
WOMEN’S HEALTH GP CONFERENCE - The Portland … · 2015-10-08 · WOMEN’S HEALTH GP CONFERENCE...
129
WOMEN’S HEALTH GP CONFERENCE The Royal Society of Medicine Saturday 19 th September 2015 E: [email protected] T: 0207 390 6057 F: 0207 390 6069
Transcript of WOMEN’S HEALTH GP CONFERENCE - The Portland … · 2015-10-08 · WOMEN’S HEALTH GP CONFERENCE...

WOMEN’S HEALTH GP CONFERENCE
The Royal Society of Medicine
Saturday 19th September 2015
E: [email protected] T: 0207 390 6057 F: 0207 390 6069

Obstetrics
• Approximately 1600 deliveries per annum
• 55% of our clientele are self funding
• 45% are funded by private medical insurance
E: [email protected] T: 0207 390 6057 F: 0207 390 6069

Maternity Safety
• All patients are pre-booked and pre-assessed against robust criteria
• MDTs for high risk deliveries
• Average length of stay – 3 Days
• Resident Consultant Obstetric Anaesthetists
• Interventional Radiologists
• Consultant Lactation Midwives
• High midwife to patient ratio
• Consultant Paediatrician and Neonatologists E: [email protected] T: 0207 390 6057 F: 0207 390 6069


Maternity Packages Consultant Led Care (packages start from £5,850 excluding consultant fees) Midwife Led Care (packages start from £6,850 all inclusive) One call to our Maternity Line and we take care of everything: 0207 390 6068
E: [email protected] T: 0207 390 6057 F: 0207 390 6069

Standard Room
Reception
Nursery
5 bed labour ward with adjoining dedicated emergency obstetric theatre 29 postnatal rooms including suites & deluxe rooms Nursery & transitional care Neonatal Unit – 3 cot NICU, 4 cot SCBU PICU – 10 Beds 12 bed dedicated gynaecology ward
First Class Facilities
Birthing pool

Follow on Paediatric Services • Services for the newborn include: baby check, hearing
check by audiologist, Congenital Hip Dysplasia and Birthmark services
• Approximately 1,500 inpatient admissions and over 3,500 day cases per annum
• Average length of inpatient stay is 5 days
• Patients are insured, self pay, embassy and charity sponsored
• Over 50,000 children’s outpatient visits per annum • Over 120 top specialist paediatric consultants

Gynaecology in a Women’s Hospital
Diagnostics • Imaging – US/MRI • Urodynamics • Pathology and
histology • Excellent colposcopy
facilities
Gynae Consultant subspecialists • Minimal access surgery • Endometriosis • Urogynaecology • Outpatient hysteroscopy &
ERCPs • Strong link to HCA’s cancer
networks
• Dedicated gynaecology nursing team in outpatients, theatre and wards
• Specialist women’s health physiotherapy team
E: [email protected] T: 0207 390 6057 F: 0207 390 6069

Why refer to the Portland? • At an average London and Home county GP practice, approximately one in every 5
families will have their children covered on their Medical Insurance Policy
• Quick access to London’s top Specialists who undertake a true MDT approach • Three operating theatres, one emergency operating theatre on the labour ward and an
onsite Adult High Dependency Unit, Neonatal Intensive Care Unit, Special Care Baby Unit, Transitional Care Unit and Paediatric Intensive Care Unit.
• Patient care is tailored to the individual
• All rooms have ensuite facilities where one parent/partner can stay at all times
E: [email protected] T: 0207 390 6057 F: 0207 390 6069

GP Liaison Team
• Same day and next day paediatric appointments available Monday to Saturday
• Referrals accepted by email, fax and post – either named or unnamed referrals
• All referral requests responded to within one working day and patient contacted directly for appointment
• Audiology, Imaging and Therapy departments accept referrals directly from GPs
T: 0207 390 6057 F: 0207 390 6069 E: [email protected] W: www.theportlandhospital.com

New: CPD GP Webinars
• Interactive webinars with dual aspect showing both Consultant and presentation
• Log in from your practice or home
• Weekday, lunchtime talks for one hour
• CPD certificates provided via email after each meeting
• Register on our website: www.theportlandhospital.com/GP
Please speak to one of the team if you are interested.
E: [email protected] T: 0207 390 6057 F: 0207 390 6069


Prof Ellis Downes FRCOG,
Consultant Obstetrician & Gynaecologist, The Portland Hospital
www.ellisdownes.com
Heartsink GP Gynaecology
19th September 2015 Royal Society of Medicine

Gynaecological Heartsinkers !
• “Thick note syndrome”
• Fed-up • Stroppy • Seen many doctors • “I want it sorting out”

Clinical Challenges
• Vaginal discharge • Bleeding on OCP • Pelvic pain • Pre-Menstrual syndrome

Vaginal Discharge



Vaginal Discharge
• Common • Is it serious ?
– Carcinoma
• Is it infective ? – Triple swabs (HVS, ECS, Chlamydia)
• How can it be treated ?

