulated biloma formation is an exceptional clinical entity classified as type IV in recent literature. This case highlights the diversity of GBP presentation and stresses the physician’s awareness of an uncommon pathogenesis and unspecific findings to successfully manage this rare entity.
b
Fig. 1 a/b: Abdominal CT scan
CT examination revealed a fluid collection (11.3x5.8x5.3cm) between the left hepatic lobe and lesser curvature of the stomach – antibiotic treatment was initiated. In a second step diagnosis of a biloma was made by puncture material analysis. On endosonography and MRCP neither obvious signs of bile source nor communication with bile ducts could be demonstrated.
Fig. 2: CT-guided drainage
II. Our Patient
III. Intervention CT-guided drainage was followed by surgical revision through an upper midline laparotomy which evacuated two litres of bile fluid surrounded by a pseudocystic capsule. A 5mm leaking hole in the gallbladder was identified as bile source. Open retrograde cholecystectomy, abdominal lavage and drainage were performed followed by an uneventful postoperative course.
IV. Results
V. Conclusion
Niemeier classification Type 1 (acute): Associated with free perforation into the peritoneal cavity. Type 2 (subacute): Persisting perforation at the perforation site, pericholecystic abscess and localized peritonitis. Type 3 (chronic): Perforation consists of internal or external fistula formation Type 4 (chronic): Low-grade leakage from the bile resulting in a biloma without severe symptoms
A 76-year old man presented with a one week medical history of intermittent colicky right upper quadrant abdominal pain and fever. He reported abdominal distension, anorexia, weightloss and postprandial nausea and vomitus. Clinical and laboratory findings showed a severe systemic inflammation but normal serum bilirubin and liver transaminase levels.
a
b
References: 1 O. W. Niemeier, “Acute free perforation of the gall-bladder,” Ann. Surg., vol. 99, no. 6, pp. 922–924, 1934. 2 F. Ausania, S. Guzman Suarez, H. Alvarez Garcia, P. Senra Del Rio, and E. Casal Nuñez, “Gallbladder perforation: morbidity, mortality and preoperative risk prediction.,” Surg Endosc, Aug. 2014. 3 I. Başara and M. Seçil, “Spontaneous asymptomatic gallbladder perforation.,” Quant Imaging Med Surg, vol. 4, no. 3, pp. 212–213, Jun. 2014.
Encapsulated subhepatic biloma after gallbladder perforation Kreienbuehl A. , Frischknecht A., Melcher G. A. Department of Surgery, Hospital of Uster
We report a rare case of gallbladder perforation (GBP) with consecutive biloma formation presenting with an unspecific symptomatic.
I. Introduction
Top Related