Women and work: An investigation of the association between health and employment status in...
9
Sm. Sri. Med. Vol. 19, No. 4, pp. 423-431. 1984 Printed in Great Britain. All rights reserved 0277-9536184 $3.00 + 0.00 Copyright f:, 1984 Pergamon Press Ltd WOMEN AND WORK: AN INVESTIGATION OF THE ASSOCIATION BETWEEN HEALTH AND EMPLOYMENT STATUS IN MIDDLE-AGED WOMEN* SUSAN JENNINGS, CHERYL MAZAIK and SONJA MCKINLAY Cambridge Research Center/AIR, 22 Hilliard Street, Cambridge, MA 02138, U.S.A. Abstract-Considerable controversy has appeared in recent epidemiological literature on the association between unemployment and health. Other recent research suggests that there is an assocaition between women’s employment status and their physical and mental health. Although the nature of this association has still to be specified, it is of increasing importance given the dramatic rise in work force participation in the last few decades. This paper analyzes the results of the first large U.S. epidemiological study of the menopause in over two decades, comprising a random sample (n = 8114, response rate = 77%) from the general population of women aged 45-54 in Massachusetts. Women who were employed for pay (69x), full time homemakers (24%) and women who were unemployed themselves (5%) or living with an unemployed spouse (2%) were included in this analysis of data from the cross-sectional phase of the study. Comparisons between a variety of measures and employment status are reported, as are the intervening effects of sociodemographic variables and social support measures. The importance of the ‘healthy worker effect’, especially for homemakers, is analyzed, Finally, a small subsample of recently unemployed women from the first round of the longitudinal phase of the study is analyzed to demonstrate additional information to be gained through a longitudinal design. Perhaps stimulated by the worldwide economic in- stability characterizing the last decade, a recent de- bate has focused on the possible impact of economic conditions on health. One viewpoint, expressed pri- marily through the work of Brenner [l-6], maintains that increases in mortality and morbidity are associ- ated with downturns in the economy, an analysis of particular interest during this time of high un- employment. Eyer, on the other side of the debate, argues that periods of prosperity result in increased sickness and death in the population. In documenting their positions both Brenner and Eyer, among others, rely on macro-social analyses examining correlations between economic indicators, mainly unemployment rates and population-based health statistics, mainly mortality and morbidity rates. Although Brenner does not focus his investigations on possible causal linkages between the state of the economy and the health of individuals, he does suggest the following factors: decreased financial resources for medical care and adequate diet; in- creased stress; disruption of social support networks; and increased at-risk behaviors such as smoking or alcohol and drug use [3,5,6]. Eyer analyzes similar data but comes to conclu- sions very different than those reached by Brenner. By discounting the lag time between changes in the unemployment rate and mortality rate increases, Eyer locates the source of stress in the boom portion of the *The research for this paper is supported by Grant No. AG-03111 from the National Institute on Aging, National Institutes of Health, Principal Investigator, S. McKinlay, to whom project enquiries should be sent. The authors would like to acknowledge the con- tributions of Sharon Perkins and John B. McKinlay to the preparation of this paper. business cycle rather than in the recessionary periods [7-lo]. He also argues that unemployment does not have enough impact, as measured in previous epi- demiological studies, to account for the variation in the crude death rates associated with the business cycle [I 1, 121. While the argument that economic conditions have an impact on an individual’s health has intuitive appeal, major criticisms of the methodology and analyses in both Brenner and Eyer’s work have been raised. These criticisms have focused on four areas: (1) the particular measures selected to oper- ationalize concepts of health status and economic conditions; (2) the use of ecological data to explain causation on an individual level; (3) the use of statistical methods from economic forecasting, especially detrending and lag analysis, in hypothesis testing; and (4) the inadequacy of the explanation of the mech- anism by which changes in the economy increase the risk for disease and death in the population [13-191. Neither the disagreement between Brenner and Eyer nor the criticism of their work rules out the existence of an association between economic in- stability and health outcomes, or diminishes its relevance for health policy. Studies of individuals experiencing job loss [20-221 find an association between job loss and negative health outcomes, although the exact nature of this relationship is complex. Personal characteristics of unemployed individuals and their social environment seem to influence the health outcomes experienced. However, studies of this nature have been criticized on the basis of the questionable generalizability of results from small samples or homogeneous populations [23]. 423
-
Upload
susan-jennings -
Category
Documents
-
view
212 -
download
0
Transcript of Women and work: An investigation of the association between health and employment status in...

Sm. Sri. Med. Vol. 19, No. 4, pp. 423-431. 1984 Printed in Great Britain. All rights reserved
0277-9536184 $3.00 + 0.00 Copyright f:, 1984 Pergamon Press Ltd
WOMEN AND WORK: AN INVESTIGATION OF THE ASSOCIATION BETWEEN HEALTH AND
EMPLOYMENT STATUS IN MIDDLE-AGED WOMEN*
SUSAN JENNINGS, CHERYL MAZAIK and SONJA MCKINLAY Cambridge Research Center/AIR, 22 Hilliard Street, Cambridge, MA 02138, U.S.A.
Abstract-Considerable controversy has appeared in recent epidemiological literature on the association between unemployment and health. Other recent research suggests that there is an assocaition between women’s employment status and their physical and mental health. Although the nature of this association has still to be specified, it is of increasing importance given the dramatic rise in work force participation in the last few decades. This paper analyzes the results of the first large U.S. epidemiological study of the menopause in over two decades, comprising a random sample (n = 8114, response rate = 77%) from the general population of women aged 45-54 in Massachusetts. Women who were employed for pay (69x), full time homemakers (24%) and women who were unemployed themselves (5%) or living with an unemployed spouse (2%) were included in this analysis of data from the cross-sectional phase of the study. Comparisons between a variety of measures and employment status are reported, as are the intervening effects of sociodemographic variables and social support measures. The importance of the ‘healthy worker effect’, especially for homemakers, is analyzed, Finally, a small subsample of recently unemployed women from the first round of the longitudinal phase of the study is analyzed to demonstrate additional information to be gained through a longitudinal design.