Management Options
• Examine the patient • Recent smear • Treat Infection
– Bacterial vaginosis , Clindamycin / Metronidazole – Candida albicans, diflucan, cannesten
• Candida sub-typing – 95% Albicans – 5% Glabrata sensitive to NYSTATIN

Sterile Vaginal Discharge Management Options • Change / start OCP to manipulate
oestrogen / progestagen ratio. • Clindamycin cream • Live natural yogurt douches • Loop excision / cervical cautery • Strong reassurance

Vitamin D Deficiency
• Vit D affects collagen metabolism • 200 women with chronic discharge
– High dose vitamin D suppositories – After 6 weeks, 79% “less discharge”
(Schulte – Uebbing, 2014)
Gynaecological Nightmare
• Problem I’ve had 100 million different types of OCP
and I bleed on them all.

Management Options
• Persevere for 4 /12, don’t “chop and change”
• Smear / chlamydia • Compliance ? • Change progestagenic component • Rarely USS • Even more rarely hysteroscopy

Pelvic Pain

“Dear Doctor,
Please see this 32 year patient with pelvic pain. I don’t know what can be done for her, in truth I am only referring her
to give myself a break.
Dr X”

Chronic Pelvic Pain
• Six month duration • Multi-factorial aetiology
– gynaecological – bowel – bladder – muscular-skeletal – psychological
• Depressed / Anxious
Scope Of The Problem
• Wide ranging prevalence • 5% - 33% • 581 women attending GP
– 39% pain at some time – 11% pain lasting more than 5 days
• Steege 1996
• 1/3 women attending gynae clinics have pelvic pain as dominant symptom

picture of endometriosis

picture of ovarian endometriosis

Adhesions

Pelvic Pain - Management Options • History & Examination • Reassure • MSU, Triple Swabs, Pelvic USS • Regulate diet
– laxative abusers
• OCP / Provera 20mg continuously • Tender bladder – cranberry juice,
– low dose antibiotics
• LH-RH agonists • Refer

Pre-Menstrual Syndrome
• 5-30% of women have significant PMS – (PMS O’Brien 2007)
• Significant personal, family and employment implications
• Poor evidence base • Establish diagnosis with diary

Management Options • First Line
– Exercise & lifestyle – Vitamin B6 – OCP – Luteal phase SSRI’s
• Second Line – Oestrogen patches – Higher dose, continuous SSRI’s
• Third Line – GnRh + HRT

Elephant picture

Issues in early pregnancy…. Emma Kirk MRCOG MD

Objectives
Appreciate the most common early pregnancy
complications Understand some early pregnancy terminology
Understand what you can do and what we can
do

Early Pregnancy
Vaginal Bleeding Pelvic Pain Unsure dates
Previous early pregnancy loss Hyperemesis
Gravidarum
Previous infertlity
Medical Condition
Unplanned pregnancy
Excited!

Sarah…
35 years old P0+1 (TOP)
Trying to conceive for the past 6 months Normal smear 2 years ago
Positive pregnancy test LMP ? 5 weeks ago Light PV spotting and cramp like pains

Folic acid 400mcg 5mg for high risk groups
Urine dipstick
BP and weight
What next?

