
![主讲:罗英瑾upload.htexam.net/jiangyi/1207130404423932.pdf解剖学 第[5]页 客服电话:400-678-1009 第一篇 运动系 组成:骨:杠杆 骨连结:枢纽 骨骼肌:动力](https://static.fdocuments.net/doc/165x107/5e2b84a559e3390455224d78/eicec-e-c5e-oecei400-678-1009-cc-ec.jpg)




Languages
Pages
Legal

肌肉骨骼系统
骨 骼
Content
骨骼大体解剖
骨组织学
骨组织新陈代谢
骨组织生物力学
骨折愈合
骨骼疾病
骨折愈合(不愈合)
骨坏死
骨折疏松
器械、生物材料,药物,细胞,因子
4
By age 25 the skeleton is completely hardened
206 bones make up the adult
skeleton (20% of body mass) 80 bones of the axial skeleton
126 bones of the appendicular skeleton
The actual number of bones in the human
skeleton varies from person to person
骨骼的大体解剖
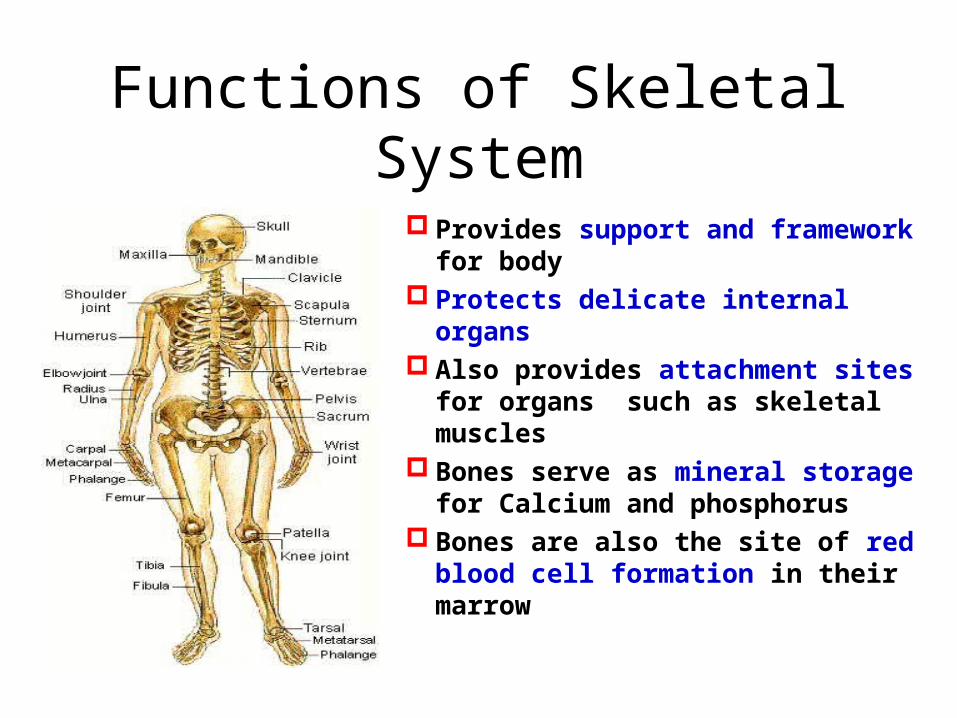
Functions of Skeletal System
Provides support and framework for body
Protects delicate internal organs
Also provides attachment sites for organs such as skeletal muscles
Bones serve as mineral storage for Calcium and phosphorus
Bones are also the site of red blood cell formation in their marrow

Bone as a signalling centre
314 | NATURE | VOL 481 | 19 JANUARY 2012
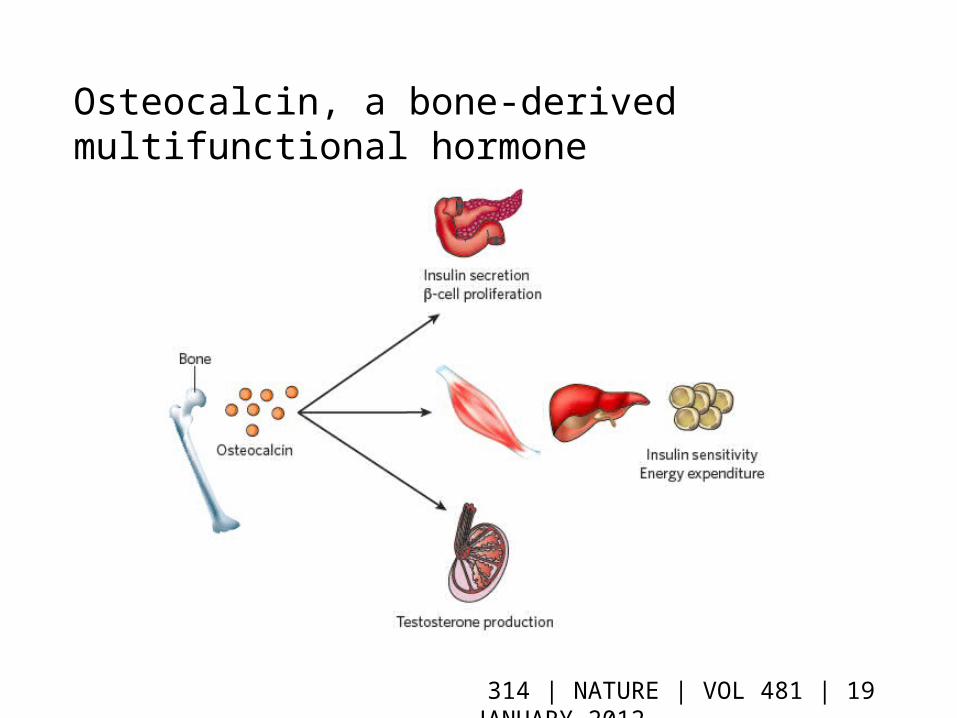
Osteocalcin, a bone-derived multifunctional hormone
314 | NATURE | VOL 481 | 19 JANUARY 2012
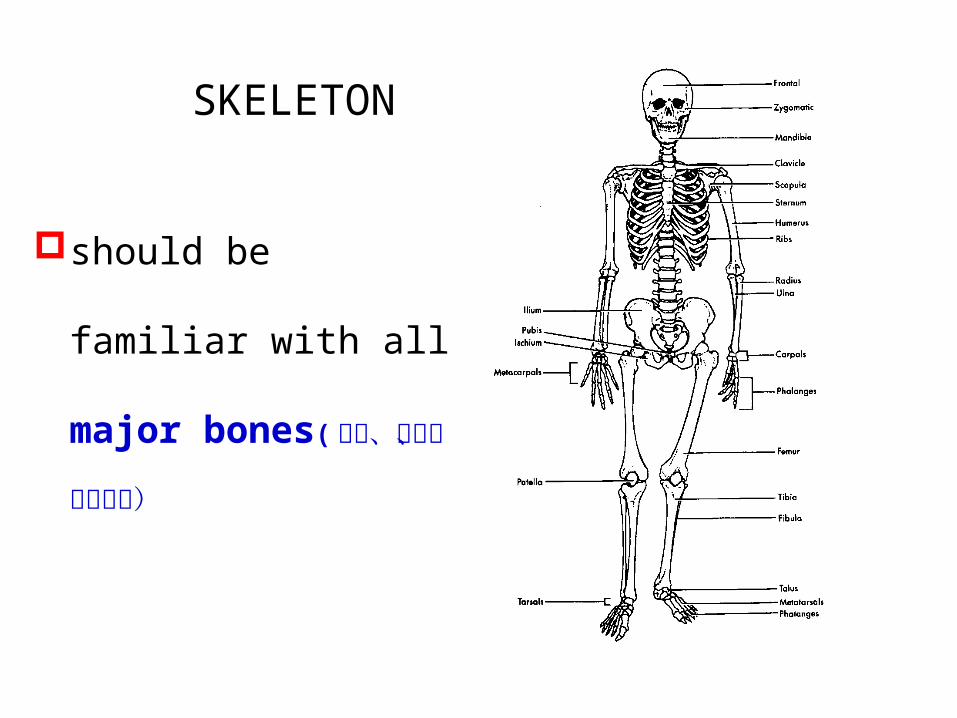
should be familiar with
all major bones( 脊柱、
骨盆、四肢长骨)
SKELETON
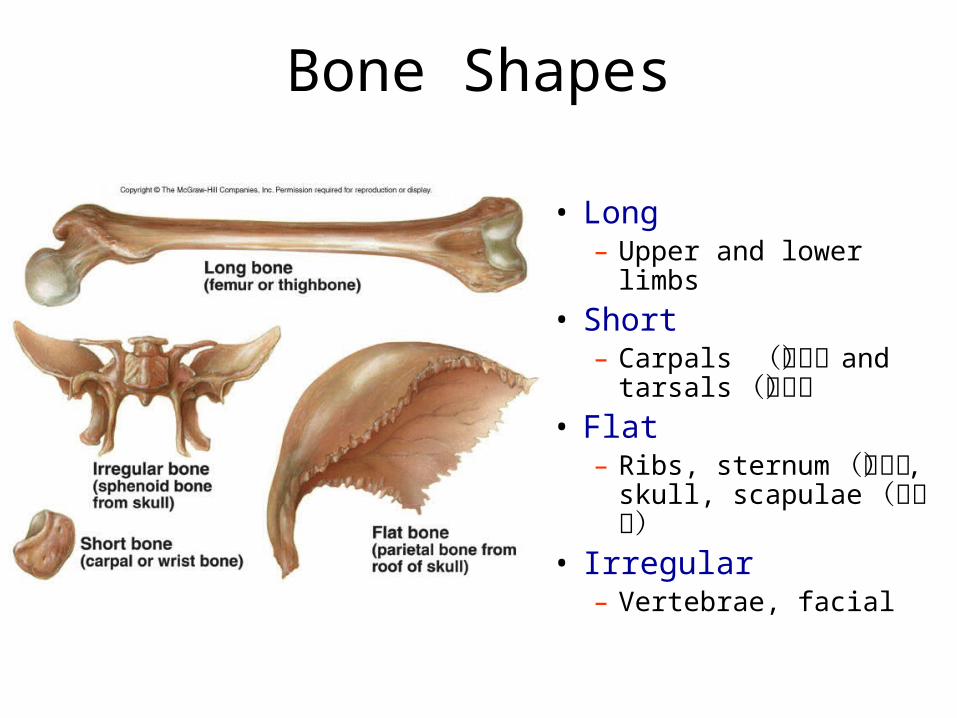
Bone Shapes
• Long– Upper and lower limbs
• Short– Carpals (腕骨) and
tarsals (跗骨)• Flat
– Ribs, sternum (胸骨) , skull, scapulae (肩胛骨)
• Irregular– Vertebrae, facial
10
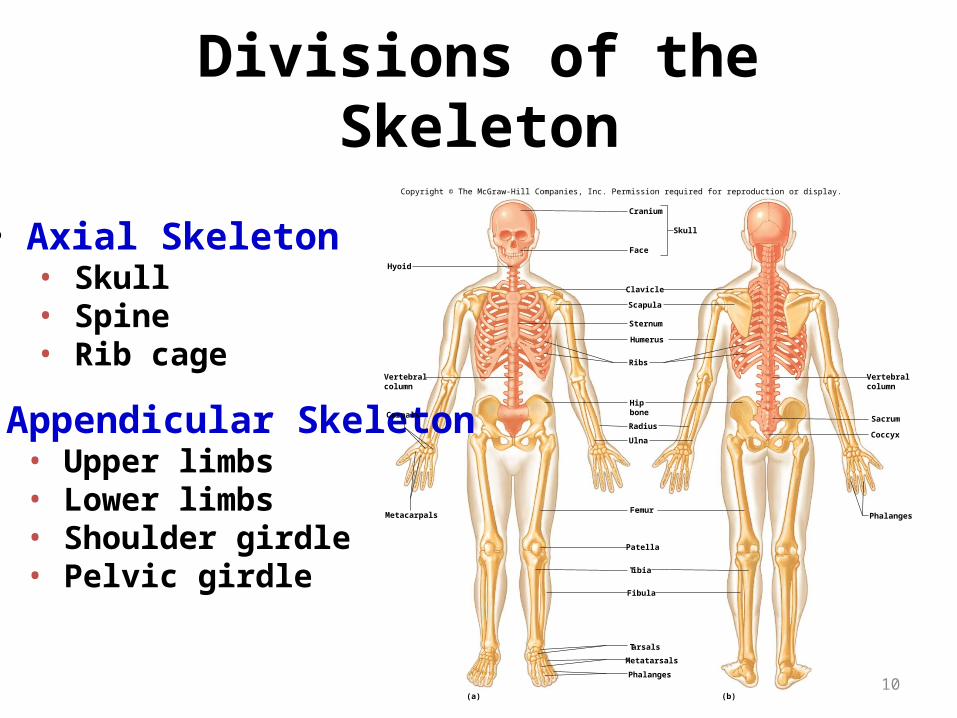
Divisions of the Skeleton
• Axial Skeleton• Skull • Spine • Rib cage
• Appendicular Skeleton• Upper limbs• Lower limbs• Shoulder girdle• Pelvic girdle
Hyoid
Cranium
Face
Clavicle
Scapula
Sternum
Ribs
Humerus
Ulna
Hipbone
Radius
Femur
Patella
Tibia
Fibula
Tarsals
Metatarsals
Phalanges
Phalanges
Skull
Vertebralcolumn
Vertebralcolumn
Sacrum
Coccyx
Carpals
Metacarpals
(a) (b)
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
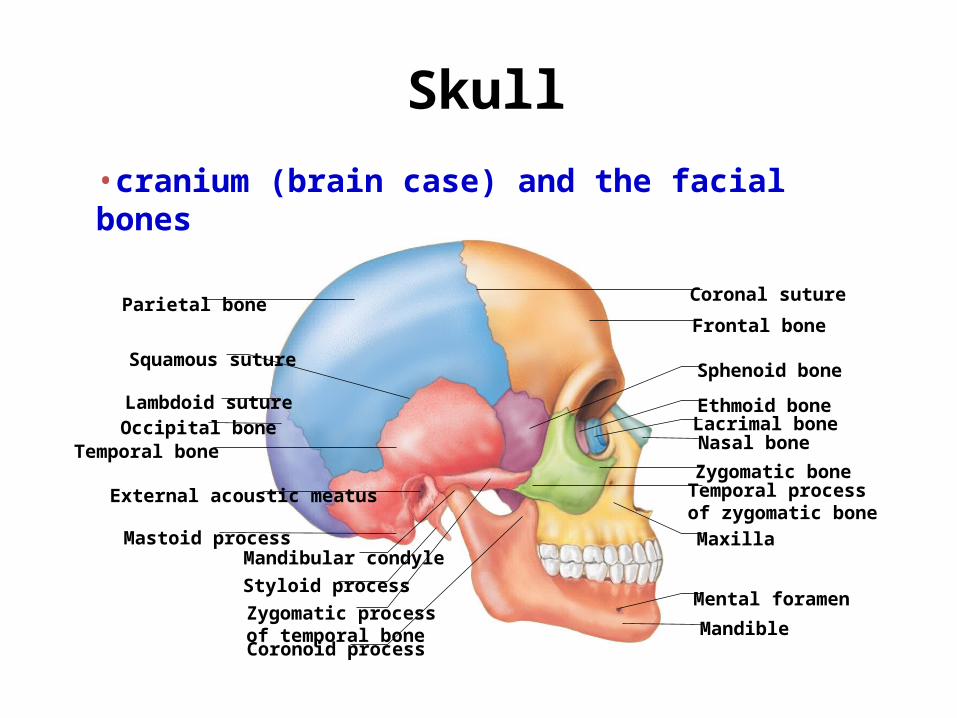
Coronal suture
Frontal bone
Sphenoid bone
Ethmoid boneLacrimal boneNasal bone
Zygomatic bone
Maxilla
Mental foramen
MandibleCoronoid process
Styloid process
Mandibular condyleMastoid process
External acoustic meatus Temporal processof zygomatic bone
Zygomatic processof temporal bone
Occipital boneTemporal bone
Parietal bone
Lambdoid suture
Squamous suture
Skull•cranium (brain case) and the facial bones
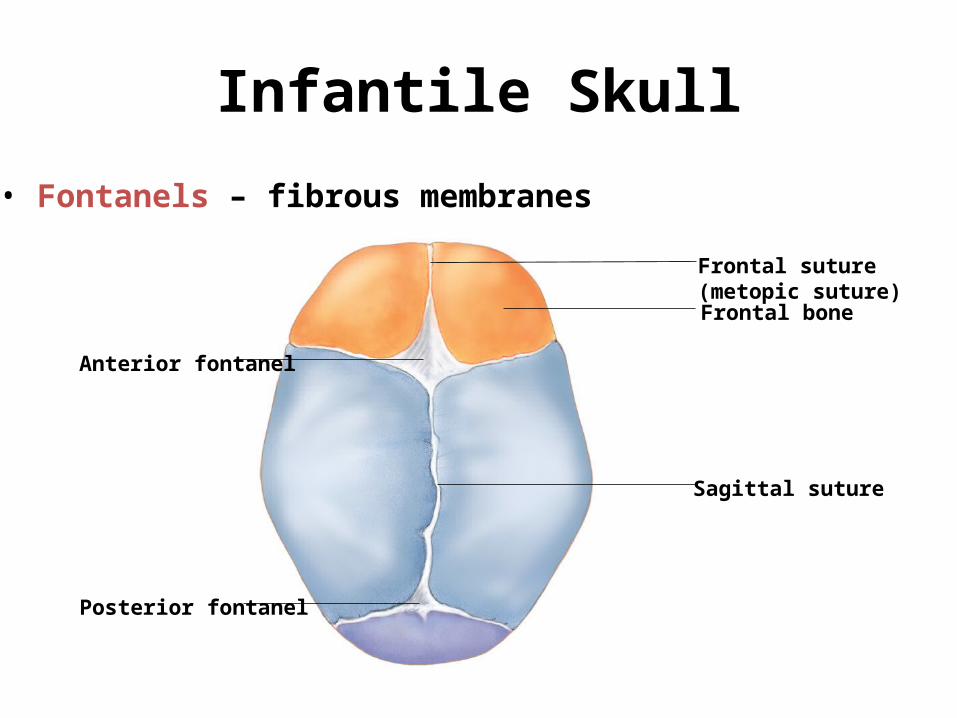
Infantile Skull
• Fontanels – fibrous membranes
Anterior fontanel
Posterior fontanel
Frontal bone
Frontal suture(metopic suture)
Sagittal suture
13
Vertebral Column
The vertebral column, or spinal column,
consists of many vertebrae separated
by cartilaginous intervertebral discs.
14
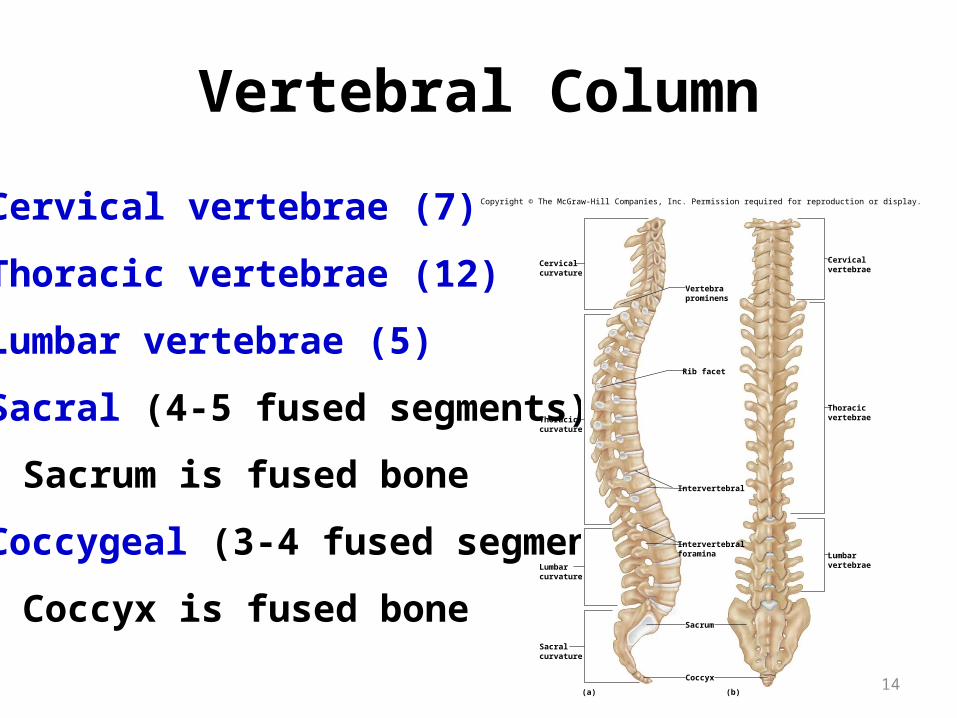
Vertebral Column
Cervical vertebrae (7)
Thoracic vertebrae (12)
Lumbar vertebrae (5)
Sacral (4-5 fused segments)
• Sacrum is fused bone
Coccygeal (3-4 fused segments)
• Coccyx is fused bone
(b)(a)
Cervicalcurvature
Thoraciccurvature
Lumbarcurvature
Lumbarvertebrae
Thoracicvertebrae
Cervicalvertebrae
Sacralcurvature
Vertebraprominens
Rib facet
Intervertebral
Intervertebralforamina
Sacrum
Coccyx
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
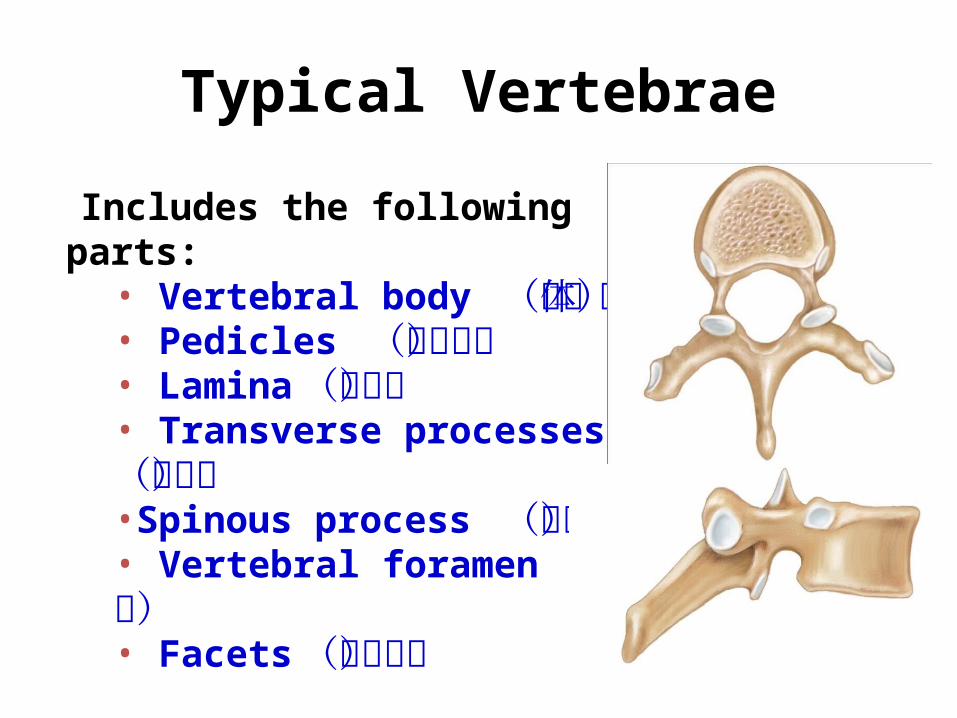
Typical Vertebrae
Includes the following parts:• Vertebral body (椎体)• Pedicles (椎弓根)• Lamina (椎板)• Transverse processes (横突)•Spinous process (棘突)• Vertebral foramen (椎孔)• Facets (关节突)
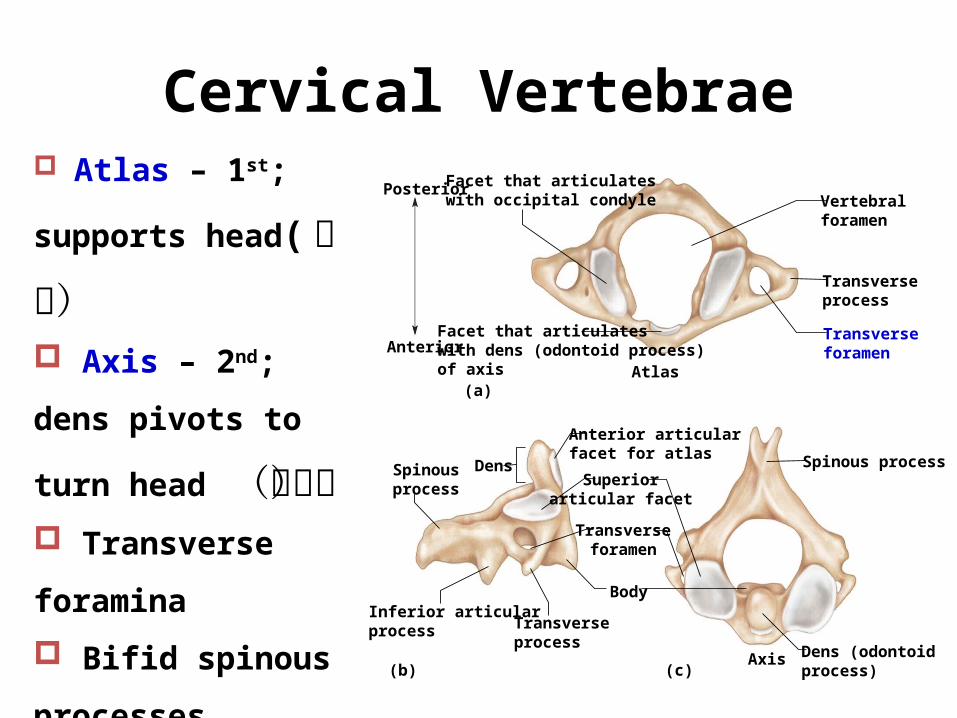
Cervical Vertebrae Atlas – 1st; supports
head( 寰椎) Axis – 2nd; dens pivots
to turn head (枢椎) Transverse foramina
Bifid spinous
processes
Vertebral prominens
– useful landmark(b) (c)
(a)
Anterior
Posterior
Atlas
Axis
Body
Dens (odontoidprocess)
Spinous processDens
Inferior articularprocess
Facet that articulateswith dens (odontoid process)of axis
Facet that articulateswith occipital condyle
Spinousprocess
Anterior articularfacet for atlas
Transverseforamen
Transverseprocess
Superiorarticular facet
Vertebralforamen
Transverseprocess
Transverseforamen
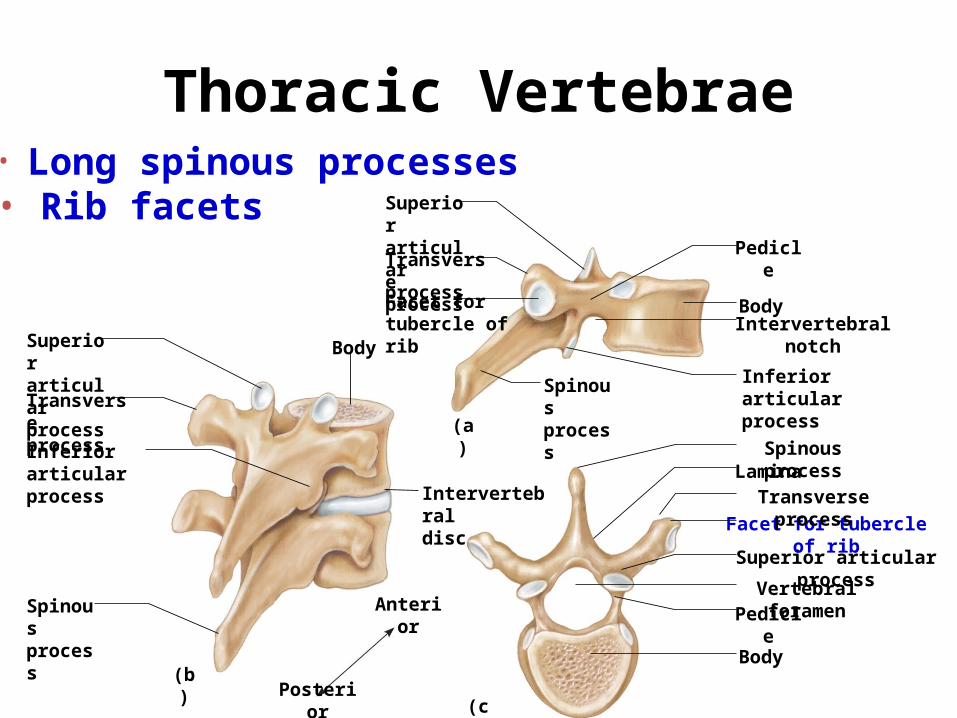
Thoracic Vertebrae
BodySuperiorarticularprocess
Spinousprocess
Transverseprocess
Inferior articularprocess
Intervertebraldisc
Anterior
Posterior
Body
PedicleVertebral foramen
Superior articular process
Facet for tubercle of rib
Transverse processLamina
Spinous process
Inferior articularprocess
Intervertebral notchBody
Pedicle
SuperiorarticularprocessTransverseprocessFacet fortubercle of rib
Spinousprocess
(a)
(c)
(b)
• Long spinous processes• Rib facets