Perhaps stimulated by the worldwide economic in- stability characterizing the last decade, a recent de- bate has focused on the possible impact of economic conditions on health. One viewpoint, expressed pri- marily through the work of Brenner [l-6], maintains that increases in mortality and morbidity are associ- ated with downturns in the economy, an analysis of particular interest during this time of high un- employment. Eyer, on the other side of the debate, argues that periods of prosperity result in increased sickness and death in the population. In documenting their positions both Brenner and Eyer, among others, rely on macro-social analyses examining correlations between economic indicators, mainly unemployment rates and population-based health statistics, mainly mortality and morbidity rates.
Although Brenner does not focus his investigations on possible causal linkages between the state of the economy and the health of individuals, he does suggest the following factors: decreased financial resources for medical care and adequate diet; in- creased stress; disruption of social support networks; and increased at-risk behaviors such as smoking or alcohol and drug use [3,5,6].
Eyer analyzes similar data but comes to conclu- sions very different than those reached by Brenner. By discounting the lag time between changes in the unemployment rate and mortality rate increases, Eyer locates the source of stress in the boom portion of the
*The research for this paper is supported by Grant No. AG-03111 from the National Institute on Aging, National Institutes of Health, Principal Investigator, S. McKinlay, to whom project enquiries should be sent. The authors would like to acknowledge the con- tributions of Sharon Perkins and John B. McKinlay to the preparation of this paper.
business cycle rather than in the recessionary periods [7-lo]. He also argues that unemployment does not have enough impact, as measured in previous epi- demiological studies, to account for the variation in the crude death rates associated with the business cycle [I 1, 121.
While the argument that economic conditions have an impact on an individual’s health has intuitive appeal, major criticisms of the methodology and analyses in both Brenner and Eyer’s work have been raised. These criticisms have focused on four areas:
(1) the particular measures selected to oper- ationalize concepts of health status and economic conditions;
(2) the use of ecological data to explain causation on an individual level;
(3) the use of statistical methods from economic forecasting, especially detrending and lag analysis, in hypothesis testing; and
(4) the inadequacy of the explanation of the mech- anism by which changes in the economy increase the risk for disease and death in the population [13-191.
Neither the disagreement between Brenner and Eyer nor the criticism of their work rules out the existence of an association between economic in- stability and health outcomes, or diminishes its relevance for health policy. Studies of individuals experiencing job loss [20-221 find an association between job loss and negative health outcomes, although the exact nature of this relationship is complex. Personal characteristics of unemployed individuals and their social environment seem to influence the health outcomes experienced. However, studies of this nature have been criticized on the basis of the questionable generalizability of results from small samples or homogeneous populations [23].
423

424 SUSAN JENNINGS et al.
Catalan0 and Dooley [23] have attempted to com- bine both levels of analysis in their most recent work -a large-scale longitudinal survey. They examine a series of measures of the economy of the Los Angeles- Long Beach metropolitan area as well as individual- level data gathered from respondents on health status, age, sex, socio-economic status and the experi- ence of job-related and other stressful life events. Although recommending further study, their findings support two important associations: first, that be- tween contraction in the economy and the individual experience of negative job or financial events; and second, that between the experience of negative job or financial events and increased reporting of illness or injury. In the iirst case the association holds only for middle class respondents, thus indicating a need to clarify the reasons for this differential impact. In the second case, they note the limited number of individual characteristics studied and suggest further investigation in order to specify the re- lationship. Finally, Catalan0 and Dooley, find no evidence for a connection between ‘positive’ job or financial events and increased reporting of illness and injury that would be consistent with Eyer’s hypothesis.
Almost all of the work to date has focused on ‘macro’ statistics and/or samples of men, or of both sexes. There has been a deaith of research which includes large numbers of women and sufficient data on their employment circumstances. At the national level, the U.S. Current Population Survey, for exam- ple, does not include data on health, while the U.S. Health Interview Survey considers only ‘current’ or ‘usual’ occupation. Several studies have examined the complex relationship between employment status and health in women, but the utility of these studies has been limited both by inappropriate study design and by the failure to consider potentially important inter- vening variables that might confound the relationship [24,25].
The importance of studying the impact of employ- ment on the health of women lies in such features as: (a) their increasing labor force participation and (b) the existence of a substantial proportion who do not consider themselves in the labor force, but rather ‘homemakers’.
Female labor force participation has undergone considerable change over the last four decades. The percentage of women employed for pay has increased from 33% in 1950 to 53% in 1975, with prediction of over 60% by 1990 [26,271. This trend encompasses increasing numbers of single women who work to support themselves and their families as well as married women who are part of dual-income families [ZS]. In 1982, approx. 17% of all families were maintained by a woman and 51% of all married women were employed or looking for work 1291. The type of labor force participation has also changed with the number of women employed in managerial positions, the professions, and other traditionally male occupations increasing markedly [24, 291. Fur- thermore, in line with their increased labor force participation, women now constitute a sizeable pro- portion (42%) of the unemployed [29]. Therefore, specification of the association between health and employment status in women is an important area of
research with implications for future health policy decisions, especially as previous studies have tended to exclude women.