Speculum examination? Ectropion ~40% Cervical cancer 7.5 in 100,000 pregnancies
Ultrasound?
Pregnancy location Viability Dating Number of fetuses
What next?
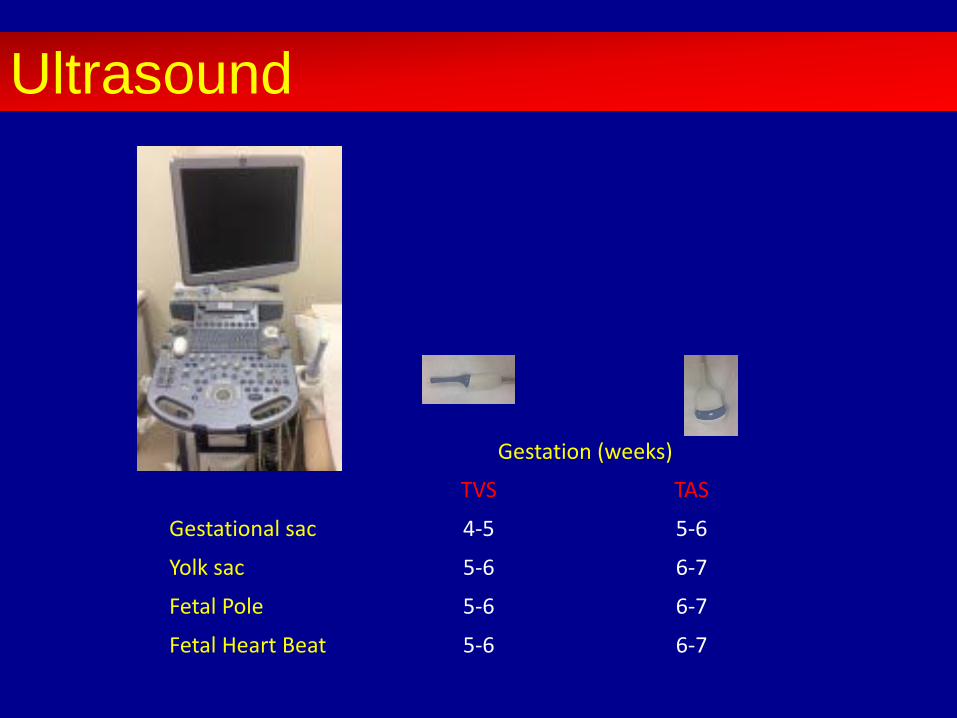
Gestation (weeks)
TVS TAS
Gestational sac 4-5 5-6
Yolk sac 5-6 6-7
Fetal Pole 5-6 6-7
Fetal Heart Beat 5-6 6-7
Ultrasound
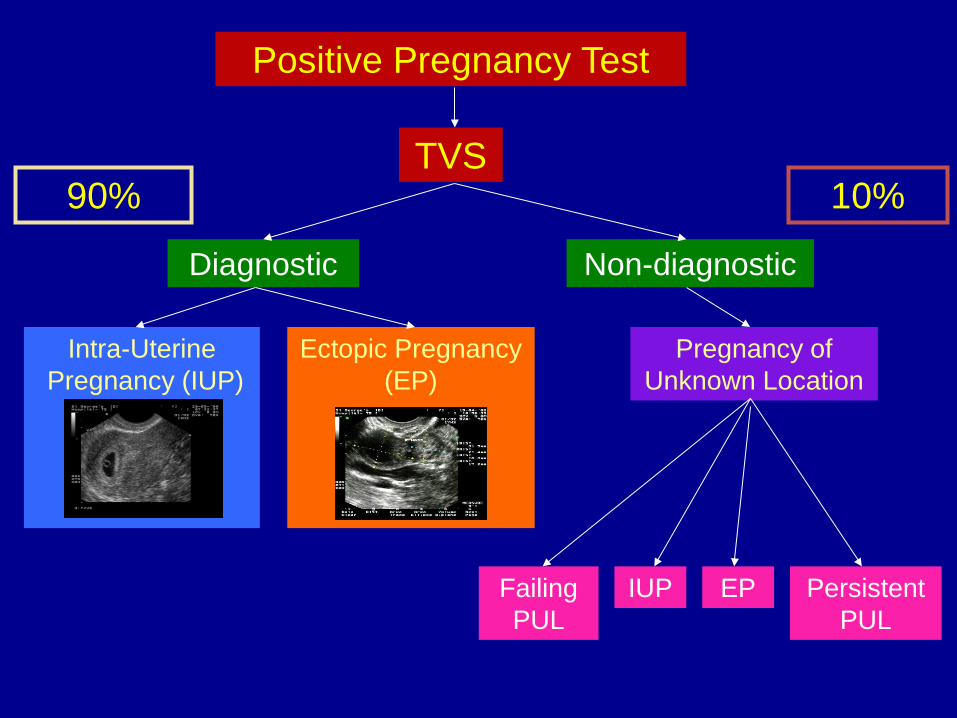
Ectopic Pregnancy (EP)
Intra-Uterine Pregnancy (IUP)
Positive Pregnancy Test
TVS 10% 90%
Diagnostic Non-diagnostic
Pregnancy of Unknown Location
IUP EP Failing PUL
Persistent PUL

Viable Intrauterine Pregnancy = 6+5
Sarah…..

CRL Subsequent loss of viability < 5mm 7.2% 6-10mm 3.3% > 10mm 0.5%
Miscarriage rates once FH seen

Non-invasive pre-natal testing Harmony, Panorama, Nifty
Nuchal USS
Booking for antenatal care Bloods : FBC, Sickle and Thalassaemia screen, Rubella,
Hep B, Syphillis serology, Blood group and antibody MSU
What next?

