Workforce Study of Endocrinologists
76
WORKFORCE STUDY OF ENDOCRINOLOGISTS Final Report Prepared for: The Endocrine Society The American Association of Clinical Endocrinologists The American Diabetes Association The Association of Program Directors of Endocrinology, Diabetes, and Metabolism American Thyroid Association Lawson Wilkens Pediatric Endocrine Society Prepared by: The Lewin Group Paul F. Hogan Colleen Hirschkorn Jared Hughes Brian Simonson Michael H. Cardwell March 17, 2001
-
Upload
roger961 -
Category
Health & Medicine
-
view
626 -
download
2
Transcript of Workforce Study of Endocrinologists

WORKFORCE STUDY OF ENDOCRINOLOGISTS
Final Report Prepared for: The Endocrine Society The American Association of Clinical Endocrinologists The American Diabetes Association The Association of Program Directors of Endocrinology, Diabetes, and Metabolism American Thyroid Association Lawson Wilkens Pediatric Endocrine Society Prepared by: The Lewin Group Paul F. Hogan Colleen Hirschkorn Jared Hughes Brian Simonson Michael H. Cardwell March 17, 2001

WORKFORCE STUDY OF ENDOCRINOLOGISTS
Final Report
Prepared for: The Endocrine Society
The American Association of Clinical Endocrinologists
The American Diabetes Association The Association of Program Directors of
Endocrinology, Diabetes, and Metabolism American Thyroid Association
Lawson Wilkens Pediatric Endocrine Society
Prepared by: The Lewin Group
Paul F. Hogan Colleen Hirschkorn
Jared Hughes Brian Simonson
Michael H. Cardwell
March 17, 2001

Table of Contents
1. INTRODUCTION AND BACKGROUND......................................................................................................1
1.1 PURPOSE ..........................................................................................................................................................1 1.2 WORKFORCE STUDIES......................................................................................................................................1 1.3 ENDOCRINOLOGISTS AS PHYSICIANS................................................................................................................2 1.4 MARKET-BASED ANALYSIS AND LIMITATIONS................................................................................................2
2. CURRENT WORKFORCE..............................................................................................................................3
2.1 DEFINING THE CURRENT WORKFORCE.............................................................................................................3 2.2 DEMOGRAPHIC CHARACTERISTICS OF THE CURRENT WORKFORCE .................................................................5 2.3 GEOGRAPHIC DISTRIBUTION OF ENDOCRINOLOGISTS ......................................................................................8
3. SUPPLY AND DEMAND ISSUES.................................................................................................................10
3.1 METHOD AND DATA.......................................................................................................................................10 3.2 SUPPLY ISSUES...............................................................................................................................................12
3.2.1 Trends in Residencies and Fellowships ...............................................................................................12 3.2.2 Retirement Rates ..................................................................................................................................16
3.3 DEMAND ISSUES ............................................................................................................................................17 3.3.1 Demand for Services............................................................................................................................17 3.3.2 Population Dynamics...........................................................................................................................24 3.3.3 Managed Care .....................................................................................................................................26 3.3.4 Econometric Estimates of the Effects of Managed Care and Other Factors Affecting Demand .........30 3.3.5 A “Benchmark” Estimate of Current Endocrinologist Clinical Demand............................................34 3.3.6 Earnings of Endocrinologists ..............................................................................................................36
4. PROJECTIONS OF THE SUPPLY OF AND DEMAND FOR ENDOCRINOLOGISTS .......................39
4.1 BASELINE.......................................................................................................................................................39 4.2 CASE 1: OVERALL ASSESSMENT ....................................................................................................................41 4.3 CASE 2: SENSITIVITY TO ASSUMPTION REGARDING INITIAL EXCESS DEMAND..............................................49 4.4 CASE 3: EFFECT OF INCREASE IN DIABETES ON DEMAND ..............................................................................53 4.5 CASE 4: GROWTH IN FELLOWSHIP POSITIONS ................................................................................................56 4.6 CASE 5: OTHER SUPPLY FACTORS ................................................................................................................59 4.7 CONCLUSION..................................................................................................................................................63
5. SUMMARY ......................................................................................................................................................64
6. REFERENCES.................................................................................................................................................68
7. APPENDIX A: TECHNICAL ADVISORY PANEL PERSPECTIVES .......................................................1
265991

Workforce Study of Endocrinologists
1. INTRODUCTION AND BACKGROUND
1.1 Purpose A consortium consisting of The Endocrine Society, the American Association of Clinical Endocrinologists and the American Diabetes Association, with participation by The Association of Program Directors of Endocrinology, Diabetes, and Metabolism; the American Thyroid Association; and Lawson Wilkens Pediatric Endocrine Society, has asked The Lewin Group to conduct a workforce study of endocrinologists. The primary purpose of this paper is to present the results of this workforce study. Following this introduction, the report consists of three major sections. In the first, we define and describe the current workforce, its training and certification status, and its demographic characteristics. The second section examines the factors affecting the supply of endocrinologists and the factors affecting the demand for endocrinologists. In the third portion of the paper, we apply the Endocrinologist Workforce Model. Using this model, we examine the endocrinologist workforce over the next 20 years, projecting demand and supply under alternative scenarios regarding the health care market demand for and the supply of the services of endocrinologists. We provide an overall assessment of the workforce over the next 20 years.
1.2 Workforce Studies Interest in physician workforce issues can be traced at least to the late 1960’s. The predominant concern was the adequacy of the physician workforce--ensuring that there were sufficient physicians to meet patient needs. The Graduate Medical Education National Advisory Committee (GMENAC) was founded in 1976 by the U. S. Department of Health Education and Welfare to estimate the need for physicians, by specialty, in the year 1990. The primary concern was to insure that there would be sufficient physicians to meet the need. The Committee systematically began estimating the need for various physician specialties, using estimates based on the judgments of experts--a method that has come to be known as the “GMENAC” method. While the notion of centralized planning of physician supply was implicit in GMENAC, it became somewhat more explicit with the establishment of the Council on Graduate Medical Education (COGME) in 1986. The emphasis shifted from concern regarding too few physicians, in general, to concern that there were too many specialists relative to generalists. Centralized planning of residency positions became explicit in the Clinton Administration’s proposal for health care reform, the Health Security Act, in 1993. The prospect of centralized planning of residency positions placed a premium on determining whether a given physician specialty was a shortage specialty or a surplus specialty. Consequently, it sparked a renewed interest in models of the physician workforce. In a particularly influential and controversial article, Weiner (1994) projected, based on the staffing patterns of staff-model health maintenance organizations (HMOs), that there would be a substantial excess supply of specialists by the year 2000. The challenge of centralized planning for physician supply diminished substantially when Congress failed to pass a major health care reform bill. Today, the focus of physician specialty
The Lewin Group, Inc. 1 265991

Workforce Study of Endocrinologists
workforce studies is typically the effect of market factors such as managed care and competition from other providers on the demand for the services of the specialty. These issues have become relatively more important than estimates of the more normative or prescriptive concept of need. The goal is a better understanding of the effects of market trends on demand and supply, and how the profession as a whole, as well as individual physicians, can adapt to those trends.
1.3 Endocrinologists as Physicians Endocrinology concerns the study of all factors affecting the secretion and circulation of hormones and their role in health and disease. The primary source of hormones is the endocrine system, which encompasses the major endocrine glands, including the thyroid, pancreas, parathyroid, pineal, adrenal, ovaries, testes and pituitary glands, but other organs also secrete hormones. Endocrinologists include those who are engaged in the research and study of endocrinology, and those who are engaged in the clinical application of that research. This may include physicians, biochemists, physiologists, geneticists, immunologists, pharmacologists, molecular and cellular biologists, and others. Here, our primary focus is endocrinologists who are physicians. Most are engaged in the clinical practice of endocrinology and, perhaps, in the education of physicians in the clinical practice of endocrinology.
1.4 Market-Based Analysis and Limitations Two points should be made at the outset. First, there is no attempt in this study to determine the “right” number of endocrinologists in a normative or needs-based sense. The estimates of demand are based on market conditions which reflect underlying epidemiological conditions or “need”. But, they also embody the market realities that generate effective demand for health care: insurance coverage, the degree of managed care penetration, the distribution of income, and competition from other providers. Hence, no necessary normative significance should be attributed to the demand estimates, nor to associated market “equilibria”.1 Second, we provide predictions of future supply and demand over the next twenty years. While the predictions have the appearance of precision, there are too many variables to achieve such precision, in practice. Events that can not now be anticipated will undoubtedly have a significant and unpredictable influence on the demand for endocrinologists ten or twenty years from now. Thus, our point estimates should be interpreted as representing a broad range, under the assumption that all other factors are constant. Our overall market assessment is based on the systematic analysis of a number of cases or scenarios that our research indicates are likely to affect future demand and supply. Undoubtedly, there will be factors arising that will affect future markets that cannot currently be anticipated. An advantage of a workforce model is that the implications of alternative assumptions or projections regarding the future can be evaluated quickly.
1 The only additional significance of an estimated equilibrium point--a point at which demand is approximately
equal to supply--is that the number and incomes of endocrinologists will be stable at that point. If demand exceeds supply, one can anticipate rising incomes and increases in the numbers of endocrinologists, and vice versa if supply were to exceed demand.
The Lewin Group, Inc. 2 265991

Workforce Study of Endocrinologists
2. CURRENT WORKFORCE
2.1 Defining the Current Workforce Defining and counting the current workforce may seem like a straightforward task, hardly worth reporting. However, there are a number of alternative criteria for defining the current supply of endocrinologists which lead to different current estimates. The choice is important, because this “baseline” number will permeate all subsequent analyses. The Technical Advisory Panel to our study was instrumental in helping us define the current stock. In defining endocrinologists for the purpose of our workforce study, we consider several issues. • Specialties as self-reported to the AMA • Credentials such as subspecialty board certification from ABIM • Formal professional training in the form of fellowships • Other specialties which, in practice, might substitute for endocrinology in some practice
areas but could not be considered endocrinologists, such as OB/GYN, urology, and others. Using the above as general guidelines, we propose to define endocrinologists for the purposes of the workforce study as any MD or DO who meets the following criteria as self-reported to the American Medical Association: 1) Must claim at least one of the following as either a primary or secondary specialty:
endocrinology (END), diabetes (DIA), reproductive endocrinology (REN) or pediatric endocrinology (PDE). Physicians who have been trained or certified in an endocrinology subspecialty but do not practice it as a specialty should not be included.
2) Must not claim “Resident” as their current major professional activity. Only physicians who have completed their training and have entered the workforce should be considered.
3) Must not claim obstetrics (OBS or OBG) as either a primary or secondary specialty. Many OB/GYNs claim an endocrinology subspecialty but do not, in fact, practice endocrinology as their primary focus.
4) If REN, must have completed Graduate Medical Training (GMT) in either Pediatrics (PD) or Internal Medicine (IM).
5) Must have completed GMT in one of the four specialties listed above or be board-certified in an endocrinology subspecialty. See Table 1.
We separate endocrinologists into three specialty groups: reproductive, pediatric and general/diabetes. The number of DIA specialists is relatively small, and the majority of them also specialize in END. All the DIA specialists included in our population of endocrinologists are board certified in endocrinology. About 63% of them indicate fellowship training in endocrinology, which is only slightly lower than all other endocrinologists. The following is a step-by-step summary, by specialty group, of the implications of our criteria, showing how many physicians are eliminated when a criterion is applied.
The Lewin Group, Inc. 3 265991

Workforce Study of Endocrinologists
Table 1. Summary of Selection Criteria by Specialty Group Primary Specialty END/DIA REN PDE Total Self-reported endocrinology specialists 4193 1008 884 6085 Residents -7 -2 -85 -94 OBS specialists -53 -573 0 -626 REN, did not complete GMT in PD or IM 0 -394 0 -394 Subtotal 4133 39 799 4971 a) GMT-trained in endocrinology 2547 11 586 3144 b) Board-certified 3611 28 506 4175 c) Board-certified and/or completed GMT 3623 28 719 4506
After eliminating those physicians who did not meet our first four selection criteria, we are left with 4,971. The last three lines on the table above show alternative scenarios for our final selection of physicians. Line (a) shows only those physicians who completed a fellowship in their respective subspecialties. Line (b) shows only those physicians who have been certified by their respective subspecialty boards. Line (c), our preferred definition, shows all physicians who fit the criteria for either (a) or (b): either board-certified or fellowship-trained. The American Board of Internal Medicine reports on its website that 3,987 ABIM certificates have been issued in the US in endocrinology as of January 2000, while our current AMA file shows that 3,824 physicians are board-certified in endocrinology. However, 338 physicians in our file are board-certified in endocrinology but do not claim END or DIA as a specialty. Of those, 238 (73%) claim urology as either a primary or secondary specialty. We exclude them from our analysis.2 Our data also shows that only 2,871 physicians completed a fellowship in endocrinology. If we omit those who did not complete a fellowship, we lose roughly a third of our population in END. Furthermore, it appears that GMT training increases for latter cohorts of physicians. That is, of board-certified endocrinologists who received their MD before 1973, it is reported that only 33% completed a fellowship in endocrinology, while of those who received their MD in 1973 or later, 84% completed a fellowship. For that reason, we recommend including all physicians who are either board-certified or fellowship-trained in an endocrinology specialty or subspecialty. The fact that our estimates of the total number who are board certified are within about 150 of ABIM’s total number of diplomates certified suggests that these are properly certified endocrinologists. 3 The following is a summary of endocrinologists by major professional activity (MPA), using our preferred definition as described above.
2 This decision is based on the advice of the TAP. 3 Some TAP members expressed surprise that there were a significant number of board-certified endocrinologists
who did not report formal fellowship training in endocrinology. This information is self-reported by the physicians, and there may be errors. However, we do note that the proportions that report certification but do not report fellowship training in endocrinology were much greater for those who were graduated from medical school prior to 1973. We suspect that the typical path for certification may have changed over time, but the TAP members could not confirm this based on their knowledge and experience.
The Lewin Group, Inc. 4 265991

Workforce Study of Endocrinologists
Table 2. Major Professional Activities of Endocrinologists
Major Professional Activity END/DIA REN PDE Total % of Total Office-Based Practice 2389 21 400 2810 64.30% Research 465 2 102 569 13.02% Full-Time Hospital Staff 355 3 99 457 10.46% Administration 134 1 13 148 3.39% Medical Teaching 130 1 16 147 3.36% Not Classified/Other 150 0 89 239 5.47%
Total 3623 28 719 4370 100.0%
Table 3 presents the same information separately for adult and pediatric endocrinologists.
Table 3 Major Professional Activities
Adult and Pediatric Endocrinologists Major Professional Activity Non-PDE % of Total PDE % of Total Office-Based Practice 2410 66.0% 400 55.6% Research 467 12.8% 102 14.2% Full-time Hospital Staff 358 9.8% 99 13.8% Administration 135 3.7% 13 1.8% Medical Teaching 131 3.6% 16 2.2% Not Classified / Other 150 4.1% 89 12.4%
Total 3651 719 The primary activity of the majority of both adult and pediatric endocrinologists is office-based clinical practice. Higher proportions of pediatric endocrinologists are full-time hospital staff compared to adult endocrinologists, and only a small portion of each are engaged in teaching.
2.2 Demographic Characteristics of the Current Workforce The median age for all endocrinologists, as we have defined them, is 49, as of 1999. About 71.9% of endocrinologists are male. The median age of male endocrinologists is 51, while the median age of female endocrinologists is 44. Table 4 summarizes the age and sex distribution of endocrinologists, as of 1999.
Table 4 Age and Sex Distribution of Endocrinologists
Age N % Male % Female <40 638 49.5% 50.5% 40-49 1631 62.9% 37.1% 50-59 1423 82.4% 17.6% 60-69 574 92.5% 7.5% 70 + 104 90.4% 9.6%
Total 4370 71.9% 28.1%
The Lewin Group, Inc. 5 265991