Looking at the association between health and employment in a sample of women provides a unique opportunity to analyse different subgroups. Com- parisons can be made among employed women, the unemployed but available for employment, and the unemployed but not presently available for employ- ment. Only a study of women includes sufficient numbers, in this last subgroup of individuals who are outside of the paid labor force (i.e. women who categorize themselves as full-time homemakers), thus allowing further specification of the relationship tween unemployment and health. Warr and Parry [30] have noted that while most men without jobs are considered unemployed, not all women without jobs are so labelled. It is also possible to examine. in the same sample, the indirect impact of unemployment on women who report that their partners are un- employed.
This paper has as its goal the further investigation of the relationship between unemployment and health outcomes, with the individual woman as the unit of analysis. To this end, it reports initial results of both cross-sectional and preliminary longitudinal data gathered as part of an ongoing epidemiological study of middle-aged women, which provides an opportunity to examine this controversial association in the context of a wide variety of potentially inter- vening and/or confounding variables in a large- representative sample.
METHODS
The sample
Women born from 1926 to 1936 were sampled from the Massachusetts Street Lists using a two-stage, stratified cluster sampling design, with selectlzn probabilities proportional to size at the first stage and
Table 1. Some socio-demographic characteristics of the cross-
sectional sample (n = 7628)’
Age: Range: 45-55 years at time of survey Mean: SO
Educational background: < I2 years--18.1”” I2 years47.1””
> I2 years-34.8””
Race: White-96.6”” Black- 2.7” Other- 0.7”:
Marital status: Never married- 5.9”” Married living with partner-75.4:;
Divorced. separated, widowed--18.7””
Composition of household: Lives alone- 7.6”; Lives without partner or extended
family but with children-IO. I”:, Lives with partner only-18.0””
Lives with partner and children only49.5”” Lives with partner and extended famdy-14.8””
Employment status: Employed for pay-69. I”” Full-time homemaker-23.7””
Unemployed- 5.1”” Any of above with unemployed spouse- 2.1””
*Full-time students. retired individuals and those with missing information on the employment status questions (6”” of the original sample) were not included in these analyses.

Women and work 425
simple random sampling at the second. As sampling frames, the street lists provide almost complete cov- erage of the state’s voter-eligible adult population, with information on the year of birth and occupation, amon; other items. These lists are updated annually by law in all cities and towns.
Just over 12,000 names were selected for the initial cross-sectional survey and sent a mailed question- naire. Utilizing survey procedures developed by Dillman [31 J. two mailings and a reminder postcard were sent to everyone. Remaining non-respondents were then contacted by telephone, if available, or were sent a final mailing with address correction requested. The overall response rate for this survey was 779~ of eligible respondents (approx. 8100
. women), with higher responses in the lower income towns. Table 1 provides a brief description of the cross-sectional sample. It should be noted that the racial distribution is representative of the Massachu- setts population and does not indicate lower response rates for this subgroup.
Women identified from this survey as pre- menopausal (menses in the last 3 months) are being followed currently with a telephone interview every 9 months for over 4 years. Women without telephones or with unlisted telephone numbers are contacted in person. Just under 3000 were eligible, and the first follow-up was completed with a 96% response rate. Preliminary longitudinal data are also considered for all women reporting a change in status from paid employment on the cross-sectional instrument to unemployment in the first follow-up interview (9 months later). This small subgroup (n = 52 or 1.7%) does not include women who were not employed at the time of the cross-sectional survey, even if they now consider themselves unemployed.
Variables of interesl
The employment status variable was initially di- vided into four, mutually exclusive categories: em- ployed for pay, full time homemaker, unemployed and living with an unemployed spouse regardless of own employment status. Although both full-time and part-time employees were included in the paid employment category, the majority (69.2%) were employed full-time. The unemployed group included women both looking and not looking for work as well as those who were unemployed but with a job to which they might return. Preliminary analysis using the x2 test for independence showed no significant associations (at 51 = 0.05) between type of un- employment and any of the health measures or intervening variables. Additional investigation indi- cated that women who were unemployed themselves
*Only self-perceived health status. and the professional and lay help-seeking variables showed significant associ- ations in x’ analysis with the indirect/direct un- employment variable at cx = 0.05. None were significant at CY = 0.01. Furthermore. there was no particular pattern to non-significant associations in any of the other variables.
tRespondents were asked if they currently had diabetes, high blood pressure. asthma, allergies or eczema, heart disease. an ulcer, arthritis or rheumatism or cancer.
and those with unemployed spouses had similar responses on health status variables, although more of those with unemployed spouses were in the lower education and income groups*. As the total number of women either unemployed or with an unemployed spouse was relatively small (n = 550), it was decided to combine them into one unemployment category for subsequent analyses.
Many large-scale studies have had to rely on limited measures of health status in their analyses. For example, Catalan0 and Dooley [23] used a single dichotomously coded variable to indicate whether the individual had been ill or injured in the 3 months prior to the survey. In order to examine a wider range of possible health associations with unemployment, several measures of health status and health/illness behavior were considered in this analysis. Table 2 provides a detailed list of the health status variables considered.
The selection of potentially intervening or con- founding variables was based on both previous re- search and the data available in the study. To explore the possibility of a healthy worker effect (i.e. the selection process whereby people in poorer health are less likely to seek or gain employment or are more likely to become unemployed than those in better health) suggested by others [25,32], an attempt was made to measure this factor directly. Women not currently employed for pay were asked how im- portant their health status was as a reason for staying home and not joining the labor force. The number of chronic conditions experienced by the respondent was also selected as an indirect measure of this effect?, although it is recognized that the cross- sectional nature of the design does not allow deter- mination of the causal direction of the relationship between this measure of health status and the re- spondent’s employment status. In order to add a measure of severity to the count of chronic conditions experienced, the number of days in the 2 weeks prior to the interview in which the respondent was pre- vented from carrying out her normal activities was incorporated into the measure. A more detailed dis- cussion of the healthy worker effect is provided below.
