




Languages
Pages
Legal

By Jeanie Ward
Iron Deficiency Anemia
What is wrong?
What causes Iron Deficiency Anemia in Children?
Iron Deficiency Anemia
Manifestations: Pallor; Pale mucus membranes Enlarged spleen and heart Poor muscle tone with decreased activity Fatigue
Diagnosis low hemoglobin (<11g/100mL) Low hematocrit (<33%) RBC are small and hypochromic Serum iron levels are low ( 30μg/mL)
Iron Deficiency Anemia Treatment
Oral iron supplements
What additional supplement should be give
What is important to teach regarding diet? What foods high in iron?
Sickle cell Disease
What is wrong?
What causes the cell to sickle?
Low Oxygen tension (less than 60%-70%)
Low blood pH (acidosis)
Increased blood viscosity (dehydration, fever, hypoxia)
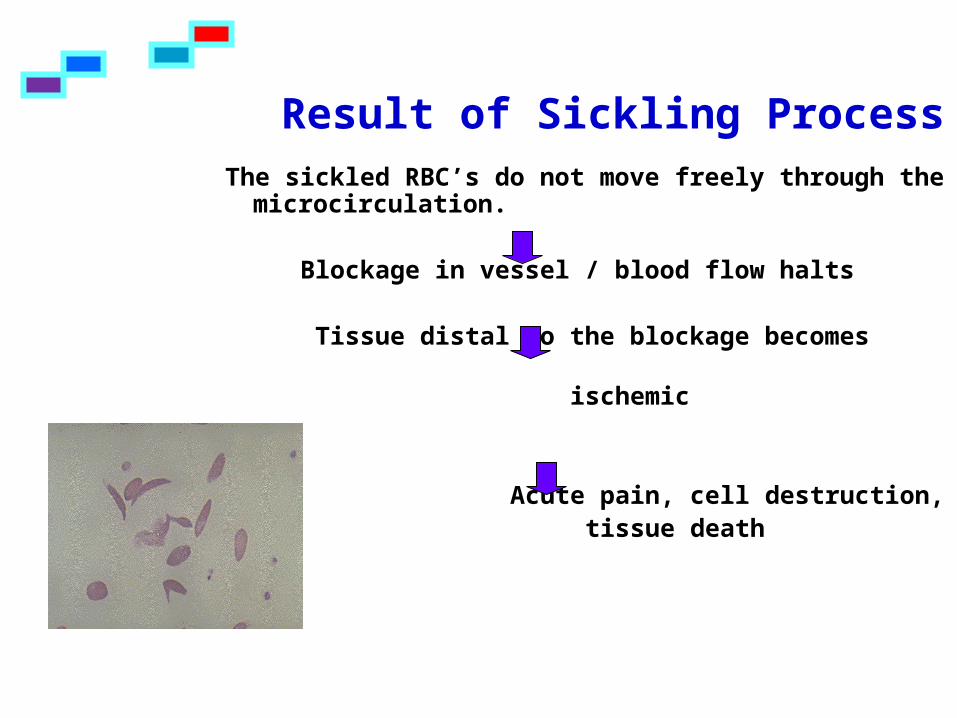
Result of Sickling ProcessThe sickled RBC’s do not move freely through
the microcirculation.
Blockage in vessel / blood flow halts
Tissue distal to the blockage becomes ischemic
Acute pain, cell destruction, tissue death
Assessment
General Manifestations Chronic anemia (Hgb. 6-9 g/dl.), pallor,
weakness. Unable to do physical activities because of lack of stamina
Fatigue, malaise Anorexia Jaundice Possible delayed sexual maturation Marked susceptibility to sepsis Possible growth retardation – with long
bones disproportionately long.
Types of Sickle Cell Crisis
Vaso-Occlusive Crisis
Occurs from the pooling of many of the new sickled cells in vessels with resulting tissue hypoxia
May last from one day to several weeks
Manifestations of Vaso-Occlusive Crisis
Bone Pain Most outstanding symptom Mainly in the bones of the extremities
and joints, but can occur anywhere Abdominal and back pain is common Related to necrosis of bone tissue Parents may notice this with refusal to
move an extremity, crying out with joint movement or joint touched.
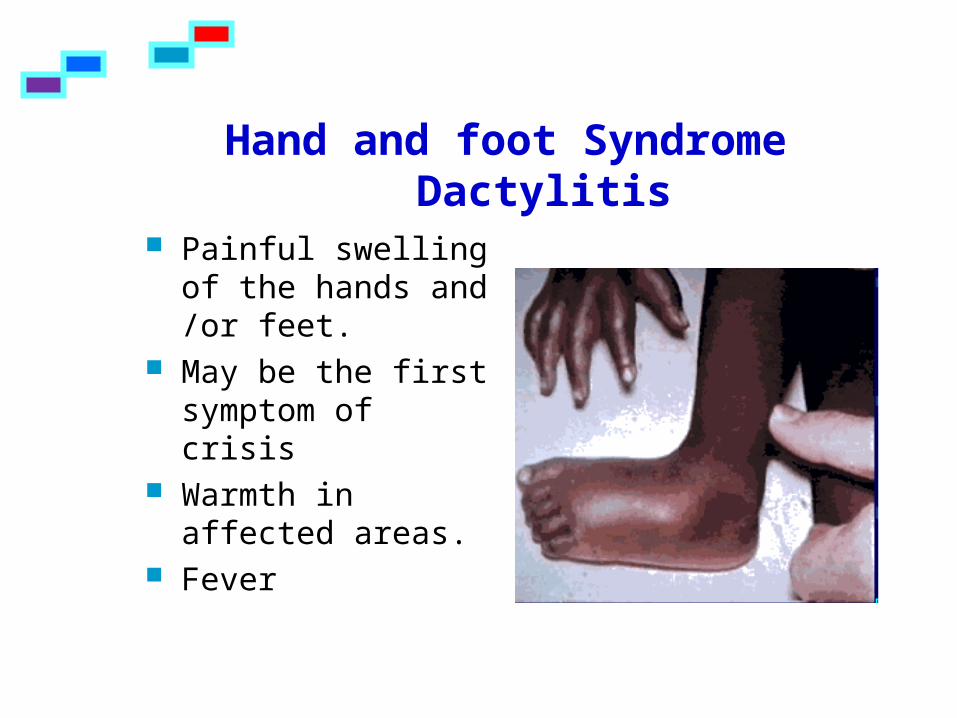
Hand and foot SyndromeDactylitis
Painful swelling of the hands and /or feet.
