




Languages
Pages
Legal


Improved outcomes of combined modality management of unruptured intracranial aneurysms: Lower
morbidity alters treatment recommendationsChristopher S. Ogilvy MD; Noah J Jordan BS; Alejandro Enriquez-Marulanda; Luis C Ascanio MD; Ajith J. Thomas MD
Neurosurgical Service, Beth Israel Deaconness Medical Center, Harvard Medical School. Boston, Massachusetts, UnitedStates
IntroductionDecision-making in thetreatment of unrupturedintracranial aneurysms isbased on the evaluation of thepatient and lesion-specificrisks balanced against thenatural history risk of rupture.The purpose of this study wasto evaluate combinedmodality treatment risks ofunruptured aneurysms.
MethodsData was collectedprospectively and analyzedretrospectively in 658unruptured aneurysms in 553patients over four years fromJanuary 2014 through 2017.The recommendation for thelowest risk treatment modalitywas made by a team oftreating physicians whoperform both endovascularand surgical repair ofaneurysms. Functionaloutcomes were assessed withthe mRS scores at the lastclinical visit. Good functionaloutcomes included mRSscores from 0 to 2 and pooroutcomes mRS scores from 3to 6.Logistic regression modelingwas used to generate curvesof probabilities of a goodoutcome for both anterior andposterior circulationaneurysms, stratified bylesion size and patient age.
Results553 patients were identified,harboring 658 aneurysms.Most patients were female(77.6%). The median patientage was 59 years old and themedian aneurysm size atmaximal diameter was 6 mm.Treated aneurysms were morecommon in the anteriorcirculation (n=589, 89.5%),especially at the internalcarotid artery (47.3%). Mostaneurysms were saccular inshape (95.6%). Endovasculartreatment was used in 407(61.8%) aneurysms whilemicrosurgical clipping wasperformed in 251 (38.2%)aneurysms. The median timeof last clinical visit was 5.5months [IQR 1.2 – 12.5months].
Table 1
Table 2
Results (Cont...)Complications occurred in 66procedures (9.9%). Of these,38 (5.7%) were neurologiccomplications (Table 2).There were 20 procedureswith ischemic complicationswhere 6 resulted in pooroutcomes, 5 with hemorrhagiccomplications where oneresulted in a poor outcome.28 (4.2%) non-neurologiccomplications occurred duringor after procedures. None ofthese complications resultedin permanent neurologiceffects.
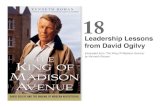
Figure 1 shows theprobabilities of good outcomes(mRS 0-2) and its 95%confidence intervals in the lastclinical visit plotted againstage stratified by aneurysmssizes.
Figure 1
Results (Cont...)Although the probability ofgood outcomes is similaracross ages, as the aneurysmsize gets bigger, endovascularapproaches increases.
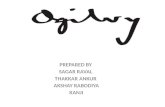
Figure 2 shows theprobabilities of poor outcomes(in Glasgow Coma Scale,GOS) in unrupturedaneurysms surgically treated(left) and probabilities of pooroutcomes (in mRS) with thecombined treatmentmodalities plotted against age(right).We found lower risks oftreatment using combinedmodality therapy for largerlesions in the anteriorcirculation. In the posteriorcirculation, only endovasculartherapy was performed andpoor outcomes were morelikely in aneurysms of 5-9.9mm
Results (Cont...)Our data published in 2003using clipping alone (on theleft side) shows higher risks ofpoor outcomes using surgeryalone. However, directcomparisons cannot be made.
Figure 2
ConclusionsThis data highlights the needfor continued stratification oftreatment-related risk analysisfor patients with unrupturedaneurysms. With lower overallrisks of combined modalitytreatment, justification oftreating smaller lesions andolder patients in both theanterior and posteriorcirculation is possible. Thesereported treatment-relatedrisks must be carefullyweighed against stratifiednatural history risks in theultimate decision to treat anunruptured aneurysm.
References1. Ogilvy CS, Carter BS.Stratification of outcome forsurgically treated unrupturedintracranial aneurysms.Neurosurgery. Jan2003;52(1):82-87; discussion87-88.