The importance of socio-economic status @ES) as an intervening variable is indicated in the Catalan0 and Dooley study [23]. Therefore, both education and per capita household income were included in the initial analyses, although it became apparent that they were highly correlated and provided similar measures of socio-economic status in this sample. Since there were considerable missing data on the income variable (n = 1124) and significant differences on health measures were found between those with missing income data and other respondents, it was decided to use education as the measure of SES. Several studies have suggested that social support networks also might provide a mediating effect on the impact of unemployment [20,21,33]. Accordingly, the following measures of social support networks were included: the composition of the respondent’s household and the number of friends and relatives usually seen or talked to at least once a week. A more detailed examination of social support networks is being presented in a separate paper.

426
HEALTH MEASURES (A) Health status variables
SUSAN JENNINGS et al.
Table 2. Variables of interest
iI)
(2)
(3)
(4)
(5)
Self-assessed health status
Compared to other women of the same age: worse, same or better Self-assessed health status
Compared to self last year: worse, same or better Number of physical symptoms
Experienced in 2 weeks prior to survey: total number reported of the following: diarrhea or constipation. persistent cough, stomach ache, backache, headache, sore throat, achesjstiffness in joints Number of psychological symptoms
Experienced in 2 weeks prior to survey: total number reported of the following: dizzy spells, lack of energy, irritability, feeling blue or depressed, shortness of breath, trouble sleeping, loss of appetite Total number of symptoms
Experienced in 2 weeks prior to survey: total number out of all of the physical and psychological symptoms with the addition of cold sweats, hot flushes, menstrual problems and fluid retention
(B) Health /illness behavior variables
(1) Discussing a personal health problem with a health professional in the 2 weeks prior to the survey: yes or no (2) Discussing a personal health problem with a relative or friend in the 2 weeks prior to the survey: yes or no (3) Total number of types of medications used in the 2 weeks prior to the survey from the following list: aspirin/Tylenol or other
non-prescription pain reliever, tranquilizers, diet pills, vitamin/iron/mineral supplements, birth control pills, hormone pills containing estrogen, hormone creams for vaginal dryness, sleeping pills, medicinal herbs or teas, medicine for stomach upset
(4) Tranquilizer or sleeping pill use in the 2 weeks prior to the survey: yes or no (C) Preventive health measures
(1) Pap smear test: within last 3 years, over 3 years ago, never or don’t know (2) Breast self-exam practices: once a month, less often, never (3) Current cigarette use: yes o* no
INTERVENING OR CONFOUNDING VARIABLES (A) Age (in years at last birthday) (B) Education: < 12 years, 12 years, > 12 years (C) Household composition
Lives without partner or extended family (alone or with children) Lives with partner (with or without children) Lives with extended family (with or without family)
(D) Number of relatives usually seen or talked to in one week
0, 1-4, 5 or more (E) Number of friends usually seen or talked to in one week
0, I-4, 5 or more (F) Chronic health conditions
0 chronic conditions and 0 restricted activity days in the prior 2 weeks; Not in the first category but less than two chronic conditions and less than three restricted activity days; in none of the above categories
Table 2 provides additional information on all inter- vening variables.
Analysis
Several methods of analyzing contingency tables were employed because the majority of variables considered were nominal. In general, x2 tests for independence and Cramer’s V statistic were used to evaluate zero-order associations between employ-
ment and health status measures. Residuals were examined in order to determine which cells were contributing the most to the overall x2 statistic. A discussion of these procedures can be found in Blalock [34] or Reynolds [35]. These relationships between employment and health status measures were then examined controlling for potential inter- vening variables, using a summary x2 adjusting for stratification by the levels of the intervening vari-
Table 3. Measures of association between employment status and health measures
Health measure r! Cramer’s V
Health status variables
Current health status compared to other women of same age Current health status compared to self last year Total number of symptoms reported Physical symptoms reported Psychological symptoms reported Health illness behaviors
Professional help-seeking Lay help-seeking Total number of types of drugs Tranquilizer/sleeping pill use Preventative health measures
Pap smear test Breast self-exam practices Current cigarette use
l **p <O.OOl. l *P <O.Ol.
NS = nonsignificant at 3~ = 0.05.