42 years old G1P0 9+5 according to LMP Moderate PV bleeding 1st positive pregnancy test 4 weeks
ago
Hannah……

‘Early Intrauterine Pregnancy of Uncertain Viability’ Rescan 7-14 days
Hannah……

Empty Sac (Empty GS ≥ 25 mm diameter)
Missed Miscarriage (CRL ≥ 7mm no FH)
Criteria for diagnosis of miscarriage
Addendum to GTG No 25 (Oct 2006): The Management of Early Pregnancy Loss
2011

Misdiagnosis of miscarriage

27 years old G1P0 ?3+2 according to LMP Positive pregnancy test Unplanned pregnancy Took emergency contraception
Estelle……

Left tubal ectopic pregnancy Serum hCG 1708 IU/L Laparoscopic left salpingectomy
Estelle……

Ectopic Pregnancy
11 in 1000 pregnancies >10,000 diagnosed in the UK each year > 90% can be diagnosed on USS prior to treatment
Risk factors: Tubal damage – infection, surgical Age Smoking IVF IUCD use

Ectopic Pregnancy Interstitial
Intramural
Cervical
Tubal
LSCS Scar

Ectopic Pregnancy Management
1. Surgical Laparoscopic or open Salpingectomy / salpingostomy
2. Medical Methotrexate
3. Expectant
No difference in subsequent intrauterine pregnancy rates, however the ectopic pregnancy is managed.

36 years old G3P2
5+6 according to LMP Heavy PV bleed
Nadia……
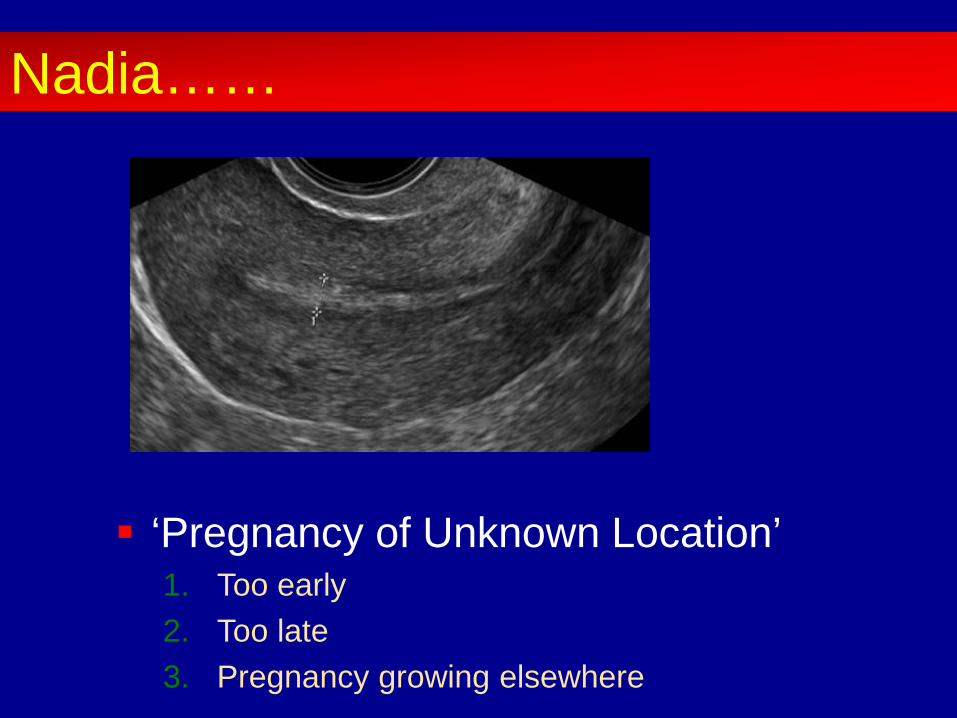
‘Pregnancy of Unknown Location’ 1. Too early 2. Too late 3. Pregnancy growing elsewhere
Nadia……

• Absence of an intra-uterine pregnancy
• Inspection of Pouch of Douglas for echogenic free fluid
• Clear visualization of both ovaries and adnexae
• Inspection of interstitial portion of Fallopian tubes
Classification as a PUL

5/40 PV spotting
• Gestation sac may be visualised from 31 days (4+3)
• Gestational age unreliable: – Wrong dates – Irregular cycles – Failing pregnancy
4/40 Mild pelvic pain
PUL – Early intrauterine pregnancy?

• 5.9% women presenting with apparent complete miscarriage (heavy bleeding with clots and empty uterus on TVS) found to have an ectopic pregnancy
Condous et al., 2005
• If no previous USS confirming IUP – treat as a PUL
9/40 Heavy bleeding with clots
? 6/40 PV spotting
PUL – Miscarriage?

• 74% ectopic pregnancies visualised on first TVS performed
• 25% initially classified as a PUL
• 6.8% PUL ultimately diagnosed as an ectopic pregnancy
Kirk et al. 2007
7/40 PV spotting
PUL – Ectopic pregnancy?