18
Lumbar Vertebrae
• Large bodies• Thick, short spinous processes
(c) Lumbar vertebra
Lamina
Pedicle
Body
Vertebral foramen
Spinous process
Superior articularprocess
Transverse process
Sacral canal
Tubercleof mediansacral crest
Auricularsurface
Posterior sacralforamenSacral hiatus
Coccyx
Sacrum
Superior articular process
Sacral promontory
Anterior sacralforamen
(a) (b)
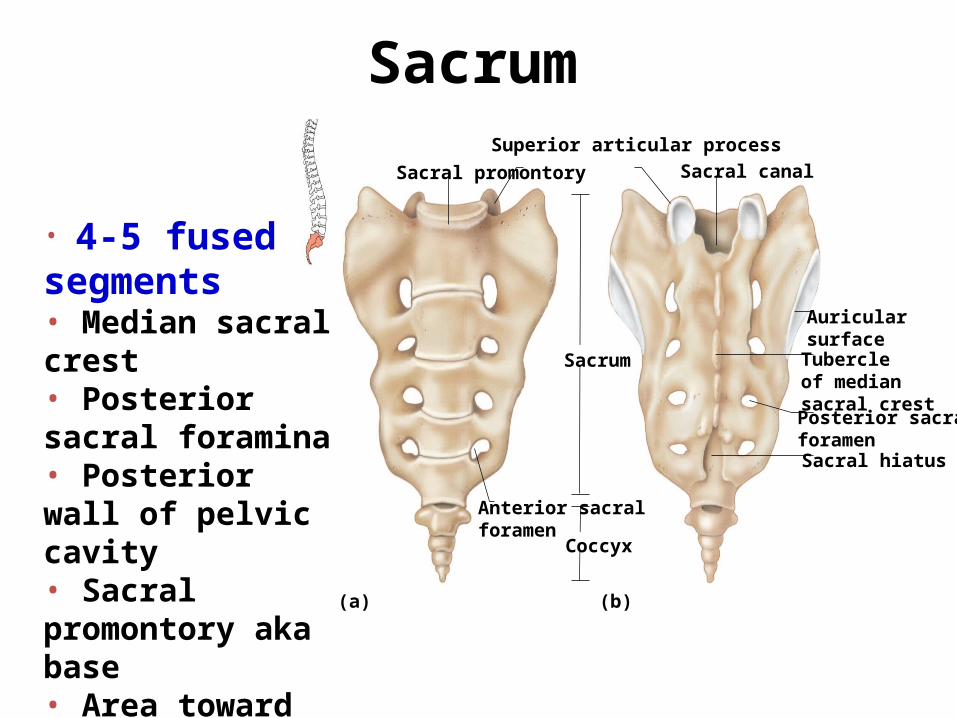
Sacrum
• 4-5 fused segments• Median sacral crest• Posterior sacral foramina• Posterior wall of pelvic cavity• Sacral promontory aka base• Area toward coccyx is the apex
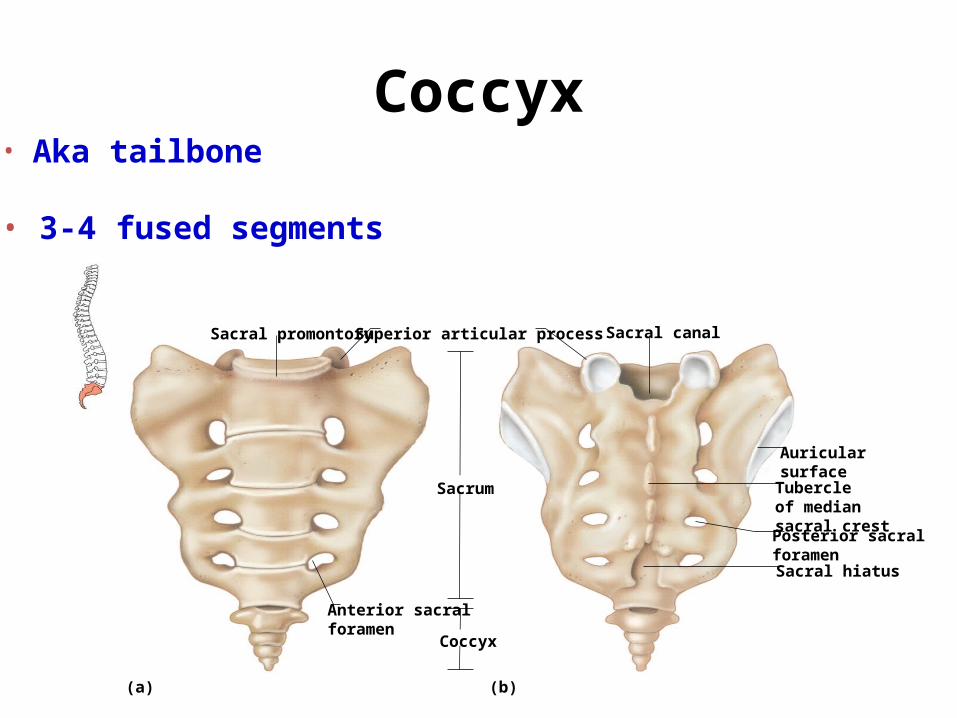
Coccyx• Aka tailbone
• 3-4 fused segments
Sacral canal
Tubercleof mediansacral crest
Auricularsurface
Posterior sacralforamenSacral hiatus
Coccyx
Sacrum
Superior articular processSacral promontory
Anterior sacralforamen
(a) (b)
21
Thoracic Cage
• The thoracic cage includes the ribs, the
thoracic vertebrae, the sternum, and the
costal cartilages that attach the ribs to the
sternum.
22
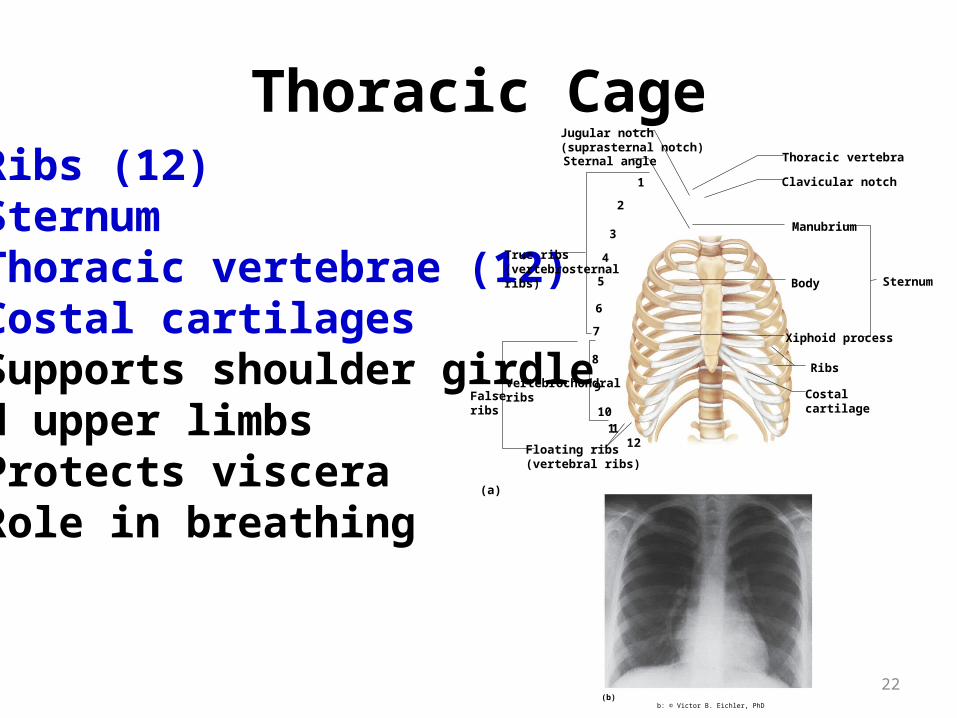
Thoracic Cage• Ribs (12)• Sternum• Thoracic vertebrae (12)• Costal cartilages• Supports shoulder girdleand upper limbs• Protects viscera• Role in breathing
1
2
3
4
5
6
7
8
9
1011
12
True ribs(vertebrosternalribs)
VertebrochondralribsFalse
ribs
(a)
Floating ribs(vertebral ribs)
SternumBody
Manubrium
Ribs
Costalcartilage
Xiphoid process
Thoracic vertebra
Clavicular notch
Sternal angle
Jugular notch(suprasternal notch)
(b)b: © Victor B. Eichler, PhD
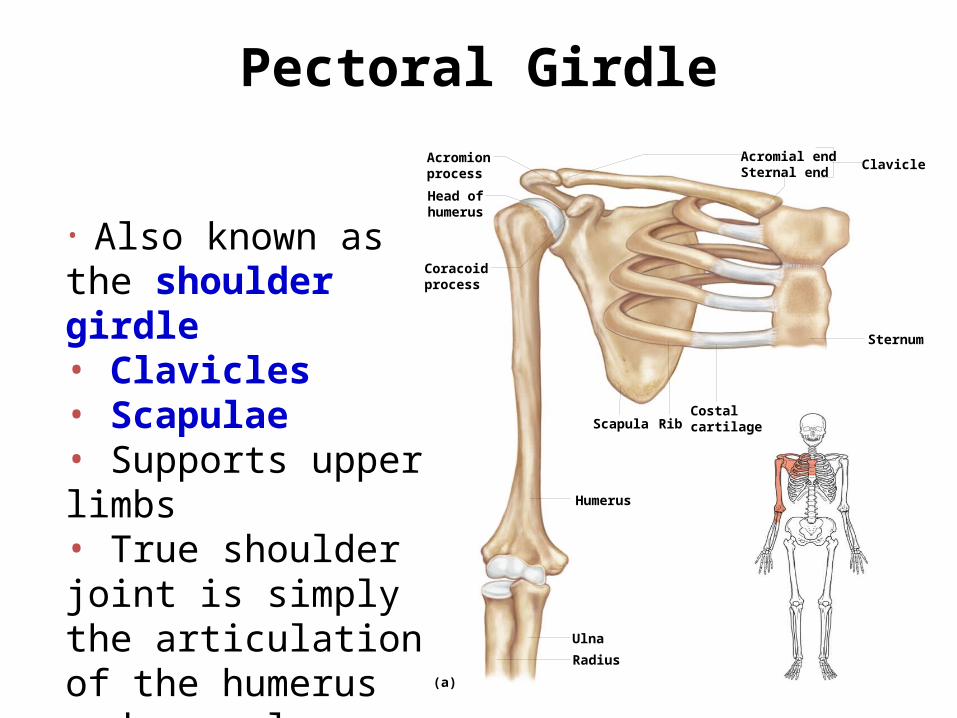
Pectoral Girdle
• Also known as the shoulder girdle • Clavicles• Scapulae• Supports upper limbs• True shoulder joint is simply the articulation of the humerus and scapula
Sternum
CostalcartilageRibScapula
Humerus
Ulna
Radius
Clavicle
(a)
Coracoidprocess
Head ofhumerus
Acromionprocess
Acromial endSternal end
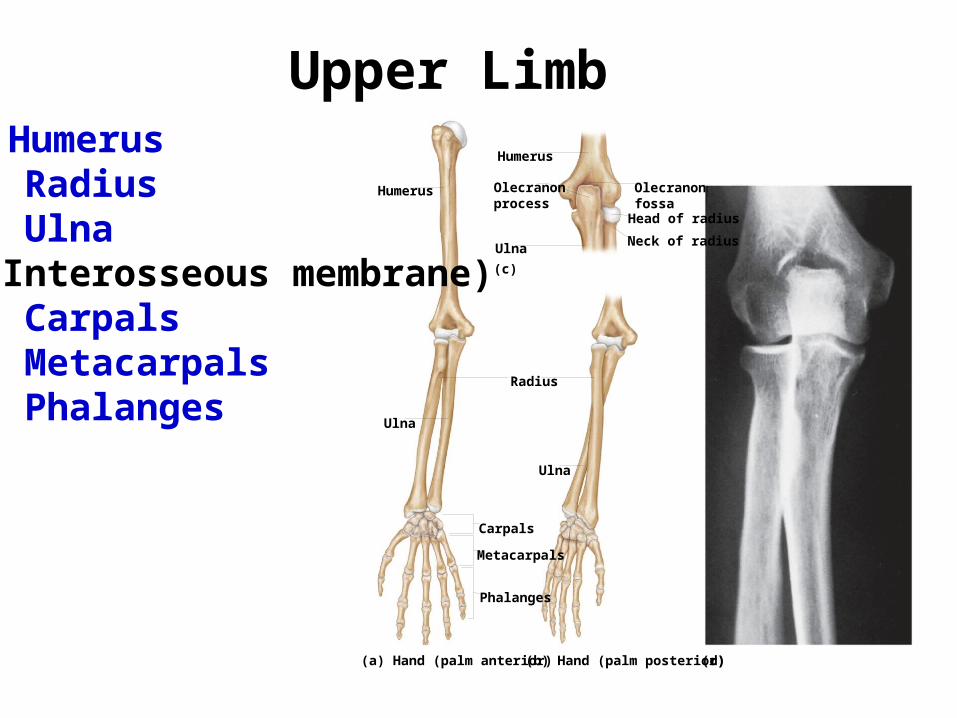
Upper Limb
Olecranonprocess
Head of radius
Neck of radiusUlna
Olecranonfossa
Carpals
Metacarpals
Phalanges
Humerus
Humerus
Ulna
Ulna
Radius
(c)
(d)(a) Hand (palm anterior) (b) Hand (palm posterior)
• Humerus• Radius• Ulna(Interosseous membrane)• Carpals• Metacarpals• Phalanges
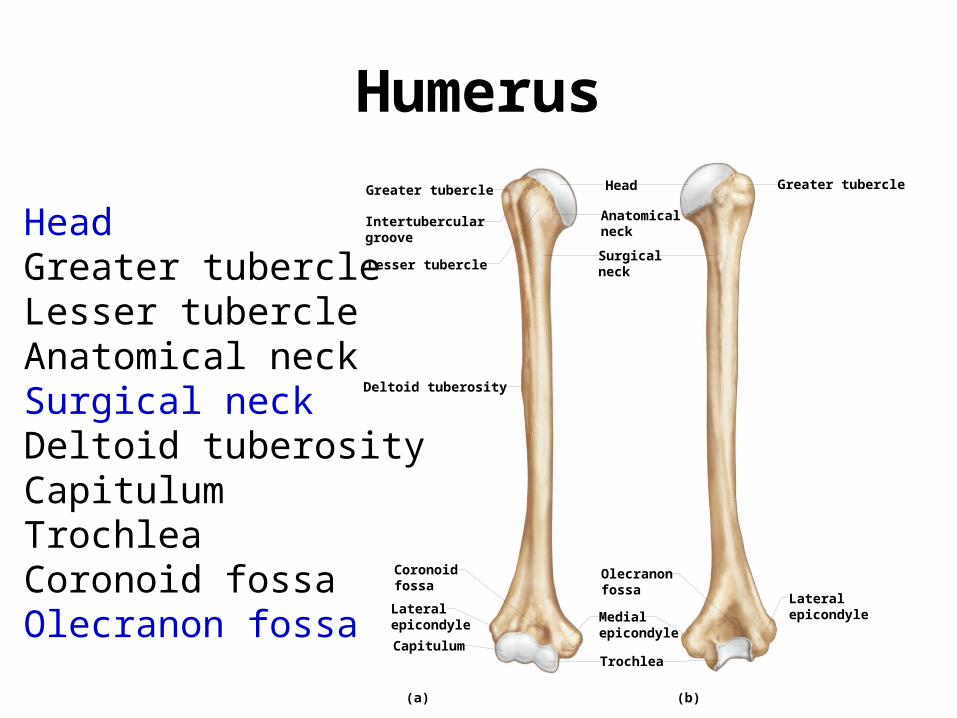
Humerus
• Head• Greater tubercle• Lesser tubercle• Anatomical neck• Surgical neck• Deltoid tuberosity• Capitulum• Trochlea• Coronoid fossa• Olecranon fossa
CapitulumTrochlea
Deltoid tuberosity
Head
Lesser tubercle
Greater tubercle Greater tubercle
(a) (b)
Lateralepicondyle
Coronoidfossa
Intertuberculargroove
Medialepicondyle
Olecranonfossa
Anatomicalneck
Surgicalneck
Lateralepicondyle
26
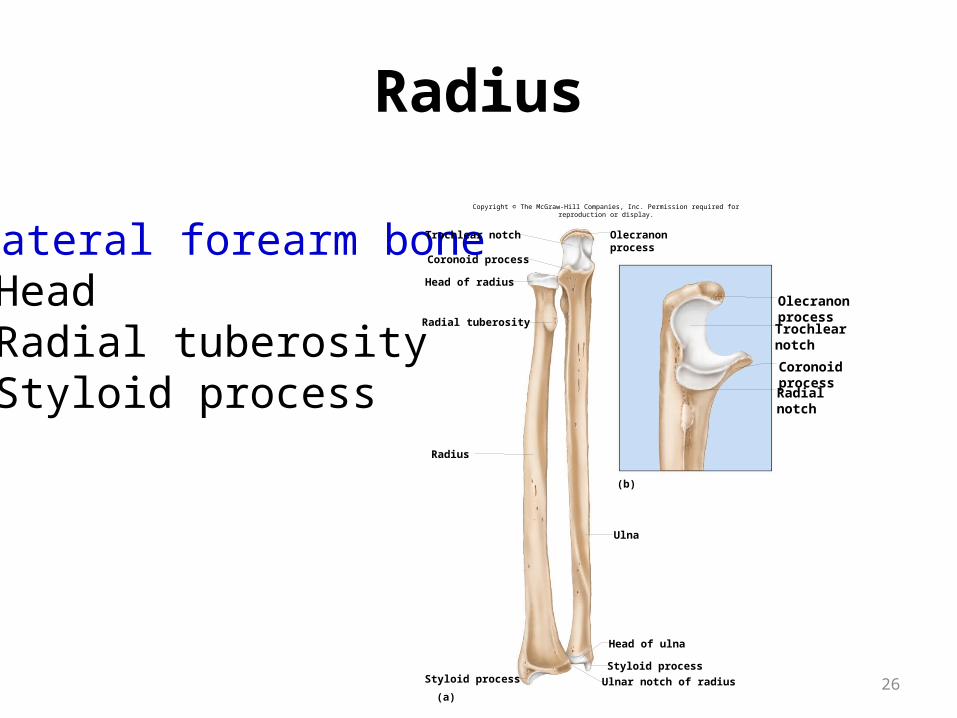
Radius
• Lateral forearm bone• Head• Radial tuberosity• Styloid process
Styloid process Ulnar notch of radius
Styloid process
Head of ulna
Ulna
Radius
Radial tuberosity
Head of radius
Coronoid process
Trochlear notch Olecranonprocess
(b)
(a)
OlecranonprocessTrochlearnotch
CoronoidprocessRadialnotch
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
27
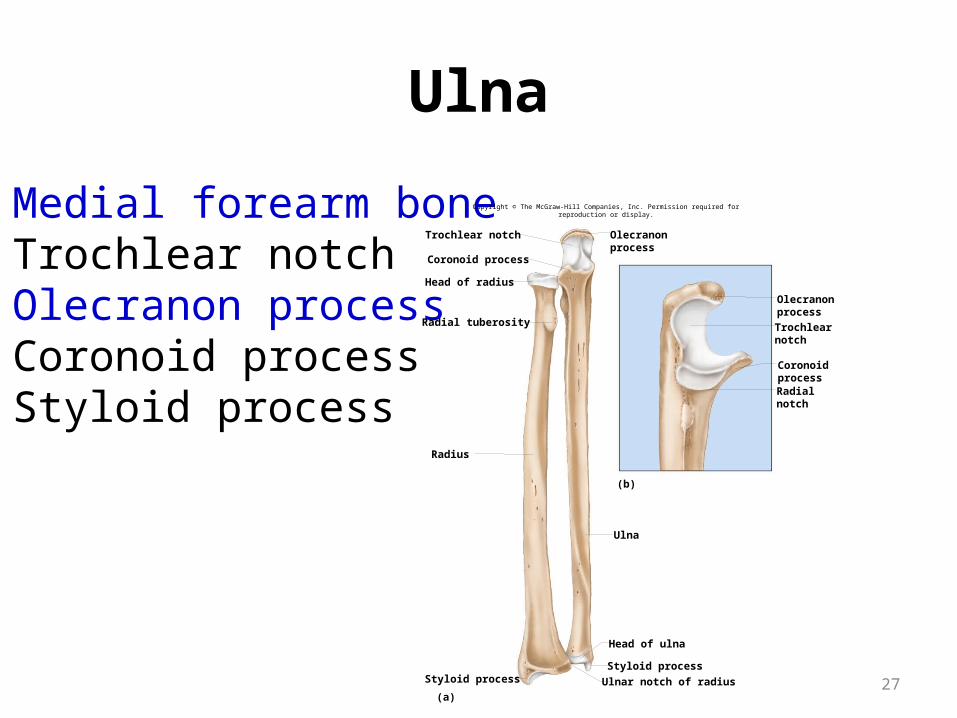
Ulna
• Medial forearm bone• Trochlear notch• Olecranon process• Coronoid process• Styloid process
Styloid process Ulnar notch of radius
Styloid process
Head of ulna
Ulna
Radius
Radial tuberosity
Head of radius
Coronoid process
Trochlear notch Olecranonprocess
(b)
(a)
Olecranonprocess
Trochlearnotch
CoronoidprocessRadialnotch
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
28
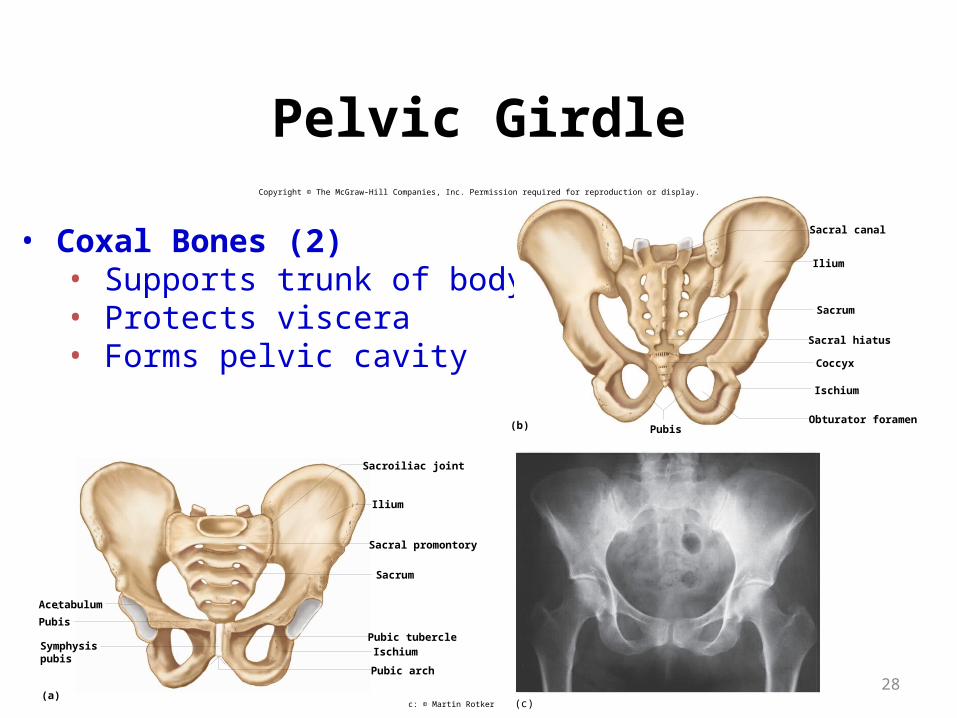
Pelvic Girdle
• Coxal Bones (2)• Supports trunk of body• Protects viscera• Forms pelvic cavity
Sacrum
Sacral promontory
Sacroiliac joint
Acetabulum
Pubis
Symphysispubis
(a)
Pubic arch
IschiumPubic tubercle
Ilium
Obturator foramen
Ischium
Coccyx
Sacral hiatus
Sacrum
(b)
Ilium
Sacral canal
Pubis
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
(c)c: © Martin Rotker
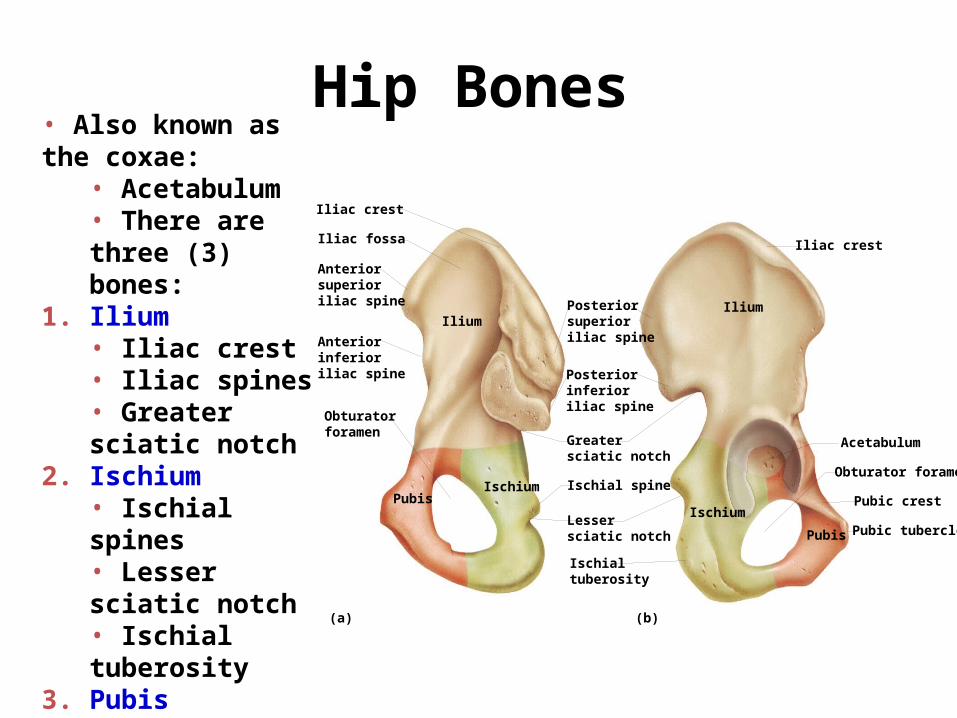
Hip Bones• Also known as the coxae:
• Acetabulum • There are three (3) bones:
1. Ilium• Iliac crest• Iliac spines• Greater sciatic notch
2. Ischium• Ischial spines• Lesser sciatic notch• Ischial tuberosity
3. Pubis• Obturator foramen• Symphysis pubis• Pubic arch
Iliac crest
Iliac crestIliac fossa
IliumIlium
Ischium
IschiumPubis
Pubis
Ischial spineObturator foramen
Acetabulum
Pubic crest
Pubic tubercle
(b)(a)
Anteriorsuperioriliac spine
Anteriorinferioriliac spine
Posteriorsuperioriliac spine
Posteriorinferioriliac spine
Greatersciatic notch
Lessersciatic notch
Ischialtuberosity
Obturatorforamen
30
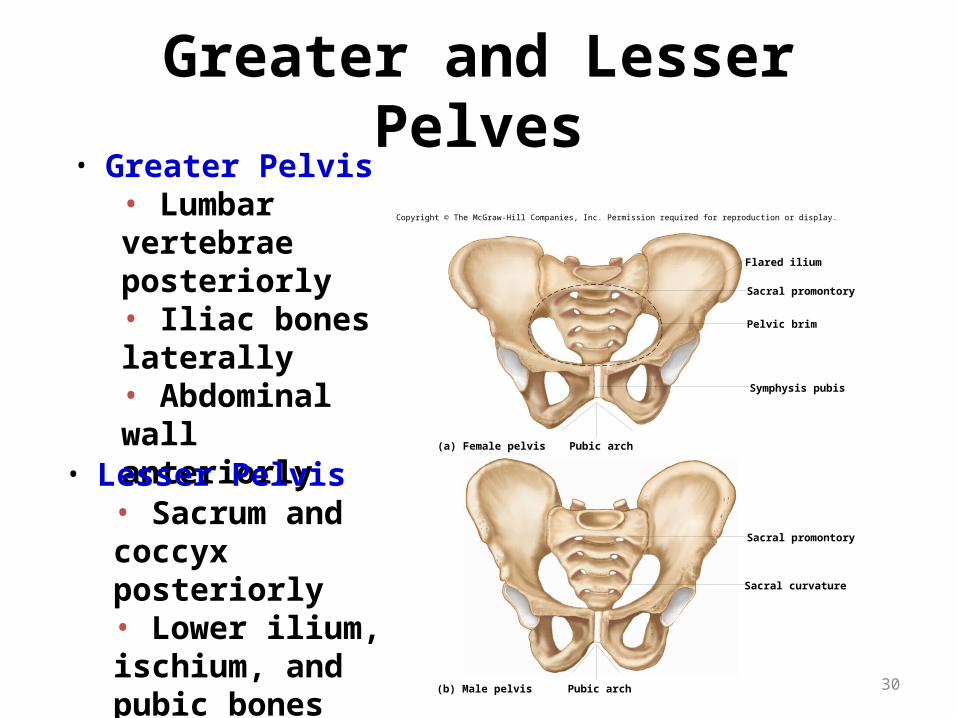
Greater and Lesser Pelves• Greater Pelvis
• Lumbar vertebrae posteriorly• Iliac bones laterally• Abdominal wall anteriorly
• Lesser Pelvis• Sacrum and coccyx posteriorly• Lower ilium, ischium, and pubic bones laterally and anteriorly
Sacral promontory
Flared ilium
Pelvic brim
Symphysis pubis
Pubic arch
Pubic arch
(a) Female pelvis
(b) Male pelvis
Sacral promontory
Sacral curvature
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
31
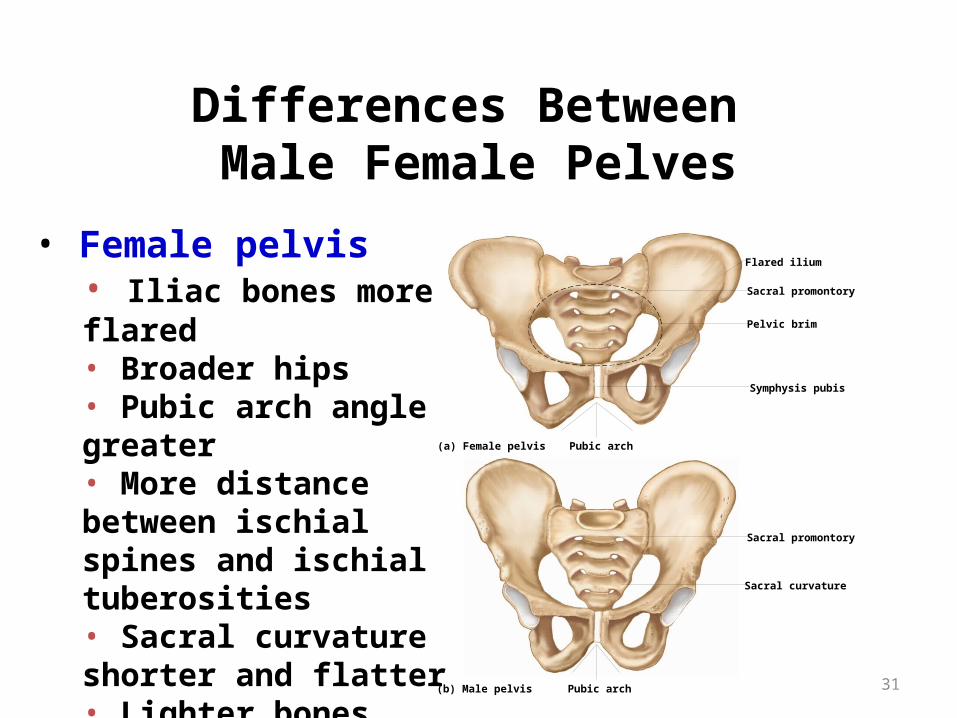
Differences Between Male Female Pelves
• Female pelvis• Iliac bones more flared• Broader hips• Pubic arch angle greater• More distance between ischial spines and ischial tuberosities• Sacral curvature shorter and flatter• Lighter bones
Sacral promontory
Flared ilium
Pelvic brim
Symphysis pubis
Pubic arch
Pubic arch
(a) Female pelvis
(b) Male pelvis
Sacral promontory
Sacral curvature