135.776”* 0.096 35.189*** 0.048 35.431*** 0.039 30.971”’ 0.037 43.289”’ 0.044
17.257’*’ 0.048 22.592*‘* 0.055 24.788” 0.033 44.674*** 0.078
10.492 (NS) 0.026
6.7095 (NS) 0.021 5.930 (NS) 0.028
Women and work 427
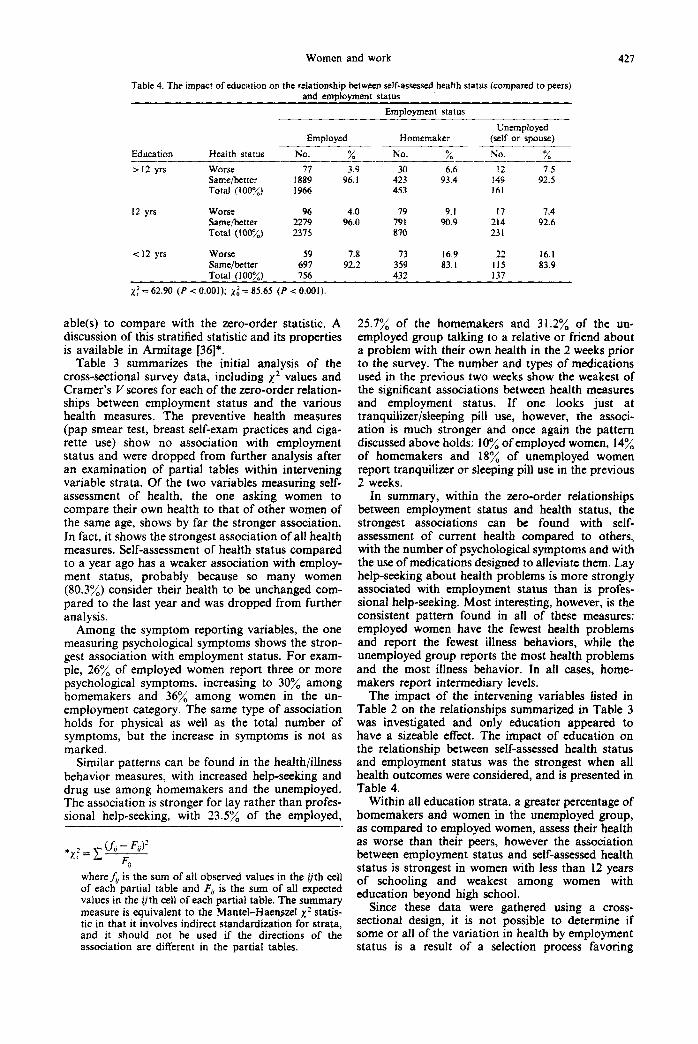
Table 4. The impact of education on the relationship between self-assessed health status (compared to peers) and employment status
Employment status
Education
> 12 yrs
Health status
Worse Same/better Total (100%)
Employed
NO. % -
77 3.9 1889 96. I 1966
Unemployed Homemaker (self or spouse) ---
No. % No. % - ---__ 30 6.6 12 7.5
423 93.4 149 92.5 453 161
12 yrs Worse 96 4.0 79 9.1 17 7.4 Same&etter 2219 96.0 791 90.9 214 92.6 Total (100%) 2375 870 231
t12 yrs worse 59 7.8 73 16.9 22 16.1 Same/better 697 92.2 359 83. I II5 83.9 Total (100%) 756 432 137
x,2 = 62.90 (P < 0.001); ,y: = 85.65 (P < 0.001)
able(s) to compare with the zero-order statistic. A discussion of this stratified statistic and its properties is available in Armitage [36]*.
Table 3 summarizes the initial analysis of the cross-sectional survey data, including x2 values and Cramer’s V scores for each of the zero-order relation- ships between employment status and the various health measures. The preventive health measures (pap smear test, breast self-exam practices and ciga- rette use) show no association with employment status and were dropped from further analysis after an examination of partial tables within intervening variable strata. Of the two variables measuring self- assessment of health, the one asking women to compare their own health to that of other women of the same age, shows by far the stronger association. In fact, it shows the strongest association of all health measures. Self-assessment of health status compared to a year ago has a weaker association with employ- ment status, probably because so many women (80.3%) consider their health to be unchanged com- pared to the last year and was dropped from further analysis.
Among the symptom reporting variables, the one measuring psychological symptoms shows the stron- gest association with employment status. For exam- ple, 26% of employed women report three or more psychological symptoms, increasing to 30% among homemakers and 36% among women in the un- employment category. The same type of association holds for physical as well as the total number of symptoms, but the increase in symptoms is not as marked.
Similar patterns can be found in the health/illness behavior measures, with increased help-seeking and drug use among homemakers and the unemployed. The association is stronger for lay rather than profes- sional help-seeking, with 23.5% of the employed,
where& is the sum of all observed values in the ijth cell of each partial table and F, is the sum of all expected values in the 0th cell of each partial table. The summary measure is equivalent to the Mantel-Haenszel x2 statis- tic in that it involves indirect standardization for strata, and it should not be used if the directions of the association are different in the partial tables.
25.7% of the homemakers and 31.2% of the un- employed group talking to a relative or friend about a problem with their own health in the 2 weeks prior to the survey. The number and types of medications used in the previous two weeks show the weakest of the significant associations between health measures and employment status. If one looks just at tranquilizer/sleeping pill use, however, the associ- ation is much stronger and once again the pattern discussed above holds: 10% of employed women, 14% of homemakers and 18% of unemployed women report tranquilizer or sleeping pill use in the previous 2 weeks.
In summary, within the zero-order relationships between employment status and health status, the strongest associations can be found with self- assessment of current health compared to others, with the number of psychological symptoms and with the use of medications designed to alleviate them. Lay help-seeking about health problems is more strongly associated with employment status than is profes- sional help-seeking. Most interesting, however, is the consistent pattern found in all of these measures: employed women have the fewest health problems and report the fewest illness behaviors, while the unemployed group reports the most health problems and the most illness behavior. In all cases, home- makers report intermediary levels.
The impact of the intervening variables listed in Table 2 on the relationships summarized in Table 3 was investigated and only education appeared to have a sizeable effect. The impact of education on the relationship between self-assessed health status and employment status was the strongest when all health outcomes were considered, and is presented in Table 4.
Within all education strata, a greater percentage of homemakers and women in the unemployed group, as compared to employed women, assess their health as worse than their peers, however the association between employment status and self-assessed health status is strongest in women with less than 12 years of schooling and weakest among women with education beyond high school.
Since these data were gathered using a cross- sectional design, it is not possible to determine if some or all of the variation in health by employment status is a result of a selection process favoring

428 SUSAN JENNINGS et al.
Table 5. The impact of chrome conditions and restricted actiwty (R.A.) days on the relationship between self-assessed health status and employment status
Employment status
Employed Homemaker Unemployed Sickness variable Health status No. “; No. o0 No. n0
No. chronic Worse -F--- I.1 17 31 0 0 cond. or R.A. Same/better 2507 98.9 783 97.9 145 100 days Total (loo?:) 2534 800 145
I Chronic Worse 137 6.1 83 10.7 17 94 cond. and/or Same/better 2116 93.9 694 89.3 164 90.6 I-2 R.A. days Total ( 100%) 2253 717 181
2+ Chronic Worse 68 20.2 85 45 5 25 51.0 cond. and/or Same/better 269 19.8 102 54.5 24 49.0 3+ R.A. days Total (100%) 331 187 49
xi = 94.637 (P < 0.001); zf = 57.264 (P < 0.001). Because of small frequencies. the first two strata of the sickness variable were combined before calculating xi.