• Ectopic pregnancy • Intra-uterine pregnancy • Failing PUL • Persistent PUL
7-20% 30-50% 50-70% < 5%
PUL - Clinical Outcomes

Serial hCG levels 0 hrs: 435 IU/L 48 hrs: 96 IU/L
Progesterone level 8 nmol/L
Negative pregnancy test 2 weeks later
Nadia……

18 years old G1P0
10+3 according to LMP PV bleeding Unplanned pregnancy USS at BPAS – no pregnancy seen
Charlie……
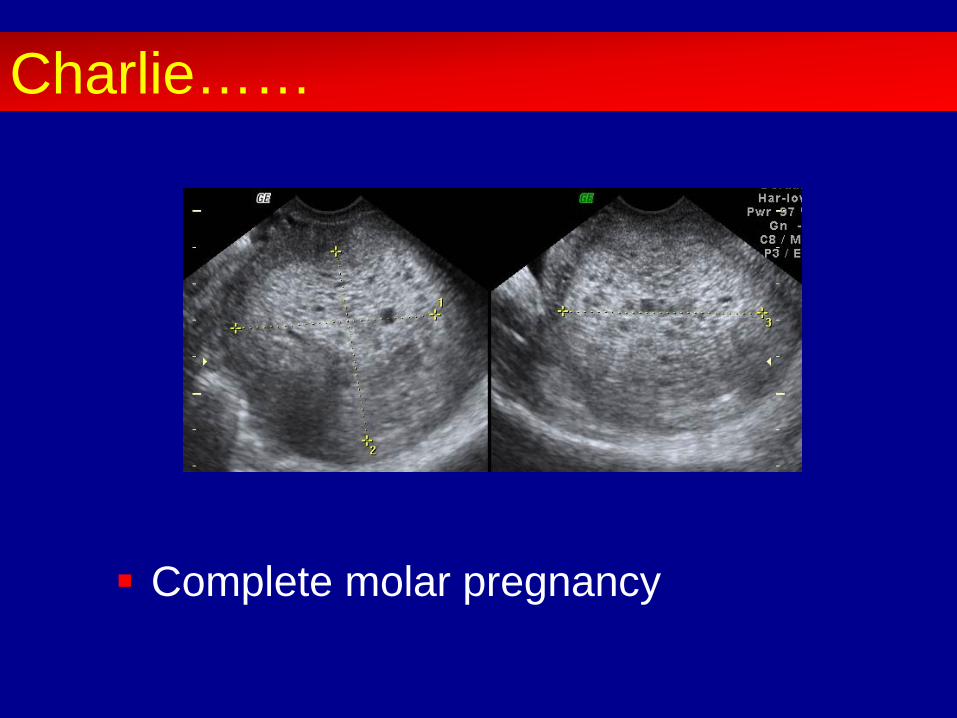
Complete molar pregnancy
Charlie……

1 in 750 pregnancies Increased risk at extremes of reproductive
age Refer to Regional Trophoblastic Centre
Risk of malignancy:
Partial mole - < 1% Complete mole – 8-20%
Gestational Trophoblastic Disease

Surgical evacuation of the uterus Histology confirmed complete molar
pregnancy Referred to Charing Cross Regional
Trophoblastic Unit
Charlie……

28 years old G2P1
7+2 according to LMP Vomiting Urine ketones ++++.
Roshni……

Excessive vomiting Ketosis > 5% loss in body weight
IV fluids Anti-emetics Vitamins
USS for reassurance
Hyperemesis Gravidarum

USS often recommended to exclude multiple pregnancies and GTD
Case control study – 286 cases of HG, 286 controls - 3.1% incidence of twins in each group (P>0.999) - incidence of early pregnancy failure 0.7% in women with HG compared
to 7.0% in controls (P<0.0001) - one case of GTD had HG but also had bleeding - USS therefore not clinically necessary other than for maternal
reassurance Kirk et al 2006, Hum Reprod
Hyperemesis Gravidarum

Viable monochorionic diamniotic twin pregnancy
Roshni……

Number of chorionic sacs can be accurately assessed by 5 weeks.
Number of fetuses must wait until the 6th week when heart beats can be seen.
After 7-8th week – amnionicity can be determined.
Multiple Pregnancy

• Any concerns refer for early assessment including USS: Pregnancy location Viability Accurate dating to time future tests Amnionicity and chorionicity in multiple pregnancies
• No need for routine speculum examinations or serum hCG levels
Summary

When the normal pregnancy becomes abnormal
Job Title – Department The Portland Hospital
Miss Shazia Malik MRCOG Consultant O&G
Subspecialist Reproductive Medicine www.shaziamalik.co.uk