Workforce Study of Endocrinologists
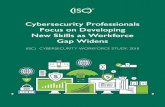
The median age of endocrinologists is greater than for physicians as a whole, and for many specialties. This is probably because the typical path to becoming a fellowship-trained endocrinologist, which would include a residency in internal medicine or pediatrics and a two or three year fellowship program in endocrinology, suggests that there are virtually no endocrinologists under age 30. Most would not become board-certified until they are in their mid-thirties. It is also interesting that, although over 70% of endocrinologists are male, the sex distribution is about even for those under age 40. In 1999, about 46% of endocrinology fellows were female. In adult endocrinology, 44% were female while in pediatric endocrinology about 55% were female.4 The following graph of the age distribution of male, female, and total endocrinologists illustrates the points made in the previous paragraph.5
Figure 1 Age Distribution of Endocrinologists (1999)
0
50
100
150
200
250
29 33 37 41 45 49 53 57 61 65 69 73 77
Age
Phys
icia
ns
TotalM aleFemale
The next two figures break out the age distribution for adult endocrinologists and pediatric endocrinologists.
4 The National Study of Graduate Medical Education in Internal Medicine (NaSGIM) and the American Board of
Pediatrics. 5 We note that there is a “spike” in the age distribution of endocrinologists at about age 56. This would be the
cohort that was graduated from medical school in about 1973.
The Lewin Group, Inc. 6 265991

Workforce Study of Endocrinologists
Figure 2 Age Distribution of Adult Endocrinologists
0
20
40
60
80
100
120
140
160
180
31 35 39 43 47 51 55 59 63 67 71 75 80
Age
Phys
icia
nsTotalM aleFemale
Figure 3
Age Distribution of Pediatric Endocrinologists
0
5
10
15
20
25
30
35
40
45
29 33 37 41 45 49 53 57 61 65 69 73 79
Age
Phys
icia
ns
TotalM aleFemale
We note that the age distribution of adult endocrinologists parallels that of the distribution of all endocrinologists. The age distribution of pediatric endocrinologists, on the other hand, suggests that approximately the same number of women and men were becoming pediatric endocrinologists as early as about the 1972 medical school class, while more women than men were becoming pediatric endocrinologists in medical school classes after about 1985.
The Lewin Group, Inc. 7 265991

Workforce Study of Endocrinologists
2.3 Geographic Distribution of Endocrinologists Overall, there are 1.6 endocrinologists per 100,000 population (1999). Endocrinologists are more highly concentrated in New England (3.3 per 100,000) and in the Middle Atlantic (2.4 per 100,000) regions of the country, as measured by physicians per 100,000 population. They are least concentrated in the East South Central and Mountain census regions (1.1 per 100,000). Table 5 summarizes this geographic distribution.
Table 5 Endocrinologists per 100,000 Population by Census Region
Census Division Endocrinologists % of Total Docs/100k Population East North Central 587 13.4% 1.32 East South Central 176 4.0% 1.06 Middle Atlantic 929 21.3% 2.43 Mountain 183 4.2% 1.06 New England 438 10.0% 3.26 Pacific 722 16.5% 1.64 South Atlantic 746 17.1% 1.51 West North Central 247 5.7% 1.32 West South Central 342 7.8% 1.13
Total 4370 1.60 Table 6 presents the number of endocrinologists per 100,000 population for the 20 largest metropolitan statistical areas (MSAs). For information, the HMO penetration rate, the proportion of the population that is enrolled in a health maintenance organization, is displayed. Of the 20 largest metropolitan statistical areas, Boston enjoys the highest concentration of endocrinologists at 5.39 per 100,000, while Riverside-San Bernardino, Ca. has the lowest ratio at 0.89. Boston also enjoys the greatest number of pediatric endocrinologists per 100,000 while Oakland and Phoenix have the lowest ratios for pediatric endocrinologists.
Table 6 Endocrinologists per 100,000 Population
20 Largest MSAs
MSA Population Pediatric Non-Pediatric TotalHMO
PenetrationLos Angeles-Long Beach, CA 9,180,255 0.29 1.81 2.10 56.4%New York City 8,546,786 0.76 2.94 3.70 33.4%Chicago 7,854,558 0.27 1.67 1.94 24.5%Philadelphia 4,916,192 0.41 1.95 2.36 49.0%Detroit 4,770,489 0.19 1.09 1.28 28.5%Washington, DC 4,683,894 0.60 3.27 3.86 35.6%Boston 4,159,286 0.96 4.40 5.39 37.8%Houston 3,973,964 0.23 1.16 1.38 26.7%Atlanta 3,805,402 0.24 1.42 1.66 29.3%Dallas 3,290,011 0.21 1.19 1.40 18.3%Riverside-San Bernadino, CA 3,161,545 0.16 0.73 0.89 53.2%Phoenix-Mesa, AZ 3,034,730 0.13 1.05 1.19 34.1%San Diego 2,862,167 0.24 1.82 2.06 48.2%Minneapolis-St. Paul 2,846,974 0.18 1.62 1.79 37.8%Orange County, CA 2,750,079 0.25 1.53 1.78 45.9%Nassau-Suffolk Counties, NY 2,678,377 1.19 3.14 4.33 38.0%St. Louis 2,599,580 0.27 1.23 1.50 39.5%Baltimore 2,477,762 0.32 1.17 1.49 40.8%Oakland 2,396,765 0.13 1.34 1.46 67.1%Seattle-Bellevue-Everett, WA 2,336,471 0.17 2.23 2.40 19.7%
Endocrinologists Per 100k Population
The Lewin Group, Inc. 8 265991

Workforce Study of Endocrinologists
Tables 7 and 8 present the number of endocrinologists per 100,000 for the 20 MSAs with the lowest and highest ratios, respectively. The Dallas-Fort Worth and Austin-San Marcos areas of Texas would appear to be areas of opportunity for endocrinologists.
Table 7 20 MSAs with the Lowest Concentrations of Endocrinologists
MSA Population Pediatric Non-Pediatric TotalHMO
PenetrationFort Worth-Arlington, TX 1,617,803 0.12 0.49 0.62 31.0%Austin-San Marcos, TX 1,132,973 0.09 0.62 0.71 21.6%Norfolk-Virginia Beach-Newport News, VA 1,554,374 0.13 0.58 0.71 29.6%Las Vegas 1,393,611 0.00 0.79 0.79 26.2%Riverside-San Bernadino, CA 3,161,545 0.16 0.73 0.89 53.2%Orlando 1,571,854 0.25 0.64 0.89 37.5%Grand Rapids, MI 1,049,059 0.29 0.67 0.95 31.6%Phoenix-Mesa, AZ 3,034,730 0.13 1.05 1.19 34.1%Salt Lake City-Ogden, UT 1,309,170 0.23 0.99 1.22 33.4%Fort Lauderdale 1,538,042 0.20 1.04 1.24 36.5%Detroit 4,770,489 0.19 1.09 1.28 28.5%Houston 3,973,964 0.23 1.16 1.38 26.7%Milwaukee 1,438,313 0.21 1.18 1.39 41.4%Dallas 3,290,011 0.21 1.19 1.40 18.3%Monmouth-Ocean, NJ 1,100,731 0.36 1.09 1.45 30.8%Oakland 2,396,765 0.13 1.34 1.46 67.1%Charlotte-Gastonia-Rock Hill, NC-SC 1,410,540 0.35 1.13 1.49 21.4%Tampa-St. Petersburg-Clearwater, FL 2,283,594 0.22 1.27 1.49 37.2%West Palm Beach-Boca Raton, FL 1,071,902 0.09 1.40 1.49 36.5%Baltimore 2,477,762 0.32 1.17 1.49 40.8%
Endocrinologists Per 100k Population
Table 8 20 MSAs with the Highest Concentration
MSA Population Pediatric Non-Pediatric TotalHMO
PenetrationBoston 4,159,286 0.96 4.40 5.39 37.8%San Francisco 1,675,185 0.78 3.82 4.60 66.9%Raleigh-Durham-Chapel Hill, NC 1,101,470 1.18 3.18 4.36 24.5%Nassau-Suffolk Counties, NY 2,678,377 1.19 3.14 4.33 38.0%Washington, DC 4,683,894 0.60 3.27 3.86 35.6%New York City 8,546,786 0.76 2.94 3.70 33.4%Hartford 1,250,000 0.32 3.36 3.68 41.5%Indianapolis 1,526,061 0.79 2.49 3.28 22.9%Newark, NJ 1,949,556 0.51 2.56 3.08 25.0%San Antonio 1,554,852 0.13 2.64 2.77 23.8%Nashville 1,170,028 0.34 2.39 2.73 39.8%New Orleans 1,297,554 0.46 2.23 2.70 26.1%Pittsburgh 2,324,660 0.69 1.98 2.67 34.2%Middlesex-Somerset-Hunterdon, NJ 1,134,947 0.18 2.38 2.56 29.5%Portland, OR 1,846,177 0.54 2.00 2.55 49.0%Bergen-Passaic, NJ 1,384,850 0.51 2.02 2.53 24.8%Miami 1,982,883 0.66 1.82 2.47 56.5%Seattle-Bellevue-Everett, WA 2,336,471 0.17 2.23 2.40 19.7%Providence 1,300,000 0.38 2.00 2.38 41.8%Philadelphia 4,916,192 0.41 1.95 2.36 49.0%
Endocrinologists Per 100k Population
The Lewin Group, Inc. 9 265991

Workforce Study of Endocrinologists
Finally, the following figure summarizes the geographic distribution of endocrinologists across the United States. Areas of highest concentration are in New England, Florida, and along the coast of California. Areas of lowest concentration include the Central and Mountain states.
Figure 4 Concentration of Endocrinologists Across the U.S.
0.0 - 0.20.2 - 0.40.4 - 1.01.0 - 3.03.0 - 37.5
3. SUPPLY AND DEMAND ISSUES In Section 3.1, we briefly summarize our methods for projecting the supply of and demand for the services of endocrinologists. Next, in Section 3.2, we consider factors affecting supply. In particular, we examine the number and fill rate of fellowship positions, and trends in subspecialization among residents in internal medicine. We also consider trends in retirement and withdrawal from the labor force. In Section 3.3, we consider factors affecting demand. Section 3.3.1 analyzes estimates of the current services for which endocrinologists receive reimbursement, how they have changed over time, and the share of other providers of the services with whom endocrinologists may compete. Section 3.3.2 examines trends in population growth. Section 3.3.3 examines the trends in managed care both across the country and over time. Section 3.3.4 presents econometric (statistical) estimates of factors affecting the demand for the services of endocrinologists, including managed care, household income, and insurance. Section 3.3.5 presents a “benchmark” estimate of the demand for endocrinologists, using a Kaiser Permanente staff model HMO plan as a benchmark. Finally, Section 3.3.6 presents information on the earnings of endocrinologists compared to other physician specialties.
3.1 Method and Data We approach the analysis of supply and demand using a number of different methods and data sources. We do this for two (related) reasons. First, the data for the analysis of supply and, especially, demand for physician specialties, particularly the smaller specialties, is less than abundant. This is unfortunately the case, also, for endocrinology. We attempt to push the available empirical data to the greatest extent possible in our analyses, although the data is less
The Lewin Group, Inc. 10 265991

Workforce Study of Endocrinologists
than perfect for any particular approach. However, it does allow us to pursue a number of alternative approaches, albeit imperfectly. Second, we believe that the alternative approaches are, in a sense, quite complementary to the overall goals of the analysis. Use of different methods and data sources, none perfect in its own right, provides a test of how robust the estimates are and how sensitive they are to data and method. To the extent that the alternatives tend to converge to similar conclusions, they provide greater confidence in the conclusion. To the extent that they do not, it provides a sense of the degree of uncertainty associated with any single estimate. A major source of information was our Technical Advisory Panel (TAP) chaired by Dr. Helena Rodbard.6 The TAP was a source of institutional and clinical information relevant to the endocrinology physician workforce. Moreover, the TAP’s opinion and judgment of the current state of the health care market for the services of endocrinologists, its future state, and factors affecting it were useful and were integrated with objective sources of data. Appendix A summarizes some of the insights provided by the panel with regard to issues that are a matter of informed judgment. The following table provides a brief overview of the methods and data sources used in the analysis of supply and demand.
Table 9 Methods and Data Sources Used in Analysis of Supply and Demand
Supply Method Description Data Sources Inventory and Fellowship Model
Ages existing workforce using mortality and retirement rates. Adds new entrants as a function of fellowship positions and fill rates. Models pediatric and adult endocrinologists separately.
• AMA Masterfile • ACGME data on residency
/fellowships positions • Fellowship program director’s
survey • ABIM (NaSGIM) and ABP • Roehrig and Janyan (1986)
Demand Population ratio Projects demand for physicians as a function of
population. Demand increases with population growth, other things being equal, but is adjusted for the effects of managed care growth, insurance coverage, household income and other providers.
• Area Resource File • AMA masterfile • Census • National Ambulatory Medical
Care Survey
6 The TAP members were Drs. William F. Young, Stephen F. Hodgson, Mark Molitch, Mary Lee Vance, Steven M.
Petak, Wayman W. Cheatam, Richard F. Spark, Gerald Bernstein, Francine Kaufman, and Hossein Gharib. They are relieved of any responsibility for how we interpreted and applied their insights.
The Lewin Group, Inc. 11 265991

Workforce Study of Endocrinologists
Table 9 Methods and Data Sources Used in Analysis of Supply and Demand, continued
Demand Econometric Model of Demand
Under the hypothesis that endocrinologists will, at the margin, migrate toward areas of high demand for their services and away from areas of low demand, this statistical model relates the geographic distribution of endocrinologists to factors affecting demand, such as the HMO penetration rate, the proportion of the population insured, and other factors.
• AMA masterfile • Census • Interstudy Competitive Edge • Area Resource File
Epidemiology-Based Estimates
Office visits and, in some cases, procedures are tabulated by disease category. Implied demand is estimated based on time required to provide the services. Future demand is projected as function of growth/decline in incidence/prevalence and in competing providers.
• HCFA BMAD files • National Ambulatory Care
Survey
Benchmark estimate Ratio of endocrinologists to covered lives in a closed care integrated care delivery system, such as a staff model HMO, is calculated. After adjusting for differences in the age distribution between closed beneficiary population and the US population, the “benchmark” estimate is project to the US population as a whole. Estimate is interpreted as the demand for Endocrinology services under the same economic conditions and care quality provided in the closed population.
• Kaiser Permanente enrollment and provider data
• Census
The primary demand model is the population ratio model, augmented by estimates of the effect of managed care, income, insurance and other providers derived from the econometric model. The other methods of estimating current and future demand supplement this model. The supply model and the population-driven demand model form a system from which future projections are obtained. Section 4 of this paper will report projections using the supply and demand models.
3.2 Supply Issues
3.2.1 Trends in Residencies and Fellowships The most important factor affecting the supply of endocrinologists is the number completing fellowships in endocrinology each year. To estimate future supply, it is important to determine how many enter the endocrinology workforce from fellowship programs each year. This will depend not only on the positions and fill rates, but also on the lengths of the programs. According to the Accreditation Council for Graduate Medical Education (ACGME), there were 457 adult endocrinology fellowship positions in 132 programs offered in 1999. According to
The Lewin Group, Inc. 12 265991

Workforce Study of Endocrinologists
NaSGIM, there were 393 fellows enrolled in endocrinology in 1998-1999, a fill rate of about 86%. ACGME also reports that there were 143 positions in pediatric endocrinology in 1999 and, according to the American Board of Pediatrics, there were 115 fellows enrolled in pediatric endocrinology in 1998-1999, for a fill rate of 80%. Using our supply model, we estimate that about 171 fellows in adult endocrinology and about 37 fellows in pediatric endocrinology enter the market each year. An important factor in determining how many enrolled adult endocrinology fellows there will be in the future is the number of third year residents in internal medicine. As Figure 5 indicates, the number of third year IM residents has been growing over time. From about 4,000 in 1976-1977, the number has grown to over 7,000 in 1998-1999.
Figure 5 Third Year IM Residents
However, the rate and number at which IM residents continue into a subspecialty, such as endocrinology, has been declining. This is indicated in Table 10.
Table 10 IM Residents Continuing into Subspecialty Fellowship Programs
Year IM Residents Completing Training
First-year IM Subspecialty Fellows
IM Subspecialization Rate
1978 4547 2965 65.2% 1984 5559 3028 54.5% 1992 5936 3497 58.9% 1995 6306 3107 49.3% 1997 6920 2696 39.0%
The Lewin Group, Inc. 13 265991