May be the first symptom of crisis
Warmth in affected areas.
Fever
Cerebrovascular accident
Vaso-occlusion in the brain results in cerebral infarction which causes variable degreesof neurologic damage
Hemiplegia Aphasia Seizures Vision changes Headaches Alterations in level of consciousness
Acute Chest Syndrome Blockage of blood vesselsin the chest leads to Pneumonia and acute chest syndrome
Chest pains Fever, cough Dyspnea, retractions
Leading cause of death in SCD.
Priapism
Persistent painful erection of the penis occurring when penile blood flow is obstructed.
Hepatomegaly
Enlarged liver with jaundice and hepatic coma.
related to damage to the kidneys
Hematuria

Aplastic Crisis
Diminished RBC production resulting in severe anemia
Manifested by: Malaise, lethargy Headache Pallor fainting
Aplastic Crisis Profound anemia- low RBC
count is lifelong. The average RBC life is down to an average of 10-20 days in SCA.
Jaundice, elevated bilirubin Reticulocytosis Bone marrow producing 3-4
times more RBC’s than normal

Acute Sequestration Crisis
Sickled cells become trapped in the spleen obstructing blood flow with pooling and enlargement of the spleen.
Leads to shock and hypovolemia
Circulatory collapse and death can occur in less than 30 minutes
Spleen Function
Acts as a filter against foreign organisms that infect the bloodstream.
Filters out old RBC’s from the bloodstream and recycles them
Minor Role: Manufacturers RBC’s toward end of fetal
life and after birth, taken over by bone marrow.Acts as a blood reservoir.
Spleen in the Infant
Soft, purplish-red organ that lies under the diaphragm on the left side of the abdominal cavity
Filters old blood and clears bacteria
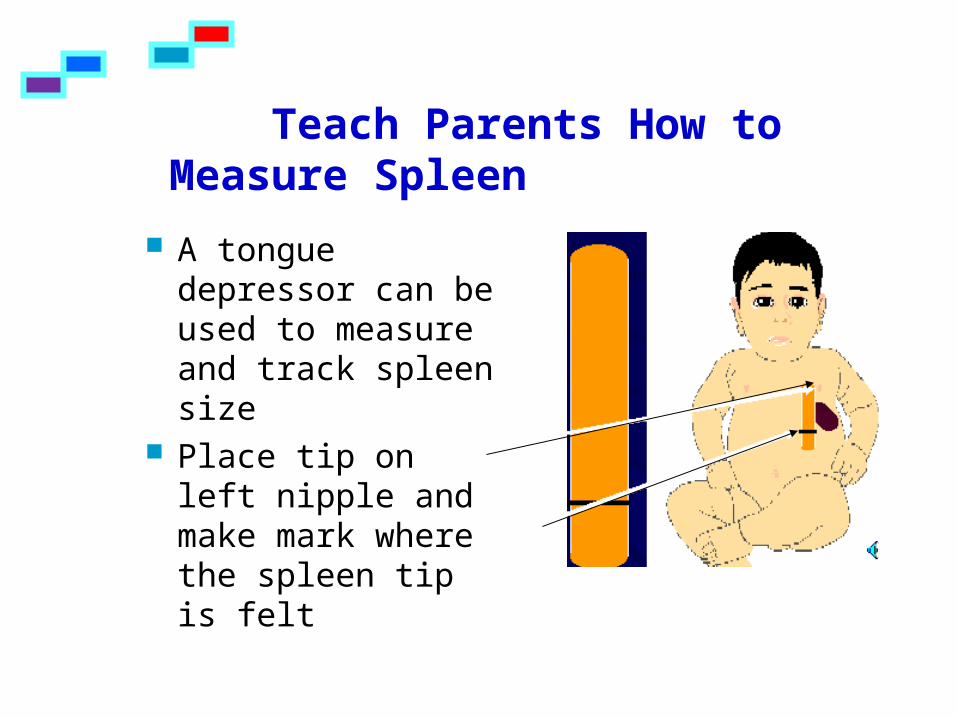
Teach Parents How to Measure Spleen
A tongue depressor can be used to measure and track spleen size
Place tip on left nipple and make mark where the spleen tip is felt
Treatment for Sequestration Crisis
Intravenous fluids
Blood transfusion
Spleen removal
Effects of Chronic Crisis States on the Child’s Body
Spleen – more susceptible to infection. Gradual fibrosis and scarring with reduction in spleen activity. Asplenia.