32
Lower Limb
• Femur
• Patella
• Tibia
• Fibula
• Tarsals
• Metatarsals
• Phalanges Metatarsals
Fibula
Tibia
Tibia
Patella
Femur
Fibula
(c) Lateral view
Fibula
Tibia
Lateralcondyle
(d) Posterior view
(b)
Medialcondyle
Femur
Tarsals
Phalanges
Femur
Patella
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

Femur
• Longest bone of body• Head• Fovea capitis• Neck• Greater trochanter• Lesser trochanter• Linea aspera• Condyles• Epicondyles
Neck Head
Fovea capitis
(a) (b)
Lateralcondyle
Medialcondyle
Intercondylarfossa
Medialepicondyle
Patellarsurface
Lateralepicondyle
Greatertrochanter Gluteal
tuberosityLessertrochanter
Lineaaspera
34
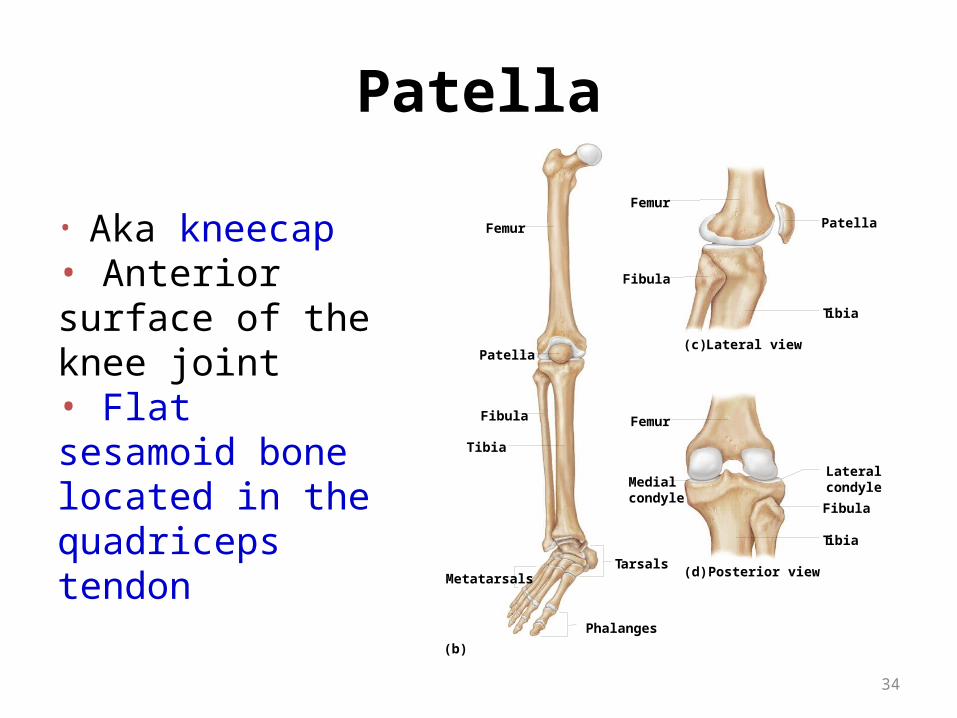
Patella
• Aka kneecap• Anterior surface of the knee joint• Flat sesamoid bone located in the quadriceps tendon
Metatarsals
Fibula
Tibia
Tibia
Patella
Femur
Fibula
(c) Lateral view
Fibula
Tibia
Lateralcondyle
(d) Posterior view
(b)
Medialcondyle
Femur
T arsals
Phalanges
Femur
Patella
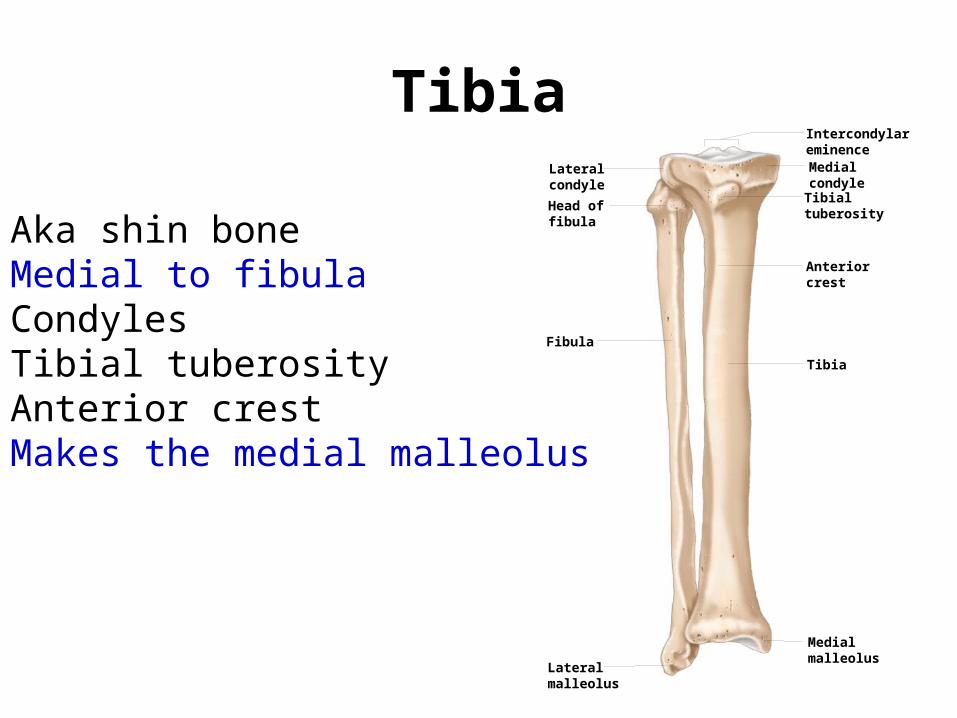
Tibia
• Aka shin bone• Medial to fibula• Condyles• Tibial tuberosity• Anterior crest• Makes the medial malleolus
Tibia
Fibula
Medialmalleolus
Tibialtuberosity
Anteriorcrest
Medialcondyle
Intercondylareminence
Lateralmalleolus
Lateralcondyle
Head offibula
Fibula
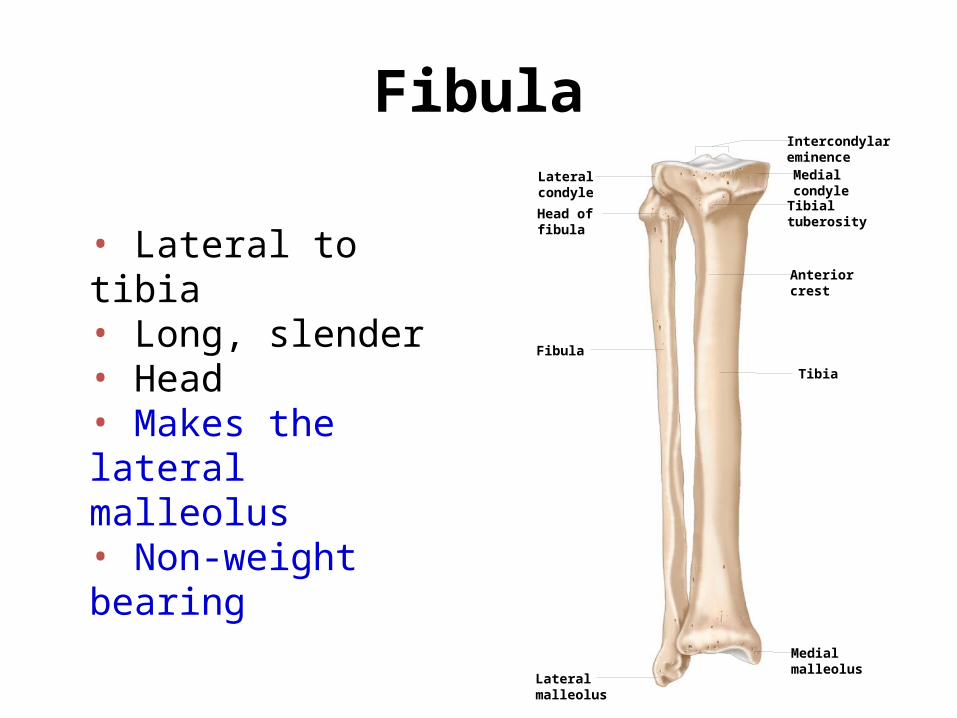
• Lateral to tibia• Long, slender• Head• Makes the lateral malleolus• Non-weight bearing
Tibia
Fibula
Medialmalleolus
Tibialtuberosity
Anteriorcrest
Medialcondyle
Intercondylareminence
Lateralmalleolus
Lateralcondyle
Head offibula
37
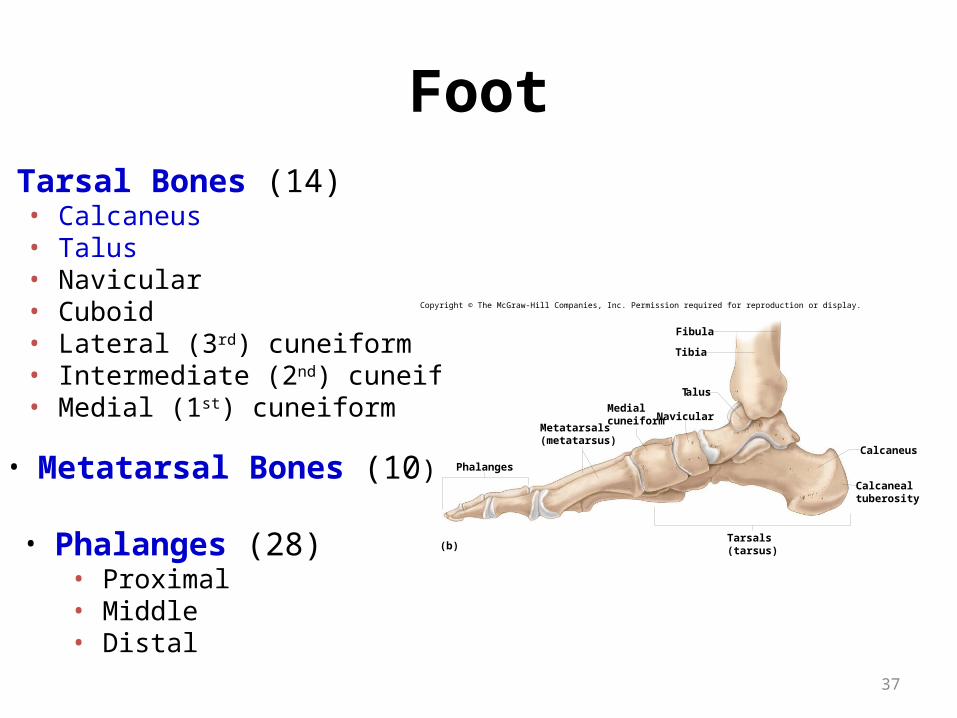
Foot• Tarsal Bones (14)
• Calcaneus• Talus• Navicular• Cuboid• Lateral (3rd) cuneiform• Intermediate (2nd) cuneiform• Medial (1st) cuneiform
• Metatarsal Bones (10)
• Phalanges (28)• Proximal• Middle• Distal
(b)
Tibia
Fibula
Talus
Navicular
Phalanges
Calcaneus
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Medialcuneiform
Metatarsals(metatarsus)
Tarsals(tarsus)
Calcanealtuberosity
骨骼的组织学