Table 6. The impact of chronic conditions and restricted activity (R.A.) days on the relauonstup between tranauilizer use and emalovment status
Sickness variable
Employment status __-
Employed Homemaker Unemployed Tranquilizer _ _.__.___~ ___~ -._.._ --- .~.~ - ..-. _ . . . _... .
“Se No. “:, No. O,, No. 0, 0
No. chronic Yes 170 6.1 60 7.6 16 10.7 cond. or R.A. No 2378 93.3 735 92.4 134 89.3 days Total (100%) 2548 795 150
I Chronic Yes 272 12.0 124 16.0 35 19.8 cond. and/or No 1987 88.0 652 84.0 142 80.2 l-2 R.A. days Total (100%) 2259 776 177
2+ Chronic Yes 74 21.8 58 31.0 IS 36.7 cond. and/or No 266 78.2 129 69.0 31 63.3 3+ R.A. days Total ( 100%) 340 187 49
n;= 37.46 (I’ < 0.001); 1; = 23.46 (P < 0.001).
healthier workers or, conversely, if some or all of the variation in health measures is explained by differences in employment status. Data from the study do suggest, however, that some portion of the association between employment status and health may be explained by a healthy worker effect*. For example, among women in the unemployed group, 3 1.3% report that poor health is of high or medium importance as a reason for not working. The com- parable figure for homemakers is 27.5%.
Two lines of investigation of the healthy worker effect were pursued. First, the variable combining the number of chronic conditions and the number of restricted activity days was used. This ‘sick’ variable was significantly associated (P < 0.001) with the vari- able which rated poor health as a reason for not working. More specifically, in the healthiest category, only 14.1% of the women reported poor health to be of high or medium importance in their decision to stay home, compared to 67.1% in the least healthy category of this variable. Accordingly, the zero-order associations between employment status and mea- sures of health were re-examined controlling for the ‘sick’ variable. Cramer’s V scores were calculated for each partial table and then compared. A consistent
*For the purposes of this portion of the analysis, women who have been considered to be in the unemployed category as a result of their spouse’s unemployment have been removed from consideration.
pattern emerged once again. In every case, within the healthiest group, associations between employment status and measures of health status and illness behavior were weak. Only those with self-assessed health status and tranquilizer/sleeping pill use were significant at CL = 0.05. In the least healthy group, the associations were much stronger, with all but total medication use achieving significance at a = 0.05. The impact of chronic conditions/restricted activity days on the relationship between self-assessed health status and employment status is presented in Table 5. The analagous relationship with tranquilizer use is presented in Table 6. In both cases the size of the zero-order association is reduced when this score is adjusted for stratification by levels of the sickness variable.
In order to investigate further the healthy worker effect, all women reporting that poor health was of moderate or high importance as a reason for not working, i.e. the unhealthy non-workers (n = 509), were deleted from the data set. The association between self-assessed health status (compared to peers) and employment status and that between tranquilizer/sleeping pill use and employment status was re-examined. Tables 7 and 8 summarize these results. With the unhealthy non-workers removed, the x2 value is sizeably reduced. The greatest changes appear among women who label themselves home- makers. In fact, with the unhealthy non-workers removed, employed women and homemakers report

Women and work 429
Table 7. The relationship between employment status and self- assessed health status (compared to peers) with and without
‘unhealthy non-workers’*
Employment status
Employed Homemakers Unemployed _I___ __.__~__~~ ~___ __-
Health status No. _qb___ No. 4; No. %
With ‘unhealrh?: non -workers’ Worse 232 4.5 185 10.5 11.2 Same/better 489 1 95.5 I579 89.5
3;: 88.8
Total (100%) 5123 1764 375 x: = 94.637 (P < 0.0001)
Wirhoul ‘unhealfhy non-workers’ Worse 232 4.5 36 2.7 16 5.1 Same/better 489 1 95.5 1319 97.3 265 94.3 Total (100%) 5123 1355 281
Y:: = 10.94 (P < 0.01)
*Women with unemployed husbands are excluded from analysis.
similar results on the health status and tranquilizer/ sleeping pill use measures. There are reductions in the percentages of unemployed women who assess their health as worse than their peers and report tranquilizer/sleeping pill use, but they are not as large as with homemakers. The x2 values for the associ- ation between health status and employment status do not change markedly when they are adjusted for stratification by education levels or the sickness vari- able: when education is controlled for, xi = 11.75 and 1: = 13.05; when sickness is controlled for, xi = 10.95 and x: = 8.94. The zero-order association between tranquilizer/sleeping pill use and employment status also shows little change after it is adjusted for levels of the sickness variable: xi = 8.42 and xf = 7.60. While it is not possible to establish definitely the existence of a healthy worker effect on the basis of cross-sectional findings, these data suggest that a sizeable portion of the association between health and employment status may be explained by the fact that many women who choose to stay out of the labor force (i.e. homemakers) do so because of poor health. It also appears that a portion of the association between unemployment and health among women may be explained by the fact that some women who become unemployed, lose their jobs because of poor health. Clearly these findings are worth investigating with a prospective study design.