Liver – enlarged, firm, tender Brain – single episode of sickling CVA,
seizures Heart – enlarges and murmurs develop Lungs – pulmonary edema and stasis Kidneys – hematuria, unable to concentrate
urine Bone Infarcts – hands and feet swell.
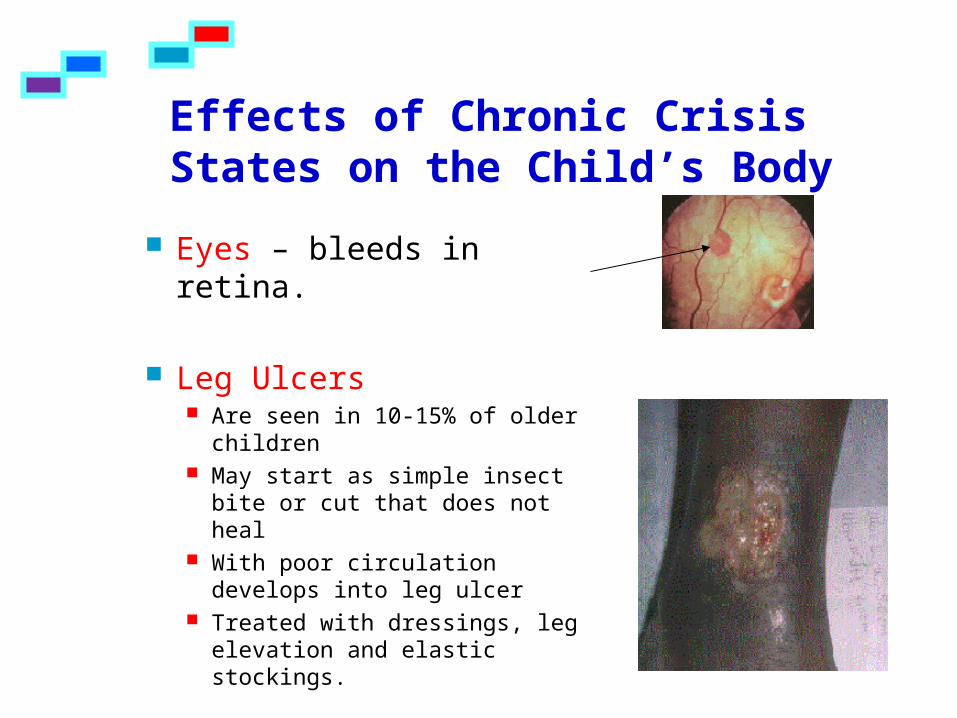
Effects of Chronic Crisis States on the Child’s Body
Eyes – bleeds in retina.
Leg Ulcers Are seen in 10-15% of older
children May start as simple insect bite
or cut that does not heal With poor circulation develops
into leg ulcer Treated with dressings, leg
elevation and elastic stockings.
Diagnostic Tests
CBC – low hgb and hct
Hemoglobin electrophoresis – used to determine type of hemoglobin. When you pass an electric charge through a solution of hemoglobin, distinct hemoglobins move different distances, depending on their composition. This technique differentiates between normal hemoglobin (A), Sickle hemoglobin (S).
Goals in Care
The is NO CURE for the disease
Treat the Symptoms Relieve the pain
Provide oxygenation
Adequate hydration
Pain Management
Give analgesics as ordered Schedule nursing care to allow for
optimal rest Position joints with pillows Application of warmth Promote circulation through passive
ROM
Oxygenation
Assess Oxygen saturation- pulse oximetry. Should be 95% or >.
Administer Oxygen for short period of time to keep saturation levels up.
Bedrest to minimize energy expenditure and oxygen consumption
Administer blood transfusions
What are Complications associated with frequent blood
transfusions?
Allergic reaction
Circulatory overload
Iron Overload Give Desferal, an iron-chelating agent,
to decrease the iron levels
Oxygenation
Prevent infection, dehydration Avoid emotional stress, overfatigue Avoid prolonged exposure to heat
and cold Avoid low oxygen environment
Hydration/ Electrolyte Replacement
Encourage fluid intake, at least the minimum amount of fluid required daily for that child’s weight. (1-2x maintenance)
Record I & O. Monitor electrolyte balance Give parents written instructions on
specific amount of daily intake needed. Assess signs of dehydration (decreased
urination, thirst) Teach parents measures to prevent
dehydration such as avoiding heat / stress.
Prevent Infection
With the spleen damaged, has greater chance of getting sepsis.
Avoid know sources of infection Assess Vital Signs and report elevated
temperatures. Treat with Ibuprofen, NOT ASA.
Place on prophylactic antibiotics such as Penicillin VK 250 mg twice a day, through age 5 yrs
Prevent Infection Immunizations
Hepatitis B series Recipient of blood and blood products.
Pneumococcal Pneumovax for now at age 24 months
and 5 years, with an improved vaccine coming on the market soon for administration to infants.
Meningococcal vaccine H. influenzae vaccine
Child / Parent Teaching Assess baseline knowledge and teach
accordingly: Causes of disease and consequences, genetic
counseling Situations that cause sickling Signs of developing crisis, infection, When to call the doctor
Keep in school, promote normal g&d as much as possible
Allow for decreased endurance - let the child set his or her own pace during strenuous exercise, and to take rest breaks when fatigue
Explain some complications: CVA, anemia, swollen spleen, liver problems
Support child and family
Critical Thinking
Which of the following nursing diagnoses should receive priority during a vaso-occlusive crisis in a 14 year old with sickle cell anemia?A. Alteration in comfortB. Ineffective individual copingC. Decreased cardiac outputD. Ineffective airway clearance
Critical Thinking
Which of these instructions should the parents of a child who has recovered from a sickle cell crisis receive?A Isolate child from known sources of
infectionB Avoid contact with all childrenC Restrict child’s intake during the nightD Reinforce the basics of trait
transmission
Hemophilia
What goes wrong?