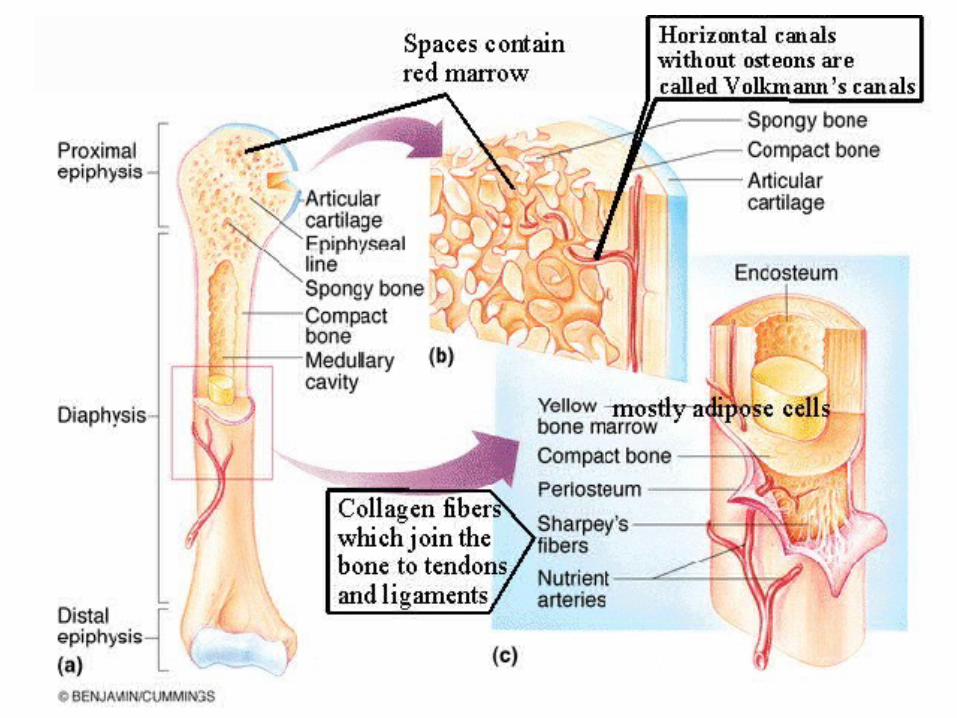
Long boneDiaphysis: long shaft of boneEpiphysis: ends of boneEpiphyseal plate: growth plateMetaphysis: b/w epiphysis and diaphysisArticular cartilage: covers epiphysisPeriosteum: bone covering (pain sensitive)Sharpey’s fibers: periosteum attaches to underlying
boneMedullary cavity: Hollow chamber in bone
- red marrow produces blood cells- yellow marrow is adipose.
Endosteum: thin layer lining the medullary cavity
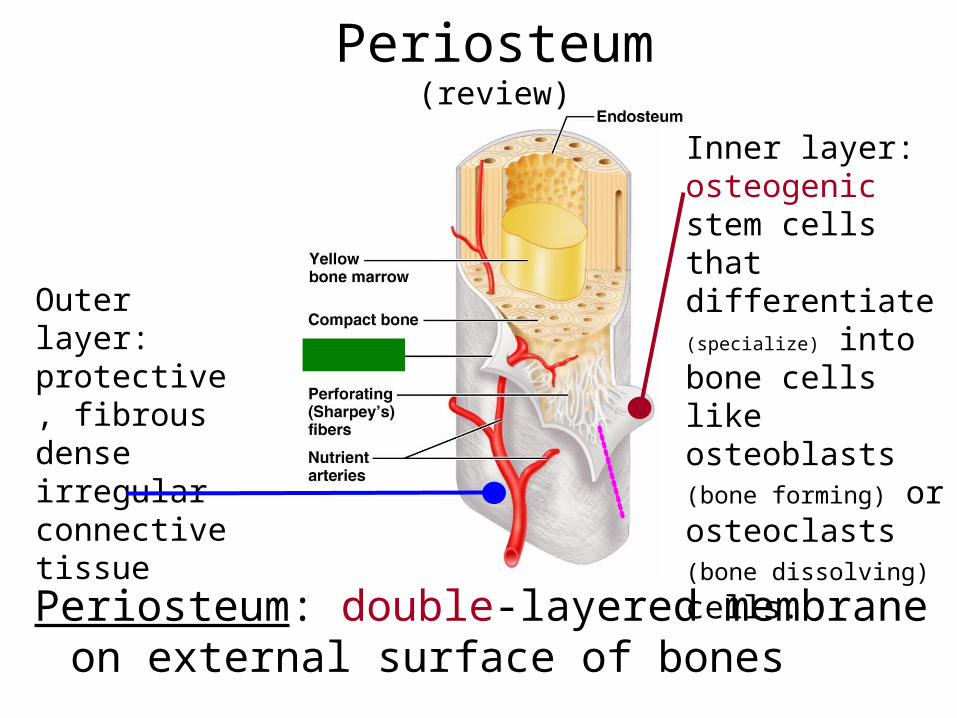
Periosteum(review)
Periosteum: double-layered membrane on external surface of bones
Inner layer:osteogenic stem cells that differentiate (specialize) into bone cells like osteoblasts (bone
forming) or osteoclasts (bone
dissolving) cells.
Outer layer: protective, fibrous dense irregular connective tissue
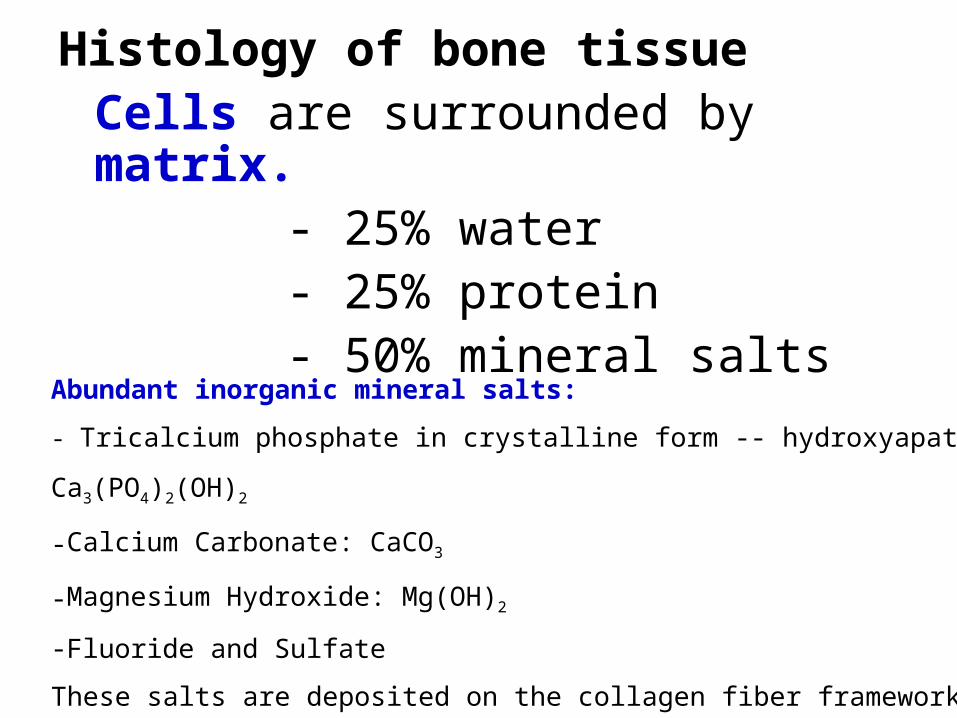
Histology of bone tissueCells are surrounded by matrix.
- 25% water- 25% protein- 50% mineral salts
Abundant inorganic mineral salts:
- Tricalcium phosphate in crystalline form -- hydroxyapatite Ca3(PO4)2(OH)2
-Calcium Carbonate: CaCO3
-Magnesium Hydroxide: Mg(OH)2
-Fluoride and Sulfate
These salts are deposited on the collagen fiber framework (tensile strength)
and crystallization occurs.- calcification or mineralization
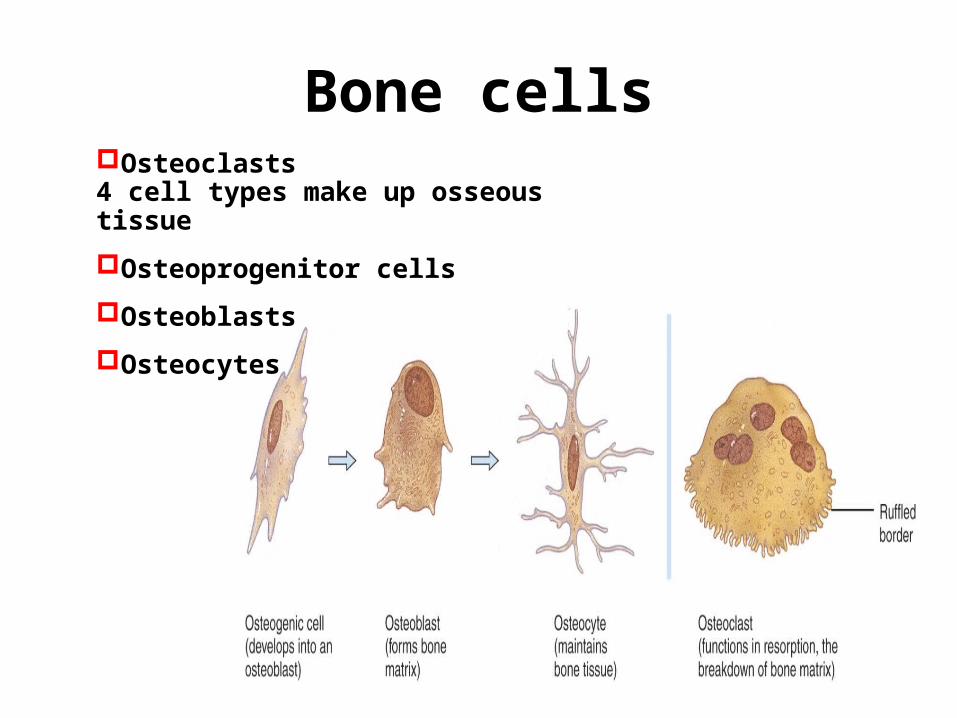
Bone cellsOsteoclasts4 cell types make up osseous tissue
Osteoprogenitor cells
Osteoblasts
Osteocytes
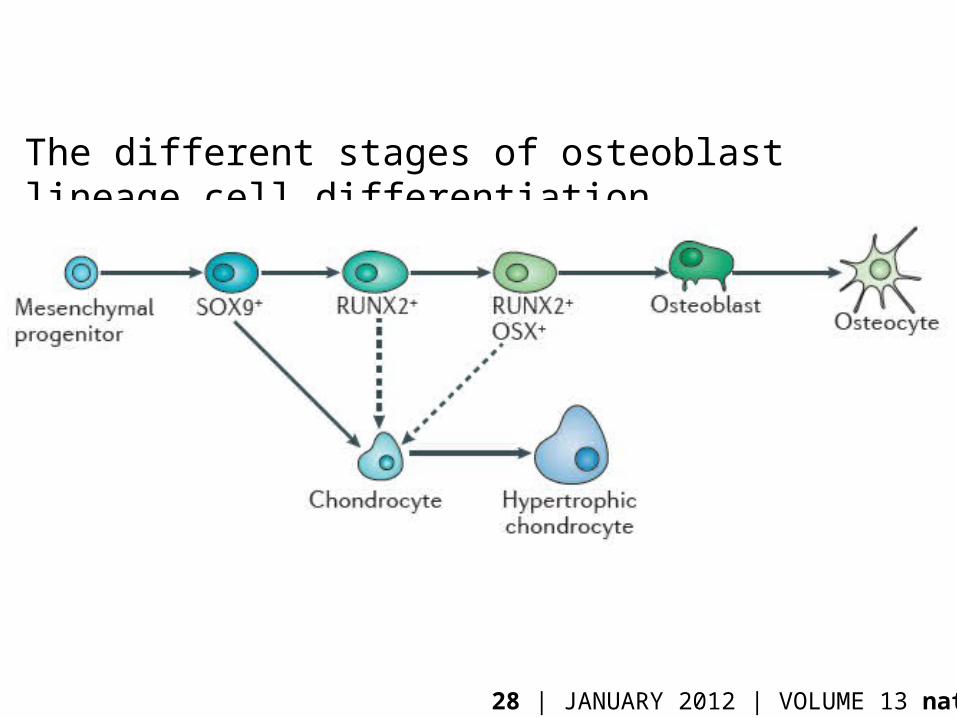
The different stages of osteoblast lineage cell differentiation
28 | JANUARY 2012 | VOLUME 13 nature
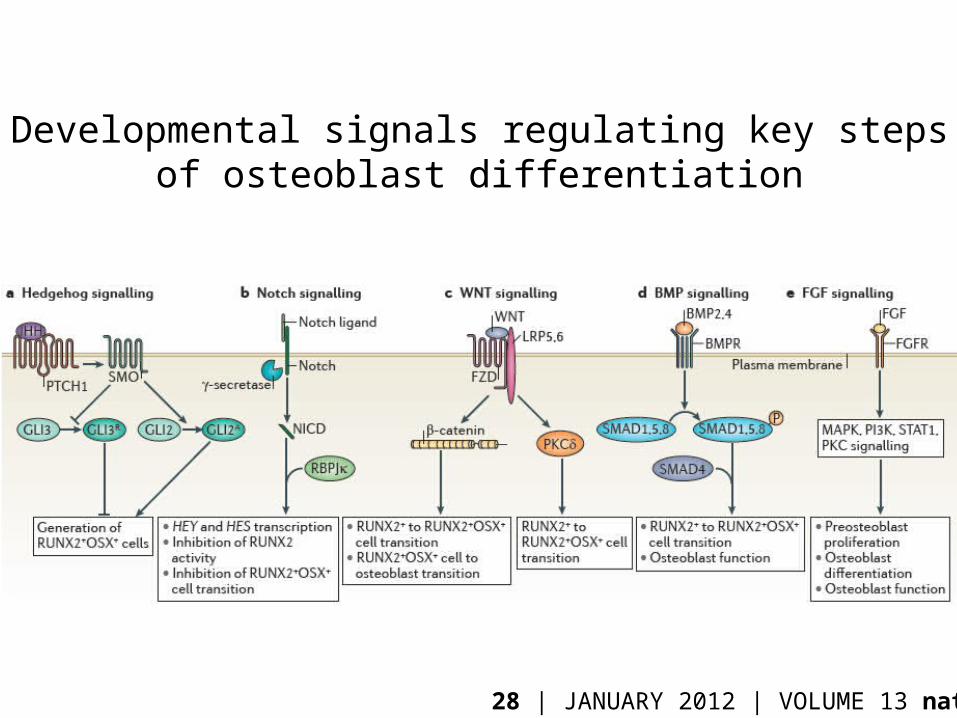
Developmental signals regulating key steps of osteoblast differentiation
28 | JANUARY 2012 | VOLUME 13 nature
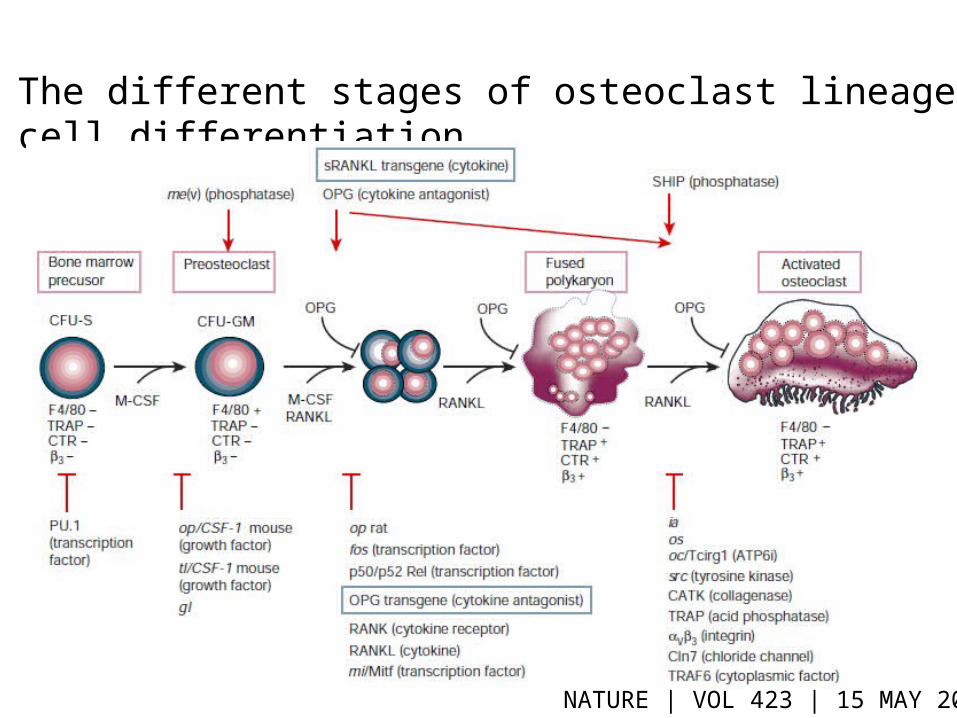
The different stages of osteoclast lineage cell differentiation
NATURE | VOL 423 | 15 MAY 2003
6-47
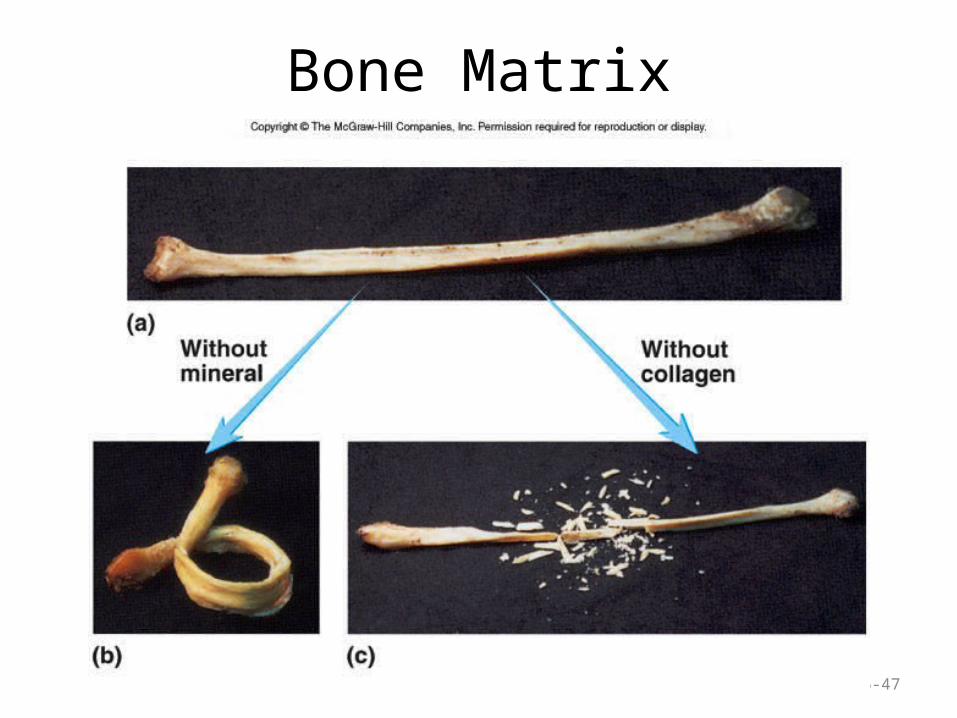
Bone Matrix
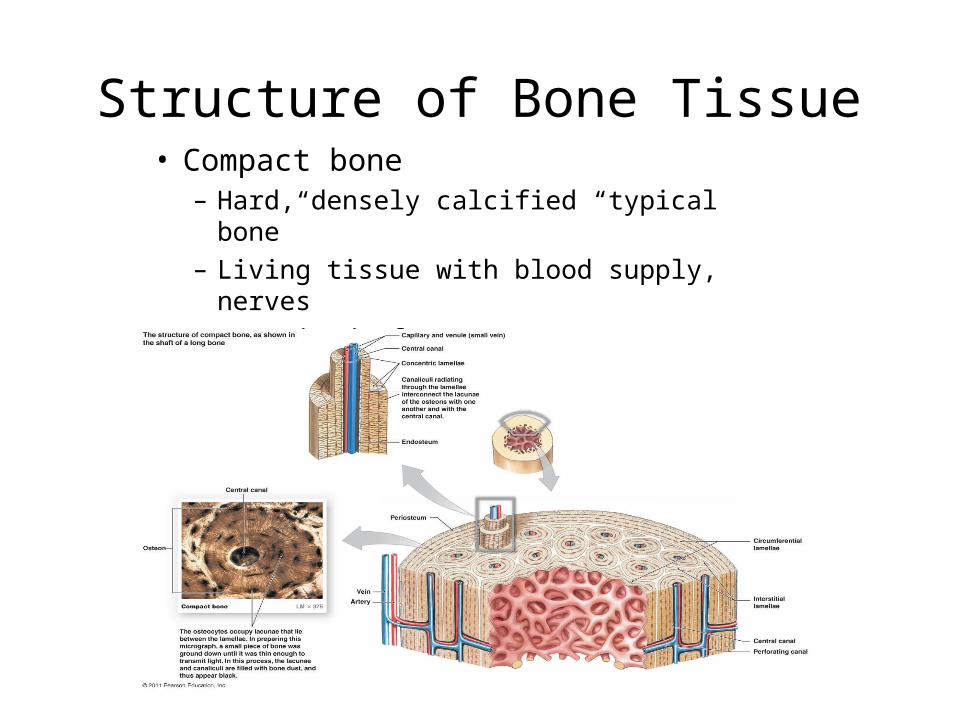
Structure of Bone Tissue• Compact bone
– Hard, densely calcified “typical bone”– Living tissue with blood supply, nerves– Organized of osteons
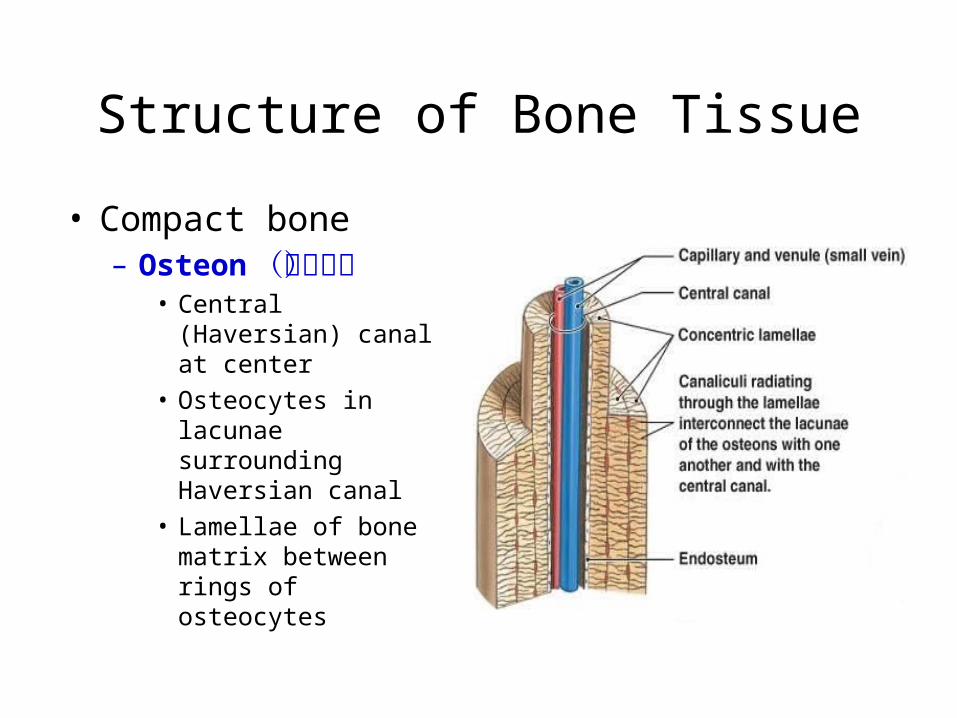
Structure of Bone Tissue
• Compact bone– Osteon(骨单元)
• Central (Haversian) canal at center
• Osteocytes in lacunae surrounding Haversian canal
• Lamellae of bone matrix between rings of osteocytes

