
Generations 2014 When the Age Bubble andthe Youth Bubble Collide- for MD Anderson
Upload
stacey-lucianCategory
view
214download
3
When to operate on Adult Scoliosis patients
and when to say ‘No’
Frank Schwab, MDJean-Pierre Farcy, MDNew York University School of Medicine
NYU-Hospital for Joint DiseasesDepartment of Orthopaedic SurgeryNYU-Hospital for Joint DiseasesDepartment of Orthopaedic Surgery

What is Adult Scoliosis?


• Coronal plane deformity
• Sagittal plane deformity
• Imbalance/malalignment– Focal
– Regional
– Global
What is Adult Scoliosis?
Adolescent deformity in an adultAISA
De-novo deformity…of agingDDS
Scoliosis
Prevalence– AIS 2-4% of screened pediatric population
– Adult >60% of screened elderly population#
Demographics :Life expectancy, birth rates….Significant growth of aging population segment
# Schwab et al. SPINE 2005 May 1;30(9):1082-5

Adolescent Idiopathic Scoliosis:surgical treatment
Classification• Lenke• King
Curve pattern• apex• distribution• sagittal• overhang
Skeletal maturity• Risser sign
Surgical strategy
Curve severity• Cobb angle• progression

Adult Scoliosis Scoliosis:treatment approach
Skeletal maturity• Risser sign
PTPain MgmtBracingSurgery
Curve severity• Cobb angle• progression
Cosmesis
Pain
Disability
Classification?

Spineskeletalmaturity
30’sdisc degen.MRI changes
50’sfacet DJDdisc collapse
Unfavorable degeneration
Stable spineankylosis
stenosis spondylo deformity
The aging spine
Adult Scoliosis
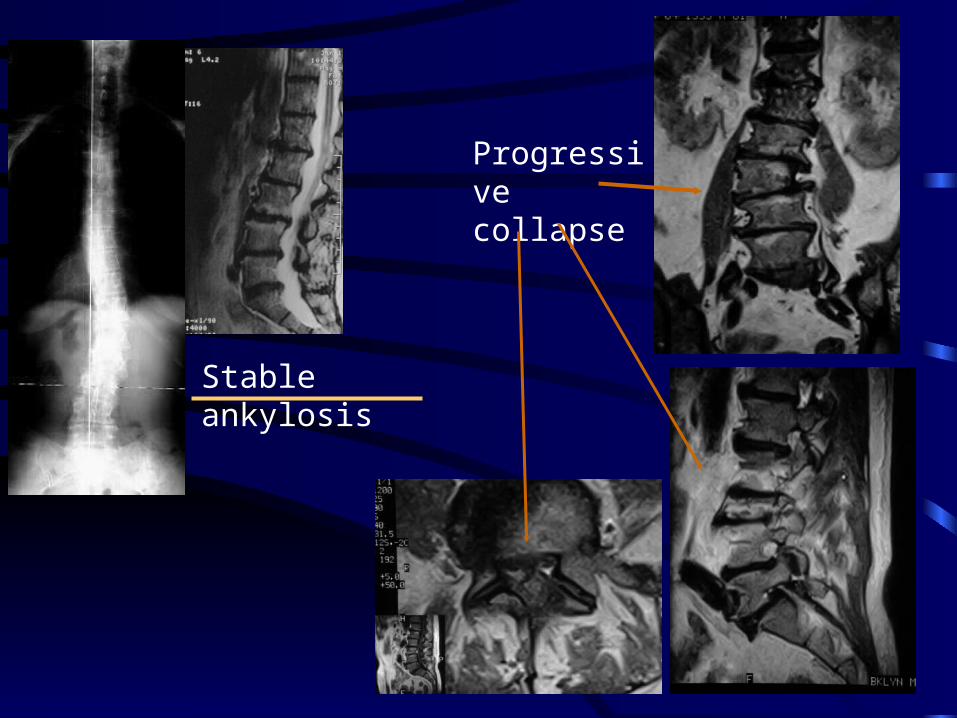
Stable ankylosis
Progressive collapse

Adult Scoliosis / Deformity
What are the disability / pain generators ?
325 patients (Schwab, Farcy. SDSG. SRS 2004)
• thoracolumbar/lumbar scoliosis• SRS instrument, ODI• radiographic-clinical correlation
98 patients (Schwab,Farcy. SPINE 2004)• adult scoliosis, all levels• SF-36 • radiographic-clinical analysis

Adult Scoliosis : Clinical impact
• Significant – Spondylolisthesis
– Lateral Subluxation
– Lumbar lordosis
– Thoracolumbar alignment
– Apical level
– Sagittal Balance (SVA)
• Not significant
– Coronal Cobb
– Age
– Adolescent vs. de-novo degenerative scoliosis
Statistically significant: SRS-22, ODI, SF-12/36