Who gets this?
Do Hemophiliacs bleed more Profusely than people without Hemophilia?
Hemophiliacs bleed mainly from minor cuts
True or False
Related to the deficiency of AHF
Interviewing the Child with Hemophilia – Subjective Data
Recent traumas and measures used to stop bleeding
Length of time pressure was applied before bleeding subsided
Was swelling increased after surface bleeding subsided
Did swelling and stiffness occur without apparent trauma
Assessment
Prolonged bleeding anywhere from
or in the body.
When is it most often diagnosed?
Assessment Surface bruising - Bleeding from trauma into
soft tissues and muscles (the ileopsoas muscle around the hip, calf, forearm, upper arm, achilles tendon, buttocks, retroperitoneal.
Hematuria
Hemarthrosis - bleeding into joints (knees, elbows, ankles, shoulders, hips, wrists in descending order of frequency)
Assessment CNS bleeding - Major cause of death Signs and Symptoms of CNS bleeds
Persistent or increasing headache Repeated vomiting Sleepiness or a change in normal behavior Sudden weakness or clumsiness of an arm or leg Stiffness of the neck or complaints of pain with neck
movement Complaints of seeing double The development of crossed eyes Poor balance when walking, a lack of coordination Convulsions or seizures
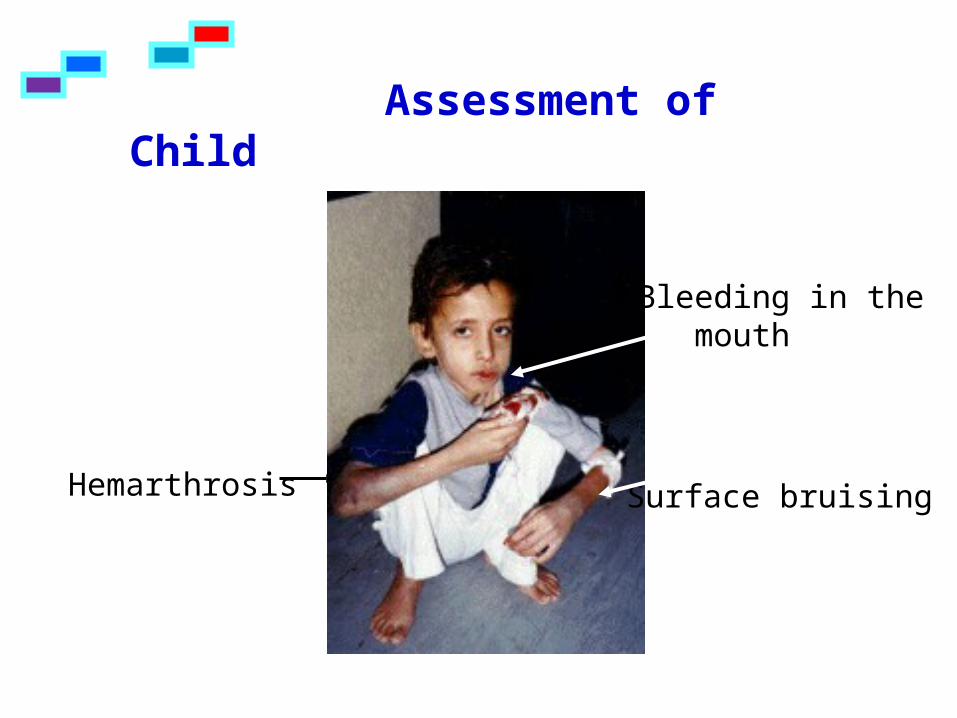
Assessment of Child
Hemarthrosis
Bleeding in the mouth
Surface bruising
Diagnostic Tests
DNA testing for the trait Blood Tests
1. Partial Thromboplastin Time (PTT) – Prolonged
2. Bleeding time – Prolonged > 2 hrs.
3. Platelet count and Prothrombin time – Normal
4. Low levels of Factor VIII
Goals
Prevent and control Bleeding
Prevent crippling effects / Decrease pain
Child/ Parent Teaching
Interventions to Prevent or Control Bleeding
What is the basic priority treatment to stop or prevent bleeding in people with hemophilia A?
Why this is the priority?
Additional Interventions to Prevent and Control Bleeding
Administration of DDAVP (desmopressin acetate) nasal spray used to stimiulate release of factor VIII. Used with mild hemophilia
Apply local pressure for 10-15 minutes
Elevate joint above level of heart
Apply cold compresses to promote vasoconstriction
Prophylactic administration of factor VIII
Interventions to Prevent Crippling effects / Decrease Pain
During bleeding episode—elevate joint and immobilize
ROM after acute episode Exercise unaffected joints and
muscles. Give analgesics before Physical therapy. Do NOT give Aspirin.
Watch diet/ weight – excessive weight stresses the joints
What is the crippling Effect of Repeated bleeds into a Joint?
Bleeding in joints, especially knees, ankles and elbows can lead to: loss of range of motion muscle loss destruction of the joints themselves
Child / Parent Teaching
Measures to prevent injury/ providing a safe environment
Early recognition of bleeding episodes
Keep current on immunizations Hepatitis B – because recipient of blood
and blood products
Child / Parent Teaching
How to administer factor VIII. Children often learn how to infuse
themselves at the age of eight or ten. Then, the hemophiliac is able to treat himself at home, at school, at camp or on vacation.