Longitudinal data
Complete data from the first follow-up of the longitudinal phase of the menopause study are not
Table 8. The relationship between employment status and tran- quilizer/sleeping pill use with and without ‘unhealthy non-workers’*
Employment status
Tranquilizer/ Employed Homemakers Unemployed sleeping pill -____ _.
use No. :, No. 9; No. “/,
Wirh ‘unhealthy non-workers’
Yes 516 10.0 242 13.8 69 18.4 No 4630 90.0 1516 86.2 307 81.6 Total (loo:<) 5146 1758 376
x; = 37.46 (P < 0.0001)
Without ‘unheo1th.v non-wrkm’
Yes 516 10.0 130 9.7 43 15.2 No 4630 90.0 1213 90.3 239 84.8 Total (100::) 5146 1343 282
z; = 8.424 (P < 0.015)
*Women with unemployed husbands are excluded from analysis.
available, however it was possible to identify all women who had become unemployed in the 9 months between the cross-sectional survey and the first follow-up. Although lower health status and higher levels of illness behavior were associated with un- employment in the cross-sectional analysis, clearly not all (or even most) of the women experiencing unemployment reported low health status. Despite the limitations of a small sample size (n = 52) it was hoped that preliminary analysis of the longitudinal data would allow identification of characteristics of women who reported negative changes on health measures after experiencing a job loss. These results are inserted more to highlight the advantages of the longitudinal design than to provide definitive findings.
The most noteworthy finding is the low frequency of negative health outcomes. Only 10 women (I 9.2%) reported a decrease in health status, while 6 (11.5%) reported that their health status actually improved. Symptom reporting also showed minor changes. As additional symptoms were added to the list for the follow-up interview, it was necessary to compare the percentage (and not the actual number) of possible symptoms reported. Although anywhere from one- third to one-half of the women had increases in total symptom reporting, physical symptom reporting and psychological symptom reporting, the changes were quite small and the mean percentage change in each case was approximately zero.
Each of the four outcome variables (change in self-assessment of health status, and change in the percentage of the three types of symptoms) was run against the following measures: age, education, household composition, the ‘sick’ variable described above, change in household income or in health insurance coverage, work experience (more than half/ less than half of adult life), occupational category on the cross-sectional survey and a measure of stressful life events involving individuals close to the respondent. Only household income was significantly associated with any of the health change variables (and then only with total symptom change and psychological symptom change). However, many of the tables were too sparse for the x2 statistic to be a valid test. Patterns in the percentage on tables are interesting, with consistent patterns appearing in the following measures: work history, income change, household composition and stressful events. A larger percentage of women who had worked at least half of their adult life, of those experiencing a decrease in household income, of those living in households with no partner or extended family member, and of those experiencing a greater number of stressful events reported a decrease in health status and an increase in all symptom measures. Unfortunately, it was not possible to examine the healthy worker effect in this first follow-up. This analysis will be conducted as soon as the data are available and will be reported at a later date,
DISCUSSION
The consistency of the association between em- ployment status and health measures is striking. These findings are consistent both with the work of’

430 Sus~r-4 JENNINGS er al.
Nathanson [37,38], Woods and Hulka [39] and oth- ers who have found that women who work are healthier than those who do not. While unemployed women are the least healthy, full-time homemakers are less healthy than employed women. These findings are in contrast to those reported by Ver- brugge [40] who found that women outside the paid labor force were the least healthy group. It is possible that differences in ages in the two samples may account for the different findings. Nonetheless, our findings suggest that employment may have health benefits. The consequences of unemployment, at least for middle-aged women, may include both the loss of this protective effect as well as the stressful con- sequences of job loss (e.g. decrease in income, adjust- ment to changes in daily patterns along with changes in the social support network).
The possibility of a healthy worker effect explain- ing a portion of the association between employment status and the various health measures cannot be ruled out and is, in fact, suggested by our findings. Poor health may explain why many women leave or remain out of the labor force, thus accounting for findings that homemakers are less healthy than em- ployed women. Although the healthy worker effect appears to be stronger for homemakers than for unemployed women, poor health may also increase the likelihood of job loss or the difficulty of finding a new job. These findings do not necessarily negate the salutogenic effect of employment noted above as it is impossible to determine, in a sample of middle- aged women, whether the decision to leave the labor force was based on poor health or, conversely, if poor health was a consequence of long-term absence from the labor force and now affects the decision to stay home. Clearly, it will be important to determine the impact of employment on health as well as the impact of health on employment before effective policy re- lating to women and employment can be proposed.
A prospective study, beginning with women in late adolescence and continuing over the life course, would allow the complex relationship between em- ployment and health in women to be completely explained, although a series of smaller prospective studies of women at various life stages would con- tribute to a greater understanding at this question.
Education seems to function as a confounding variable in the association between employment status and health. Once it is controlled for, the associations between employment status and health measures are reduced. However, education has less power as an intervening variable when the unhealthy non-workers are removed from the data set. As the inverse relationship between health status and measures of socio-economic status has been found in numerous previous studies [41], this finding is not surprising. Measures of social support networks do not influence the association between employment and health in this sample. Further analyses with more refined measures of social support networks will be conducted to investigate this finding.
While most relationships discussed are significant, the associations are relatively weak (i.e. small values of Cramer’s V) and differ in strength depending upon the health measure selected for consideration. Furthermore, not all women experience negative out-
comes as a result of job loss (at least within the 9 month period following that job loss). It will be possible to identify the characteristics of women who are most likely to suffer negative consequences and design interventions specifically for them.
Many questions remain unanswered about the complex relationship between employment/unem- ployment and health. The ongoing study of meno- pause from which these data derive will enable us to unravel this relationship. We are currently collecting the following additional information: responses to a clinical depression scale designed for epidemiological research (the CES-D Scale) [42]; detailed measures of social support networks and help-seeking behaviors: and data on lifestyle behaviors such as alcohol use and diet. Given the prospective design, we will be able to link these findings to baseline data reported here and to changes experienced every 9 months. Any changes in employment status can be examined, including re-entry into a job, so that Eyer’s hypothesis can be tested. Finally, it will be possible to link these individual-level data to macro-level changes in the economy at the state or local level.