Workforce Study of Endocrinologists
In fact, the five-year trend in enrollments is negative for all the major (traditional) IM subspecialties, except gerontology and nephrology, as shown in Table 11. (Note that these are total enrollments, not simply first year.)
Table 11 Trends in Total Fellowship Enrollment for Traditional IM Subspecialties
Subspecialty 94/95 95/96 96/97 97/98 98/99 Annual Change
5-year Change
Cardiology 2657 2532 2363 2238 2149 -4.2% -19.1% Gastroenterology 1189 1128 1026 901 938 -4.7% -21.1% Pulmonary or CCM 1360 1320 1228 1189 1183 -2.8% -13.0% Nephrology 670 636 634 658 676 0.2% 0.9% Endocrinology 459 435 433 410 393 -3.1% -14.4% Hematology or Oncology 1226 1185 1105 1091 1077 -2.6% -12.2% Infectious Diseases 688 672 612 598 593 -3.0% -13.8% Rheumatology or A&I 330 290 270 261 278 -3.4% -15.8% Geriatrics 185 210 242 278 323 11.1% 74.6%
Total 8764 8408 7913 7624 7610 -2.8% -13.2% Over the period, endocrinology has experienced about a 14% decline in total enrollment, or an annual rate of decline of about 3% per year. This is close to the overall average of the subspecialties of about a 13% total decline. Table 12 shows the change in new (first year) enrollments between 1995 and 1997 for the IM subspecialties. They are consistent with the decline in total enrollments, and indicate about a 16% decline in endocrinology, which is consistent with the average 13% decline over all of the major subspecialties. Nephrology experienced the smallest decline over the period.
Table 12 Changes in First Tear Subspecialty Enrollments
1995-1997 Subspecialty 1995 1997 % Change Cardiology 764 680 -11.0% Pulmonology/CCM 514 446 -13.2% Hematology/Oncology 450 408 -9.3% Gastroenterology 440 319 -27.5% Nephrology 316 303 -4.1% Infectious Disease 293 264 -9.9% Endocrinology 191 160 -16.2% Rheumatology 139 116 -16.5%
Total 3107 2696 -13.2% Hence, though there is an increase in the number of IM residents, there has been a distinct downward trend in the number of IM residents who choose to continue with a subspecialty fellowship program after completing their IM residency. The rate of decline in endocrinology enrollment is slightly above the average rate of decline in enrollments across all major subspecialties. International medical school graduates (IMGs) constituted 57% of fellows in adult endocrinology programs in 1999 and about 50% of fellows in pediatric endocrinology programs.
The Lewin Group, Inc. 14 265991

Workforce Study of Endocrinologists
An important “supply” issue is the proportion of IMG fellows who remain in the United States after graduation and practice. While we do not have detailed information concerning fellows in endocrinology, per se, about 50% of IMGs are, in fact, United States citizens or have permanent residency status in the United States, across all graduate medical education programs. Only about 30% of IMGs are in the United States with J-1 /J-2 visa status.7 Unless a waiver is granted, those who have J-1/J-2 visas to attend residency or fellowship programs in the United States must leave the U.S. for a period of at least two years upon completion of their training. While there is no data on precisely what proportion of IMGs do, in fact, ultimately practice in the United States, the consensus view of experts is that most ultimately do remain in the United States. Based on our discussions with experts at the Bureau of Health Professions (BHPr) and elsewhere, we estimate that at least 80% of IMGs practice in the United States. Hence, most IMGs contribute to supply in the United States. The proportion of endocrinologists who completed training and leave with job offers in hand has remained constant or increased over the last five years. Most fellows are satisfied with the job options available to them after completing training. In 1999, there were 234 first time board examination takers, 169 in Endocrinology, Diabetes and Metabolism and 65 in Pediatric Endocrinology. The following map illustrates the location and number of advertised job opportunities for endocrinologists, taken from the websites of the Endocrine Society and AACE in July 2000.
Figure 6 Advertised Job Opportunities for Endocrinologists
July 2000
4
1 4
1
3
8
4
17
2 2
14
2
4
1
3 in the “Midwest”
13
2
2
2
1
11
1
3
1
4
1
1
1
1
1 2
1
The Lewin Group, Inc. 15 265991
7 Journal of the American Medical Association, September 2000, Appendix 6, Table II, p. 1116.

Workforce Study of Endocrinologists
3.2.2 Retirement Rates A second factor that affects the supply of endocrinologists is the age and rate at which endocrinologists withdraw from practice. We do not have endocrinologist-specific rates. The following figure presents retirement rate patterns across all physicians, conducted in the late 1980’s.8
Figure 7 Retirement Rate Patterns for Physicians
Retirement Rate
0.0000
0.0200
0.0400
0.0600
0.0800
0.1000
30 35 40 45 50 55 60 65 70 75
This pattern of retirement rates suggests that the rate begins to rise when physicians are in their late forties, but begins a more dramatic climb starting at age 59. The rate rises to about eight per cent per year beginning at age 67. At an 8% annual retirement rate, a cohort of practicing physicians is reduced by 50% in about 8 years. In addition, mortality rates begin to become important beyond age 60. Together, retirements and mortality reduce an age cohort of practicing physicians by about 80% through age 75. The combined effect is shown in Figure 8, in the cumulative continuation rate.9
The cumulative rate remains virtually 100% until about age 48, and begins a rapid decline starting at about age 60, reaching 20% at age 75. An important issue is whether events in the healthcare market, coupled with secular trends, have lead to earlier retirements, on average, in recent years. If so, supply would be less than is implied by these rates.
8 Roehrig, CS and Janayan, AM. “Physician Separation Rate Estimation,” unpublished report to the Health
Resources and Services Administration, Vector Research, September 4, 1986. 9 Roehrig, CS and Janayan, AM. “Physician Separation Rate Estimation,” unpublished report to the Health
Resources and Services Administration, Vector Research, September 4, 1986.
The Lewin Group, Inc. 16 265991

Workforce Study of Endocrinologists
Figure 8 Cumulative Continuation for Physician Age Cohorts
Demand Issues
Cumulative Continuation Rate
0%20%40%60%80%
100%120%
< 30 35 40 45 50 55 60 65 70 75
3.3 Demand Issues
3.3.1 Demand for Services In this section, we examine two sources of information regarding the services performed by endocrinologists. From this data, we will obtain insights regarding reimbursement for those services, how demand has changed over time, and providers who, potentially, compete with endocrinologists in providing those services. Medicare Data Data from the Medicare program is limited in that it applies only to Medicare beneficiaries--typically those age 65 or over. But, this is an important population and one that is expected to grow from 14.2% of the population in 2000 to 18.6% of the population by 2020. Moreover, it is a group for which detailed and relatively complete claims data is available. The Medicare BMAD Beneficiary file, which includes data regarding reimbursement for physicians office visits, procedures, and other outpatient services, indicates that while total Medicare Part B reimbursements declined by 1.46% across all part B providers between 1995 and 1998, it increased slightly, by 0.4%, for endocrinologists.10
10 Dollar values for both 1995 and 1998 are reported in 1998 dollars.
The Lewin Group, Inc. 17 265991

Workforce Study of Endocrinologists
Table 13 Reimbursement for Medicare Part B Services
1995-1998 Comparison Medicare Part B
Reimbursement Endocrinology
Reimbursement As Share of Part B Total
1995 $ 46,355,712,108 $ 148,911,501 0.32% 1998 $ 44,367,066,279 $ 150,711,104 0.34%
Change -1.46% $ +0.40% +5.74% In Table 14, we compare the dollar volumes of the top procedures billed by endocrinologists in 1995 and 1998. The “top” procedures or services are defined as those that account for the highest dollar volume of reimbursements to endocrinologists. The dollar volume and the share they represent of total reimbursements of endocrinologists are shown in the table. Office visits are, of course, the most important reimbursement service. Office visits represented about 29.4% of all Part B reimbursements to endocrinologists in 1995 and 32.8% in 1998. Total dollar volume grew by almost 24% and its share grew by about 12% of the period. The service that grew the most over the period was “Dual energy X-ray study”(DEXA study) which grew from $1.1 million to $4.5 million, a growth of over 400% and a growth in its share of 268%.11 This suggests that osteoporosis may be an area of significant growth for endocrinologists as the population ages. There were no procedures or services that suffered a large, absolute dollar decline over the period. “Subsequent hospital care” suffered a decline in its share, bur actually increased in dollar volume. The largest absolute dollar decline was “Assay thyroid stimulating hormone”, “initial hospital care” and “follow-up in-patient consult.
Table 14 Top Reimbursement Services and Procedures for
Endocrinologists by Dollar Volume 1995 and 1998
HCPCS Procedure Code
MedicareReimbursement
1995% of 1995
Total
MedicareReimbursement
1998% of 1998
Total% Changein Share
Office/outpatient visit, est 39,912,126$ 29.37% 49,446,305$ 32.81% 11.72%Subsequent hospital care 26,853,997$ 19.76% 27,602,371$ 18.31% -7.31%Office consultation 8,157,651$ 6.00% 10,416,608$ 6.91% 15.15%Initial inpatient consult 8,846,257$ 6.51% 10,150,167$ 6.73% 3.47%Initial hospital care 4,905,944$ 3.61% 4,692,793$ 3.11% -13.74%Dual energy x-ray study 1,113,456$ 0.82% 4,551,704$ 3.02% 268.63%Office/outpatient visit, new 2,735,961$ 2.01% 3,009,788$ 2.00% -0.80%Glycated hemoglobin test 2,563,036$ 1.89% 2,917,063$ 1.94% 2.63%Thyroid panel w/TSH 2,622,266$ 1.93% 2,592,287$ 1.72% -10.85%Assay thyroid stim hormone 2,273,161$ 1.67% 1,989,170$ 1.32% -21.09%Hospital discharge day 1,753,476$ 1.29% 1,806,483$ 1.20% -7.10%Nursing facility care,subseq 1,427,019$ 1.05% 1,803,719$ 1.20% 13.98%Follow-up inpatient consult 2,024,267$ 1.49% 1,757,242$ 1.17% -21.72%Drawing blood for specimen 1,660,085$ 1.22% 1,677,514$ 1.11% -8.88%Lipid panel 1,283,228$ 0.94% 1,576,860$ 1.05% 10.81%
11 In part, this may be due to the Health Care Financing Administration’s recognition of this procedure for billing purposes.
The Lewin Group, Inc. 18 265991

Workforce Study of Endocrinologists
Table 14a provides the same comparison, but is based on claims volume rather than dollar volume. The charts are generally consistent. Note that the number of glucose blood tests roughly doubled between the two periods, while “reagent strip/blood glucose” procedures declined by 50%, suggesting a substitution in preferred practice and technology. Procedures specifically associated with diseases of the thyroid appear to have dropped between the two periods.
Table 14a Top Reimbursement Services and Procedures
Endocrinologists by Claims Volume 1995 and 1998
HCPCS Procedure Code1995 Medicare
Claims% of 1995
Total1998 Medicare
Claims% of 1998
Total% Change in Share
Office/outpatient visit, est 1,439,796 24.26% 1,550,927 25.40% 4.69%Subsequent hospital care 819,326 13.80% 731,427 11.98% -13.24%Drawing blood for specimen 582,897 9.82% 593,468 9.72% -1.05%Glycated hemoglobin test 201,456 3.39% 244,663 4.01% 18.03%Assay quantitative, glucose 156,722 2.64% 154,740 2.53% -4.04%Glucose blood test 64,406 1.09% 146,727 2.40% 121.40%Lipid panel 74,545 1.26% 124,119 2.03% 61.81%Automated hemogram 158,035 2.66% 121,090 1.98% -25.54%Office consultation 97,570 1.64% 108,279 1.77% 7.85%Initial inpatient consult 100,366 1.69% 101,213 1.66% -2.00%Assay thyroid stim hormone 104,314 1.76% 101,024 1.65% -5.88%Influenza immunization 84,782 1.43% 85,333 1.40% -2.18%Comprehen metabolic panel -- -- 81,217 1.33% --Admin influenza virus vac 76,052 1.28% 74,169 1.21% -5.22%Reagent strip/blood glucose 137,478 2.32% 72,960 1.19% -48.42%
Finally, Table 15 presents the procedures which, among all procedures performed by endocrinologists, constitute the procedures for which the endocrinologists’ share is the highest. Note that other providers may, in fact, perform a higher share of the total volume for that procedure. However, this will be a procedure for which the endocrinologists share is high, compared to other procedures endocrinologists perform. Note, also, that they are not necessarily those procedures which provide endocrinologists with their largest shares of their total reimbursement. Other providers who perform a large share of the procedures are also shown.
The Lewin Group, Inc. 19 265991

Workforce Study of Endocrinologists
Table 15 Endocrinologist Services for which Share is High
HCPCS Procedure Code Endocrinology CardiologyGeneral Practice
Family Practice
Internal Medicine
Clinical Laboratory
Glycated protein 19.14% 4.08% 4.41% 9.71% 31.65% 26.00%Reagent strip/blood glucose 8.89% 1.69% 5.83% 29.77% 37.21% 5.67%Glucose blood test 7.55% 1.83% 8.39% 24.10% 36.24% 13.79%Total assay, TT-3 6.50% 2.81% 1.13% 2.72% 10.19% 71.86%Dual energy x-ray study 6.14% 0.92% 2.13% 6.02% 22.59% 0.04%Assay, free thyroxine 5.50% 2.78% 0.82% 6.17% 19.65% 57.20%Glycated hemoglobin test 5.25% 0.88% 0.79% 7.76% 15.56% 64.90%Thyroid panel w/TSH 3.19% 3.04% 1.33% 5.22% 14.41% 67.89%Assay quantitative, glucose 2.86% 1.75% 3.98% 17.66% 20.08% 47.35%Assay thyroid stim hormone 1.88% 1.33% 0.75% 7.11% 15.88% 66.84%Assay, total thyroxine 1.65% 1.82% 0.75% 4.82% 11.88% 73.98%Hepatic function panel 1.46% 4.15% 1.00% 8.64% 16.95% 56.91%Blood lipoprotein assay 1.44% 5.21% 1.13% 5.80% 15.64% 66.42%Lipid panel 1.37% 4.42% 1.29% 9.72% 20.00% 57.41%Drawing blood for specimen 1.11% 4.41% 2.57% 15.17% 23.63% 35.49%13-18 blood/urine tests 1.03% 1.89% 1.01% 4.59% 13.23% 64.68%
The procedure for which endocrinologists’ share is highest, among all procedures which endocrinologists perform, is a laboratory test for glycated protein. Internal medicine specialists, however, perform the largest share of this procedure. In fact, IM specialists are the largest physician provider of all of the procedures for which endocrinologists’ share is significant. This is true for two reasons. First, almost all endocrinologists are also board certified in internal medicine. Hence, clinical practice areas naturally overlap. Second, there are significantly more IM specialists than endocrinologists, or almost any other specialty. Hence, by sheer numbers, IM specialists will be the dominant specialist in almost any area of clinical practice they conduct. National Ambulatory Medical Care Survey (NAMCS) The NAMCS data is more general than Medicare in that it includes all patients, not just those that are eligible for Medicare. It is a survey that is based on a sample of providers. It captures office visits by provider type and, most importantly, reason for visit. Moreover, it has weights which permit generalization to the U.S. population. A weakness of the data, however, is that there are very few endocrinologists in the survey.12 We analyzed NAMCS data from 1993 through 1998. Data beyond 1998 is not yet available. Because few endocrinologists are captured in the survey each year, our analysis compares two three-year periods: 1993, 1994, and 1995 are compared to 1996, 1997, and 1998. Combining the data into two three-year periods will improve the precision relative to annual comparisons. This data source indicates that office visits to endocrinologists increased substantially between the two periods. There were more than twice as many office visits to endocrinologists in the three-year period 1996-1998 compared to the earlier three-year period, 1993-1995. This is consistent with the direction of change indicated by the more precise Medicare data, which
12 Because it is a random sample, the results for endocrinologists will be “unbiased” in the
statistical sense of that term. However, because there are relatively few endocrinologists, the sampling variance may be high and the results imprecise.
The Lewin Group, Inc. 20 265991