Critical Thinking
A 12 year old hemophiliac child has been admitted to the hospital for hemarthrosis. Which of these expected outcomes should receive priority in the child’s care?A. Family will receive genetic counselingB. Child will participate in appropriate
activities for present conditionC. Child and family will seek support from
National Hemophilia FoundationD. Maximum function of the joint will be
restored
Review
Following administration of factor VIII to a nine year old child admitted to the hospital with hemarthrosis, the nurse’s next action would be to: A. Elevate and immobilize the
affected jointB. Institute passive range of motion to the affected joint during the acute phaseC. Apply warm compresses to the affected jointD. Apply pressure to the area as needed

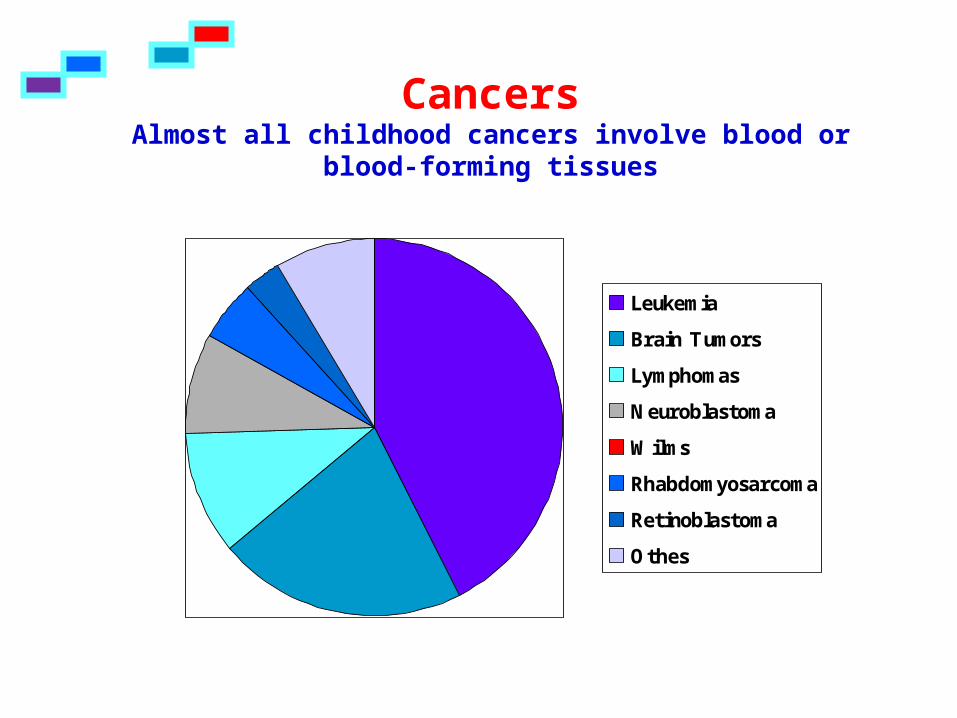
CancersAlmost all childhood cancers involve blood or
blood-forming tissues
Leukemia
Brain Tumors
Lymphomas
Neuroblastoma
Wilms
Rhabdomyosarcoma
Retinoblastoma
Othes
Brain tumors – second leading cause of death from childhood cancer. Most are cerebellar and brain stem tumors
Lymphomas Non-Hodgkins lymphomas—one-third present with a
mass in the neck or mediastinal area. Also have dyspnea, wheezing, abdominal mass or pain and lymphadenopathy.
Hodgkin’s disease – arises in single lymph node with painless nodal enlargement, followed by extension to adjacent nodes and into spleen, liver, lungs, bone marrow.
Neuroblastoma – malignant tumor arising from sympathetic NS ganglion cells outside the cranium and and can arise from anywhere along the sympathetic nervous system chain. Can also occur in retroperitoneal area, pelvis, neck.
Childhood Cancers
Wilms Tumor – solid tumor of kidney.
Rhabdomyosarcoma—malignant tumor of the striated muscle cells. occur in muscles around eye, head, neck,
extremities, GU system. Retinoblastoma – intraocular malignancy of the
retina of eye. Usually unilateral. If bilateral , hereditary. First sign is white pupil.
Others – osteogenic sarcoma/ Ewings sarcoma – tumor of bones of the trunk. Often seen in adolescence growth spurt. Found in distal femur, proximal tibia.
C = continual unexplained weight lossH = headaches with vomiting (early morning)I = increased swelling of pain in jointsL = lump or massD = development of whitish appearance in
pupilR = recurrent or persistent fevers, night
sweatsE = excessive bruising or bleedingN = noticeable paleness or tiredness
Warning Signs of Childhood Cancer
What is the major way cancer is diagnosed?
What are additional tests? Blood Tests
CBC Uric Acid
Bone Marrow Aspiration PET, SPECT MRI, CT, ultrasound
Diagnostic Tests
Radiation therapy
Chemotherapy
Surgery
Bone Marrow and Stem cell transplantation
Interventions
Radiation Therapy
Changes the DNA component ofChanges the DNA component of a cell nucleus a cell nucleus The cell cannot replicate which The cell cannot replicate which Inhibits further cell division and growthInhibits further cell division and growth
Radiation sickness- anorexia, nausea, vomiting Treated with antiemetics (Zofran or Anzimet).
Cool cloth to forehead, provide distraction, accurate I&O.