6-51
Cancellous Bone
• Consists of trabeculae– Oriented along lines of
stress
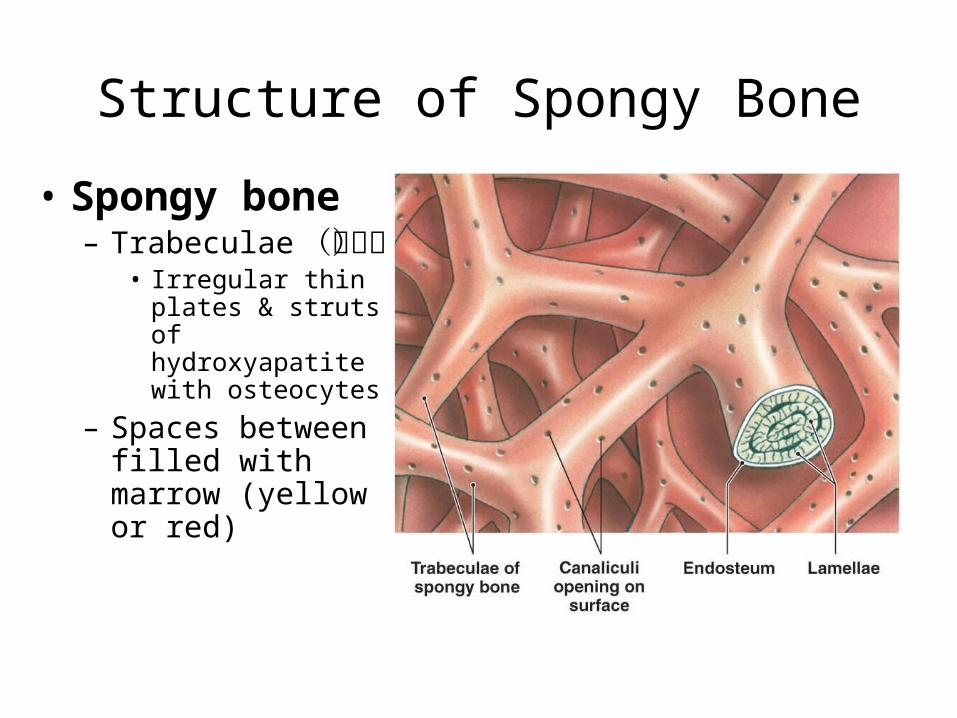
Structure of Spongy Bone
• Spongy bone– Trabeculae (小
梁)• Irregular thin plates
& struts of hydroxyapatite with osteocytes
– Spaces between filled with marrow (yellow or red)
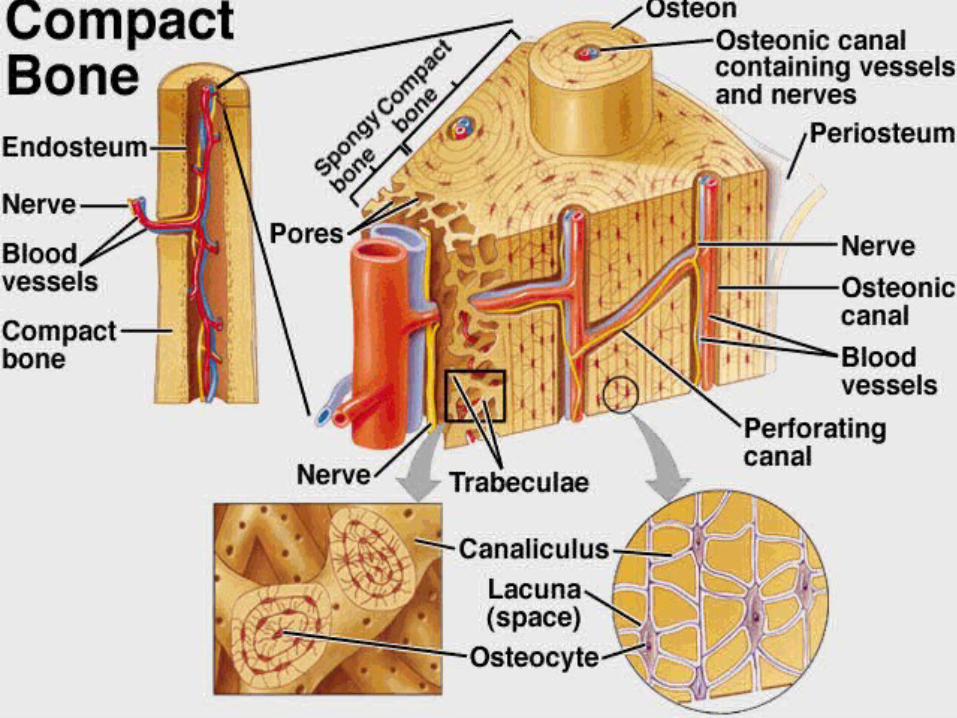
Compact vs. spongy bone
Compact bone– External layer– Arranged in osteons– Lamellae are found
around periphery and between osteons
– Central canals connected to each other by perforating canals
Spongy bone– No osteons– Arranged in trabeculae– Major type of tisse in
short, flat, irregular bones
– Much lighter than compact bone
– Supports red bone marrow

骨骼的发育
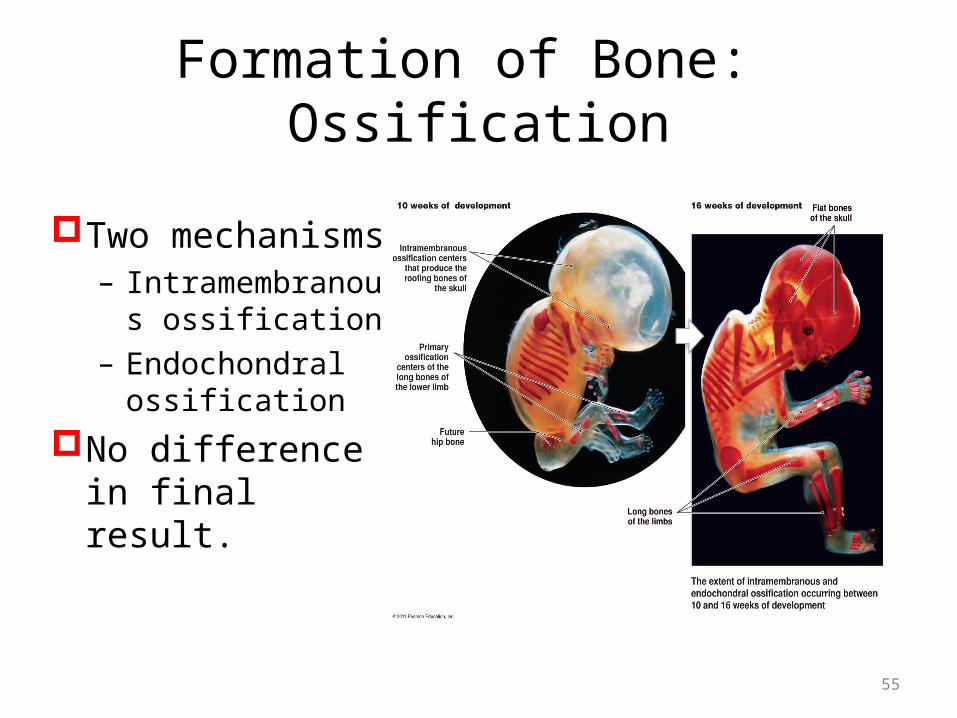
Formation of Bone: Ossification
Two mechanisms– Intramembranous
ossification– Endochondral
ossificationNo difference in
final result.
55
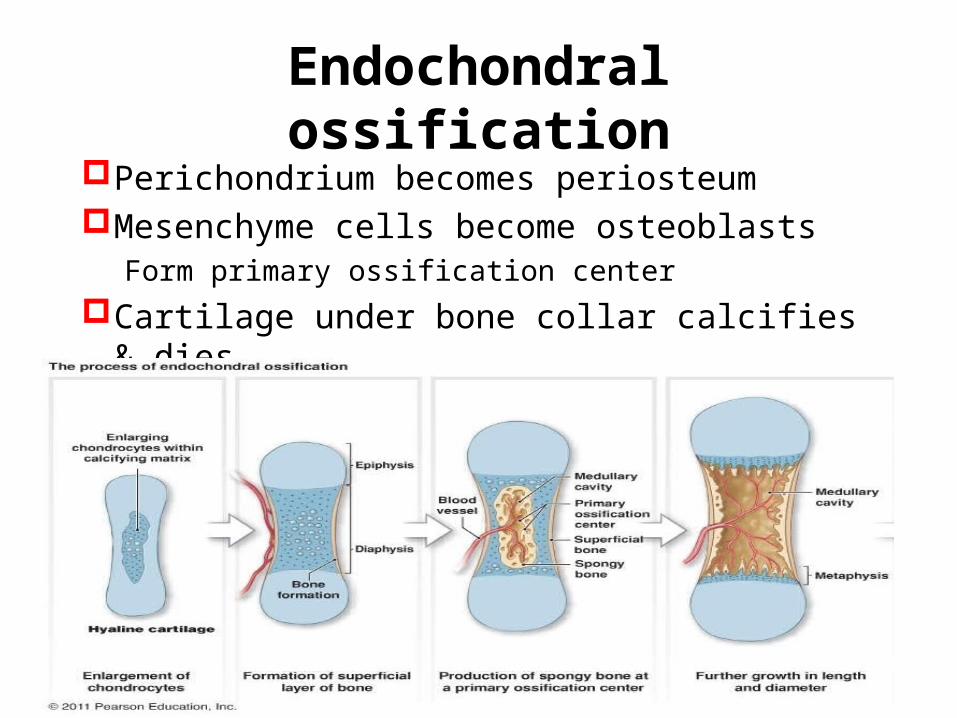
Endochondral ossificationPerichondrium becomes periosteumMesenchyme cells become osteoblasts
Form primary ossification centerCartilage under bone collar calcifies & dies
57
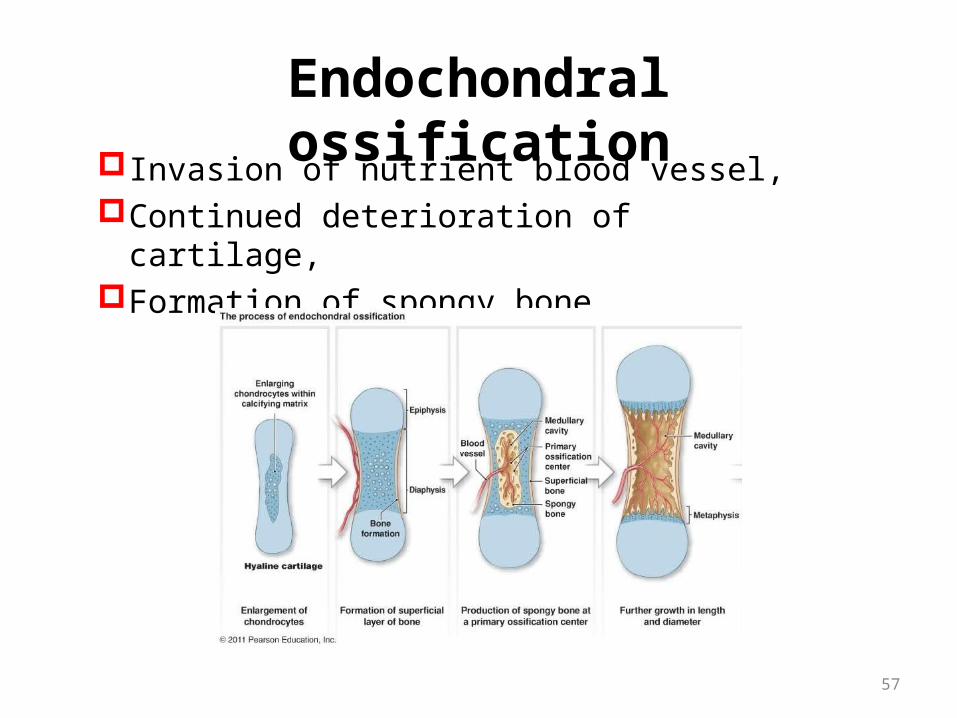
Endochondral ossificationInvasion of nutrient blood vessel,Continued deterioration of cartilage,Formation of spongy bone
58
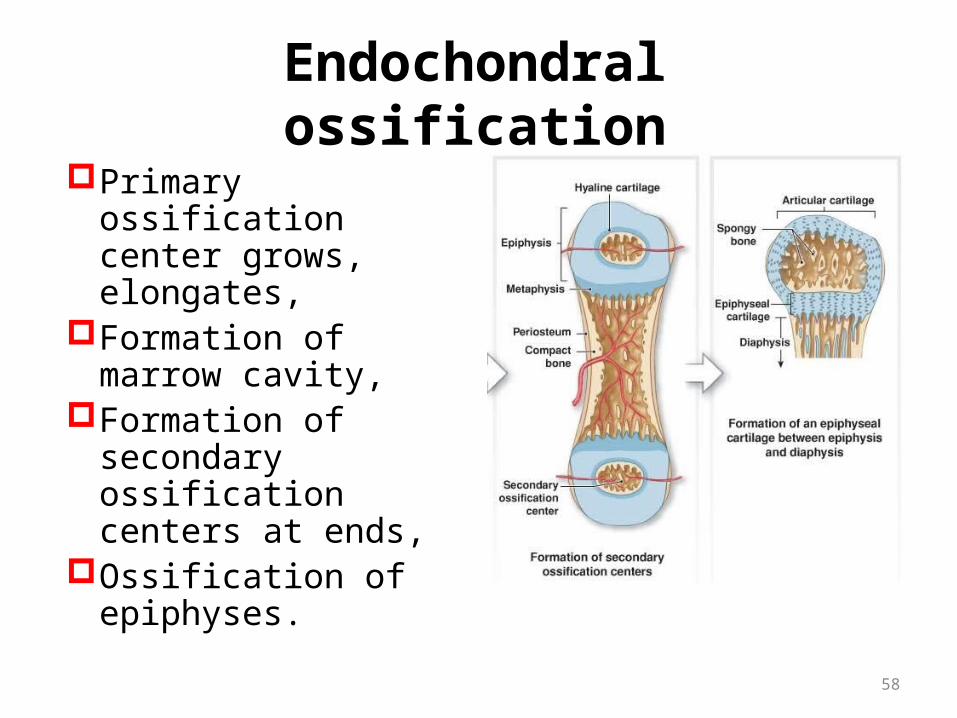
Endochondral ossificationPrimary ossification
center grows, elongates,
Formation of marrow cavity,
Formation of secondary ossification centers at ends,
Ossification of epiphyses.
Growth in Bone Length
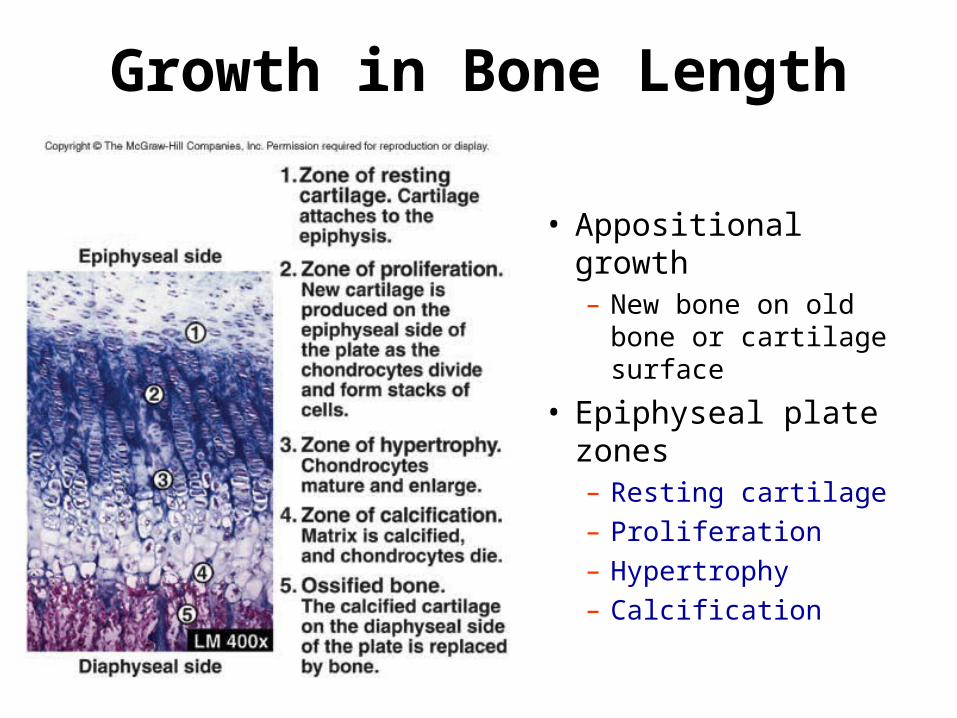
• Appositional growth– New bone on old bone
or cartilage surface
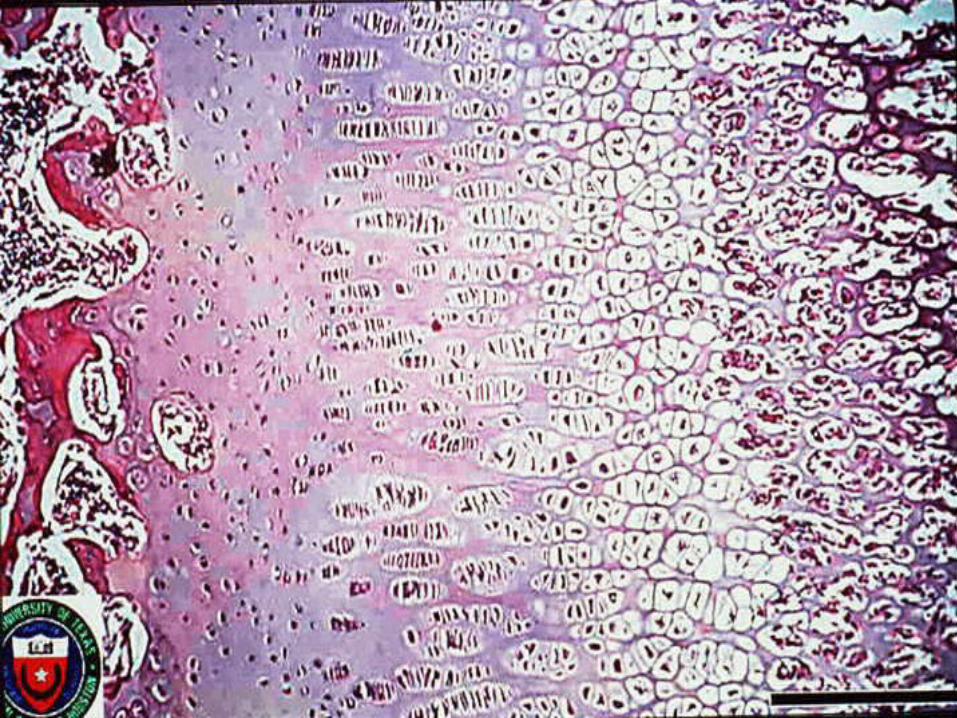
• Epiphyseal plate zones– Resting cartilage– Proliferation– Hypertrophy– Calcification
Physiology of bone growth:- epiphyseal plate (bone length)
- 4 zones of bone growth under hGH.1- Zone of resting cartilage:
- no bone growth- located near the epiphyseal plate- scattered chondrocytes- anchors plate to bone
2- Zone of proliferating cartilage- chondrocytes stacked like coins- chondrocytes divide
3- Zone of hypertrophic (maturing) cartilage- large chondrocytes arranged in columns- lengthwise expansion of epiphyseal plate
4- Zone of calcified cartilage- few cell layers thick- occupied by osteoblasts and osteoclasts and capillaries from the diaphysis- cells lay down bone- dead chondrocytes surrounded by a calcified matrix.
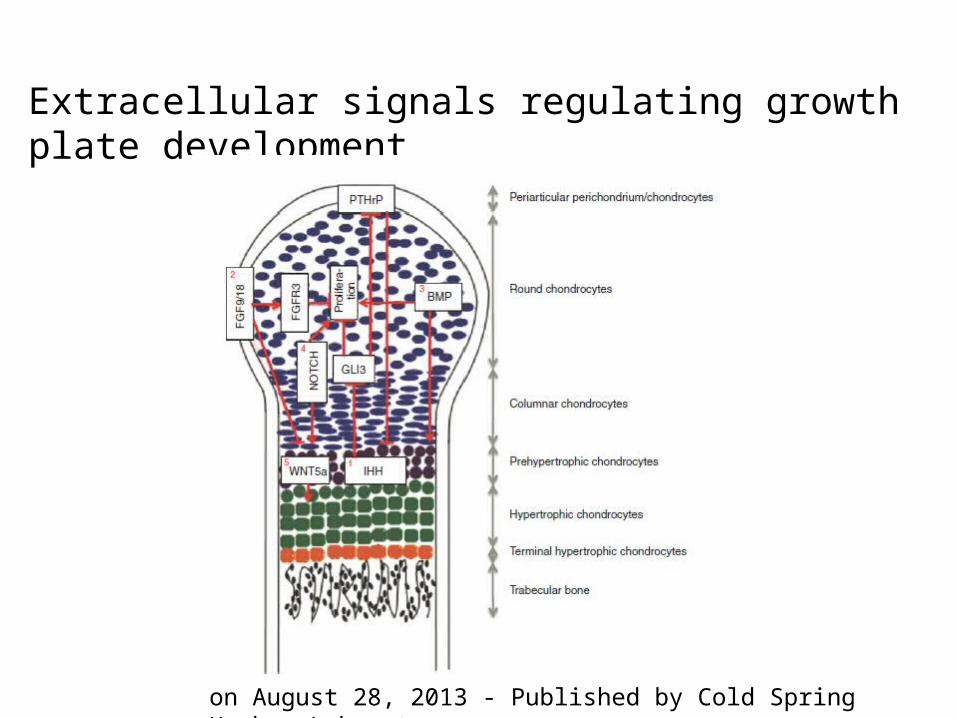
Extracellular signals regulating growth plate development
on August 28, 2013 - Published by Cold Spring Harbor Laboratory
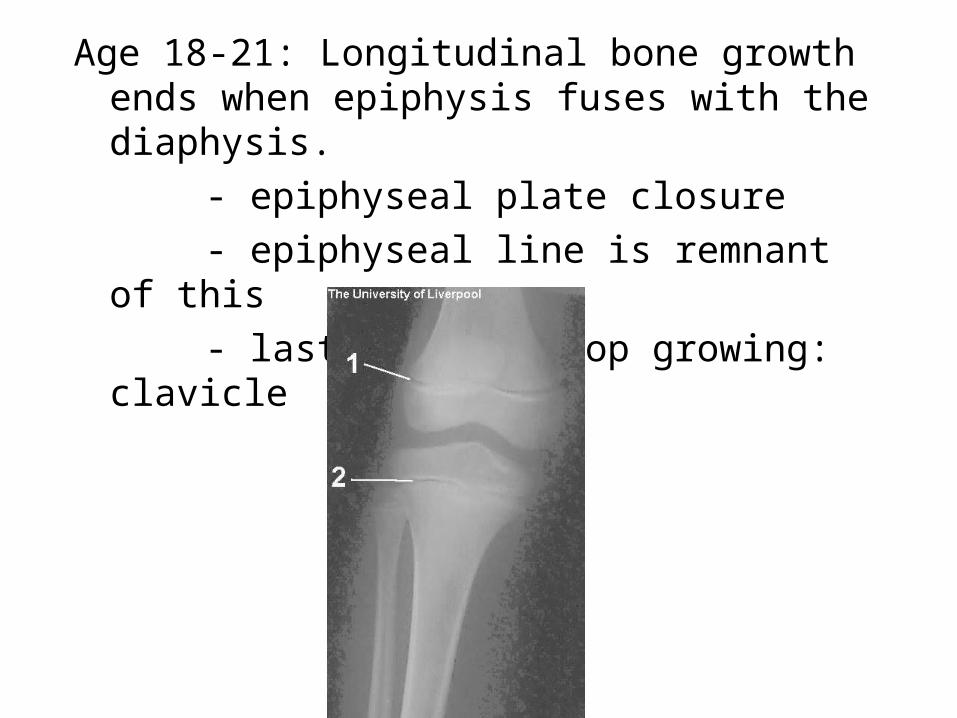
Age 18-21: Longitudinal bone growth ends when epiphysis fuses with the diaphysis.
- epiphyseal plate closure- epiphyseal line is remnant of this- last bone to stop growing: clavicle
65
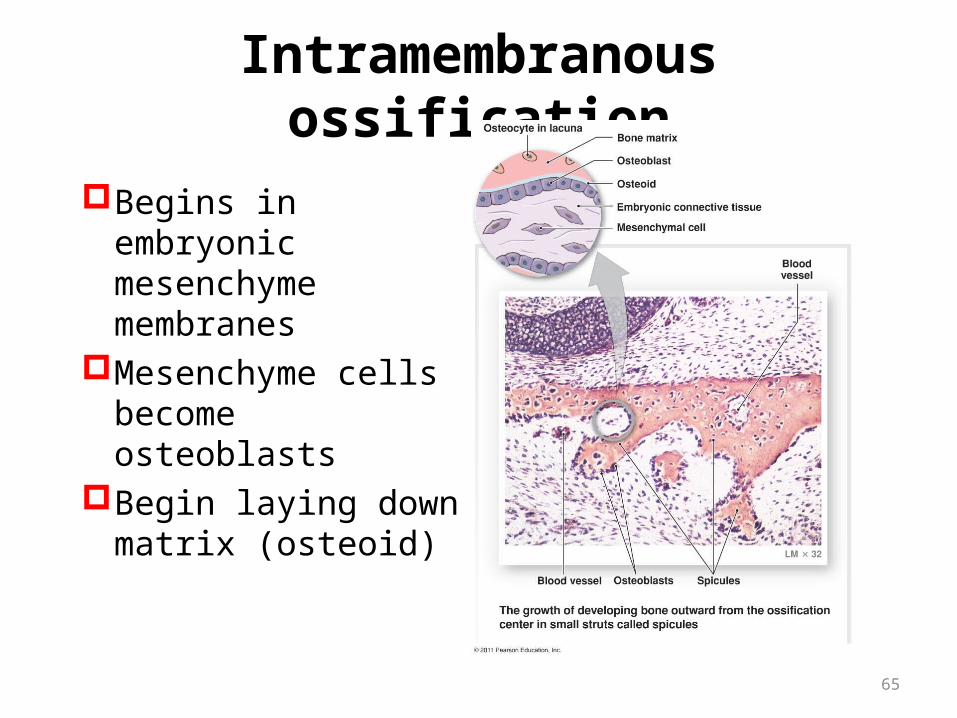
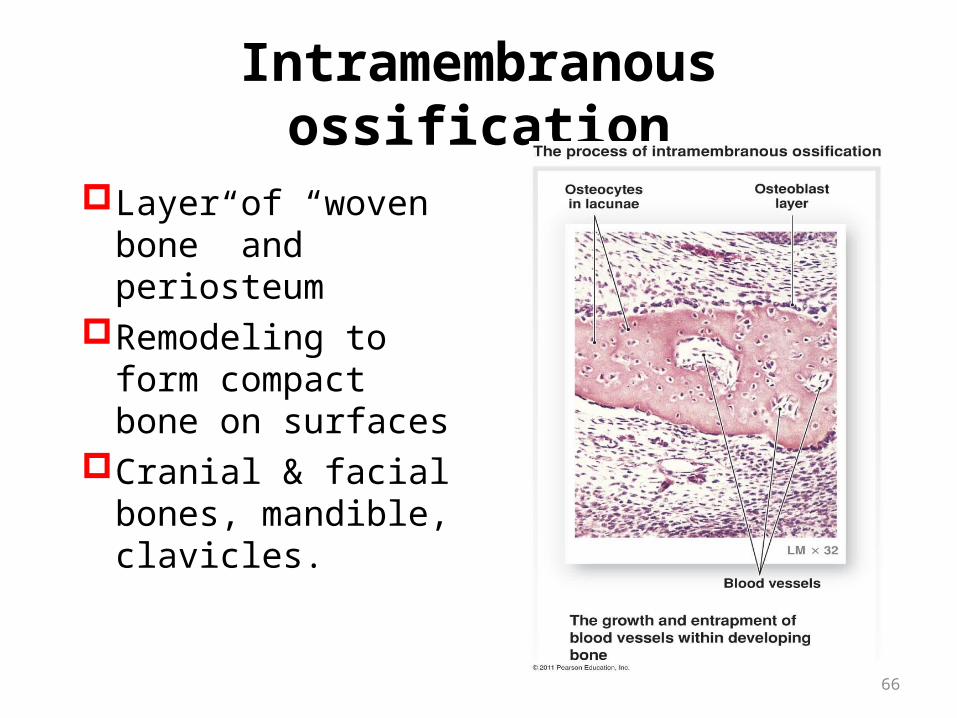
Intramembranous ossification
Begins in embryonic mesenchyme membranes
Mesenchyme cells become osteoblasts
Begin laying down matrix (osteoid)
66
Intramembranous ossification
Layer of “woven bone” and periosteum
Remodeling to form compact bone on surfaces
Cranial & facial bones, mandible, clavicles.
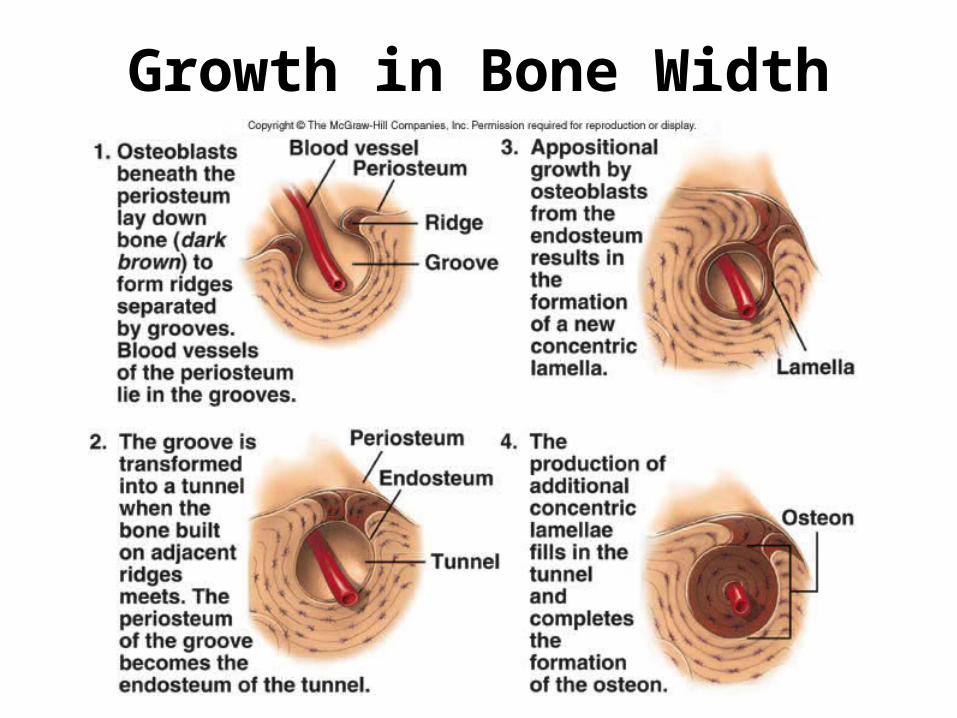
Growth in Bone Width