• Mild hypertension diastolic blood pressure 90–99 mmHg, systolic blood pressure 140–149 mmHg.
• Moderate hypertension diastolic blood pressure 100–109 mmHg, systolic blood pressure 150–159 mmHg.
• Severe hypertension diastolic blood pressure 110 mmHg or greater, systolic blood pressure 160 mmHg or greater
NICE Hypertension definitions

• Chronic hypertension is hypertension that is present at the booking visit or before 20 weeks or if the woman is already taking antihypertensive medication when referred to maternity services. It can be primary or secondary in aetiology.
• Eclampsia is a convulsive condition associated with pre-eclampsia. • HELLP syndrome is haemolysis, elevated liver enzymes and low
platelet count. • Gestational hypertension is new hypertension presenting after
20 weeks without significant proteinuria. • Pre-eclampsia is new hypertension presenting after 20 weeks with
significant proteinuria. • Severe pre-eclampsia is pre-eclampsia with severe hypertension
and/or with symptoms, and/or biochemical and/or haematological impairment.
• Significant proteinuria urinary protein:creatinine ratio is greater than 30 mg/mmol or a validated 24-hour urine collection result shows greater than 300 mg protein.
NICE Hypertension definitions

• Assess risk of gestational diabetes using risk factors in a healthy population. At the booking appointment, determine the following risk factors for gestational diabetes:
• BMI above 30 kg/m2 • previous macrosomic baby weighing 4.5 kg or above • previous gestational diabetes • family history of diabetes (first-degree relative with
diabetes) • minority ethnic family origin with a high prevalence of
diabetes. Offer women with any one of these risk factors testing for gestational diabetes
NICE Gestational Diabetes

Testing • Use the 2-hour 75 g oral glucose tolerance test (OGTT) to
test for gestational diabetes in women with risk factors (see recommendation 1.2.2). [2015]
• Offer women who have had gestational diabetes in a previous pregnancy:
• early self-monitoring of blood glucose or • a 75 g 2-hour OGTT as soon as possible after booking
(whether in the first or second trimester), and a further 75 g 2-hour OGTT at 24–28 weeks if the results of the first OGTT are normal. [new 2015]
• Offer women with any of the other risk factors for gestational diabetes a 75 g 2-hour OGTT at 24–28 weeks. [2015]
NICE Gestational Diabetes

Diagnosis • Diagnose gestational diabetes if the woman has either: • a fasting plasma glucose level of 5.6 mmol/litre or
above or • a 2-hour plasma glucose level of 7.8 mmol/litre or
above. [new 2015] • Offer women with a diagnosis of gestational diabetes
a review with the joint diabetes and antenatal clinic within 1 week. [new 2015]
• Inform the primary healthcare team when a woman is diagnosed with gestational diabetes [new 2015]
NICE Gestational Diabetes

Growth Assessment (GAP) Programme Rationale • Most 'unexplained' stillbirths were growth restricted • Customised charts and appropriate protocols should be used • Most stillbirths with IUGR are avoidable • Standardised FH measurement and referral improves detection • A/N detection improves outcome and reduces SB • In high risk pregnancy, serial scans improve detection

Growth Assessment (GAP) Programme
GAP is based on three key elements:
1. Implementation of evidence based protocols and guidelines 2. Training and accreditation of all staff involved in clinical care 3. Rolling audit and benchmarking of performance

Growth Assessment (GAP) Programme • Customised charts (GROW) delineate the Gestation Related Optimal Weight for
each baby, by
• adjusting for characteristics such as maternal height, weight, parity and ethnic origin
• predicting the growth potential by excluding pathological factors such as smoking and diabetes
GROW charts • improve the antenatal detection of fetal growth problems • avoid unnecessary investigations and • reduce anxiety by reassuring mothers when growth is normal.

Fetal Growth - Fundal Height Measurements
Explain the procedure to the mother and gain verbal consent Wash hands Have a non-elastic tape measure to hand Ensure the mother is comfortable in a semi-recumbent position, with an empty bladder Expose enough of the abdomen to allow a thorough examination 1. Mother semi-recumbent, with bladder empty. Ensure the abdomen is soft (not contracting) Perform abdominal palpation to enable accurate identification of the uterine fundus. 2. Palpate to determine fundus with two hands. Use the tape measure with the centimetres on the underside to reduce bias

Fetal Growth - Fundal Height Measurements 3. Secure tape with hand at top of fundus. Measure from the top of the fundus to the top of the symphysis pubis The tape measure should stay in contact with the skin 4. Measure to top of symphysis pubis. Measure along the longitudinal axis without correcting to the abdominal midline Measure only once 5. Measure along longitudinal axis of uterus, note metric measurement. Record the metric measurement and plot it on the growth chart.
6. Plot on customised chart, record in notes •
GROW Chart