Workforce Study of Endocrinologists
suggested about a 25% increase in office visits to endocrinologists between 1995 and 1998. Hence, both data sources are consistent with a qualitatively similar story that the demand for the services of endocrinologists has increased over the 1990s. We examine, first, the distribution of office visits by reason for visit. In the period 1996-1998, the reason for visit for slightly more than 6% of office visits was “glucose level determination.” Unfortunately, no visits were reported for this reason in the 1993-1995 periods. To make the comparisons more useful, we have combined the reported reasons “glucose level determination” and “diabetes mellitus” into one reason “diabetes mellitus” under the assumption that this distinction in reason for visit was not made in the 1993-1995 period. Figures 9 and 10 show the distribution of visit reasons for the two periods, while Figure 11 shows changes in the distribution between the two periods.
Figure 9 Distribution of Office Visits to Endocrinologists by Reason
Percentages: 1993-1995
What Endocrinologists Did Most in 1993-1995
0% 2% 4% 6% 8% 10% 12% 14% 16%
Diseases of the Thyroid
Diabetes Related Visits
Weight Gain
Tiredness,Exhaustion
General Medical Examinations
Prenatal Examination
Knee Pain
Back Pain
Cough
Injections
General Weakness
The Lewin Group, Inc. 21 265991

Workforce Study of Endocrinologists
Figure 10 Distribution of Office Visits to Endocrinologists By Reason
1996-1998
What Endocrinologists Did Most in 1996-1998
0% 5% 10% 15% 20% 25%
Diabetes Related Visits
Diseases of the Thyroid
Tiredness,Exhaustion
General Medical Examinations
Other Test Results
Diet and Nutritional Counseling
Back Pain
Other Blood Test
Cough
Progress Visit
Medication
It is interesting that “diseases of thyroid” was the most frequent reason for visit over the period 1993-1995, but that “diabetes related visits” was the most frequent reason for visit, by a substantial margin, in the 1996-1998 period. Figure 11 shows the percentage point change between the two periods in the distribution proportions (shares) of reasons for visits. Again, we observe that perhaps the most interesting change is the decline in the proportions of visits for disease of the thyroid, and the increase in the proportion of visits for diabetes mellitus.13
Figure 11 Changes in the Distribution of Reasons for Endocrinologist Office Visits
1993-1995 Compared to 1996-1998 1993-1995,1996-1998 Percentage Change in What Endocrinologists Do Most
-10%
-8%
-6%
-4%
-2%
0%
2%
4%
6%
8%
Diabetes Related V isits
Diseases of the Thyroid
Tiredness,Exhaustion
General Medical Examinations
Other Test Results
Diet and Nutrit ional Counseling
Back Pain
Other Blood Test
Cough
Progress Vis it
13 Recall, however, that we have combined “glucose level determination” with diabetes as a
reason for visit in the latter period. In the 1993-1995 period, “glucose level determination” was not reported as a reason for a visit.
The Lewin Group, Inc. 22 265991

Workforce Study of Endocrinologists
Figures 12 and 13 show, for 1993-1995 and 1996-1998, the number of office visits for selected reasons for both endocrinologists and other major specialties who provide similar services. The specialties shown include endocrinologists (END), internal medicine (IM), general and family practitioners (GP/FP), general surgery (GS), urology (U), and obstetrician and gynecology. The data indicates that there is significant room for growth in the areas where endocrinologists specialize; specifically, diabetes and thyroid problems. Moreover, it also appears that there was a substantial increase in office visits associated with diabetes and that an increasing proportion of these were to endocrinologists.
Figure 12 Office Visits by Specialty and Reason
1993-1995 Number of Visits by Specialty from 1993-1995
( In Hundred Thousands )
0
10
20
30
40
50
60
70
80
90
Diseases of the Thyroid
Weight Gain
Diabetes Related Visits
Other Endocrine, Nutrit ional and Metabolic Diseases
General Weakness
Unpredictable Menstrual Interval
Skin Rash
Tiredness,Exhaustion
Other Blood Test
Edema
ENDIMGP/FPGSUOBG
Figure 13
Office Visits by Specialty and Reason 1996-1998
Number of Visits by Specialty from 1996-1998 ( In Hundreds Thousands )
0
20
40
60
80
100
120
Diseases of the Thyroid
Diabetes Related Vis its
Heart Examination
Tiredness,Exhaustion
Fainting
Other Endocrine, Nutritional and Metabolic Diseases
Other Blood Test
Other Test Results
Benign Neoplasms
ENDIMGP/FPGSUOBG
The Lewin Group, Inc. 23 265991

Workforce Study of Endocrinologists
We note again that endocrinologists’ proportion of total visits for “diseases of the thyroid” was substantially greater in the 1993-1995 time period compared to the 1996-1998 period. Moreover, while the total number of visits for “diseases of the thyroid” was higher in the latter period, the number of visits to endocrinologists for this reason was roughly unchanged. The total number of visits for diabetes-related reasons grew substantially between the two periods, and, according to the data, the number of visits to endocrinologists for this reason more than doubled. Figure 14 shows the change in the share of office visits, by reason, for several types of providers including endocrinologists. The data indicate that the share of visits for “diseases of the thyroid” for family and general practitioners has grown substantially, and largely at the expense of internal medicine and endocrinology specialists. In contrast to “diseases of the thyroid”, endocrinologists share of visits for “diabetes-related” reasons has grown, largely at the expense of the shares of internal medicine specialists and general and family practice physicians.
Figure 14 Change in the Share of Office Visits by Reason
1993-1995 Compared to 1996-1998
1993-1995,1996-1998 Percentage Change in Endocrinologists Share of Services
-40%
-30%
-20%
-10%
0%
10%
20%
30%
Diseases of the ThyroidDiabetes Related VisitsHeart Exam
inationTiredness,ExhaustionFainting
Other Endocrine, Nutritional and Metabolic Diseases
Other Blood TestOther Test ResultsBenign Neoplasm
s
ENDIMFP/GPGSUOBG
In summary, it appears that the services performed by endocrinologists have increased substantially during the 1990’s. Of particular importance is a growth in total number and share of visits for diabetes-related reasons. Further, though our NAMCS data did not include “osteoporosis” as a reason for visit, the significant increase in DEXA studies, revealed in the Medicare data, suggests that it, too, may be an important growth area. Interestingly, it appears that visits for thyroid-related reasons have not grown and, in fact, may have declined.
3.3.2 Population Dynamics A major factor affecting the future demand for health care services is the aging population. In 2000, there were 39.149 million people age 65 or over, constituting about 14.2% of the total population. By 2010, the number over age 65 will increase to 45.501 million, which is about 15.2% of the total population. By 2020, the age 65 or over population will number 60.49 million, or 18.6% of the population.
The Lewin Group, Inc. 24 265991

Workforce Study of Endocrinologists
The following figure shows that trend in population by major age group. We observe that the age 65 and over population and the under 18 population increase over the period, while the 18-64 population declines slightly.
Figure 15 Population Trends
(Millions)
Changes in the Population by Major Age Category
020406080
100120140160180
20002002 200420062008 201020122014 201620182020
Year
POP
<1818-6465+
The overall prevalence of diabetes in the senior population (over age 70) is about 11 per cent.14 The incidence and prevalence of diabetes (Type II) increases with age. About 20% of visits to endocrinologists were for diabetes-related reasons. Because this is one of the primary diseases treated by endocrinologists, the aging population suggests that demand, from this source, is likely to increase over time with the growth in the older population. Other diseases whose incidence increases with age and in which endocrinologists specialize include osteoporosis, hypertension, and obesity. The prevalence of osteoporosis, for example, is over 25% for women age 65 or older.15 With the aging population, the increasing prevalence of these diseases will also increase the demand for the services of endocrinologists. Arguably, however, there may be greater competition from other specialists and generalists in these areas, including especially general internal medicine and gerontology. Of relevance to pediatric endocrinologists is, of course, the population that is under age 18. This population will also be increasing over the next twenty years, but not as dramatically as the population over age 65. In addition, the prevalence of conditions treated by pediatric endocrinologists is increasing the population age 6-19. Over the last twenty years, the proportion of the population, age 6-19, that is characterized as “obese” has increased from just under 5% of 14 National Center for Health Statistics, Health ,United States, 1999. Hyattsville, Md., 1999, p. 89. 15 National Center for Health Statistics, Health ,United States, 1999. Hyattsville, Md., 1999, p. 90.
The Lewin Group, Inc. 25 265991

Workforce Study of Endocrinologists
the population to just over 10% of the population.16 One consequence of this is an increasing incidence of Type 2 diabetes among the youth population.17
3.3.3 Managed Care The conventional wisdom, which we believe is supported by evidence, is that managed care has a negative effect on the overall demand for health care services, as realized by providers, and on the services of physician specialists, in particular.18 Other things being equal, we anticipate a lower demand for the services of physician specialists from a population, the higher the proportion of the population that is covered under a form of managed care and, in particular, health maintenance organizations. Hence, other things being equal, we would expect lower demand for the services of endocrinologists in areas where higher proportions of the population are in HMOs. This does not mean, of course, that the absolute level of demand for endocrinologists’ services will be lower in areas where the HMO proportion is high. It means only that demand is likely to be lower than it otherwise would be. Because there is a greater incentive to control costs and utilization in areas where the overall demand for health care services is high, it is likely that the simple correlation between measures of demand and managed care penetration rates is positive, not negative. Today, there are many different forms of “managed care” with different implications for demand. At one end of the spectrum are preferred provider organizations (PPOs) and point-of-service (POS) plans, which are analogous to discounted fee-for-service plans. At the other end of the spectrum are staff model health maintenance organizations and health maintenance organizations with a closed panel of providers and a rigid “gate-keeper” system. Our measure of managed care is the “HMO penetration rate” which is the proportion of the relevant population that is in a plan with a “gate-keeper”. Coverage for non-emergency services is denied unless the beneficiary receives the approval of the gatekeeper—typically a primary care physician.
Table 16 HMO Penetration Rate: 1996 and 1999
1996 1999 Annual Growth HMO Penetration 22.3% 30.1% 10.0% HMO Medicare Penetration 10.0% 16.5% 16.7% HMO Medicaid Penetration 24.0% 34.5% 12.1%
Table 16 shows the change in the aggregate U.S. HMO penetration rate between 1996 and 1999.19 The HMO penetration rate grew by about 10% annually between 1996 and 1999. The
16 Center for Health Statistics, Health, United States, 2000 with Adolescent Health Chartbook, , Hyattsville, Md.
2000, Tabe 69, p 248. 17 See, for example, Arlan Rosenbloom, MD, Chair; Silva Arslanian, MD; Stuart Brink, MD; Katie Conschafter,
RD, CDE; Kenneth Lee Jones, MD; Georgeanna Klingensmith, MD; Naomi Neufeld, MD; and Neil White, MD, “Consensus Statement: Type 2 Diabetes in Children and Adolescents”, Diabetes Care, vol. 3, no.3, p.381, 2000;
18 See, for example, Weiner, Jonathan P., Dr.PH, “Forecasting the Effects of Health Reform on US Physician Workforce Requirement,” Journal of the American Medical Association, July 20, 1994, v. 272, no.3.
19 The HMO penetration rate data is taken from Interstudy Competitive Edge, various editions.
The Lewin Group, Inc. 26 265991

Workforce Study of Endocrinologists
Medicare HMO rate grew by almost 17% over the same period, but is only about half of the level of the privately insured HMO penetration rate. The HMO rate is highest in the Medicaid population. Figures 16 and 17 depict the HMO penetration rate across the states in 1995 and in 1999, respectively. Note that the 1999 map is significantly darker than the 1995 map, on average.
Figure 16 HMO Penetration Across the U.S.: 1995
0 - 7 8 - 14 15 - 25 26 - 40 41 - 99
Percentage of PopulationEnrolled in HMOs:
Figure 17
HMO Penetration across the U.S.: 1999
0 - 7 8 - 14 15 - 25 26 - 40 41 - 99
Percentage of PopulationEnrolled in HMOs:
The Lewin Group, Inc. 27 265991

Workforce Study of Endocrinologists
Note that, by 1999, virtually all of the Northeast, Florida and California had penetration rates in excess of 26%. California and several Northeast states had rates in excess of 40%. The South, with the exception of Florida, and the Central States have the lowest rates. We refer the reader back to Table 6, where the HMO penetration rate was displayed for the 20 largest MSAs. Oakland and Los Angeles have the highest penetration rates among the 20 largest MSAs, while Dallas, Texas and Seattle, Washington have the lowest. Note, from Table 6, that MSAs with the highest concentrations of endocrinologists also appear to be areas of high HMO penetration rates. This illustrates the point that, while HMO penetration has a negative effect on demand, this may not be apparent in the data without taking into consideration other factors affecting demand. The most common method by which HMOs reimburse specialists is still fee-for-service or discounted fee-for-service, at least through 1996. HMOs appear to compensate endocrinologists in much the same way as they compensate other specialists, as shown in Table 17.20
Table 17 HMO Methods of Compensating Specialists (1996) Endocrinology All Specialties FFS or Discounted FFS 46.5% 46.0% Capitation 28.1% 28.6% Relative Value Scale 24.2% 24.5% Salary 1.2% 1.1%
Table 18 shows the proportions of HMOs using alternative types of provider payment methods in 1999.21 Most HMOs use some capitation for compensating both primary care physicians and specialists. However, the plurality of HMOs appears to use fee-for-service exclusively.
Table 18 HMO Methods of Payment: 1999
Primary Care Specialty Care Method % using (exclusively) % using (exclusively) Capitation 79.2% (39.6%) 64.2% (25.6%) Fee for Service 47.5% (26.7%) 60.8% (38.2%) Relative Value Scale 20% (17.2%) 23.5% (9.2%) Salary 8.3% (0.8%) 7.6% (0.0%)
Disease management represents a potential opportunity for some specialties to increase the demand for their services within a managed care environment. If the specialist can convince the HMO that their management of patients with a particular disease will result in lower costs and better outcomes, the demand for that specialty’s services will increase. The following table reports the results of HMO’s perceptions of disease management programs, by disease. Approximately half of HMOs offer disease management programs for diabetes. Moreover, those 20 The data is from Interstudy Competitive Edge report, 1996. 21 Data is from Interstudy Competitive Edge report, 1999.
The Lewin Group, Inc. 28 265991

Workforce Study of Endocrinologists
HMOs that offer disease management programs report improvements in outcomes and processes, and over 40% report cost savings.
Table 19 HMO’s Perceptions of Disease Management Programs
Disease Outcomes Processes CostsAsthma 57.4 83.1 88.6 26.7High Risk Pregnancy 50.8 57.1 86.1 57.1Diabetes 50.0 79.0 90.0 42.1Congestive Heart Failure 23.3 73.3 85.7 35.7Breast Cancer 20.5 68.8 81.8 30.8High Cholesterol 17.4 53.8 68.8 63.0Depression 17.4 56.5 54.2 40.0HIV/AIDS 15.1 64.0 68.0 62.5High Blood Pressure 13.2 56.0 56.0 56.0Peptic Ulcer 8.9 16.7 30.8 84.4Prostate Cancer 5.4 40.0 53.8 31.8Osteoporosis 3.9 0.0 0.0 76.2Allergic Rhinitis 2.3 18.2 22.2 10.0Arthritis 1.9 0.0 -- 10.0Weighted Average 65.3 77.1 44.3
% offering DM Programs
% Reporting Improvements in
Source: 1997 Interstudy Competitive Edge
Programs which demonstrate the efficacy and efficiency of management of patients with diabetes by endocrinologists, or by other specialists using protocols developed by endocrinologists, have the potential for significantly increasing the demand for the services of endocrinologists in a managed care environment. The hypothesis is that endocrinologists, using a program of diabetes management, can improve the health and well-being of beneficiaries who are diabetic while reducing overall treatment costs. Endocrinology specialists will compete with other practitioners, including primary care practitioners, for the role of disease manager for patients with diabetes. Endocrinologists have the potential for becoming the recognized provider of choice for management of diabetes. It is crucial that endocrinologists are able to demonstrate empirically the value of management of diabetes patients by endocrinologists.22
22 Some recent studies have provided evidence consistent with the hypothesis that endocrinologists can improve the
management of patients with diabetes, compared to care provided by primary care practitioners. C.S. Levatan et al, reporting in the November 1999 issue of Diabetes Care, had a significantly lower readmission rate for diabetic ketoacidosis (DKA) compared to patients under treatment by generalists. Further, earlier studies by the same authors suggested shorter lengths of stay for patients admitted for diabetes-related problems when there was consultation with an endocrinologist-led team.
The Lewin Group, Inc. 29 265991