Osteoclast and osteoblast lineage cells
28 | JANUARY 2012 | VOLUME 13 nature
骨骼的维持
Bone Remodeling
Wolff’s Law
bone is laid down where needed and resorbed where not needed
shape of bone reflects its function tennis arm of pro tennis players have cortical
thicknesses 35% greater than contralateral arm (Keller & Spengler, 1989)
osteoclasts resorb or take-up boneosteoblasts lay down new bone
Bone is Dynamic!Bone is constantly remodeling and recycling
Coupled process between:Bone deposition (by osteoblasts)Bone destruction/resorption (by osteoclasts)
5-7% of bone mass recycled weekly All spongy bone replaced every 3-4 years. All compact bone replaced every 10 years.
Prevents mineral salts from crystallizing; protecting against brittle bones and fractures
Bone Resorption
Osteoclasts are related to macrophages:
secrete lysosomal enzymes and HCl acid
Move along surface of bone, dissolving grooves into
bone with acid and enzymes
Dissolved material passed through osteoclasts and
into bloodstream for reuse by the body
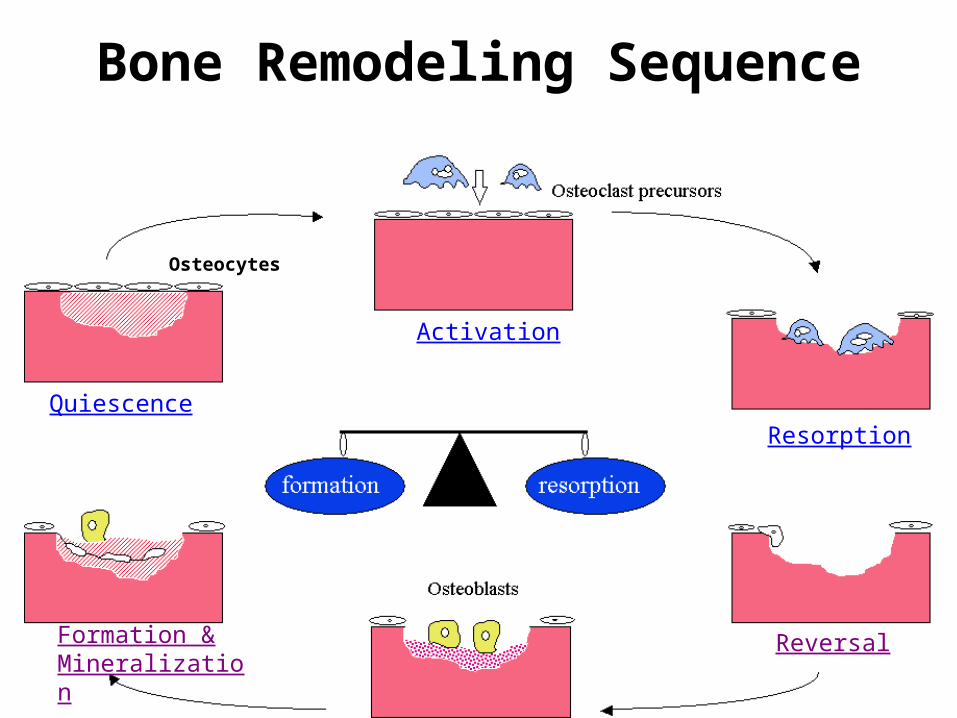
Bone Remodeling Sequence
Activation
Resorption
Reversal
Quiescence
Formation & Mineralization
Osteocytes

Age, Bone Mass and Gender
From: Biomechanics of Musculoskeletal Injury, Whiting and Zernicke
Bon
e M
ass
(g o
f C
a)
1000 5025 75
500
1000
Age (yr)
Effects of Aging on Skeletal System
• Bone Matrix decreases • Bone Mass decreases• Increased bone fractures• Bone loss causes deformity, loss of height,
pain, stiffness– Stooped posture– Loss of teeth

Changes in Bone Over TimeOlder Adults
• 30 yrs males and 40 yrs females– BMD peaks (Frost, 1985; Oyster et al., 1984)
– decrease BMD, diameter and mineralization after this
• activity slows aging process
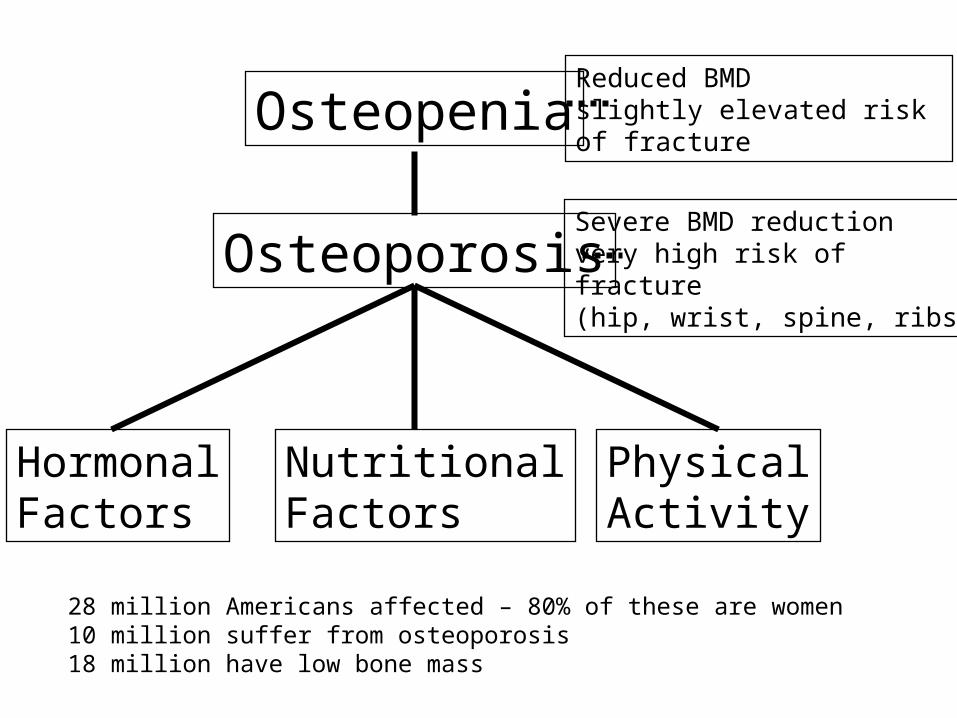
Osteoporosis
HormonalFactors
NutritionalFactors
PhysicalActivity
OsteopeniaReduced BMDslightly elevated risk of fracture
Severe BMD reductionvery high risk offracture(hip, wrist, spine, ribs)
28 million Americans affected – 80% of these are women10 million suffer from osteoporosis18 million have low bone mass
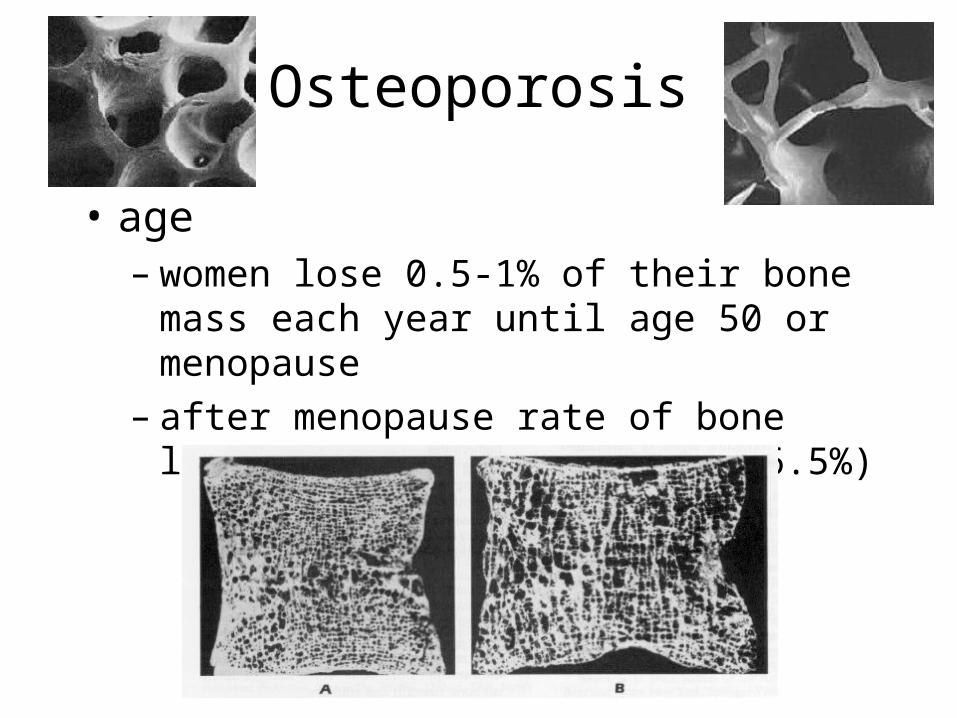
Osteoporosis
• age– women lose 0.5-1% of their bone mass
each year until age 50 or menopause– after menopause rate of bone loss
increases (as high as 6.5%)
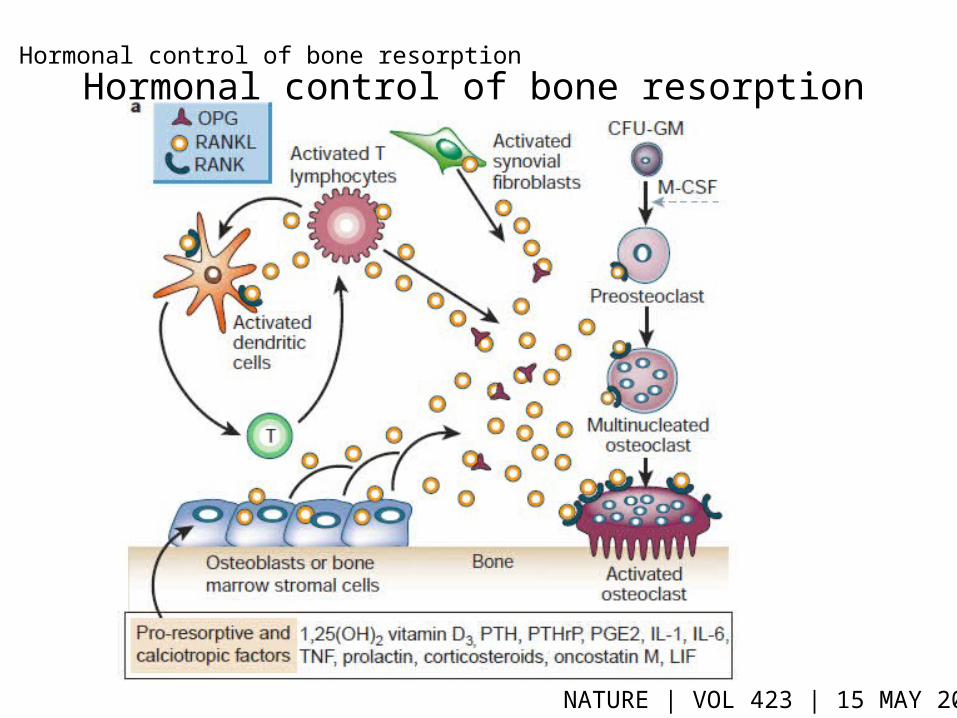
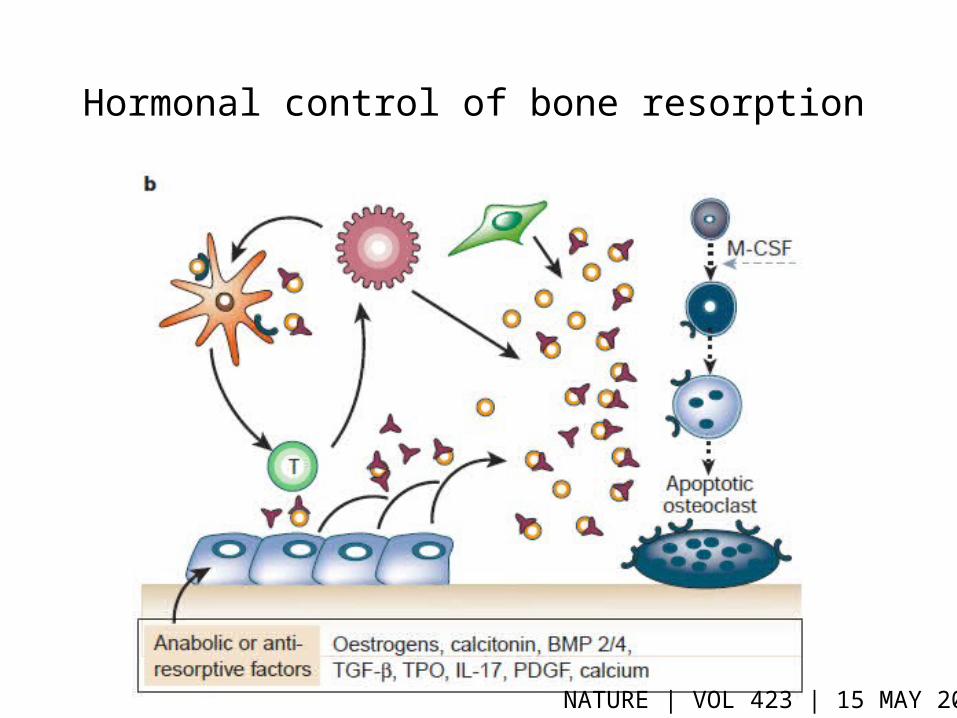
Hormonal control of bone resorption
Hormonal control of bone resorption
NATURE | VOL 423 | 15 MAY 2003
Hormonal control of bone resorption
NATURE | VOL 423 | 15 MAY 2003
骨骼的生物力学
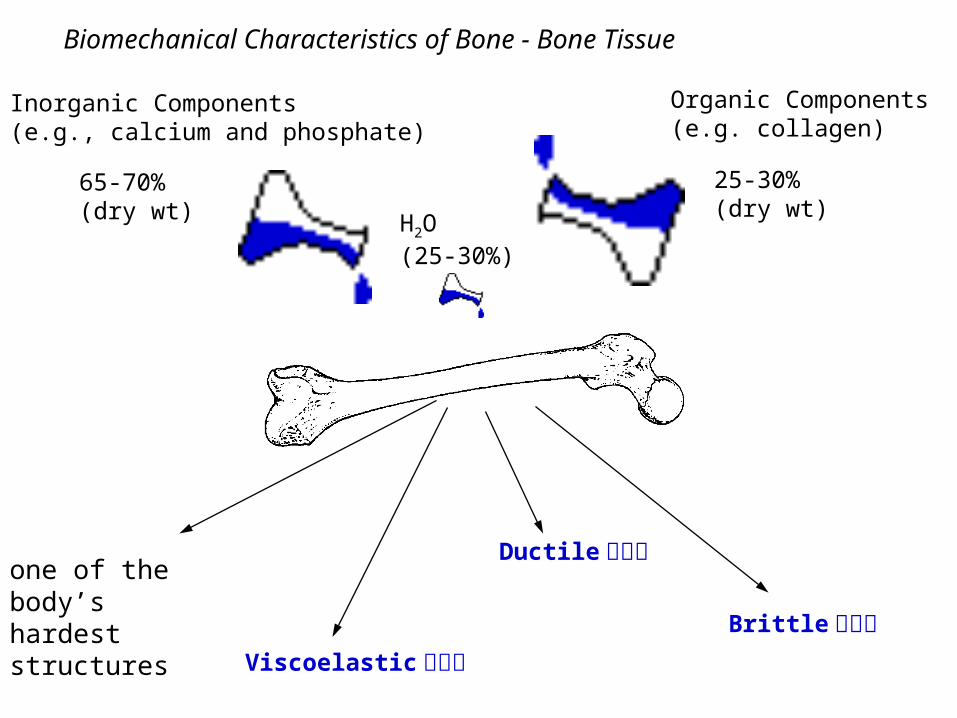
Organic Components(e.g. collagen)
Inorganic Components(e.g., calcium and phosphate)
65-70%(dry wt) H2O
(25-30%)
one of the body’s hardest structures
Viscoelastic 粘弹性
Ductile 延展性
Brittle 易脆性
Biomechanical Characteristics of Bone - Bone Tissue
25-30%(dry wt)