Adult Scoliosis: the disability / pain generators
plain radiographs
• Apical level of deformity (lumbar dominant)
• Lumbar lordosis T12-S1
• Maximal intervertebral subluxation (frontal/sagittal)
• Sagittal balance (PlC7-S1 offset)
Selected for high clinical impact: SRS, ODI, SF-36
(excluding fractures or other pathologies…)

Classification of Adult Deformity
Type I thoracic-only curve (no other curves)II upper thoracic major, apex T4-8 III lower thoracic major, apex T9-T10IV thoracolumbar major curve, apex T11-L1V lumbar major curve, apex L2-L4Type K no scoli (<100), principal sagittal plane deformity
Lumbar Lordosis A marked lordosis >400
Modifier B moderate lordosis 0-400
C no lordosis present Cobb >00
Subluxation 0 no intervertebral subluxation any levelModifier + maximal measured subluxation 1-6mm
++ maximal subluxation >7mm
Sagittal Balance N normal, <4cm positive SVA Modifier P positive, 4-9.5cm
VP very positive, >9.5cm
Schwab et al. SPINE 2006

Adult Scoliosis
Oswestry SRS Function SRS Pain Mean SD Mean SD Mean SD
p = 0.002 p < 0.001 p = 0.007Lordosis modifier A (< -40) 27 19 69 17 65 20
Lordosis modifier C ( >= 0) 37 16 57 15 56 17
Oswestry SRS Function SRS Pain Mean SD Mean SD Mean SD
p < 0.001 p < 0.001 p < 0.001Subluxation Modifier 0 27 20 68 18 64 20
Subluxation Modifier ++ 34 18 63 16 58 19
947 patients: (86% female, 14% male)Average age 48 years (SD 18)Coronal Cobb mean 460 (SD 19)
Lordosis
Subluxation
Global Balance
ODI SRS

Thus….deformity = disability ?
Yes, certain aspects …
… Not coronal Cobb angle
Sagittal plane
Coronal/Sagittal
Adult Scoliosis / Deformity
Focal: subluxationRegional: loss of lordosisGlobal: sagittal imbalance

Young adult: AISA
>500 thoracic
>300 lumbar (progressive)
Progression with disability
Curve progression likely– Disability later (potential)– More difficult to treat later
• Depending upon age
– Surgical risks greater later
Cosmetic concerns
Adult Scoliosis / Deformity: Why surgery ?
Weinstein S,. Spine 24(24), 1999
Pain unacceptable
Disability unacceptable
Risk/Benefit ratio
- favorable
Older Adult:
AISA = DDS
Pain/disability
failed conservative care
Adult Scoliosis / Deformity: Why surgery ?
Adult Scoliosis / Deformity
If the justification for surgery is acceptable….
…..when is it really reasonable to operate
Don’t do it Sure success
?

Not a candidate for surgery:
– young AISA…no disability, mild/mod curve, happy
– patient who does not want surgery
– patient is unlikely to survive surgery
– patient does not understand risk/benefit • unrealistic expectations
– planned operation is not reasonable• experience, team, environment
Adult Scoliosis / Deformity

Possibly Excellent candidate for surgery:
– young AISA…progressive, severe curve (>700)
DDS or AISA older adult:Perfectly isolated pain generator, failed extensive non-operative care
• Well informed, wishes to pursue operative care• Excellent health• Realistic expectations, highly motivated
– team has abundant experience only excellent results with planned intervention
Adult Scoliosis / Deformity

The common cases:
• Patient might consider surgery with certain assurances• Health is acceptable (not ideal), • Pain generators present (there are several), • Non-operative care tried (variable participation and response), • Expectations are overall rather realistic.• The surgeon comfortable with intervention
Adult Scoliosis / Deformity
?

How can we select the best patients for surgery ?(and how to optimize the chances of a successful outcome)
• non-operative care vs. surgery• If surgery…which strategy/approach
– Specific treatment algorithms lacking – few studies to guide us….where is the data ?
When to operate on Adult Scoliosis patients and when to say No

Adult Scoliosis: Thoracolumbar / Lumbar Deformity
Who gets surgery…and what type ? (n=809)
Operative rates– Lordosis
• Lost lordosis vs. good lordosis (B vs. A) 51% vs 37%, p<0.05
– Subluxation modifier• Marked subluxation vs. none (++ vs. 0) 52% vs. 36 %, p<0.05
– Sagittal Balance• Well balanced versus marked imbalance (N vs. VP) 39% vs.59%, p<0.05

Who gets surgery…and what type ?
Use of osteotomiesLordosis >400 lordo vs. no lordo : 25% vs. 50% p=0.01Sagittal balance no imbalance vs. >9.5cm : 25% vs. 53% p=0.01
Surgical ApproachAnterior only: Anterior only: no lost lordosis, no subluxationno lost lordosis, no subluxationCircumferential: some lost lordosis, marked subluxationPosterior only: marked loss of lordosis, marked sagittal imbalance
Fusion to sacrumLordosis Loss of lordosis more likely fusion to sacrum (p = .041)Sagittal Balance increasing positive balance: more fixation to sacrum.
(<4cm: 59%, 4-9.5cm: 80%, >9.5cm: 88%) (all p<0.05)
Adult Scoliosis: Thoracolumbar / Lumbar Deformity