Fatigue allow for naps an rest periods (coordinate
care), encourage parent to cuddle in bed with child, pillow, blankets, favorite toys
Skin reactions –erythema, tenderness
Effects of Radiation Therapy
Bone marrow suppression – anemia, neutropenia, thrombocytopenia May be on reverse isolation
Mucositis- inflammation of mucus membranes mainly the mouth
Offer soft foods, and cold foods. Frequent mouth care. Lidocaine oral to
swish in mouth (older child)
Long term – depends on part of body receiving radiation
There are several categories of antineoplastic drugs used in treating childhood cancers.
Scheduled at set times and days and by different predetermined routes.
May remain in hospital for few days at first, then later report on specific day for therapy.
Children and Parents must be taught about what to do and not to do during therapy.
Chemotherapy
Bone Marrow Suppression – neutropenia, anemia, thrombocytopenia Place in reverse isolation, keep anyone
exposed to a virus away from patient. Monitor temperature Should not receive live-virus vaccines
Bleeding Tendency (thrombocytopenia) Apply pressure to puncture site No contact sports Check urine and stool for blood Give stool softeners. WHY? Soft objects in mouth
Side effects and Toxic Reactions to Chemotherapy
Malaise and fatigue Encourage video games, movies, etc Allow visits from friends
Nausea, vomiting, diarrhea, anorexia Give anti-emetics Small frequent meals Monitor for dehydration
Altered mucous membranes Stomatitis Rectal ulcerations
Renal involvement Uric acid levels rise as a result of breakdown of
cells. The renal tubules causing renal failure. If kidney affected/damaged- chemo drugs will
not be excreted as usual and may limit drugs given.
Body Image changes Alopecia
Pain
Side effects of chemotherapy
Chemotherapy Bone marrow
suppression Alopecia Malaise/fatigue Nausea Vomiting Anorexia Stomatitis
Radiation side effects Skin reactions Fatigue Bone marrow
suppression Nausea Vomiting Anorexia Mucositis
Review of Common Side Effects of
Chemotherapy and Radiation
CurativeRemove the tumor and
cancerous tissue
PalliativeRelieve complications due to
the cancer
Surgery
The goal of therapy is to administer a lethal dose of chemotherapy and radiation therapy that will kill the cancer and then re-supply the body with bone marrow and stem cells to reconstitute immunologic function.
Healthy bone marrow or stem cells are infused into the bloodstream and migrate to the marrow space to replenish the patient’s immunologic function and help kill remaining cancer cells.
Bone Marrow and Stem Cell Transplantation
Syngeneic bone marrow comes from identical twin
Allogeneic bone marrow comes from matched sibling (one in
four chances) or someone who is histocompatible.
Autologous own bone marrow. May be harvested at time of
remission in preparation for relapse or when bone marrow is free of malignant cells. Also being used so toxic doses of chemotherapy and radiation can be administered and the bone marrow rescued.
Types of Transplantations
First --All potential donors are typed for HLA (human leukocyte antigen) compatibility.
Collection of bone marrow is a surgical procedure. The donor undergoes anesthesia for aspiration of the
bone marrow The bone marrow is then processed and frozen
When patient ready - it is infused into the recipient.
Procedure
Where is the most common site for bone marrow aspiration in children?
1. Graft-Versus-Host Disease (GVHD) – potentially lethal immunologic response of donor T cells against the tissue of the recipient. Signs and symptoms – rash, malaise, high
fever, diarrhea, liver and spleen enlargement. Because there is no cure, prevention is
essential. Careful tissue typing, irradiation of blood products which helps to inactivate mature T lymphocytes.
2. Rejection of the transplant
Side effects of Transplantation
CNS – cognitive disorders, seizures, headaches, coordination problems
Bone – asymmetric growth of bones, easy fractures, scoliosis, kyphosis
CV – cardiomyopathy (pericardial thickening) , pericardial damage
Respiratory – pneumonitis, pulmonary fibrosis GI – enteritis, bleeding, hepatic fibrosis Urinary – hemorrhagic cystitis, reflux Endocrine – decrease in growth, thyroid and
gonadal dysfunction Reproductive – decrease sperm Dental - caries Secondary malignancies
Post Therapeutic Disabilities
What is the most common form of childhood cancer?a. leukemiab. brain tumorsc. lymphomad.osteosarcoma
Ask Yourself?

The WBC's are produced so rapidly that immature cells (blast cells) are released into the circulation.
These blast cells are nonfunctional, can't fight infection, and are formed continuously without respect to the body's needs
The blasts cells then invade other organs and interfere with metabolism / function. The production of red blood cells and platelets decreases leading to anemia and thrombocytopenia.
How does that impact the body?