1.
2.
3.
4.
5.
6.
I.
8.
9.
IO.
II.
12.
13.
14.
15.
16.
17.
REFERENCES
Brenner M. H. Mend Illness and fhe Economy. Har- vard University Press, Cambridge, MA, 1973. Brenner M. H. Economic change and heart disease mortality. Am. .I. pubi. Hlth 61, 606, 1971. Brenner M. H. Trends in alcohol consumption and associated illnesses: some effects of economic changes. Am. J. publ. Hlth 65, 1279, 1975. Brenner M. H. Fetal, infant and maternal mortality during periods of economic instability. Inr. J. Hlth Serv. 3, 145, 1973. Brenner M. H. Mortality and the national economy: a review and the experience of England and Wales. 193676. The Lancer 2, 568, 1979. Brenner M. H. Personal stability and economic security. Social Policy 8, 2, 1971. Eyer J. Prosperity as a cause of death. Int. J. Hlth Serc. 7, 125, 1977. Eyer J. Does unemployment cause the death rate peak in each business cycle? A multifactoral model of death rate chanee. Int. J. Hlth Serv. 7. 625, 1977. Eyer J. Reply to Dr Cooper: a diet/stress interaction hypothesis of coronary heart disease epidemiology. Int. J. HIth Serv. 9, 161, 1979. Eyer J. Hypertension as a disease of modem society. Inc. J. Hlth Serv. 5, 539. 1915. Eyer J. Review of the “Mental Illness and the Econ- omy”. Int. J. Hlth Serv. 6, 139, 1976. Eyer J. Rejoinder to Dr Brenner. Inc. J. Hlth Sem. 6, 157, 1976. Kasl S. Mortality and the business cycle: Some ques- tions about research strategies when utilizing macro- social and ecological data. Am. J. publ. Hlth 69, 784, 1979. Lew E. Mortality and the business cycle, How far can we push an association. Am. J. publ. kth 69,782, 1979. Gravelle H. S. E.. Hutchinson S. and Stein J. Mortalitv and unemployment: a critique of Brenner’s time series analysis. The Lancer 16, 1981. Poll&k E. Book review: “Mental Illness and the Economv”. Am. J. oubl. Hlth 64. 5 12. 1974. Ratcliff K. Comments on Marshall and Funch’s critique of “Mental Illness and the Economy”. J. Hlth sot. Behar. 21, 389, 1980.

Women and work 431
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Colledge M. Economic cycles and health: towards a sociological understanding of the impact of the re- cession on health and illness. Sec. Sci. Med. 16, 1919, 1982. Spruit I. Unemployment and health in macro-social analysis. Sot. Sci. Med. 16, 1903, 1982. Kasl S. and Cobb S. Blood pressure changes in men undergoing job loss: a preliminary report. Psychosomar. Med. 32, 19, 1970. Kasl S., Gore S. and Cobb S. The experience of losing a job: reported changes in health, symptoms and illness behavior. Psychosomat. Med. 37, 106, 1975. Coates D., Moyer S. and Williams B. Yorklea study: symptoms, problems and life events. Can. J. publ. Hlth 60, 1969. Catalan0 R. and Dooley D. Health effects of economic instability: a test of economic stress hypotheses. J. HIth sot. Behar. 24, 46, 1983. Haw M. Women, work and stress: a review and agenda for the future. J. Hith sot. Behav. 23, 132, 1982.- Waldron I. Employment and women’s health. Int. J. Hlth Serv. 10, 435, 1980. U.S. Department of Labor, Bureau of Labor Statistics. U.S. Workina Women: A Data Book. Government Printing Offi&, Washington, DC. 1977. Smith R. Women in the Labor Force in 1990. Urban Institute, Washington, DC, 1979. Kahn-Hut R., Daniels A. and Colvard R. (Eds) Women and Work: Problems and Perspectives. Oxford Univer- sity Press, New York, 1982. U.S. Department of Labor, Bureau of Labor Statistics. Women ut Work: A Chartbook. Government Printing Office, Washington, DC, 1983.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
Warr P. and Parry G. Paid employment and women’s psychological well-being. Psycho/. Bull. 91, 498, 1982. Dillman D. Mail and Telephone Surveys: The Total Design Mefhod. Wiley, New York, 1978. Zimmerman M. and Hartley W. High blood pressure among employed women: a multi-factor discriminant analysis. J. Hlth sot. Behav. 23. 205. 1982. Gore S. The effect of social support in moderating the consequences of job loss. J. Hlth sot. Behav. 19, 157, 1978. Blalock H. Social Statistics, 2nd Edition. McGraw-Hill, New York, 1972. Reynolds H. The Analysis o/‘ Cross-ClassiJication. Free Press, New York, 1977. Armitage P. The chi-square test for heterogeneity of proportion after adjusting for stratification. JI R. Stat. Sot. 28B, 150, 1966. Nathanson C. Illness and the feminine role: a theoretical review. Sot. Sci. Med. 9. 57. 1975. Nathanson C. Social roles and health status among women: the significance of employment. Sot. Sci. Med. 14A, 463, 1980. Woods N. and Hulka B. Symptom reports and illness behavior among employed women and homemakers. J. Communit. Hlth 5, 36, 1979. Verbrugge L. Multiple roles and physical health of women -and men. J. Hlth sot. Behav. 27, 16, 1983. Syme S. L. and Berkman L. Social class, susceptibility and sickness. Am. J. Epid. 104, 1, 1976. Myers J. and Weissman M. Use of a self-report symp- tom scale to detect depression in a community sample. Am. J. Psychiat. 137, 1081, 1980.