Workforce Study of Endocrinologists
3.3.4 Econometric Estimates of the Effects of Managed Care and Other Factors Affecting Demand
The previous section considered the prevalence of managed care, but did not indicate its effect on the demand for the services of endocrinology. As noted in the previous section, we hypothesize that managed care has a negative effect on demand. However, this relationship will be observed only “if other factors remain the same.” That is, demand will be lower than it would otherwise be, due to increased managed care, but the prevalence of managed care is likely to be greater in areas in which demand is high due to other factors. Hence, a method which attempts to account for all or most of the factors affecting demand will have to isolate the effects of managed care on demand. Estimating the effect of factors affecting the demand for a particular physician specialty, particularly the smaller specialties, is typically stymied by a paucity of data regarding the quantity of services provided. Here, we use an alternative, stylized approach to demand that avoids this difficulty. We estimate a model of the “demand” for endocrinologists using data on the geographic distribution of endocrinologists across the United States. The fundamental hypothesis underlying the estimates is that, at the margin, endocrinologists will migrate into areas where demand is relatively strong and away from areas where demand is relatively weak. In effect, we use “number of physicians” as a proxy for services provided. Hence, using this theory, we attempt to explain the variation in the endocrinologist to population ratio across various geographical areas by the variation in factors affecting the demand for services. Based on this relationship, we infer the effects that various factors, such as insurance coverage, managed care, and household income, have on the demand for the services of endocrinologists. The model is of the general form:
),,,,(/ OSPCMCUIIfpopE d = where the population ratio of endocrinologists, interpreted as “demand”, is a function of per capita income in the area (I), the percent uninsured (UI), the managed care (HMO) penetration rate (MC), the number of primary care physicians in the area (PC), and the number of selected other specialties in the area (OS). Data Managed care data is from the Interstudy Competitive Edge Part III report from July 1999. Data included estimates of total population, total HMO enrollment, HMO Medicare and Medicaid enrollment, non-HMO Medicare and Medicaid enrollment, and uninsured population for 306 Metropolitan Statistical Areas (MSAs). Population and Median Household Income are from the 1996 Census estimates, updated through the Current Population Survey, as they appeared in the 1999 Area Resource File (ARF), produced by the Health Research and Services Administration (HRSA). Data in the ARF are listed at the FIPS (county) level but are labeled according to MSA as well. Our MSA-level
The Lewin Group, Inc. 30 265991

Workforce Study of Endocrinologists
figures for median household income were calculated by taking an average of incomes for all counties in a given MSA, weighted by the 1996 Census population of that MSA. For populations of general practitioners, general internists, and urologists, we used estimates from the 1995 and 1997 AMA Physician Characteristics and Distribution publications as they appeared in the 1999 ARF. We estimated the change in the number of physicians from 1997 to 1999 using a factor derived from the rate of change from 1995 to 1997. The number and geographic distribution of pediatric and non-pediatric endocrinologists is also from the AMA masterfile, obtained from the AMA for this project. Results We estimated three sets of regressions: one for all endocrinologists, one for pediatric endocrinologists, and one for all non-pediatric endocrinologists. Each model had as its dependent variable the number of (relevant) endocrinologist physicians per 100,000 population by MSA. Independent variables were: • Medicare HMO penetration rates, defined as HMO Medicare enrollment divided by total
Medicare beneficiaries; • Non-Medicare HMO penetration rates, defined as total HMO enrollment divided by total
non-Medicare population; • Percent uninsured population, defined as the number of uninsured persons divided by total
non-Medicare population; • Median Household Income; • General Practitioners per 100,000 population; and • General Internal Medicine physicians per 100,000 population. The dependent variable(s) were the ratio of endocrinologists to population by MSA. Table 20 presents the results when using all endocrinologists.23 The HMO penetration rate for the non-Medicare population has a negative and statistically significant effect on the demand for endocrinologists. The “elasticity” of –0.24 indicates that a 10% increase in the HMO penetration rate results in a 2.4% decline in the demand for endocrinologists. Median income has a positive effect on demand, while the percent of the population that is uninsured has a negative effect. Both estimates, however, are statistically insignificant.
23 The standard way to present regression results is to include the regression coefficient, its standard error or a t-
statistic, and an overall measure of goodness of fit, such as the “”R-square” which indicates the proportion of the variation in the physician-to-population ration that is explained by the regression equation.
The Lewin Group, Inc. 31 265991

Workforce Study of Endocrinologists
Table 20 Factors Affecting Demand
All Endocrinologists Coefficient t Stat Mean Elasticity Intercept -1.3816 -2.278 HMO Penetration for Medicare Population 1.0632 1.879 0.1175 0.0798 HMO Penetration for Non-Medicare Population -1.4070 -3.111 0.2673 -0.2401 % Uninsured Non-Medicare Population -0.1946 -0.140 0.1874 -0.0233 Median Household Income 0.00001105 0.839 35433.77 0.2501 General Practitioners/100K Population 0.0123 2.802 36.4763 0.2870 General Internal Medicine/100K Population 0.0680 30.825 35.2245 1.5286
Mean Physicians per 100K Pop: 1.5663 R Square 0.7858 Adj R-Sq 0.7815 The number of internal medicine practitioners in the area has a strong and positive influence on the demand for the services of endocrinologists, perhaps indicating a complementary relationship. The number of general practitioners also has a positive and statistically significant effect on demand, but the effect is smaller than that of internal medicine specialists. In Table 21, the results for the same model specification are shown, except that the dependent variable is non-pediatric endocrinologists per population. Again, the effect of the non-Medicare managed care penetration rate is negative and statistically significant. A 10% increase in the managed care penetration rate is associated with a 3% decline in the demand for endocrinologists. Interestingly, the Medicare managed care penetration rate has a positive and statistically significant effect on demand. A 10% increase in the Medicare managed care rate is associated with about a 1% increase in demand. The proportion of the population that is uninsured has a negative effect on demand. Though the estimate is not statistically significant, a 10% increase in the uninsured rate is associated with a -0.2% decrease in demand. Household income again has a positive effect on demand. Though not statistically significant, a 10% increase in household income is associated with a 2.7% increase in demand. Both general practice physicians and internal medicine physicians appear to have a positive influence on demand.
The Lewin Group, Inc. 32 265991

Workforce Study of Endocrinologists
Table 21 Factors Affecting Demand
Non-Pediatric Endocrinologists Coefficient t Stat Mean Elasticity Intercept -1.1821 -2.018 HMO Penetration for Medicare Population 1.0925 1.998 0.1175 0.0965 HMO Penetration for Non-Medicare Population -1.5194 -3.478 0.2673 -0.3053 % Uninsured Non-Medicare Population -0.1587 -0.118 0.1874 -0.0224 Median Household Income 0.00000849 0.667 35433.77 0.2263 General Practitioners/100K Population 0.0099 2.326 36.4763 0.2711 General Internal Medicine/100K Population 0.0613 28.764 35.2245 1.6225 Mean Physicians per 100K Pop: 1.5663 R Square 0.7588 Adj R-Sq 0.7539 Table 22 shows the results for pediatric endocrinologists alone. Very few variables are statistically significant for pediatric endocrinologists. The effects of the managed care penetration rate are not statistically significant, for example. We speculate that there are too few pediatric endocrinologists, in general, for this method of estimating demand based on geographic distribution to be applicable. Note that the proportion of the variance explained by the model for pediatric endocrinologists is only about 29%, as measured by the R2, compared to about 75% for the non-pediatric endocrinologists.
Table 22 Factors Affecting Demand for Pediatric Endocrinologists
Coefficient t Stat Mean Elasticity Intercept -0.1996 -1.052 HMO Penetration for Medicare Population -0.0300 -0.170 0.1175 -0.0149 HMO Penetration for Non-Medicare Population 0.1127 0.797 0.2673 0.1276 % Uninsured Non-Medicare Population -0.0333 -0.076 0.1874 -0.0264 Median Household Income 0.00000255 0.619 35433.77 0.3828 General Practitioners/100K Population 0.0024 1.775 36.4763 0.3774 General Internal Medicine/100K Population 0.0067 9.706 35.2245 0.9990 Mean Physicians per 100K Pop: 0.2361 R Square 0.2973 Adj R-Sq 0.2832 Summary and Limitations Using the geographic variation in the physician to population ratio, we are able to estimate the effects that various factors have on the demand for endocrinologists. In particular, we have found that the HMO managed care penetration rate has a negative and statistically significant effect on demand. A 10% increase in the penetration rate is associated with a 3% decline in demand for endocrinologists. There are two areas of caution in these estimates, however. We estimate the results based on a single cross-section. It may be that fixed factors associated with geographic location that are not measured in the regressions affect the cross-sectional variation in both the physician ratio and
The Lewin Group, Inc. 33 265991

Workforce Study of Endocrinologists
some of the explanatory variables. If so, the measured effects may be spurious. The results could be improved if we had data on multiple cross-sections. In this way, we could relate the change in the physician to population ratio in the area to the change in variables such as the managed care penetration rate, reducing the chance that the results are driven by correlation with an omitted factor. Unfortunately, we did not have sufficient data for this type of specification. Second, we base our results on the hypothesis that, at the margin, physicians make location decisions based on demand. This allows us to use the geographic distribution of physicians as a demand proxy. A preferred specification would be estimates based on actual services provided. Data limitations, again, are a major impediment to this approach.
3.3.5 A “Benchmark” Estimate of Current Endocrinologist Clinical Demand An interesting, but controversial, method for estimating the demand for physician specialties under certain stylized conditions is “benchmarking.” In this method, one observes the ratio of physicians in the specialty to population served in a closed population. The particular population represents economic conditions and quality level of care provided under those conditions. Extrapolating the ratio to the entire nation’s population, for example, provides an estimate of the demand for that specialty under the economic conditions and quality of care represented by the “closed” population. This method is used in Weiner (1994) to estimate demand under health care reform and Goodman et al (1996) for HMO, managed care, fee-for-service, and “balanced’ physician supply conditions. Below, we present an estimate of the total demand for office-based practicing endocrinologists for the U.S. as a whole, using as a model, or benchmark, Kaiser Permanente’s Middle Atlantic States health maintenance organization. This is a staff model HMO serving members in Northern Virginia, the District of Columbia, and Maryland. Kaiser is typically considered an HMO that has achieved a reasonable balance between cost-effectiveness and adequate health care. Hence, it represents demand under integrated managed care health system. The use of the benchmarking estimates rest on (at least) four assumptions. First, the “closed” population is receiving all, or almost all, of its actual and contingent care from the panel of physicians and other providers included in the analysis. If there are “leaks”—care provided to members of the population by providers outside of the panel—the estimates will understate demand. Second, the providers included in the “closed panel” are providing care only to the members of the closed population. Third, the “closed” panel is itself in equilibrium. They have the right number and mix of providers for the closed population, given the quality of care planned. Fourth, the closed population is representative, in terms of its health care needs, of the more general population to which an extrapolation is made. Differences in the health care utilization between the “closed” population and the general population that are due to differences in age composition can typically be adjusted for. However, it is more difficult to adjust for differences in the health of the populations within age groups. Such differences may arise, for example, due to “selection” effects if the closed population is formed by a health insurance plan, such as a health maintenance organization.
The Lewin Group, Inc. 34 265991

Workforce Study of Endocrinologists
Current Numbers of Endocrinologists Our data indicate that, as of 1999, there were a total of 3,651 physicians with a specialty of (non-pediatric) endocrinology and 719 pediatric endocrinologists.24 Of these, about 66% of the non-pediatric endocrinologists, or 2410, were in office-based clinical practice while 55.6% of pediatric endocrinologists were in office-based clinical practice. These numbers are consistent with the following physician-population ratios:
Table 23 Endocrinologists per 100,000 U.S. Population
Non-Pediatric Pediatric* Total Clinical Office-Based 0.9 0.15/.58 1.05 Total 1.36 0.27/1.04 1.63
*The first ratio for pediatric endocrinologists is for the total population; the second is for the population age 18 and under.
Estimates from Closed Panel HMOs Weiner (1994) reports that staffing ratios for endocrinologists across a number of HMOs range from 0.6 to 1.0 per 100,000, in 1992. The actual national estimate was 0.8 per 100,000. Kaiser Permanente’s Middle Atlantic States plan has a total of 555,775 members.25 In its panel of providers, it lists five endocrinologists and one pediatric endocrinologist. This implies a ratio of 0.899 for endocrinologists and a ratio of 0.58 for pediatric endocrinologists, within the population of the HMO. To generalize to the entire population, it is necessary to account for differences in the age distribution between the HMO population and the population as a whole. Differences in utilization by age group would imply that the ratio applicable to one population distribution may not be applicable to another. The following table compares the proportions of the population by age group.
Table 24 Population Proportions
Age Group US Population HMO Population 0-18 0.26 0.32 19-64 0.62 0.67 65+ 0.12 0.01
Clearly, the small portion of the older population in the HMO suggests that an extrapolation of an unadjusted ratio in the HMO to the US population will understate demand. For pediatric endocrinologists, no adjustment is necessary if we use the HMO ratio for the 18 and under population.
24 These physicians include those who are board certified and/or fellowship-trained. 25 Data taken from the Kaiser web site, September 2000.
The Lewin Group, Inc. 35 265991

Workforce Study of Endocrinologists
We adjust for the differences in the age distribution by constructing an index of utilization by age group. We use the number of office visits per 1,000 in population within the age group for the HMO to construct the index. Specifically, we calculate:
∑∑
=
iiHMOiHMO
iiHMOiUS
UW
UWI
,,
,,
where “W” represents the population proportion in each of the three age groups (i groups) and U is the respective utilization count, per 1,000, in the age group. The index value, I, provides, for a given total population, the ratio of utilization for a population distributed as the US population is to the utilization for a population distributed as the HMO’s population is distributed. The ratio we calculate is 1.12, indicating that health care utilization will be about 12% greater for a population of a given size if it is distributed by age as the US population is distributed, compared to the HMO population. The higher utilization translates into a greater demand for physicians. Using the HMO as a benchmark, we estimate that the US population would require about 1.0067 (non-pediatric) endocrinologists per 100,000 of population to provide health care services implied by the HMO’s ratio. This is about 2,705 practicing office-based endocrinologists, or about 12.2% more than currently (1999) are practicing. The ratio of pediatric endocrinologists employed by the HMO to the HMO population is 0.595. Applying this benchmark to the US population implies that about 412 pediatric endocrinologists, or about 3% more than we estimate, were in office-based clinical practice as of 1999. Conclusion Using the Kaiser HMO as a benchmark produces a total demand for practitioners that is surprisingly close to the current supply, when we focus on endocrinologists who are in office-based practice. Moreover, the results suggest that under integrated managed care models such as Kaiser, the demand for practicing endocrinologists is about 12% greater than current supply for non-pediatric endocrinologists and about 3% greater for pediatric endocrinologists. This “benchmark” methodology, however, rests on a number of critical assumptions which should be considered in interpreting the results.
3.3.6 Earnings of Endocrinologists The earnings of endocrinologists are not a factor affecting the demand for endocrinologists. Rather, they are the outcome of the demand for and supply of endocrinologists. When demand exceeds supply, we would expect earnings to rise. Conversely when supply exceeds demand, we would anticipate that earnings would begin to fall, or at least not rise as fast as they otherwise might. In general, there is a paucity of data on the earnings of physician specialists, especially the smaller specialists. Below, we piece together some information on median earnings of physicians
The Lewin Group, Inc. 36 265991