Compression Tension Shear Torsion Bending
Mechanical Loading of Bone
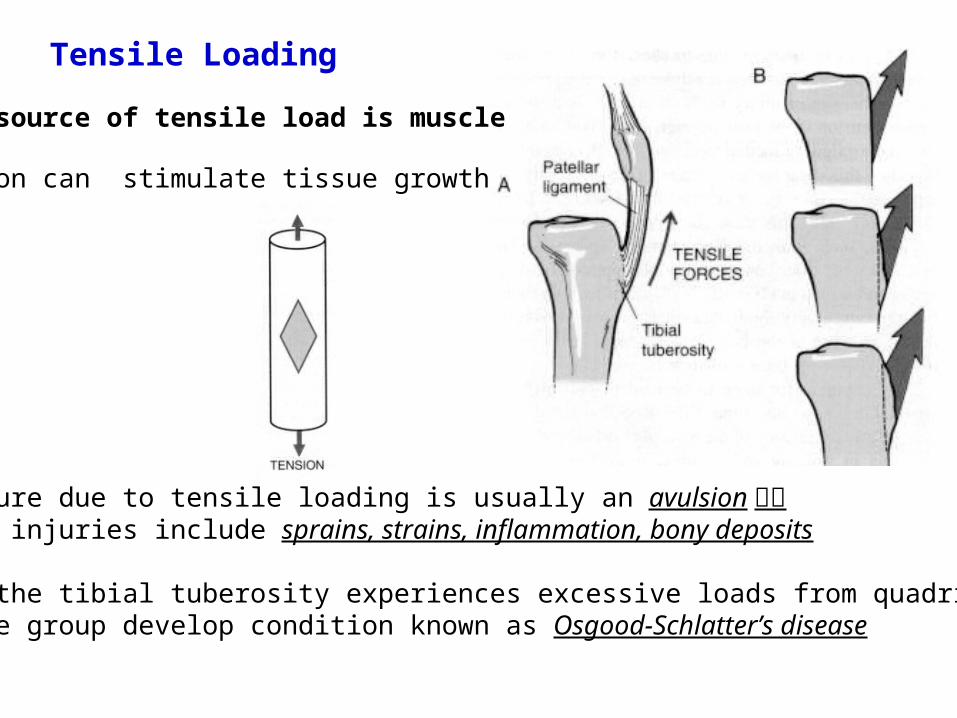
Tensile Loading
Main source of tensile load is muscle
tension can stimulate tissue growth
fracture due to tensile loading is usually an avulsion 撕裂other injuries include sprains, strains, inflammation, bony deposits
when the tibial tuberosity experiences excessive loads from quadriceps muscle group develop condition known as Osgood-Schlatter’s disease
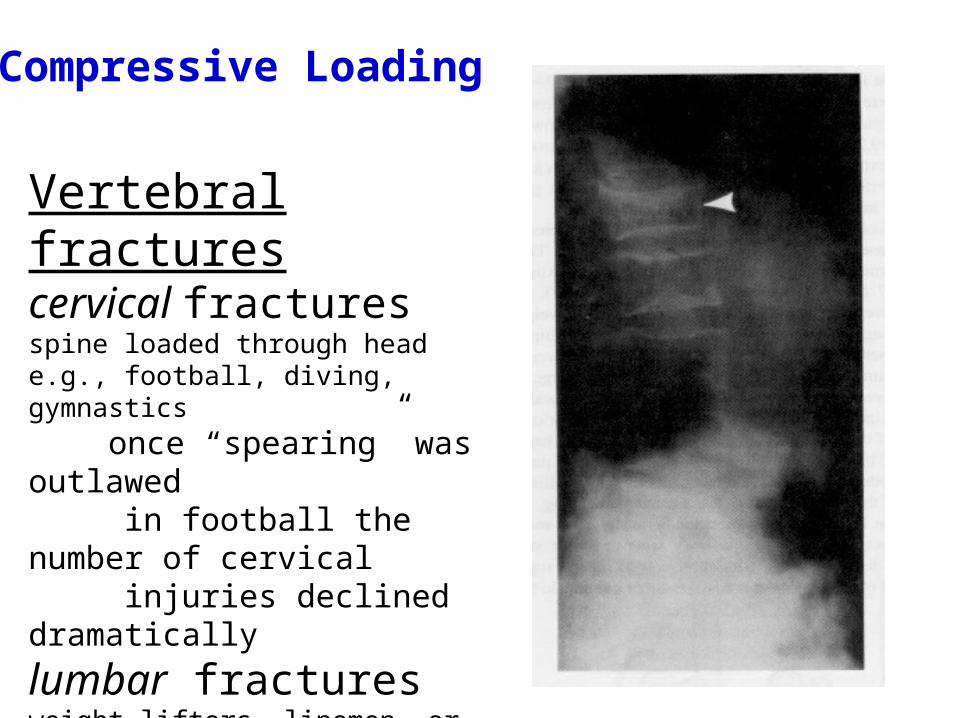
Vertebral fracturescervical fracturesspine loaded through heade.g., football, diving, gymnastics
once “spearing” was outlawed in football the number of cervical injuries declined dramatically
lumbar fracturesweight lifters, linemen, or gymnastsspine is loaded in hyperlordotic(aka swayback) position
Compressive Loading
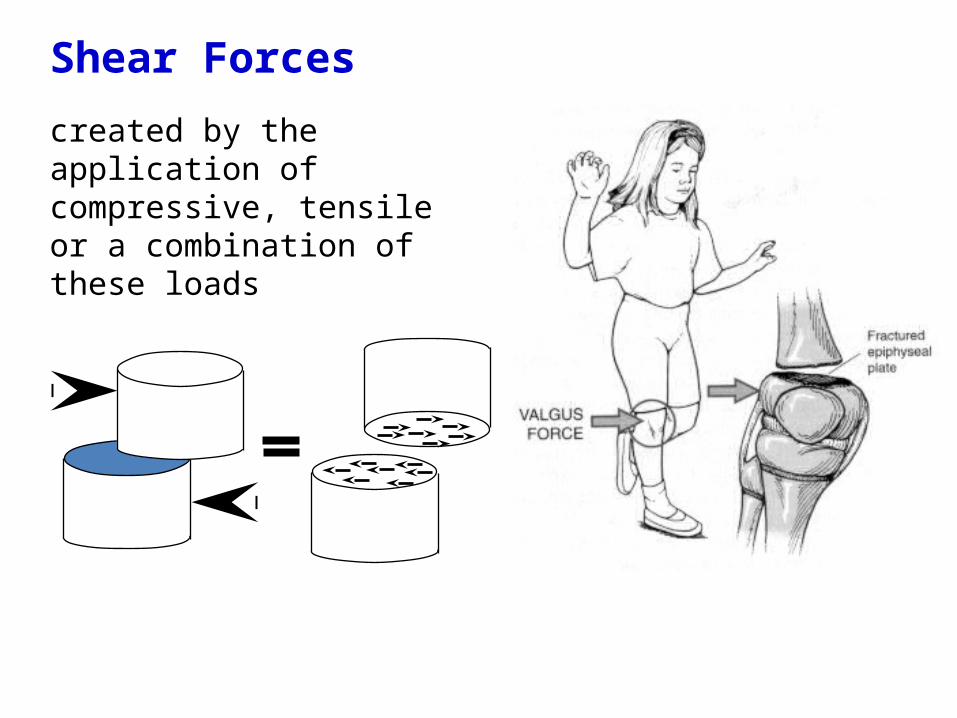
Shear Forces
created by the application of compressive, tensile or a combination of these loads
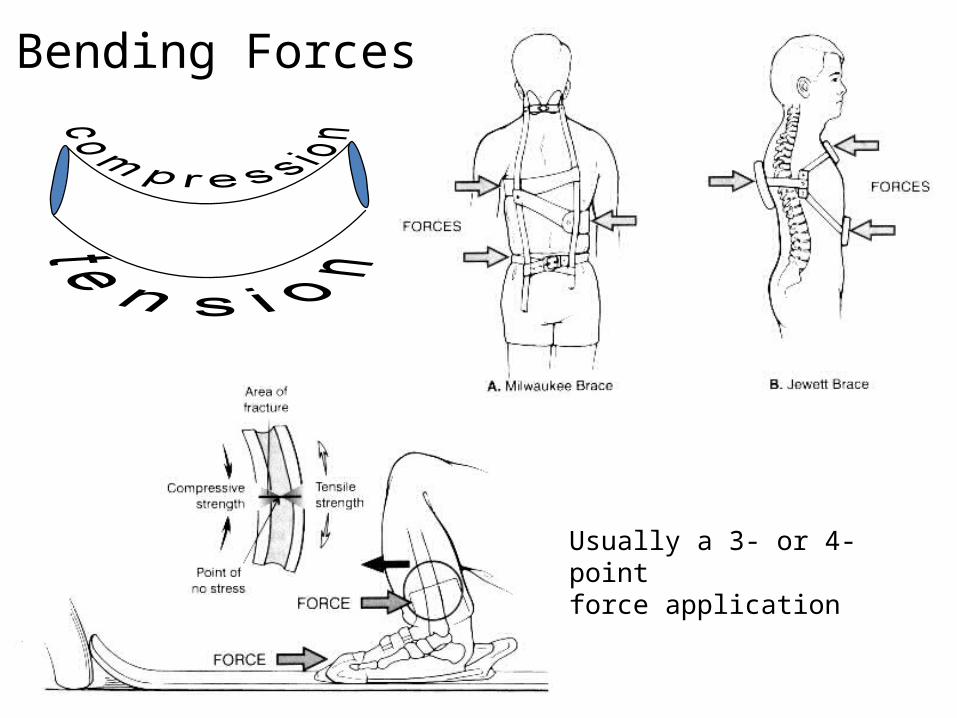
Usually a 3- or 4-pointforce application
Bending Forces
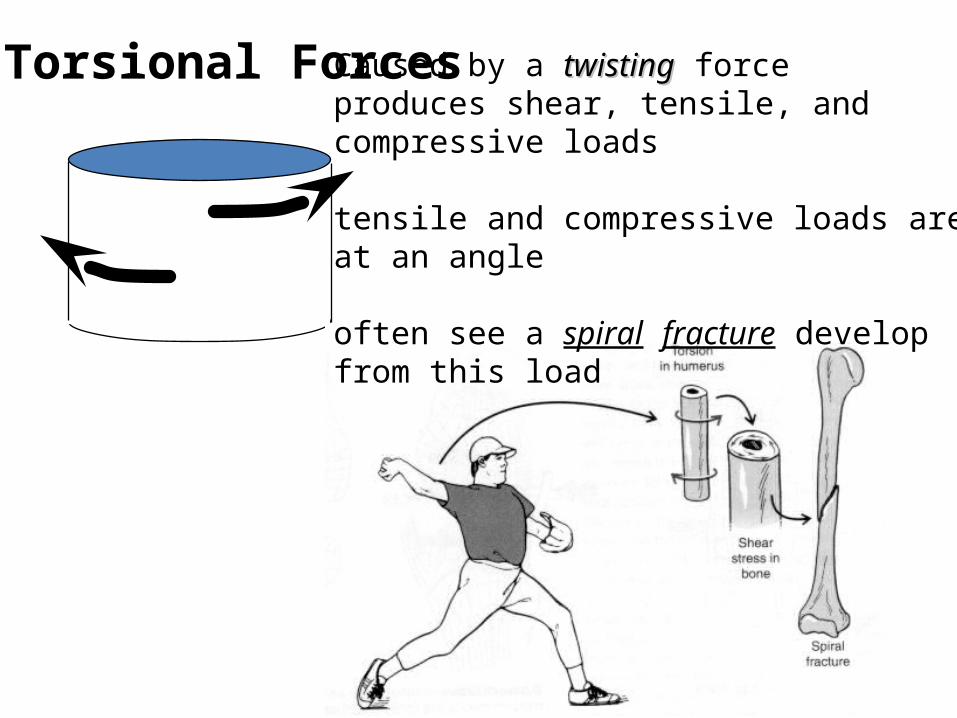
Torsional ForcesCaused by a twistingtwisting forceproduces shear, tensile, and compressive loads
tensile and compressive loads areat an angle
often see a spiral fracture developfrom this load
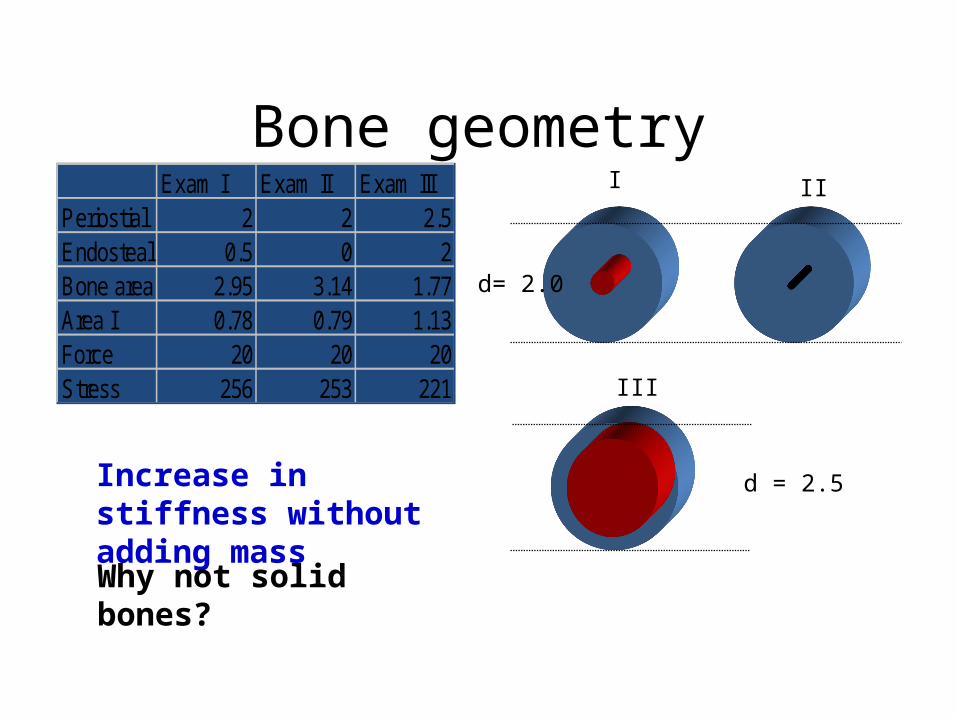
Bone geometry
d= 2.0
d = 2.5
I II
III
Exam I Exam II Exam IIIPeriostial 2 2 2.5Endosteal 0.5 0 2Bone area 2.95 3.14 1.77Area I 0.78 0.79 1.13Force 20 20 20Stress 256 253 221
Increase in stiffness without adding mass
Why not solid bones?
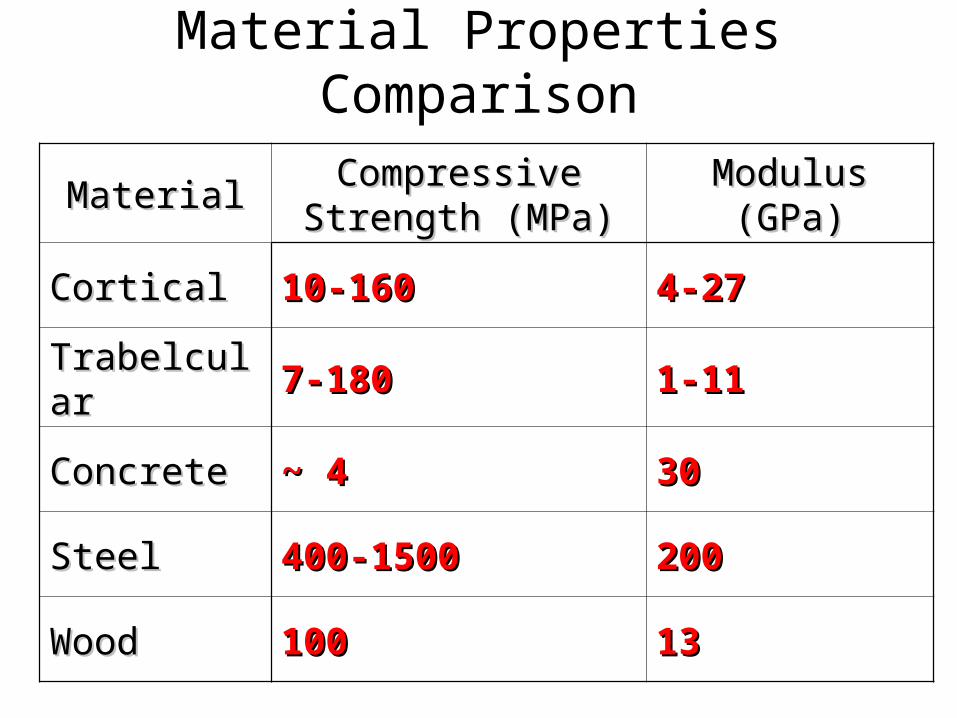
Material Properties Comparison
MaterialMaterial Compressive Compressive Strength (MPa)Strength (MPa)
Modulus Modulus (GPa)(GPa)
Cortical Cortical 10-16010-160 4-274-27
TrabelcularTrabelcular 7-1807-180 1-111-11
ConcreteConcrete ~ 4~ 4 3030
SteelSteel 400-1500400-1500 200200
WoodWood 100100 1313
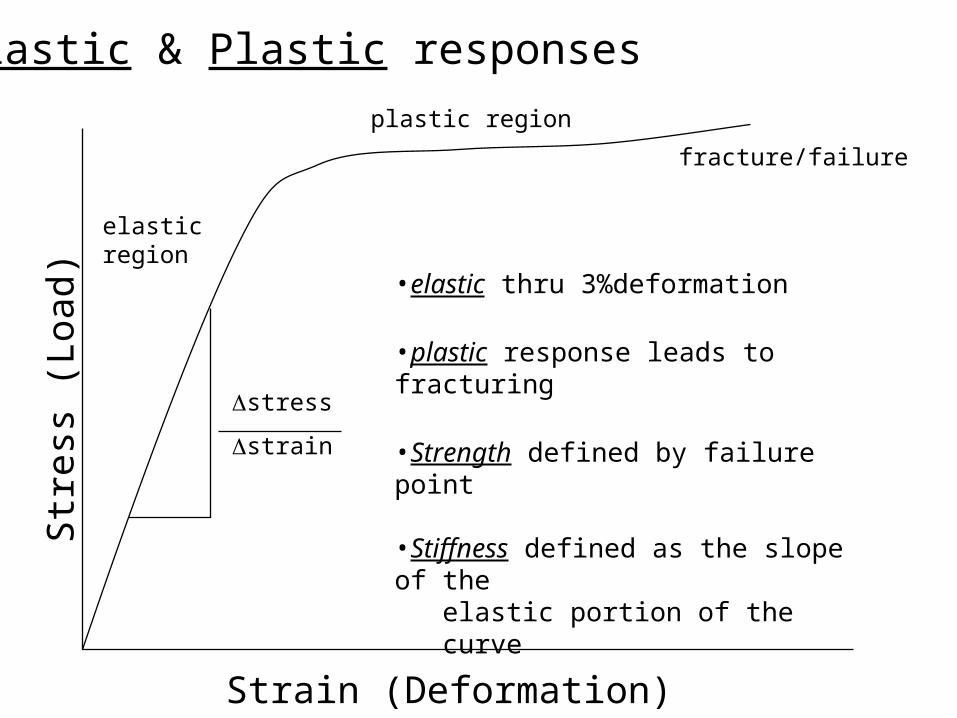
elasticregion
plastic region
fracture/failure
Str
ess
(Loa
d)
Strain (Deformation)
stress
strain
Elastic & Plastic responses
•elastic thru 3%deformation
•plastic response leads to fracturing
•Strength defined by failure point
•Stiffness defined as the slope of the elastic portion of the curve

Elastic Biomaterials (Bone)
•Elastic/Plastic characteristics
Brittle material fails before permanent deformation
Ductile material deforms greatly before failure
Bone exhibits both properties
Load/deformation curves
deformation (length)
load ductile material
elasticlimit
bone
brittle material
Fatigue of BoneMicrostructural damage due to repeated loads
below the bone’s ultimate strength – Occurs when muscles become fatigued and less able to
counter-act loads during continuous strenuous physical activity
– Results in Progressive loss of strength and stiffness
Cracks begin at discontinuities within the bone (e.g. haversian canals, lacunae) – Affected by the magnitude of the load, number of cycles,
and frequency of loading
Fatigue of Bone (Cont’)• 3 Stages of fatigue fracture
– Crack Initiation• Discontinuities result in points of increased local stress where
micro cracks form – Often bone remodeling repairs these cracks
– Crack Growth (Propagation)• If micro cracks are not repaired they grow until they encounter a
weaker material surface and change direction– Often transverse growth is stopped when the crack turns from
perpendicular to parallel to the load
– Final Fracture• Occurs only when the fatigue process progresses faster than
the rate of remodeling
http://www.orthoteers.co.uk/Nrujp~ij33lm/Orthbonemech.htm Simon, SR. Simon, SR. Orthopaedic Basic ScienceOrthopaedic Basic Science. Ohio: American Academy of Orthopaedic Surgeons; 1994.. Ohio: American Academy of Orthopaedic Surgeons; 1994.
Fatigue Fracture
A fatigue fracture may be caused by:– Abnormal muscle stress
• Loss of shock absorption• Strenuous or repeated activity
– Associated with new or different activity• Abnormal loading• Abnormal stress distribution
Fatigue Theory– During repeated efforts (as in running)
• Muscles become unable to support during impact
• Muscles do not absorb the shock
• Load is transferred to the bone
• As the loading surpasses the capacity of the bone to adapt
• A fracture develops
骨折愈合
• Fractures: Any bone break.- blood clot will form around break
- fracture hematoma- inflammatory process begins- blood capillaries grow into clot- phagocytes and osteoclasts remove damaged tissue- procallus forms and is invaded by osteoprogenitor cells and fibroblasts- collagen and fibrocartilage turns procallus to fibrocartilagenous (soft) callus
- broken ends of bone are bridged by callus- Osteoprogenitor cells are replaced by osteoblasts and spongy
bone is formed- bony (hard) callus is formed- callus is resorbed by osteoclasts and compact bone replaces
spongy bone.Remodeling : the shaft is reconstructed to resemble original unbroken bone.
6-101
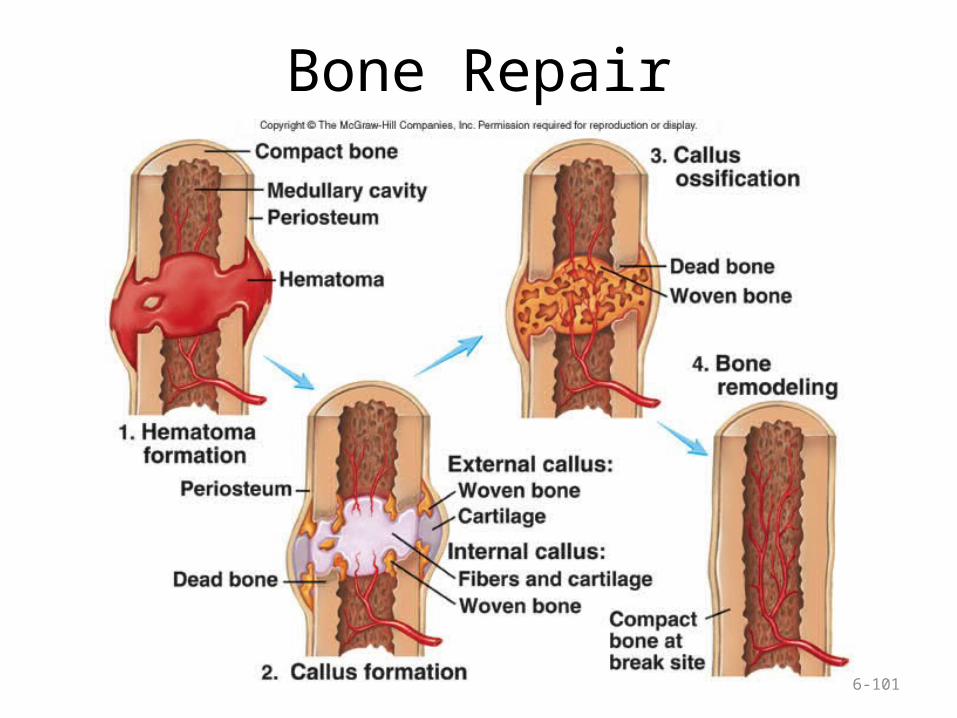
Bone Repair
Fractures MUST have ablood supply to heal
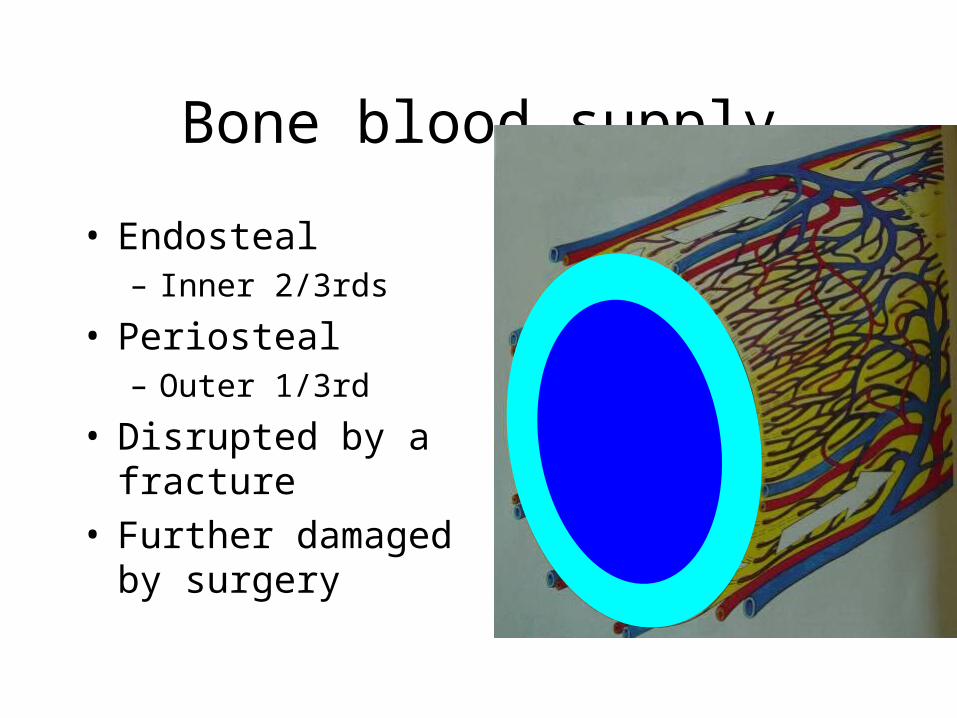
Bone blood supply
• Endosteal– Inner 2/3rds
• Periosteal– Outer 1/3rd
• Disrupted by a fracture• Further damaged by
surgery
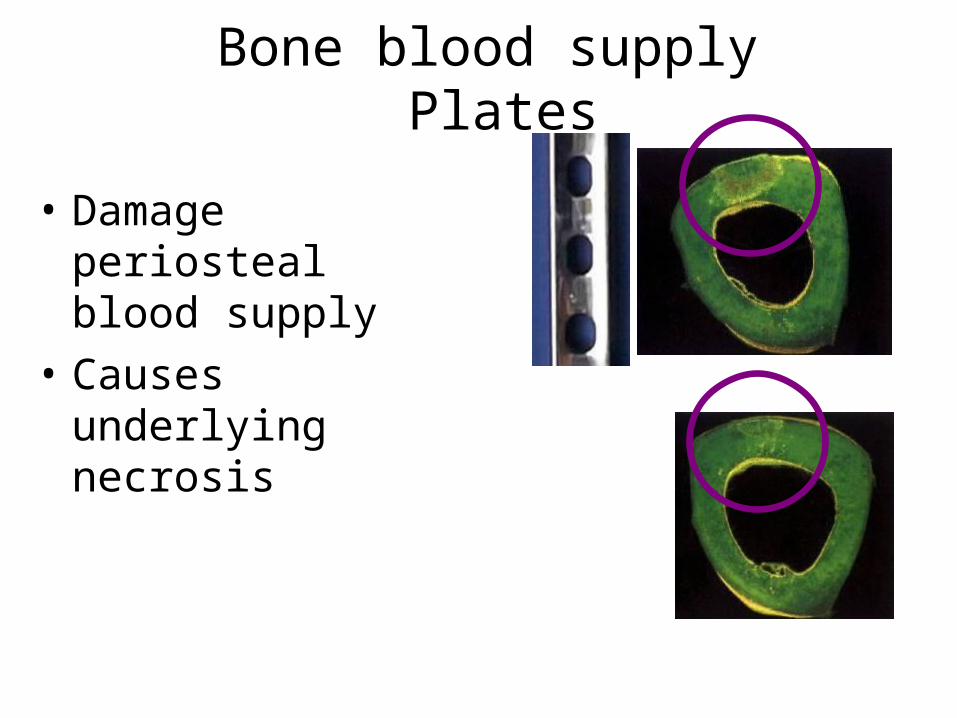
Bone blood supply Plates
• Damage periosteal blood supply
• Causes underlying necrosis
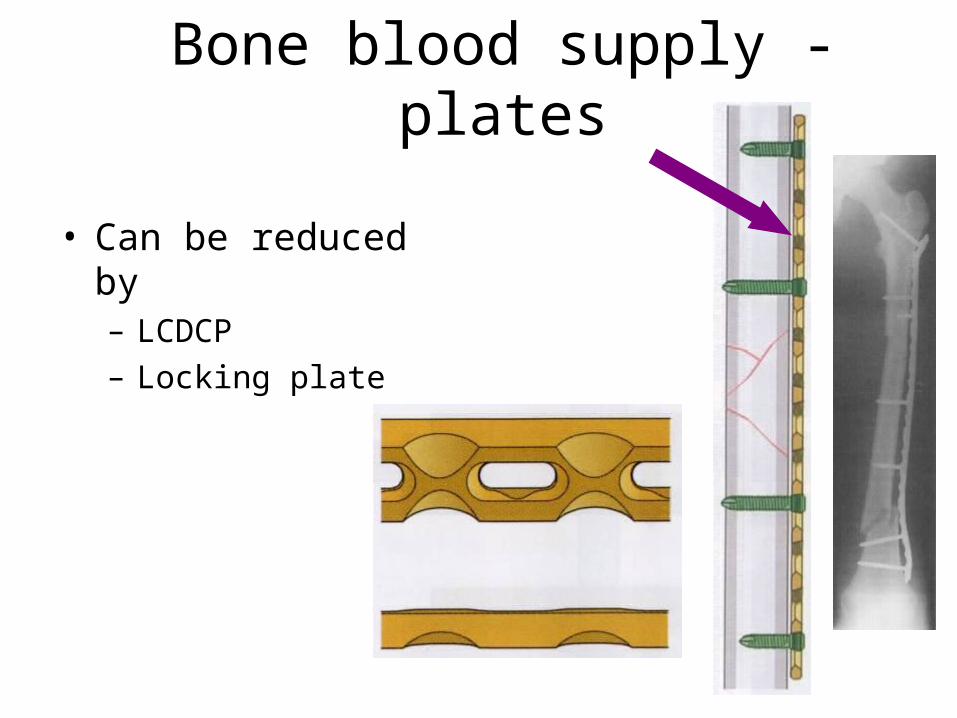
Bone blood supply - plates
• Can be reduced by– LCDCP– Locking plate