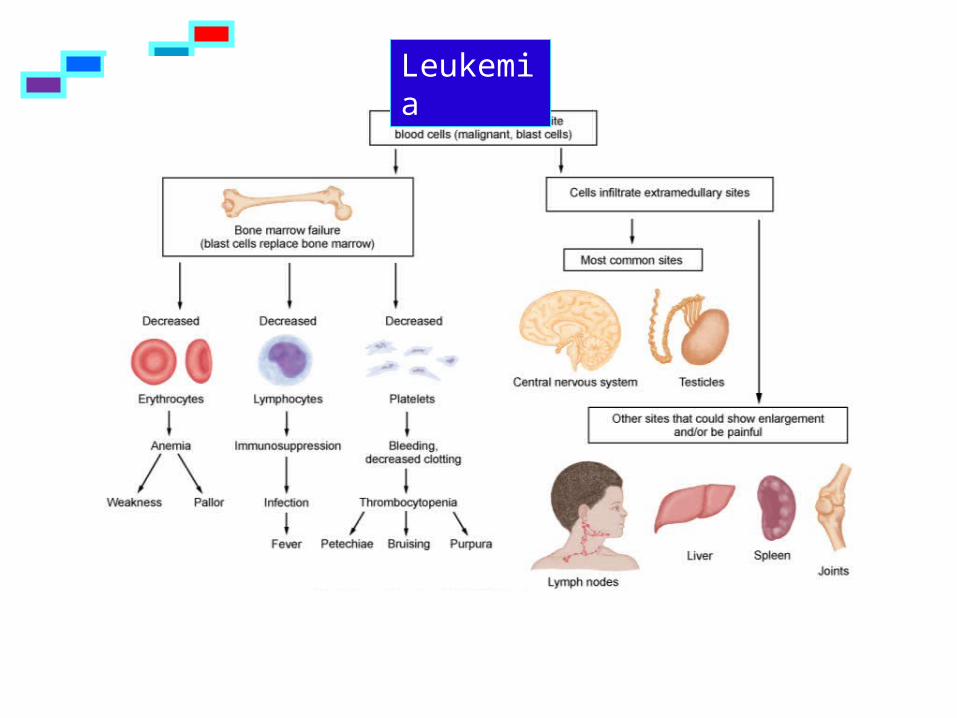
Leukemia
Bone marrow Depression results in:1. Decrease in mature WBC’s - fever2. Decrease RBC’s, Anemia- pallor, lethargy, anorexia3. Decreased Platelets/ thrombocytopenia- bleeding4. Increase cell metabolism which deprives cells of
nutrients 5. Enlargement of organs infiltrated with blast cells
results in: Bone pain Spleenomegaly. Hepatomegaly, Nephromegaly Lymphadenopathy CNS infiltration – increased ICP
Signs & Symptoms
Diagnostic Tests History and Physical
Blood Work Leukocytes are > 10,000 Platelet count, Hgb and Hct low Blast cells appear (where they normally don’t)
Bone Marrow Aspiration Used to identify the type of WBC involved,
therefore, type of leukemia
X-rays of long bones Show lesions caused by invasion of abnormal
cells
Lumbar Puncture – blast cells in the CSF
A combination of antineoplastic drugs are given for about a month
A different combination is given for about 2-3 years
Advantages of using a combination of drugs: Decrease resistance to one drug Lessening of severe side effects of massive
doses of one drug Breakdown of the tumor cell cycle at multiple
sites
Chemotherapy
1. Remission induction- most intense treatment. Large doses of antineoplastic drug administered in an effort to destroy as many proliferating cells as possible. Lasts 4-6 wks. About 95% respond.
2. Consolidation- method of destroying leukemic cells in the CNS- for children who have CNS involvement or are high risk. Given Intrathecal.
3. Remission maintenance- drugs given at specific intervals. If remain in remission for 3 yrs, treatment is discontinued. Approx 80% of children who sustain remission for 2-3 yrs continue to remain in remission and appear to be cured.
Chemotherapy Phases
Administration of Chemotherapy
When is intrathecal administration of chemotherapeutic medications
required?
Intrathecal chemotherapy is instilled in to the spinal canal for
cancers that have metastasized to the brain
What is the rationale for the use of cranial radiation in addition to chemotherapy?
What is the rationale for the use of cranial radiation in addition to chemotherapy?
Prevent infection (neutropenia, anemia) Pain Relief Nausea and vomiting Mouth discomfort-mucositis / stomatitis Fatigue Alopecia Prevent blood loss-platelet low- nose bleed most
common kind of bleed Support child and family Assist with referrals to social services, home
health agency, chaplain
Nursing Care
Community Resource Candlelighters Childhood Cancer Foundation® (CCCF)
is a national non-profit membership organization whose mission is to educate, support, serve, and advocate for families of children with cancer, survivors of childhood cancer, and the professionals who care for them.
http://www.candlelighters.org/ American Cancer Society Make a wish Foundation Leukemia Society Church and Schools
Nursing Care
Caused by the breakdown (lysis) of malignant cells which release intracellular contents into the blood.
Intracellular electrolytes overload the kidneys and can lead to kidney failure.
Further severe electrolyte imbalances cause metabolic acidosis, hyperkalemia, increase uric acid levels, hypocalcemia and cardiac arrythmias.
Tumor Lysis Syndrome p. 1325
Tumor Lysis Syndrome
PREVENTION Hydrate with IV fluids containing
bicarbonate which alkalinizes the urine preventing formation of uric acid crystals which damage the kidney
Treatment Treat with IV fluids, electrolyte
replacement, allopurinol.
An embryonic tumor of the kidney.