Workforce Study of Endocrinologists
in recent periods. The two primary sources for this data are from the American Medical Association’s Socioeconomic Monitoring System (SMS), a survey of non-federal physicians, and the Medical Group Management Association (MGMA) Physician Compensation and Productivity Survey. Table 25 presents median earnings, after expenses but before taxes, of selected non-federal physician specialties from the AMA.26 The data indicate that nominal earnings for all non-federal” physicians grew by about 20% between 1991 and 1997, but that this was approximately the increase in inflation, as measured by the Consumer Price Index, over this period. Hence, real earnings were approximately constant. The earnings of general internal medicine specialists grew by about 27.8%, or less than about 7% after inflation, while all internal medicine specialists’ nominal earnings grew by about the same as nominal earnings of pediatricians, and were roughly constant in real term, that is, after accounting for inflation. The earnings of endocrinologists, and other smaller subspecialties, are not publicly reported in this data. Obstetricians/gynecologists record no nominal growth in earnings over the period, according to the AMA data.
Table 25 Physician Median Earnings from AMA
(thousands)
1991 1995 1996 1997 Percent Change
All phys. $139 $160 $166 $167 +20% GP/FP $98 $124 $130 $132 +34.7% General IM $115 $138 $140 $147 +27.8% IM $125 $150 $150 $150 20% Pediatric $105 $129 $125 $120 20% Ob/Gyn $200 $200 $200 $200 0% Neurology $160 $160 $164 N/A Inflation $1.00 $1.13 $1.16 $1.20 +20%
Table 26 shows earnings for select, non-invasive specialties and endocrinology and metabolism, pediatric endocrinology and reproductive endocrinology, for 1997 and, for most, 1996. This data is from MGMA.27 Endocrinologists’ median earnings in 1997 are about 4% greater than general internal medicine specialists, and about 2% greater than median earnings of internal medicine practitioners who also have a subspecialty, and of rheumatologists. The median earnings of pediatric endocrinologists are about 8% greater than pediatricians. Reproductive endocrinologists’ median earnings are substantially greater than general endocrinologists or pediatric endocrinologists.
26 The data are for non-federal physicians and are taken from Physician Socioeconomic Statistics, Center for Health
Policy Research, American Medical Association, 1999-2000 edition and from Physician Marketplace Statistics, Center for Health Policy Research, American medical Association, 1997, 1996 and 1992. The data from all of these reports is derived from the AMA’s Socioeconomic Monitoring System Survey of Physicians for each respective year: 1998, 1997, 1996 and 1992.
27 The data are taken from Physician Compensation and Production Survey, Medical Group Management Association, 1998 and 1997 Report. The reader is cautioned that the sample sizes are small, particularly for the smaller specialties.
The Lewin Group, Inc. 37 265991

Workforce Study of Endocrinologists
Table 2628 Non-Invasive Physician Specialists Median Earnings
MGMA Estimates (thousands) Year Ped. End. End. Rep. End. Rheum. Hem/Onc Infect.Dis. Geriatrics 1996 $153.9 $145.8 $190.7 $150.6 $125.7 1997 $128.9 $152.3 $207.8 $150.1 $195.0 $158.4 $135.5
Earnings comparisons can be very treacherous. Physicians in private practice typically earn more than those who are salaried, and those who are in large group practices earn more than those who are in solo practice, other things being equal. Further, physicians who work longer hours will typically earn more than those who work shorter hours, other factors held constant. Moreover, physicians who are more experienced—in the age range of 45-60—typically earn more than others. These simple comparisons of median responses from a survey of physicians’ earnings do not adjust for these factors. For these reasons, as well as issues regarding the collection of earnings data in surveys, the estimates should be interpreted cautiously. Table 27 presents some workload and fee measures for internal medicine specialists.29 Total hours of work remained approximately constant throughout the period. Weeks of work (not shown) also remained constant at 48 per year. Patient visits appeared to decline slightly. Offsetting this, however, were modest increases in median first-time visit fees and a more substantial increase in median fees for established patients, calculated in constant 1992 dollars. Hence, the data suggest that, over the period of 1992-1998, changes in nominal earnings were largely due to increased fee rates, and not to increases in patient visits and hours of work.
Table 27 Workload and Fee Measures30
Internal Medicine 1992 1996 1997 1998 Change, 92-98 Total Hours 60 60 60 58 -3.4% Patient Visits 103 95 100 95 -7.8% Fee, first time $100 103.57 $104.35 $102.56 +2.6% Fee, established $42 $49.11 $51.30 $51.28 +22.1%
Finally, a recent survey of practitioners conducted by the Endocrine Society found that the average waiting time for a initial visit for a new patient in 2000 was about 37.3 days for an appointment with an adult endocrinologist and about 44.9 days for a pediatric endocrinologist. The most recent comparison to other specialties is for 1998, from the American Medical Association’s Physician Socioeconomic Statistics.31 For “all physicians” (excluding radiologists, psychiatrists, pathologists and anesthesiologists) average waiting time for an initial visit was 9.5
28 From left to right, the specialties included in the table are Pediatric Endocrinology, Adult Endocrinology,
Reproductive Endocrinology, Rheumatology, Hematology/Oncology, Infectious Diseases, and Geriatrics. 29 This data is taken from AMA’s publication, Physician Marketplace Statistics, editions 1997, 1996, and 1992; and
Physician Socioeconomic Statistics, 1999-2000. 30 Fees are calculated in constant 1992 dollars. Hence, increases shown are real increases. 31 American Medical Association, Physician Socioeconomic Statistics, 1999-2000 Ediition.
The Lewin Group, Inc. 38 265991

Workforce Study of Endocrinologists
days. For general internal medicine, waiting time was 9.9 days, while for neurology and dermatology it was 17.3 and 17 days, respectively. Hence, waiting time for endocrinologists in 2000 was two to three times greater than most other physicians in 1998. Because “waiting time” is one way to ration excess demand, these data are consistent with proposition that there is significant excess demand for endocrinologists in the current market.
4. PROJECTIONS OF THE SUPPLY OF AND DEMAND FOR ENDOCRINOLOGISTS In this section, we use the Endocrinologist Workforce Model to project the supply of and demand for endocrinologists under several sets of assumptions, or “scenarios”. The projections are designed to accomplish three things. First, they are intended to provide concrete examples of what the Workforce Model can do. Second, they are intended to provide some insight into the factors that are likely to have important effects on future demand and supply, as well as factors that may be less important. That is, they are intended to provide a “sensitivity” analysis of factors affecting the future workforce market environment. Third, we intend that the projections provide a realistic assessment of the current and future market demand and supply for endocrinologists over the next twenty years. We recognize that (at least) two major factors affect the forecast accuracy of projections. The model must be able to reflect, accurately, the effect on demand and/or supply of anticipated changes in the health care marketplace. That is, the model must be able to reflect the effects of changes in managed care; growth in insurance coverage and household incomes; the effects of an aging population on demand; and so forth. Second, the “scenarios” considered must capture the future path of variables or factors affecting demand and supply. That is, we must correctly anticipate the growth in managed care, changes in insurance coverage and income growth, changes in “competing” providers and disease incidence, and so forth. The second aspect of forecast accuracy is as much a matter of judgment and, to an extent, serendipity, as it is of science. We draw on an eclectic source of information and judgment, including our TAP members and our own judgment, in formulating some of the scenarios. The first aspect of forecast accuracy depends on the richness of the available data and the appropriateness of methods for applying it to capture the relationship between demand and/or supply and factors such as managed care. It also rests on the assumption that relations measured in the past will be preserved in the future—that is, the measured effects are stable over time. As noted previously, the data available for estimating the effects of factors affecting demand for smaller physician specialties is often less than desired. In Section 3, we described the eclectic sources of data and methods used to develop the relationships in the model.
4.1 Baseline The purpose of this “baseline” scenario is to provide a starting point for further analysis that includes only a most parsimonious set of assumptions. Our “baseline” projection makes what we believe to be a counterfactual assumption that supply and demand were approximately in equilibrium in 1999. We project the future supply of endocrinologists under the assumption that the number of fellowship positions and fill rates will remain at the 1999-2000 levels throughout the projection period, both for adult and pediatric endocrinologists. We assume that 80% of international medical school graduates (IMGs) practice in the United States after completing their fellowship. We further assume that demand is affected and increased only by aggregate
The Lewin Group, Inc. 39 265991

Workforce Study of Endocrinologists
population growth. This means, for example, that the “aging” of the population will have no additional impact on demand.
Table 28 Base Case Assumptions
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice • No change in retirement rates
Demand affected only proportionately with population growth
Figures 18A and 18B shows the Base Case for adult endocrinologists and pediatric endocrinologists, respectively. . For each graph, projected supply, indicated by rectangles is compared to projected demand, indicated by triangles, under the particular assumptions associated with the case. Note that the growth in the supply of endocrinologists—the implications of the current number of fellowship positions and current retirement rates persisting into the future—outstrips the growth in demand that is due only to an increasing population for both adult and pediatric endocrinologists, in the Base Case. The gap between supply and demand, under the Base Case assumptions, is wider for adult endocrinologists. Note that the scales differ for adult and pediatric endocrinologists because of differences in the relative sizes of the specialties.
Figure 18A Base Case: Adult Endocrinologists
Supply and Demand
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Base Case (END)
Demand
Base Case (END)
The Lewin Group, Inc. 40 265991

Workforce Study of Endocrinologists
Figure 18B Base Case: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Base Case (PDE)Demand
Base Case (PDE)
4.2 Case 1: Overall Assessment
In Case 1, we begin to incorporate the conditions which, we believe, represents the best overall assessment of current and projected future supply and demand for endocrinologists. A major assumption in the Base Case is that the market was in equilibrium in 1999. That is, demand was about equal to supply. The evidence we reviewed in section 3 of this report, and the perspective of the TAP, suggests that demand is greater than supply in the current market. That is, the current market could support more endocrinologists, without adversely affecting the earnings of those currently practicing. The TAP’s estimate was that demand exceeded supply in the current market by more than 10%. The data regarding waiting time for initial appointments for new patients, the demand estimates from closed panel HMOs, and trends in patient visits suggests that there is excess demand and that it is substantial. We estimate that excess demand in 1999 is about 15%.
In Table 29 and Figures 19A and 19B , we relax the assumption that supply and demand are equal in 1999, and incorporate our estimate that excess demand is about 15% in 1999.
Table 29 Case1A
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
• Demand affected only proportionately with population growth
• Excess demand of 15% in 1999
The Lewin Group, Inc. 41 265991

Workforce Study of Endocrinologists
Figure 19A Case 1A: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1A (END)
Demand
Case 1A (END)
Figure 19B
Case 1A: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1A (PDE)Demand
Case 1A (PDE)
With excess demand of about 15% in 1999, growth in the supply of new entrants into endocrinology is greater than growth in demand that is simply proportionate to population. Excess demand persists throughout the projection period for adult endocrinologists. Excess demand for pediatric endocrinologists persists through about 2007, where approximate equilibrium is maintained. Excess demand again emerges, however, after about the year 2017.
The Lewin Group, Inc. 42 265991

Workforce Study of Endocrinologists
Case 1A does not include other factors affecting demand and supply that are likely to change over time. Most notably, the proportion of the population under managed care has increased substantially over the last 15 years, and will increase in the future, albeit at a lower growth rate. The literature, and our analyses, suggest that managed care has a negative effect on the demand for physicians’ services, especially those of specialists. We estimate that a 10% increase in the managed care penetration rate (the proportion of the population under managed care) results in about a 2% decline the demand for endocrinologists. Case 1B is the same as Case 1A, except that it incorporates the effects of continued growth in managed care on demand. We estimate that managed care grows by 3% per year between 2000 and 2005; by 2% per year between 2006 and 2010; 1% per year between 2011 and 2015; and no growth thereafter. Case 1B assumptions are presented in Table 30, and the implications of the case for supply and demand are shown in Figures 20A and 20B.
Table 30 Case 1B
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
Current demand exceeds supply by 15% Demand grows in proportion to population Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
Figure 20A Case 1B: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1B (END)
Demand
Case 1B (END)
The Lewin Group, Inc. 43 265991

Workforce Study of Endocrinologists
Figure 20B Case 1B: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1B (PDE)Demand
Case 1B (PDE)
Accounting for continued, modest, growth in managed care has a negative effect on demand. For adult endocrinologists, demand continues to exceed supply throughout the projection period, but is in approximate equilibrium in the period 2008-2015. For pediatric endocrinologists, demand exceeds supply through about 2007, at which time some excess supply appears to emerge. However, it is modest and, by the end of the projection period, supply and demand again converge. Case 1C is the same as 1B, except that we recognize that growth in the population that is over age 65 will have a disproportionate impact on the demand for the services of adult endocrinologists, while growth in the under age 18 population has a disproportionate effect on the demand for the services of pediatric endocrinologists. 32 In Case 1C, we estimate that the growth in the over age 65 population has a 15% greater effect on the demand for the services of endocrinologists than does growth in the general population. Moreover, growth in the under age 18 population has a 15% greater effect on demand for services from pediatric endocrinologists than does growth in the general population. We believe that both the estimates for the effects are conservative for both the adult endocrinologists and the pediatric endocrinologists.
32 For example, the utilization difference between the over age 65 population and the age 18-64 population in the
Kaiser Permanente benchmark analysis was significantly greater than 15%. Moreover, according to the National Center for Healthcare Statistics, older persons had over twice as many contacts with physicians than those under age 65, and accounted for 36% of all hospital stays and 49% of all days of care in 1997.
The Lewin Group, Inc. 44 265991

Workforce Study of Endocrinologists
Table 31 Case 1C
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice • No change in retirement rates
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015
No growth thereafter
Figure 21A Case 1C: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1C (END)
Demand
Case 1C (END)
The Lewin Group, Inc. 45 265991

Workforce Study of Endocrinologists
Figure 21B Case 1C: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1C (PDE)Demand
Case 1C (PDE)
The effect of accounting for growth in age groups that have a greater effect on demand than others results in an increase in demand for both adult and pediatric endocrinologists. However, it does not change the patterns of the previous case substantially. Finally, we consider the effect of growth in real income on demand. The demand for health services increases with the real income of the beneficiary population. This was captured in our own statistical analysis of the demand for the services of endocrinologists. A 10% increase in real income is associated with about a 2% to 4% increase in demand.33 Figures 22A and 22B captures the effect of an annual 1% real growth in personal income on the demand for services from endocrinologists.
33 There are no estimates of the income elasticity of demand for the services of narrowly defined specialties such as
endocrinologists in the literature. However, our estimate is within the range of those found in the literature for health services in general. For example, Joseph Newhouse reports an income elasticity of demand for health services in the range of 0.2 to 0.4. See Free For All: Lessons from the Rand Health Insurance Experiment, A RAND Study, Harvard University Press, 1993, p. 47.
The Lewin Group, Inc. 46 265991

Workforce Study of Endocrinologists
Table 32 Case 1
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
Figure 22A Case 1:Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1 (END)
Demand
Case 1 (END)
The Lewin Group, Inc. 47 265991

Workforce Study of Endocrinologists
Figure 22B Case 1: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1 (PDE)Demand
Case 1 (PDE)
Under Case 1, depicted in Figures 22A and 22B, the projection period begins with excess demand for both adult and pediatric endocrinologists. While this excess demand shrinks through about 2010, it never disappears for adult endocrinologists. For pediatric endocrinologists, excess demand is eliminated starting at about 2008. Supply and demand are in rough equilibrium through about 2016. Starting at about 2010 for adult endocrinologists and about 2016 for pediatric endocrinologists, excess demand begins to grow again. This is true for two reasons. First, an increasing proportion of the endocrinology workforce enters retirement age. Hence, supply grows at a lower rate. Second, for adult endocrinologists, the population age 65 or older begins to grow rapidly after 2010, as the majority of the baby boomers move into the senior category. This increases the demand for adult endocrinologists. Figure 23, produced from the Endocrinology Workforce Model, illustrates the effect of the aging workforce in endocrinology. Note that a significant proportion of the current workforce in the age range of about 45 to 55. By 2010, most of these physicians will be over age 60, where the incidence of retirement is high. The cohorts directly behind them, who are in the 35-45 age range today, are numerically smaller cohorts. Hence, while new entrants grow at the same rate throughout the projection period (by our assumption) growth in supply declines because of the higher rate of retirement incidence after year 2010.
The Lewin Group, Inc. 48 265991