Weight and pregnancy • Low BMI
Obese (BMI > 29.9) • Folic acid • Heparin (VTE risk assessment) • PET • GDM • Surgery • Anaesthesia • Labour • Pre-planning essential

IVF Pregnancies • Multiple pregnancy • Maternal age • PGD • PCOS • Egg donation • Paternal factors

Social Factors
• Depression • Domestic abuse • FGM

Urinalysis
• Protein • Leucocytes • Blood • Glucose

Case Studies
• Haematuria in pregnancy • Male fetus posterior urethral valves • Renal failure

When the normal pregnancy becomes abnormal
Job Title – Department The Portland Hospital
Miss Shazia Malik MRCOG Consultant O&G
Subspecialist Reproductive Medicine www.shaziamalik.co.uk
‘WHERE ARE WE GOING WITH LAPAROSCOPIC SURGERY?’ 19th September 2015 Miss Meg Wilson Consultant Obstetrician and Gynaecologist Portland Hospital and Whittington Health

More options to operate laparoscopically.
Attempting to perform fewer diagnostic laparoscopy.
Safer and technically easier surgery (surgical principles).
Future technology
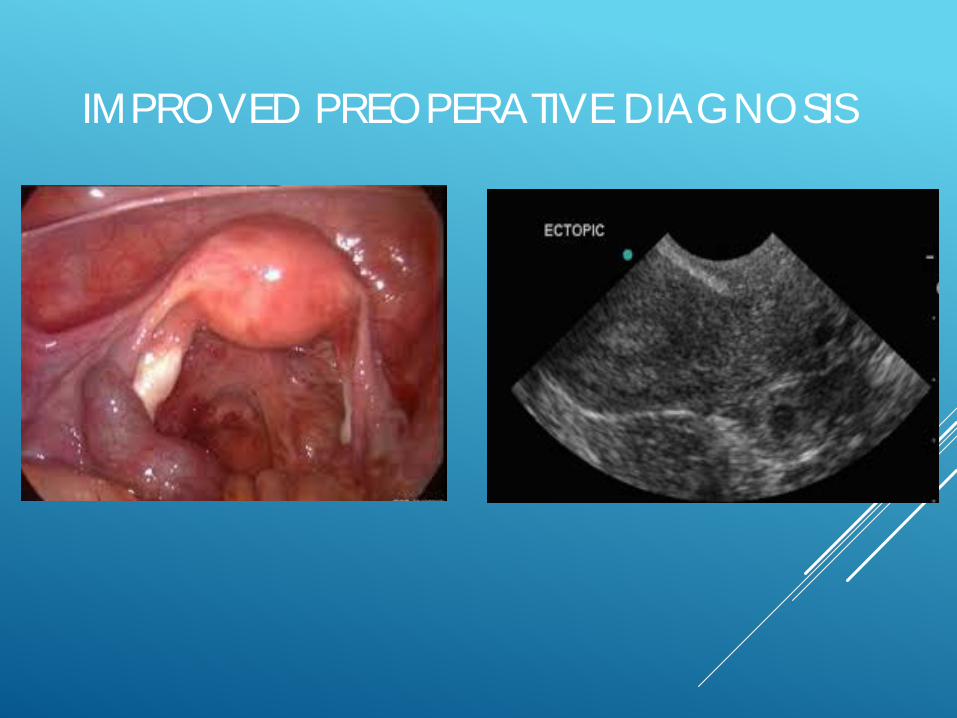
IMPROVED PREOPERATIVE DIAGNOSIS

IMPROVED PREOPERATIVE DIAGNOSIS

IMPROVED PREOPERATIVE DIAGNOSIS

AVOIDING LAPAROTOMY
Hysterectomy Myomectomy Ovarian cystectomy Oophrectomy Ruptured ectopic pregnancy

SAFETY
Risks of laparoscopy 2 in 1000 ‘serious complications’ Training - simulation Equipment improved – Improved safety profile - Laparoscopic entry - Technical advances with equipment

LAPAROSCOPIC ENTRY

SURGICAL INSTRUMENT SAFETY PROFILE- MORCELLATION
Amy Reed – Oct 2013 Laparoscopic hysterectomy for fibroids, using morcellator. Histology diagnosed Leiomyosarcoma. Campaigned to abandon use of the morcellator.

ROBOTICS

• magnified 3D high-definition vision system.
• tiny wristed instruments
that bend and rotate more than the human wrist. enhanced vision, precision, dexterity and control.