Augmentation of fracture healing
Bone GraftsBone Graft SubstitutesOsteo-inductive agentsMechanical methodsUltrasoundElectromagnetic fields
Bone Graft PropertiesOsteoconduction
3D scaffoldOsteo-induction
Biological stimulusOsteogenic
Contains living cells that can differentiate to from bone
Mesenchymal cells Osteoprogenitor cells
Structural

Osteo-inductive agents
• Transforming growth factor Superfamily– BMPs– GDFs (growth differentiation factors)– Possibly TGF-β 1, 2, and 3.
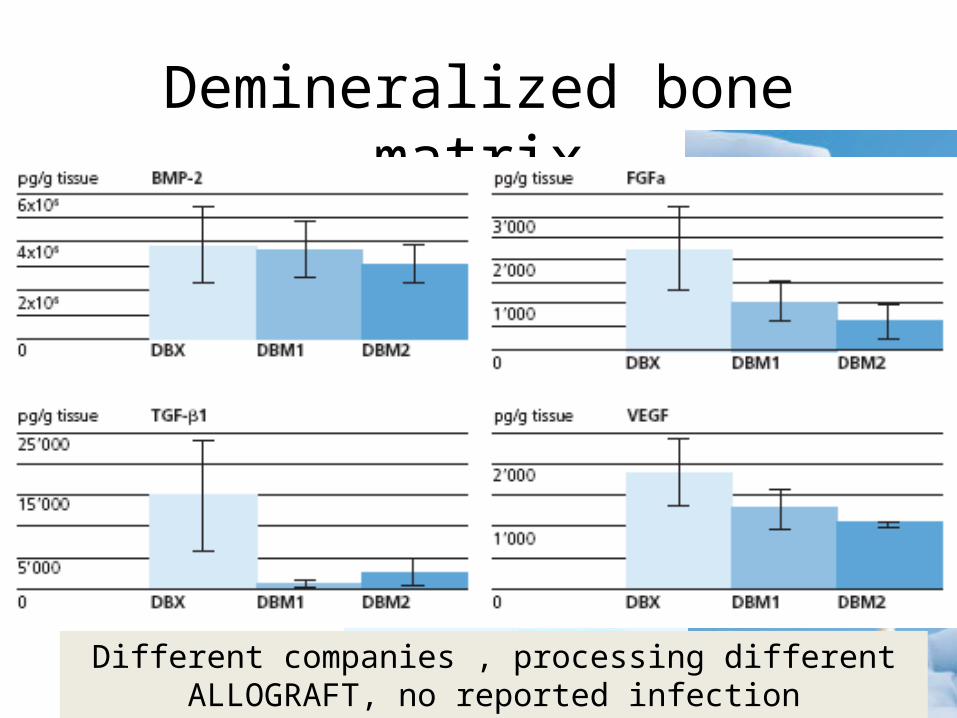
Demineralized bone matrix
• Acid extraction of allograft– type-1 collagen– non-collagenous proteins– osteoinductive growth factors: BMP, GDFs, TGF1,2 + 3
Different companies , processing differentALLOGRAFT, no reported infection transmission
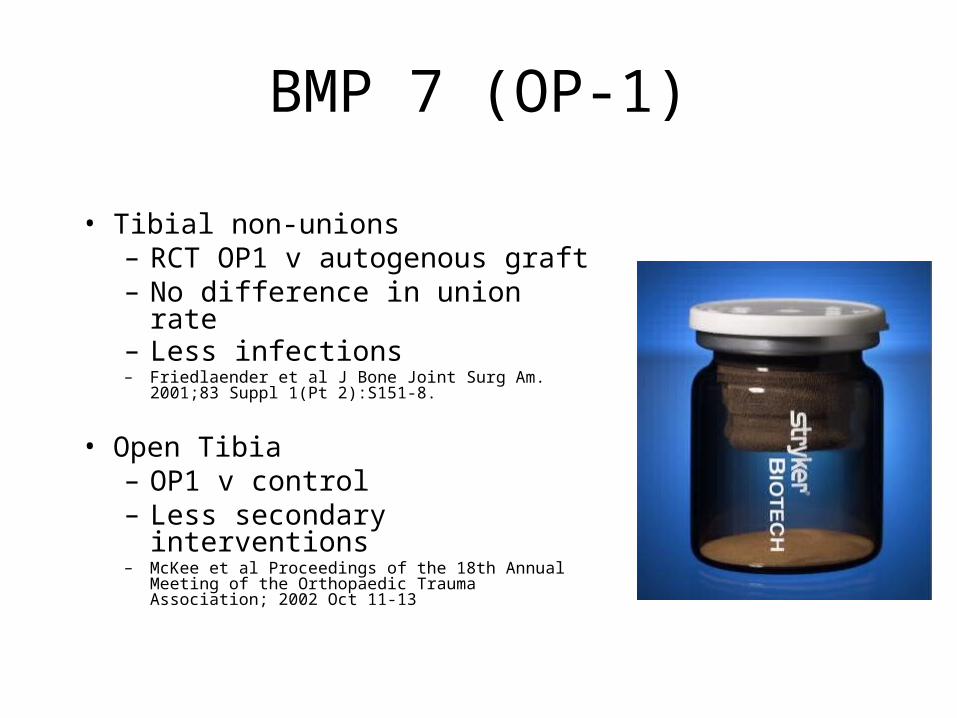
BMP 7 (OP-1)
• Tibial non-unions– RCT OP1 v autogenous graft– No difference in union rate– Less infections – Friedlaender et al J Bone Joint Surg Am. 2001;83 Suppl
1(Pt 2):S151-8.
• Open Tibia– OP1 v control– Less secondary interventions– McKee et al Proceedings of the 18th Annual Meeting of
the Orthopaedic Trauma Association; 2002 Oct 11-13
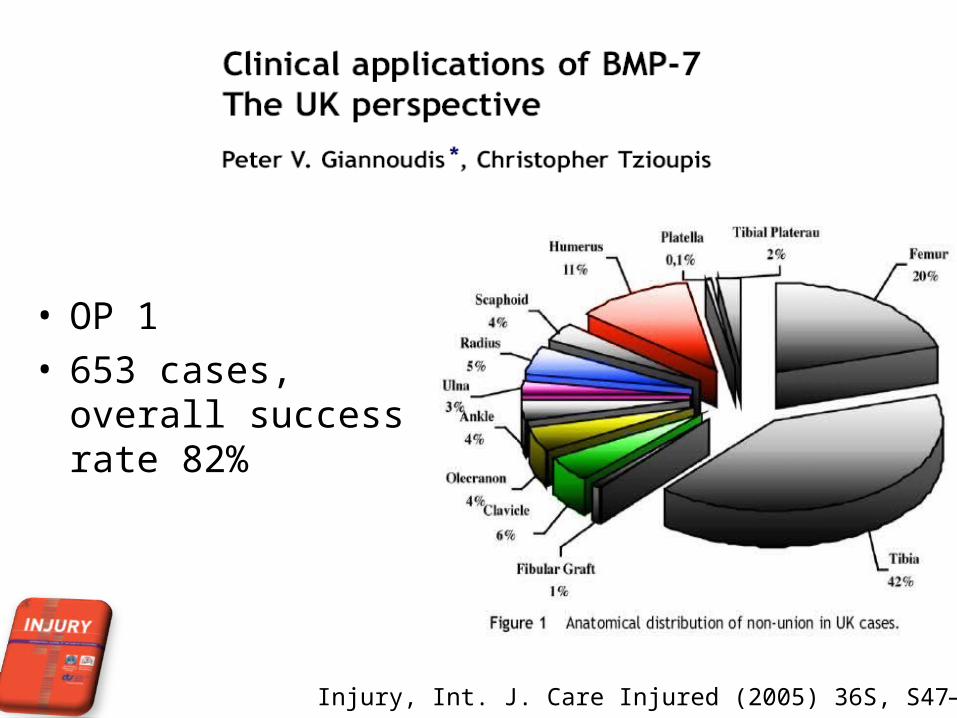
• OP 1• 653 cases, overall
success rate 82%
Injury, Int. J. Care Injured (2005) 36S, S47—S50

• BMP £ 3000 per vial• Mean number of operations
• Pre BMP 4.16• Post BMP 1.2
• Hospital stay and cost• Pre BMP 26.84 days and £ 13,844.68• Post BMP 7.8 days and £ 7338.40
• Overall cost using BMP-7 - 47.0% less.
Injury, Int. J. Care Injured (2007) 38, 371—377
BMP 2
• BESTT• Open tibial fractures
– Control v 6mg v 12mg– Higher dose
• Fewer secondary procedures• accelerated time to union• improved wound-healing• Reduced infection rateGovender et al Recombinant human bone morphogenetic protein-2 for
treatment of open tibial fractures: a prospective, controlled, randomized study of four hundred and fifty patients. J Bone Joint Surg Am. 2002;84:2123-34.

Osteoconductive
Making the break. Karin Hing's fellowship has brought independence to pursue her work on bone graft substitutes.

Osteoconductive RCT’s osteoconductive materials Vs autograft
encouraging.– Calcium sulfate
• Predictable resorption• Resorbs a little too fast
– Calcium phosphates • Tricalcium phosphate TCP• Hydroxyapatite• TCP is more rapidly absorbed than hydroxyapatite, TCP
inadequate when structural support is desired
– Injectable osteoconductive cements• Several variations

Concentrated bone marrow aspirate
• Non union – 75-95% success• Aseptic non-unions
– Only works if adequate cell concentration
– Hernigou Pet al Influence of the number and concentration of progenitor cells. J Bone Joint Surg Am. 2005;87:1430 -7
• Concentrated BM aspirate– Ongoing multicentre RCT in France– Open tibial fractures
Composite synthetic graft
• Prospective multicenter RCT• 249 long-bone #, min two years FU• Bone graft v biphasic calcium phosphate mixed with bovine
collagen + autogenous bone marrow
• No sig. diff.– More infections with bone graft (22 v 9 p=0.008)
• Chapman MW et al. Treatment of acute fractures with a collagen-calcium phosphate graft material. A randomized clinical trial. J Bone Joint Surg Am. 1997;79:495-502.

Mechanical
Controlled axial micromotionCompressionDistractionLIPUSElectromagnetic
Controlled axial micromotion
• Prospective RCT 102 tibial fractures– 1.0 mm at 0.5 Hz /30 minutes per day
• Sig. reduction– Time to union– Secondary surgery
• Kenwright J, Goodship AE. Controlled mechanical stimulation in the treatment of tibial fractures. Clin Orthop 1988;241:36-47.
Low Intensity Ultrasound
• Several RCTs• Reduced time to union
– Non-op tibia (No benefit in nailed #)
– Scaphoids– Impacted distal radius– Jones
• May reduce time to healing• JW Busse et al. The effect of low-intensity pulsed ultrasound therapy on time
to fracture healing: a meta-analysis. Canadian Medical Association Journal 2002 166: 437-441
Sonic Accelerated Fracture Healing
System (SAFHS®) -Exogen 2000®

• Acute fractures with ultrasound• Inconsistency in evidence ? Type II failure• Available evidence supports the use of ultrasound in the
treatment of acute fractures of tibia and radius treated with plaster immobilization. (non op)
• No benefit of LIPUS in the treatment of fractures of the tibia managed with intramedullary fixation.
J Trauma. 2008 Dec;65(6):1446-52
• Current evidence on the efficacy of low-intensity pulsed ultrasound to promote fracture healing is adequate to show that this procedure can reduce fracture healing time and gives clinical benefit, particularly in circumstances of delayed healing and fracture non-union.
• There are no major safety concerns. • Therefore this procedure may be used with normal
arrangements for clinical governance, consent and audit
Electromagnetic devices
• In vivo– Osteoblasts BMP,TGFs, IGF
• Small RCT– 66% vs 0 healing of tibial non-unionScott G, King JB. A prospective double blind trial of electrical capacitive coupling in
the treatment of nonunion of long bones. J Bone Joint Surg [Am] 1994;76-A:820-6.
• Several series– 64-87% union of tibial non-union

术后 3 周术前
自体自体 PRPPRP 浓集治疗骨折不愈合临床研究浓集治疗骨折不愈合临床研究
浙江省男排主力(二传)戴 ** , 男, 20 岁 骨折不愈合 11 月余
浙大案例浙大案例

骨髓干细胞治疗骨髓干细胞治疗

治疗前治疗前 治疗两年后治疗两年后
两年后股骨头坏死区体积比较。骨髓干细胞移植治疗组(实线),对照组(虚线)
骨髓干细胞治疗骨髓干细胞治疗
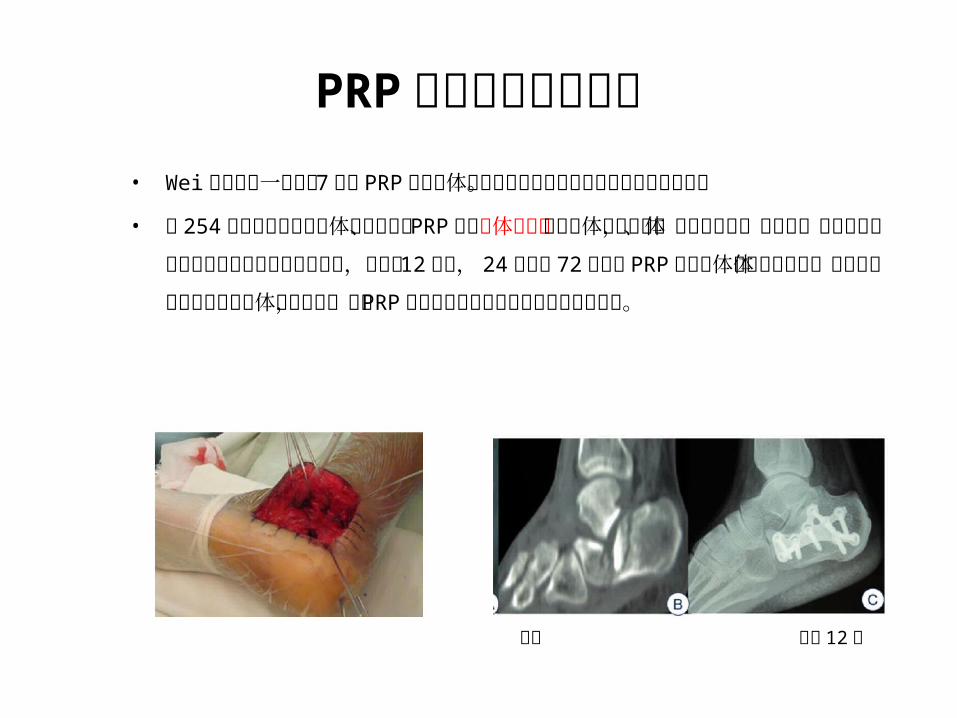
PRP 联合生物材料治疗• Wei 等进行了一项长达 7 年的 PRP 联合异体骨移植治疗跟骨关节内骨折移位
临床试验。
• 将 254 例患者随机分成自体骨移植组、 PRP 联合异体骨移植组和异体骨移植组,通过影像学、三维立体扫描断层技术和足踝功能评分评估治疗结果,发现在 12 个月, 24 个月和 72 个月时 PRP 联合异体骨移植组和自体骨移植组明显优于单纯异体骨移植组,显示 PRP 对跟骨关节内骨折移位治疗有促进作用。
术前 术后 12 月
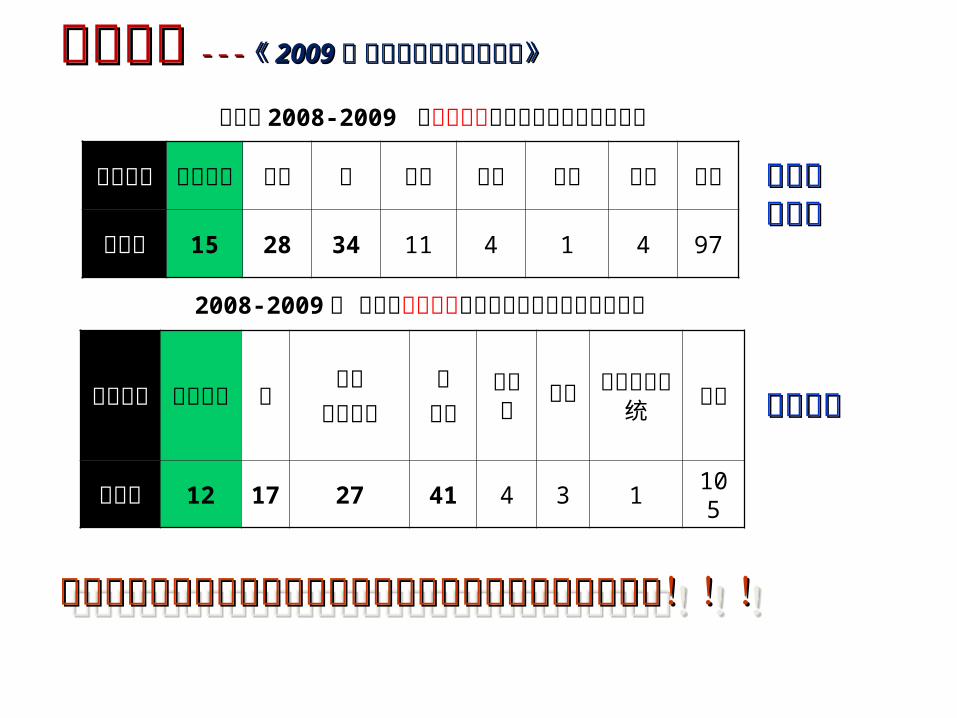
国际现状国际现状 ------ 《《 20092009 年 世界再生医学调查报年 世界再生医学调查报告告》》
2008-2009 年 已进入临床实验期的组织工程和再生医学产品
国际上 2008-2009 已市场化的组织工程和再生医学产品
产业化产业化较成熟较成熟
更新活跃更新活跃
目标组织
关节软骨 皮肤 骨 牙科 眼科 美容 其他 总
计产品
数 15 28 34 11 4 1 4 97
目标组织
关节软骨 骨
皮肤伤口愈合
心血管
糖尿病
肝脏
中枢神经系统
总计
产品数 12
17
27 41 4 3 1105
我国组织工程和再生医学技术的开发和临床转化我国组织工程和再生医学技术的开发和临床转化明显严重滞后!!!明显严重滞后!!!
我国组织工程和再生医学技术的开发和临床转化我国组织工程和再生医学技术的开发和临床转化明显严重滞后!!!明显严重滞后!!!
知识要点 能够描述脊柱组成,胸廓组成,骨盆组成
能够绘画肱骨,尺骨,桡骨,股骨,胫骨大体结构
能够描述骨的细胞和组织成分
能够绘画骨单位结构
能够描述骨组织发育主要阶段
能够描述 osteoblast 和 osteoclast 的分化阶段
能够描述骨组织的主要生物力学特性
能够描述骨愈合主要过程
能够描述骨质疏松疾病中相应“骨的宏观 / 微观结构 - 力学性能 -
osteoblast/osteoclast- 主要信号通路”每一层面的改变和相互联系,并能思考针对每一个层面改变可能采取的干预措施。

谢 谢!
Top Related