Workforce Study of Endocrinologists
Figure 23 Age Distribution of Adult Endocrinologists under Case 1
Endocrinologist Age Distributions, 2000-2020
0
20
40
60
80100
120
140
160
180
< 30 33 36 39 42 45 48 51 54 57 60 63 66 69 72 75
>
Age
Phys
icia
ns 200020102020
We believe that Case 1 is a conservative, plausible scenario. It suggests that there is current excess demand for endocrinologists and that endocrinology can continue to absorb the current rate of new entrants into the profession through the fellowship programs without the emergence of excess supply. The case accounts for continued, realistic growth in managed care, which tends to reduce demand. However, the aging population of patients coupled with increasing numbers of endocrinologists reaching retirement age—two factors which can be predicted with little uncertainty—suggest that excess demand will grow after about 2010.
4.3 Case 2: Sensitivity to Assumption Regarding Initial Excess Demand Clearly, one of the most important assumptions made in Case 1 is the extent of excess demand in the current market. Increased times for initial appointments, benchmarks with closed HMOs, analysis of growth in services, and anecdotal evidence from practitioners suggest that there is excess demand currently. Our estimate of current excess demand is about 15%. The figures below examine the sensitivity of our overall assessment to this key assumption, by considering projects under alternative assumptions regarding current excess demand.
The Lewin Group, Inc. 49 265991

Workforce Study of Endocrinologists
Table 33 Case 2: Sensitivity
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
• Current demand exceeds supply by alternative amounts: • 5%, • 10% • 20%
• Demand grows in proportion to population, except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
Figure 24A Case 2A: Adult Endocrinologists
Case 1 with 5% Initial Excess Demand
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2A (END)
Demand
Case 2A (END)
The Lewin Group, Inc. 50 265991

Workforce Study of Endocrinologists
Figure 24B Case 2A: Pediatric Endocrinologists
Case 1 with 5% Initial Excess Demand Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2A (PDE)Demand
Case 2A (PDE)
Figure 24A depicts demand and supply conditions for adult endocrinologists under the assumption of 5% initial excess demand, compared to the 15% of Case 1. Note that there is approximate equilibrium over most of the period. Demand, however, grows faster than supply as the period 2020 is approached. In the case of pediatric endocrinologists, there is excess supply in the period beyond about 2003. However, as in the case of adult endocrinologists, growth in demand exceeds growth in supply in the latter portion of the projection period, such that demand is approximately equal to supply by the year 2020.
Figure 25A Case 2B: Adult Endocrinologists
Case 1 with 10% Initial Excess Demand Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2B (END)
Demand
Case 2B (END)
The Lewin Group, Inc. 51 265991

Workforce Study of Endocrinologists
Figure 25B Case 2B: Pediatric Endocrinologists
Case 1 with 10% Initial Excess Demand Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2B (PDE)Demand
Case 2B (PDE)
In Figure 25A, the supply and demand for adult endocrinologists is shown under the assumption that initial excess demand is about 10%. In this case, excess demand persists throughout the period, to a greater or lesser extent, but begins to grow toward the end of the projection period. The case of pediatric endocrinologists is shown in Figure 25B. Though modest excess supply emerges around the year 2005, this disappears by the end of the projection period.
Finally, Figures 26 A and B presents the case in which initial excess demand is about 20%, for adult and pediatric endocrinologists, respectively. In this case, there is excess demand throughout the entire projection period for both adult and pediatric endocrinologists.
Figure 26A Case 2C: Adult Endocrinologists
Case 1 with 20% Initial Excess Demand Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2C (END)
Demand
Case 2C (END)
The Lewin Group, Inc. 52 265991

Workforce Study of Endocrinologists
Figure 26B Case 2C: Pediatric Endocrinologists
Case 1 with 20% Initial Excess Demand
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 2C (PDE)Demand
Case 2C (PDE)
Our best estimate of excess demand in the current market is about 15%. This is based on an analysis of trends in claims, an estimate from a closed panel HMO, and estimates of current waiting times for new patient appointments, as well as anecdotal information from practitioners. However, there is clearly uncertainty in any such measure. To test the sensitivity of general conclusions to this estimate, we examined alternative assumptions of 5%. 10%, and 20% current excess demand, while holding all other aspects of Case 1 constant. The overall qualitative conclusions for adult endocrinologists remain largely intact under the alternative assumptions. Conditions of approximate equilibrium or excess demand persist throughout the period, with excess demand growing in the later years of the projection period. The results are similar for pediatric endocrinologists, with one exception. If current excess demand is only 5%, it is likely that modest excess supply will persist throughout the period, though the gap is closed by the end of the period.
4.4 Case 3: Effect of Increase in Diabetes on Demand Case 1 takes into account known factors that are likely to affect the supply of and demand for endocrinologists over the next 20 years. Recent epidemiological trends, however, indicate an increase in the incidence of one of the primary diseases treated by endocrinologists, Type II diabetes.34 Case 3 is the same as Case 1, except that we assume that the incidence of diabetes increases at the rate of 1% per year, and endocrinologists’ share of patient visits for diabetes also increases by 1% per year.
34 See, for example, Arlan Rosenbloom, MD, Chair; Silva Arslanian, MD; Stuart Brink, MD; Katie Conschafter,
RD, CDE; Kenneth Lee Jones, MD; Georgeanna Klingensmith, MD; Naomi Neufeld, MD; and Neil White, MD, “Consensus Statement: Type 2 Diabetes in Children and Adolescents”, Diabetes Care, vol. 3, no.3, p.381, 2000; and Steven V. Edelman, MD, Robert R. Henry, MD, Diagnosis and Management of Type II Diabetes. Second Edition, Professional Communications, Inc. 1998.
The Lewin Group, Inc. 53 265991

Workforce Study of Endocrinologists
Table 33 Case 3
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
• Incidence of diabetes, and endocrinologists’ share of visits, grows by 1% per year.
Figures 27 and 28 present results for Case 3. If the is a modest increase in incidence of Type II diabetes of 1% per year, there will be excess demand for both adult and pediatric endocrinologists over the entire projection period. However, this excess demand disappears by about 2010 for pediatric endocrinologists and reemerges after about 2014. Excess demand grows most rapidly after 2010 for both adult and pediatric endocrinologists.
Figure 27 Case 3: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 3 (END)
Demand
Case 3 (END)
The Lewin Group, Inc. 54 265991

Workforce Study of Endocrinologists
Figure 28 Case 3: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 3 (PDE)Demand
Case 3 (PDE)
In Case 3A, we assume that the incidence of Type 2 diabetes grows by 3% per year for the under age 18 population. All other conditions remain the same as in Case 1. Figure 29 shows the implications for the supply of and demand for pediatric endocrinologists.
Figure 29 Case 3A: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1400
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 3A (PDE)Demand
Case 3A (PDE)
As Figure 29 indicates, the tendency for the current shortage of pediatric endocrinologists to disappear around the 2010 is eliminated. The excess demand increases continuously beyond 2010 under this assumption of a continuous 3% growth in the incidence of Type 2 diabetes. The
The Lewin Group, Inc. 55 265991

Workforce Study of Endocrinologists
result, if there were no offsetting actions, would be a severe and growing shortage of pediatric endocrinologists beyond 2010.
4.5 Case 4: Growth in Fellowship Positions Heretofore, we have assumed that the number of filled fellowship positions remains constant at the current level. The analysis in this section illustrates the effect that changes in the growth in fellowship positions can have on the market, testing the sensitivity of our conclusions to additional growth in fellowship positions. Over most of the decade of the 1990’s, the number of internal medicine residents pursuing fellowships in endocrinology, as well as most of the other traditional IM subspecialties, declined. The number of filled fellowship positions in endocrinology also declined. There is some anecdotal evidence, however, that this decline has ended. Case 4 examines the implications for supply and demand if the number of filled fellowship positions increases. We assume that adult fellowship positions grow by 2% per year between 2000 and 2005, and by 5% per year from 2006 through 2010. Pediatric positions are assumed to grow by 1% per year between 2000 and 2005 and by 3% between 2006 and 2010. Beyond 2010, positions remain constant.35 All other assumptions are those of Case 1.
Table 34 Case 4
Case 4 Supply Demand
Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice • Adult fellowship positions grow by 2% per
year between 2000 and 2005, and by 5% per year between 2006 and 2010.
• Pediatric fellowship positions grow by 1% per year between 2000 and 2005 and by 3% per year between 2006 and 2010.
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
35 These assumptions are close to those advocated by our Technical Advisory Panel (TAP). Their consensus
estimate was that fellowship positions would grow by 5% per year between 2005 and 2010.
The Lewin Group, Inc. 56 265991

Workforce Study of Endocrinologists
Figure 30 Case 4: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 4 (END)
Demand
Case 4 (END)
Figure 31
Case 4: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 4 (PDE)Demand
Case 4 (PDE)
As Figures 30 and 31 indicate, a modest but sustained increase in new fellowship positions is sufficient to eliminate excess demand, under the demand assumptions of Case 1, by about 2012 for adult endocrinologists and about 2008 for pediatric endocrinologists. Thereafter, the market is in approximate equilibrium, with perhaps slight excess supply.
The Lewin Group, Inc. 57 265991

Workforce Study of Endocrinologists
In Case 4A, the assumptions regarding the growth in fellowships are the same as in Case 4. However, the demand assumptions are those of Case 3. That is, we assume a 1% per year increase in the incidence of diabetes.
Table 35 Case 4A
Case 4A Supply Demand
Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates • 143 PDE positions, 80% filled
• 50% are international medical school graduates • 80% of IMGs remain in the United States to practice • Adult fellowship positions grow by 2% per year
between 2000 and 2005, and by 5% per year between 2006 and 2010.
• Pediatric fellowship positions grow by 1% per year
between 2000 and 2005 and by 3% per year between 2006 and 2010.
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Incidence of diabetes grows by 1% per year. • Modest managed care growth:
• 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
Figure 32 Case 4A: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 4A (END)
Demand
Case 4A (END)
The Lewin Group, Inc. 58 265991

Workforce Study of Endocrinologists
Figure 33 Case 4A: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 4A (PDE)Demand
Case 4A (PDE)
As illustrated in Figure 27, the increase in fellowship positions does not result in excess supply in the latter years, in this variation, because the growth in demand due to the increasing incidence of diabetes absorbs this increase.
4.6 Case 5: Other Supply Factors In this section, we test the sensitivity of the implications of Case 1—our “best estimate’ for planning purposes--to two additional “supply side” assumptions. We first consider a trend toward increasing retirements. Anecdotal evidence suggests that physicians are withdrawing from the workforce at earlier ages than in previous years. This is sometimes attributed to frustration with managed care and with Medicare billing requirements. We examine the implications under a particular set of assumptions regarding earlier retirements. We next examine the assumption that 20% of IMG fellows leave the United States upon completing their fellowship. Many experts believe that, in fact, most IMGs remain in this country to practice. However, there is little systematic empirical evidence on this issue. We consider what the implications would be if all IMG fellowship graduates were to remain in the United States to practice. Case 5 is the same as Case 1, except that we assume that there will be a trend toward early retirement among practicing endocrinologists. In particular, we assume that there will be a 10% increase in retirement rates for those over age 50 starting in 2001; in 2005 there will be another 10% increase in retirement rates for those between 50 and 64, and a 5% increase in rates for those over 65. Finally, in 2010 we assume that retirement rates for those aged 50-64 will
The Lewin Group, Inc. 59 265991

Workforce Study of Endocrinologists
increase by another 10%, while retirement rates for those over age 65 will increase by an additional 5%.36
Table 36 Case 5
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice • Retirement rates are assumed to increase
• In 2001, a 10% increase in the retirement rates for those over age 50
• In 2005, a 10% increase in the retirement rates for those between 50-64 and a 5% increase for those over age 65
• In 2010, a 10% increase in retirement rates for those between 50-64 and a 5% increase for those over age 64.
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth:
• 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Real household income grows by 1%/yr.
Figure 34 Case 5: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 5 (END)
Demand
Case 5 (END)
36 Please note that these adjustments are smaller than they may appear. The retirement rate at age 50, for example, is
about 1.0 per cent. A ten percent increase in that rate makes it only 1.1 per cent.
The Lewin Group, Inc. 60 265991

Workforce Study of Endocrinologists
Figure 35 Case 5: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 5 (PDE)Demand
Case 5 (PDE)
Case 5, as illustrated in Figures 34 and 35, suggests that increased retirement rates will have a modest effect on the workforce. Supply grows at a lower rate due to the increased retirements. Excess demand is increased somewhat due to the retirement rates. Case 5A is the same as Case 1, except that we assume that 100% of IMGs remain in the United States to practice endocrinology. A large portion of IMGs are, in fact, U.S. citizens or have permanent residency status. About 30% of IMGs in general are on J-1 visas. Unless they receive a waiver, they must leave the U.S. after completing their fellowship.37 Throughout most of our analysis, we have assumed that 80% of IMGs remain in this country to practice. In Case 5A, however, we examine how market conditions would be affected if it were the case that 100% remained.
37 Discussion with a number of experts at the Health services and Research Association, and other ogranizations, has
suggested that most IMGs remain in this country. However, there does not appear to be solid empirical evidence on this issue.
The Lewin Group, Inc. 61 265991

Workforce Study of Endocrinologists
Table 37 Case 5A
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 100% of IMGs remain in the United States to
practice • Retirement rates remain the same
• Current demand exceeds supply by 15% • Demand grows in proportion to population,
except that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth:
• 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
Real household income grows by 1%/yr.
Figure 36 Case 5A: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 5A (END)
Demand
Case 5A (END)
The Lewin Group, Inc. 62 265991

Workforce Study of Endocrinologists
Figure 37 Case 5A: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 5A (PDE)Demand
Case 5A (PDE)
Figures 36 and 37 suggest that, if it were true that all IMGs remained to practice in the United States, there would be a modest increase in supply, reducing projected excess demand somewhat. However, the basic pattern over the projection period of initial excess demand, approximate equilibrium, and then the reemergence of excess demand toward the latter part of the projection period remains the same.
4.7 Conclusion In this section, we have demonstrated effects that various factors may have on the supply of and demand for endocrinologists. We have also assessed the overall “health” of the endocrinology workforce under a number of alternative assumptions. When there is significant excess demand for services, the individual, practicing, endocrinologist can expect earnings to grow or at least remain constant. The workforce can grow without significant downward pressure on the earnings of individual practitioners. When there is excess supply, the converse of this is likely to be true. Our Case 1 reflects our assessment of the current and projected future state of the workforce for planning purposes. It suggests that there is current excess demand, but that continued growth in supply may eliminate that “cushion” within about 8-9 years. However, beyond about 2010, demand grows faster than supply for two reasons. First, the population that is over age 65 grows rapidly after 2010, as the baby boom cohorts reach retirement age. This increases the demand for services of endocrinologists, because the incidence of diseases treated by endocrinologists, such as diabetes and osteoporosis, are greater in the older population. Second, a large number of endocrinologists will, themselves, reach retirement age after 2010, slowing the growth in supply. Growth in managed care at rates faster than assumed here would increase the chances of excess supply, as would near term growth in the number of fellowship positions. Still, the evidence we examined in section 3, the aging population, and the possibility of a greater role for specialists in
The Lewin Group, Inc. 63 265991