NATURAL OROFICE TRANSLUMINAL ENDOSCOPIC SURGERY - NOTES

THANK YOU

Infertility treatment: implications of NICE
guidance Rehan Salim MD MRCOG
Consultant Gynaecologist & Subspecialist in Reproductive Medicine
St Mary’s & Hammersmith Hospitals Imperial College London NHS Trust

NICE fertility guidance cg156
• Evidence based & cost effective
• Best use of resources
• Best patient outcomes
• Best patient satisfaction

Key priorities for implementation
• Defining infertility
• a woman of reproductive age who has not conceived after 1 year of unprotected vaginal intercourse, in the absence of any known cause of infertility, should be offered further clinical assessment and investigation along with her partner
• offer an earlier referral for specialist consultation to discuss the options for attempting conception, further and appropriate treatment where:
• the women is ages 36 years or over
• there is a known clinical cause of infertility or a history of predisposing factors for infertility

Key priorities for implementation
• Unexplained infertility
• do not offer oral stimulation agents (such as clomifene citrate, anastrazole or letrozole) to women with unexplained infertility
• offer IVF treatment to women with unexplained infertility who have not conceived after 2 years (this can include up to 1 year before their fertility investigations) of regular unprotected sexual intercourse
Key priorities for implementation
• Intrauterine insemination
• for people with unexplained infertility, mild endometriosis or “mild male factor infertility” who are having regular unprotected sexual intercourse
• do not routinely offer IUI, either with or with our ovarian stimulation (exceptional circumstances include, for example, when people have social, cultural or religious objections to IVF)
• advise them to try to conceive for a total of 2 years (this can include up to 1 year before their fertility investigations) before IVF will be considered

Key priorities for implementation
• Criteria for referal for IVF
• a full cycle of IVF/ICSI includes ovarian stimulation and transfer of resultant embryos
• in women <40 years who have not conceived after 2 years regular UPSI or after 12 cycles of artificial insemination (with >6 IUI) offer 3 full cycles of IVF
• in women aged 40-42 who have not conceived after 2 years regular UPSI or after 12 cycles of artificial insemination (with >6 IUI) offer 1 full cycle of IVF/ICSI if
• no previous IVF
• “normal” ovarian reserve

Key priorities for implementation
• Embryo transfer strategies
• women <37
• 1st full cycle - single embryo transfer
• 2nd full cycle - single embryo transfer if >1 top quality embryo
• 3rd full cycle - transfer no more than two embryos
• women 37-39
• 1st and 2nd cycle- consider single embryo is >1 top quality embryo
• women 40-42
• consider double embryo transfer
• where a top quality blastocyst is available, use single embryo transfer

Key priorities for implementation
• In summary
• no IUI for unexplained infertility
• IVF if unexplained infertility for >2 years
• single embryo transfer
• increased cycle provision for IVF

IUI 2013 Age Stimulated Unstimulated
<35 13% 3989
3.5% 421
35-37 13% 1627
8% 228
38-37 11% 857
5% 131
40-42 9% 585
<5% 98
43-44 <5% 169
<5% 22
>44 <5% 61
<5% 13 HFEA FOI request 2013

IUI • No longer recommended
• no better than timed intercourse
• increased risk of multiple pregnancy
• no increase in pregnancy rate
• not clinically effective
• not cost effective

IUI pregnancy rate per cycle
Schorsch et al 2013

IUI - cumulative pregnancy rate
Schorsch et al 2013

IUI • Is there still a role
• not on the NHS!
• Unexplained infertility
• thorough work up
• 3 cycles
• 7 day IUI service

IVF • NHS vs NICE
• NW London CCG
• 1 fresh and 1 frozen
• Camden
• 3 fresh and unto 9 frozen
• Islington
• 2 fresh or 1 fresh and 1 frozen

Cumulative pregnancy rate - 3 cycle of IVF
35
57
72
0
20
40
60
80
1st cycle 2nd cycle 3rd cycle

IVF - pregnancy rate per embryo transfer

IVF - number of embryos to transfer?
• Risk of multiple pregnancy
• vs
• Risk of treatment failure

IVF - number of embryos to transfer

IVF - multiple pregnancy rate

Single embryo transfer sET MPR

IVF - summary
• Increased uptake of IVF on NHS
• Improved pregnancy rate per treatment cycle
• Reduction in multiple pregnancy rate

IVF • Not pregnant / no further NHS funding
• revisit IUI
• IVF
• modified
• improved
• diagnostic

Summary
• Shift toward funding for IVF
• IUI units - uncertain future?
• Advances in IVF not accounted for
• probable increase in cost for fertility overall?

Infertility treatment: implications of NICE
guidance Rehan Salim MD MRCOG
Consultant Gynaecologist & Subspecialist in Reproductive Medicine
St Mary’s & Hammersmith Hospitals Imperial College London NHS Trust

WOMEN’S HEALTH GP CONFERENCE
Saturday 19th September| The Royal Society of Medicine
Contact us:
E: [email protected] T: 0207 390 6057 F: 0207 390 6069
Follow us: @PortlandGPConfs
Connect with us: The Portland GP Education


