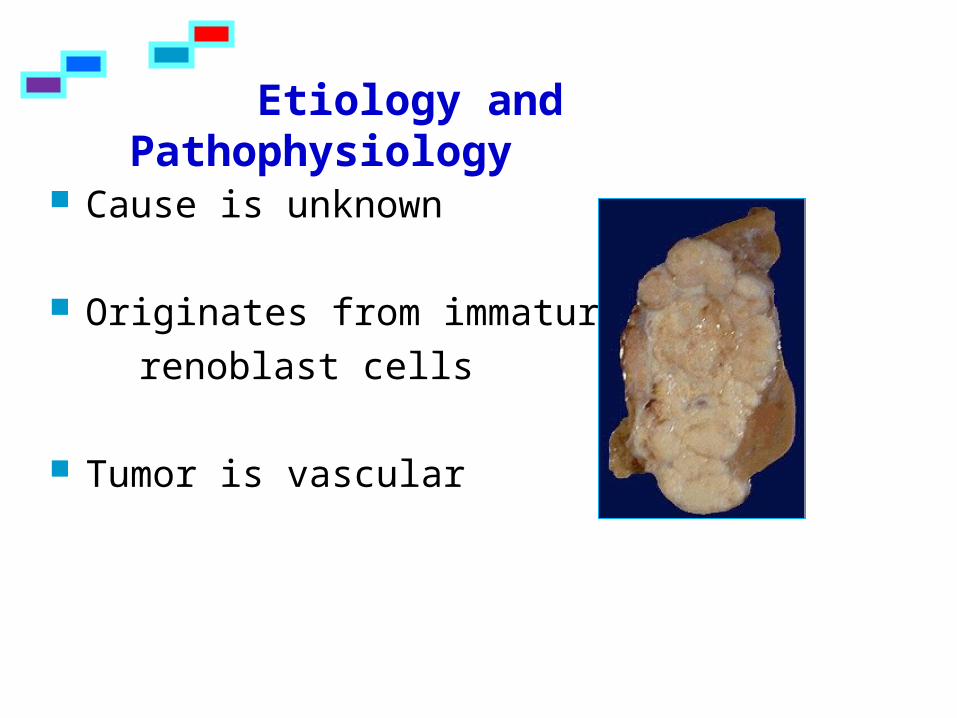
Cause is unknown
Originates from immature renoblast cells
Tumor is vascular
Etiology and Pathophysiology
Palpable abdominal mass Firm and smooth
**The abdomen should not be palpated once the diagnosis is made. Avoid palpating the tumor mass during assessment because of the risk of rupturing the protective capsule. Excessive manipulation can cause seeding of the tumor and spread of cancerous cells
Abdominal distention Fever Fatigue Late signs
Anemia Hematuria, dysuria Hypertension
Assessment
Abdominal ultrasound
CT, MRI
Biopsy
Diagnostic Tests
Nephrectomy and removal of lymph nodes
Post-op chemotherapy and / or radiation therapy
CT every 6 months for 3 years
Chest x-ray every 3 months for 3 years
Interventions
Pre-op Sign on bed ”Do Not Palpate Abdomen” Child / Parent teaching
Post-op Monitor kidney function, Strict I & O Monitor vital signs—B/P and temperature Monitor GI function– assess bowel sounds and
stool production NG tube to drainage. Measure abdominal girth.
Nursing Care
Caring for a child who is dying can be one of the hardest tasks in nursing
Children under 3 Have no understanding of own impending death May perceive family anxiety, sadness
Preschool to 5 years More afraid of separation from parents than of
thought of dying. Greatest fear is separation. Envision death as temporary, and have little of
adults’ fear of it Think of it as a long sleep, not a final process.
Nightmares increase. May feel pain / illness is a punishment for
misdeeds or thoughts May ask questions about death In long term illness – may simulate adult
response with depression, withdrawal, fearfulness, anxiety
Understanding of Death
School Age 5-9 Begin to understand that death is
permanent May think it is something that only happens
to adults Become aware of what is happening to them
when their disorder has a fatal prognosis. Concerns center around fear of pain, fear of
being left alone and leaving parents and friends.
May associate death with sleep and may be afraid to go to sleep without someone near them.
May associate death with darkness—want light left on in room
Adolescent, older school age By age 10 have an adults concept of death,
realizing that it is inevitable, universal, and irreversible. Have more understanding than adults realize.
Understand that death is the cessation of life. Emotional outbursts may reflect anger View death as fearsome and fascinating
(increase in adolescent suicide). May feel immune to death and deny symptoms
for longer than usual because they believe it is impossible that anything serious could happen to them.
Some adolescents consider themselves alienated from their peers and unable to communicate with their parents for emotional support feeling alone in their struggle.
Understanding Death
1. Elicit child's understanding of death before discussing
2. Encourage children to express feelings in own way through play, drawings, or verbalization to promote free expression.
3. Provide a safe, acceptable outlet for expressions of feelings
4. Structure care of child to allow child choices and participation in process within constraints of physical condition
5. Help child maintain independence and control; normal ADL as much as possible (set realistic goals)
6. Realize that they will go through the stages of dying: denial, bargaining, anger, depression, acceptance
Nursing Care Child
1. Spend time with family to listen, answer questions, and provide information. Discuss issues with parents before discussing with child.
2. Provide opportunities for family to express their emotions and deal with their feelings. Parental reactions: continuum of grief process and usually depend on previous experiences with loss, intellectualization.
3. Reactions may depend on relationship with child and circumstances of illness or injury
4. Reactions depend on degree of guilt felt by parents-help them sort out
Nursing Care Parents
5. Assist parents in expressing fears, concerns, grief to enable them to appropriately support child
6. Assist parents to understand sibling' possible reactions to terminally ill child· Guilt- believing they caused the problem or
illness· Jealousy- wanting equal attention from
parents· Anger- feelings of being left behind
7. Support, enhance parent-child communication, enhance parents' ability to support child
8. Refer to parent, family support groups- not alone, help focus, open communication, provide information
Nurse needs to care for self.
Care of the caregiver is imperative if the nurse is to provide physical and psychosocial care for families at such a difficult time.
Caring for dying children and their families can be stressful and emotionally demanding.
Nursing Care Nurse
Top Related