Workforce Study of Endocrinologists
disease management suggest that excess demand for endocrinologists will persist through the year 2020, though at rates generally lower than are currently experienced. Epidemiological considerations, such as increasing incidence of Type 2 diabetes, could result in significantly greater excess demand over the period. On the other hand, growth in managed care above what is projected here, or more rapid growth in supply through increasing numbers of fellowship positions, could reduce or eliminate excess demand.
5. SUMMARY In this report, we examine the characteristics of the current endocrinology workforce, factors affecting supply and demand, and provide projections of the supply of and demand for endocrinologists under alternative scenarios. Based on these projections, and our analysis of specific factors affecting demand and supply, we provide an overall assessment of the market for the services of endocrinologists over the next twenty years. There is no attempt in this study to determine the “right” number of endocrinologists in a normative or needs-based sense. The estimates of demand are based on market conditions that reflect underlying epidemiological conditions or “need”. But, they also embody the market realities that generate effective demand for health care: insurance coverage, the degree of managed care penetration, the distribution of income, and competition from other providers. We provide predictions of future supply and demand over the next twenty years. While the predictions have the appearance of precision, there are too many variables to achieve such precision, in practice. Events that cannot now be anticipated will undoubtedly have a significant and unpredictable influence on the demand for endocrinologists ten or twenty years from now. Thus, our point estimates should be interpreted as representing a broad range, under the assumption that all other factors are constant. Our overall market assessment is based on the systematic analysis of a number of cases or scenarios that our research indicates are likely to affect future demand and supply. Undoubtedly, there will be factors arising that will affect future markets that cannot currently be anticipated. We distinguish between pediatric endocrinologists and “adult” (endocrinology and metabolism) endocrinologists in most of the analysis. On average, adult endocrinologists are older and more often male than pediatric endocrinologists. Over 65% of adult endocrinologists and 55% of pediatric endocrinologists are engaged in office-based clinical practice. Endocrinologists are most highly concentrated in the New England and Middle Atlantic States, and least concentrated in the East South Central and Mountain States. Of the twenty largest MSAs, endocrinologists are most highly concentrated in Boston and Nassau-Suffolk Counties in N.Y. They are least concentrated in Riverside-San Bernardino Counties in California, Dallas, and Houston, Texas. Enrollment in fellowship programs drives the supply of endocrinologists. Currently, there are 393 fellows enrolled in adult endocrinology programs, and about 115 fellows enrolled in pediatric endocrinology. There has been a modest downward trend in enrollment in endocrinology fellowship programs over the 1990’s. Examination of both Medicare Part B data and data from the National Ambulatory Care Survey indicated that the demand for services of endocrinologists has increased over the 1990’s. This was especially evident in the NAMCS data., though it does suffer from small sample sizes. The
The Lewin Group, Inc. 64 265991

Workforce Study of Endocrinologists
NAMCS data suggested that, in comparing the three-year period 1993-1995 to the three-year period 1996-1998, office visits to endocrinologists for diabetes-related reasons increased substantially relative to office visits for thyroid disease-related reasons. Managed care has an important impact on the demand for the services of endocrinologists. We estimate that a 10% increase in the “HMO penetration rate” results in about a 2.4% decline in the demand for the services of endocrinologists. However, disease management programs are now found with some frequency in managed care organizations. About 50% of organizations sampled in 1997 reported disease management programs in diabetes. This suggests that such programs for diseases such as diabetes have the opportunity to increase the demand for the services of endocrinologists in a managed care environment. Analysis of the administrative databases, surveys, and the views of our Technical Advisory Panel suggested that the current market could absorb a greater number endocrinologists than are currently in the workforce, without adversely affecting those in the workforce. A “benchmark” estimate, using a Kaiser Permanente HMO, suggested that the current population could absorb about a 12% increase in practicing endocrinologists. This was consistent with the views of our TAP, as well as the trends we observed in the increase in demand for the services of endocrinologists in the Medicare and NAMCS data from the 1990’s. Analysis based on average waiting time for appointments for new patients suggest that even greater excess demand may exist in the current market. Finally, applying the Endocrinologist Workforce Model, we analyzed the effects that various factors may have on the supply of and demand for endocrinologists. We also assessed the overall “health” of the endocrinology workforce under a number of alternative assumptions. When there is significant excess demand for services, the individual practicing endocrinologist can expect earnings to grow or at least remain constant. The workforce can grow without significant downward pressure on the earnings of individual practitioners. When there is excess supply, the converse of this is likely to be true. Our Case 1, reproduced here, reflects our assessment of the current and projected future state of the workforce that we believe is useful for planning purposes. It suggests that there is excess demand in the current market, but that continued growth in supply may reduce the amount of excess demand through about 2010. At that time, a combination of slower growth in supply, due to a large number of endocrinologists reaching retirement age, coupled with growth in demand through increases in the over age 65 population, will tend to increase excess demand for adult endocrinologists. Programs, such as the emphasis of endocrinologists as disease managers for patients with diabetes, could further increase demand, as could continued growth in the incidence of Type 2 diabetes and other diseases. Further, if there is an emerging trend toward somewhat earlier retirement, excess demand could become severe if there is not an offsetting increase in the number of fellowship positions.
The Lewin Group, Inc. 65 265991

Workforce Study of Endocrinologists
Table 38 Case 1
Supply Demand Current fellowship positions and fill rates persist into future • 457 END positions, 86% filled
• 57% are international medical school graduates
• 143 PDE positions, 80% filled • 50% are international medical school
graduates • 80% of IMGs remain in the United States to
practice No change in retirement rates
• Current demand exceeds supply by 15% • Demand grows in proportion to population, except
that the over 65 population growth results in a 15% greater increase in the demand for adult endocrinologists and that growth in the under age 18 population has a 15% greater increase in demand for pediatric endocrinologists.
• Modest managed care growth: • 3%: 2000-2005 • 2%: 2006-2010 • 1%: 2011-2015 • No growth thereafter
• Growth in real personal income of 1% Per year.
Figure 38 Case 1: Adult Endocrinologists
Supply and Demand
0
1000
2000
3000
4000
5000
6000
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1 (END)
Demand
Case 1 (END)
The Lewin Group, Inc. 66 265991

Workforce Study of Endocrinologists
Figure 39 Case 1: Pediatric Endocrinologists
Supply and Demand
0
200
400
600
800
1000
1200
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
Year
Endo
crin
olog
ists
Supply
Case 1 (PDE)Demand
Case 1 (PDE)
Case 1, our overall assessment of current and future market conditions for endocrinologists, suggests both current and future excess demand for endocrinologists. Growth in managed care at rates faster than assumed here would reduce, and perhaps eliminate, future excess demand, as would growth in the number of fellowship positions. Still, the evidence and data we examined including the aging population, retirement of older endocrinologists, the possibility of a greater role for specialists in disease management, and recent epidemiological trends suggest that the major workforce issue over the next twenty years is likely to be too few, not too many, endocrinologists.
The Lewin Group, Inc. 67 265991

Workforce Study of Endocrinologists
6. REFERENCES American Medical Association, Physician Socioeconomic Statistics, Center for Health Policy
Research, 1999-2000 edition. American Medical Association, Physician Marketplace Statistics, Center for Policy Research,
1997/1998. American Medical Association, Physician Marketplace Statistics, Center for Policy Research,
1996. American Medical Association, Physician Marketplace Statistics, Center for Policy Research,
1992. Center for Health Statistics, Health, United States, 2000 with Adolescent Health Chartbook,
Hyattsville, Md. 2000. Edelman, Steven V., MD, Henry, R.R., MD, Diagnosis and Management of Type II Diabetes,
Second Edition, Professional Communications, 1998. Goodman, David C. M.D., Elliot S. Fisher, M.D., Thomas A. Bubolz, Ph.D., Jack E. Hohr,
James F. Poage, Ph.D., and John E. Wennberg, M.D., “Benchmarking the US Physician Workforce. Journal of the American Medical Association, December 11, 1996, v. 276, no. 22.
Hodgson, Stephen F., MD, MACE, “AACECare: A Proposal for the Future.” Interstudy Competitive Edge, 1996, 1997, 1998, 1999. Journal of the American Medical Association, September 2000, Appendix 6. Levitan, C.S., et al, Diabetes Care, November 1999. Medical Group Management Association, Physician Compensation and Production Survey, 1998
Report (based on 1997 data.) and 1997 Report (based on 1996 data.). National Center for Health Statistics, Health , United States, 1999. Hyattsville, Md. 1999. Newhouse, Joseph and the Insurance Experiment Group. Free For All: Lessons from the Rand
Health Insurance Experiment, A RAND Study, Harvard University Press, 1993 Roehrig CS and Janayan A.M. “Physician Separation Rate Estimation,” Vector Research,
September 4, 1986. Rosenbloom, Arlan MD, Chair; Silva Arslanian, MD; Stuart Brink, MD; Katie Conschafter, RD,
CDE; Kenneth Lee Jones, MD; Georgeanna Klingensmith, MD; Naomi Neufeld, MD; and
The Lewin Group, Inc. 68 265991

Workforce Study of Endocrinologists
Neil White, MD, “Consensus Statement: Type 2 Diabetes in Children and Adolescents”, Diabetes Care, vol. 3, no.3, p.381, 2000.
Weiner, Jonathan P., Dr.PH, “Forecasting the Effects of Health Reform on US Physician Workforce Requirement,” Journal of the American Medical Association, July 20, 1994, v. 272, no.3.
The Lewin Group, Inc. 69 265991

Workforce Study of Endocrinologists
7. APPENDIX A: TECHNICAL ADVISORY PANEL PERSPECTIVES
The Technical Advisory Panel graciously agreed to spend a day providing their perspective on issues and assumptions that require expert judgment. In preparation for the session in Chicago held on July 15, the TAP completed a brief survey. The survey addressed future growth in fellowship positions and future changes in retirement patterns for endocrinologists. The following is a summary of the results. 1. How do you expect filled fellowship positions to change over the next five years for Endocrine, Diabetes and Metabolism? N pct averagea. Remain about the same 1 17% -1%b. Increase by less than 5% per year. 1 17%c. Increase by 10% or more per year. 1 17%d. Decrease by less than 5% per year. 2 33%e. Decrease by 10% or more per year. 1 17%
2. How do you expect filled fellowship positions to change over the next five years for Pediatric Endocrinology? N pct averagea. Remain about the same 2 33% 1%b. Increase by less than 5% per year. 3 50%c. Increase by 10% or more per year. 0 0%d. Decrease by less than 5% per year. 0 0%e. Decrease by 10% or more per year. 1 17%
3. Do you anticipate that the retirement patterns of endocrinologists will change over the next 5-10 years? N pct a. Remain about the same. 1 17% b. Tendency toward earlier retirement. 4 67%c. Tendency toward later retirement. 1 17%
4. What is the most significant issue in graduate medical education for endocrinology? N pcta. Interest among Internal Medicine residents in pursuing an endocrinology subspecialty. 6 100%b. GME funding for fellowship positions in endocrinology. 0 0%c. Curriculum and focus changes. 0 0%d. Other (specify) 1 17%
The Lewin Group, Inc. 1 265991

Workforce Study of Endocrinologists
5. What are the most significant negative factors affecting the futuredemand for and economic viability of endocrinologists? Please circle/listall that are important. (Circle A, P, or B) N pcta. Managed care. 6 100%
b. Medicare reimbursement changes (e.g., a PPS for outpatient visits.) 6 100%c. Cost of documentation (Medicare, Medicaid.) 3 50%d. Competition from other specialists 3 50%e. Competition from primary care practitioners 2 33%f. Changes in science/technology 0 0%g. Other (specify) 0 0%
6. What are the most significant positive factors affecting the futuredemand and economic viability of endocrinologists? Please circle/list allthat are important.(Circle A, P, or B) N pcta. Aging population. 5 83%b. Increased awareness of the cost-effectiveness of endocrinologistmanagement of certain diseases (e.g., diabetes) by medical directors. 4 67%c. Use of methods to lower cost of patient care by endocrinologists (e.g.,increased use of nurse practitioners, physician’s assistants byendocrinology practice.) 3 50%
d. New areas for practice (e.g., primary care, non-traditional diseases.) 3 50%e. Changes in science/technology 5 83%f. Other (specify) 1 17%
7. What has been the effect of managed care on the demand for servicesof endocrinologists?(Circle A, P, or B) N pcta. It has not had much of an effect. 0 0%b. It has had a modest negative effect on demand. 3 50%c. It has had a significant negative effect on demand. 1 17%d. It has had a positive effect on demand. 1 17%
8. The best way for endocrinology to adjust to managed care is:(Circle A, P, or B) N pcta. Convince managed care medical directors of the cost-effectiveness ofmanagement of certain diseases by endocrinologists. 6 100%b. Use allied health care professionals (nurse practitioners, physicianassistants) to increase practice efficiency. 3 50%c. To practice within integrated groups including other specialists andprimary care practitioners. 3 50%d. To find additional practice areas, such as primary care, or other(please specify) 0 0%e. Other (specify) 1 17%
The Lewin Group, Inc. 2 265991

Workforce Study of Endocrinologists
9. Primary competing specialties include (circle all that apply):(Circle A, P, or B) N pcta. Primary care 5 83%b. Internal medicine 5 83%c. Rheumatologists 3 50%d. Urologists 3 50%e. Nephrologists 4 67%f. Hematologists 0 0%g. Gerontologists 2 33%h. OB/GYN 4 67%i. Other (specify) 1 17%
10. Primary complementary (referring) specialties include:(Circle A, P, or B) N pcta. Primary care. 4 67%b. Cardiologists 1 17%c. Nephrologists 1 17%d. Internal Medicine 6 100%e. Gerontologists 0 0%f. Urologists 2 33%g. OB/GYN 3 50%h. Other (please specify) 1 17%
11. The current number of endocrinologists (1999) per 100, 000 population, in urban areas is 1.93. Under prevailing demand conditions for the clinical practice of endocrinology: (Circle A, P, or B) N pct a. This ratio is about right and can be sustained without significant changes in the income of endocrinologists. 1 17% b. This ratio cannot be sustained. It is too high, for current conditions, and will result in lower incomes and/or endocrinologists leaving the specialty. 0 0%c. Under current demand conditions, the health care market could absorb significantly more practicing endocrinologists, without adversely affecting the incomes of those in the profession. 4 67%d. Other (specify or comment.) 0 0%
12. The current number of endocrinologists (1999) per 100, 000 population, in rural areas is 0.255. Under prevailing demand conditions for the clinical practice of endocrinology: (Circle A, P, or B) N pct averagee. This ratio is about right and can be sustained without significant changes in the income of endocrinologists. 1 17% 83%f. This ratio cannot be sustained. It is too high, for current conditions, and will result in lower incomes and/or endocrinologists leaving the specialty. 0 0%g. Under current demand conditions, the health care market could absorb significantly more practicing endocrinologists, without adversely affecting the incomes of those in the profession. 5 83%h. Other (specify or comment.) 0 0%
The Lewin Group, Inc. 3 265991

Workforce Study of Endocrinologists
The Lewin Group, Inc. 4 265991
The responses to the survey served as a starting point as these, and other, issues were discussed in the day-long meeting. The key results of the discussion were the following, based on median responses: • The panel believed that there would be no growth in endocrinologist fellowship positions
between 2000 and 2005, but that there would be a 5% growth between 2005 and 2010. • The panel believed that the average age of retirement for endocrinologists would decline by
5% between 2000 and 2005, but that there would be no additional change between 2005 and 2010.
• The panel believed that current demand for the services of endocrinologists could support a
10% increase in endocrinologists in both urban and rural areas. • The panel believed that most other specialists, including primary care, were, on net, either
complementary to endocrinology or neutral. That is, they did not believe that any particular specialist group had a negative effect on the demand for their services.
• The panel believed that the aging population would increase the demand for the services of
endocrinologists by about 15% above the increase due to aggregate population growth alone. Both the initial survey responses and the subsequent discussion and estimates by the panel member suggest a relatively optimistic scenario, in the near term, for endocrinologists. There was unanimous agreement that the current health care market could support greater numbers of endocrinologists than are currently practicing. Moreover, managed care has only a modest negative affect on demand, and all agreed that one of the best ways to adjust was to convince the managed care industry of the efficiency and efficacy of disease management by endocrinologists for certain diseases, such as diabetes.