How about surgical outcomes ?
• 111patients 1-year follow up• 45 patients 2-year follow up• Adult Thoracolumbar / Lumbar major curves• Surgical treatment, complete data
– Full-length standing x-rays (0,12,24 months)
– SRS, ODI, SF-12
Adult Scoliosis: Thoracolumbar / Lumbar Deformity

Mean SRS Total Score at Baseline and Two Years by Lordosis Modifier
0
10
20
30
40
50
60
70
80
Baseline Two Year
Measurement Period
Mea
n S
core
Marked Lordosis
Moderate Lordosis
No Lordosis
2-year Surgical outcome: Lordosis modifier
Lordosis modifier ‘C’…most improved
Lumbar Lordosis A marked lordosis >400
Modifier B moderate lordosis 0-400
C no lordosis present Cobb >00

Mean Oswestry Disability Index at Baseline and Two Years by Sagittal Balance Modifier and Surgical Approach
0
10
20
30
40
50
60
Baseline Two Year
Measurement Period
Mea
n S
core
<40 Anterior
<40 Circum
<40 Posterior
40 to 95 Circum
40 to 95 Circum
96+ Circum
96+ Circum
2-year Surgical outcome: sagittal balance (surgical approach)Sagittal Balance N normal, <4cm positive SVA Modifier P positive, 4-9.5cm
VP very positive, >9.5cm
with anterior approach did worst (VP posterior-only also not so good)P, VP did best with circumferential fusion
N
posterior
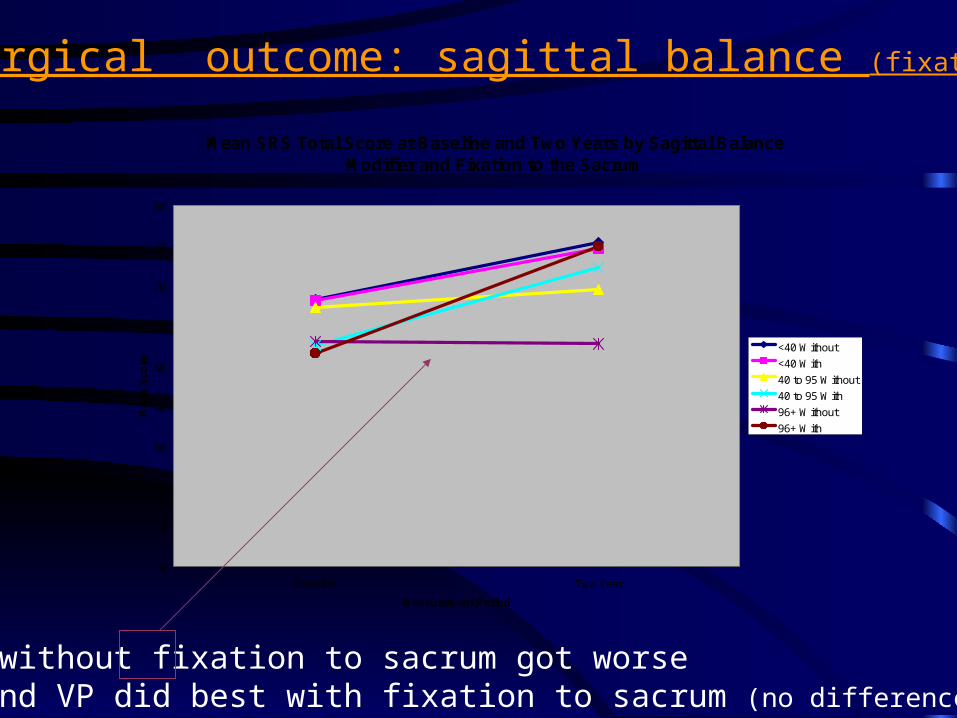
Mean SRS Total Score at Baseline and Two Years by Sagittal Balance Modifier and Fixation to the Sacrum
0
10
20
30
40
50
60
70
80
90
Baseline Two Year
Measurement Period
Mea
n S
core
<40 Without
<40 With
40 to 95 Without
40 to 95 With
96+ Without
96+ With
2-year Surgical outcome: sagittal balance (fixation to sacrum)
VP without fixation to sacrum got worseP and VP did best with fixation to sacrum (no difference for N)

Mean SF-12v2 PCS at Baseline and Two Years by Osteotomy
0
5
10
15
20
25
30
35
40
45
50
Baseline Two Year
Measurement Period
Mea
n S
core
No Osteotomy
Osteotomy
2-year Surgical outcome: osteotomy or not ?
Patients who had osteotomy did better !

Baseline to Two-Year Changes: Significant Interaction
ODI / SRS Total Score by lordosis • patients with no lordosis (C) greatest improvement,
• Patients with marked lordosis (A) little or no improvement
ODI / SRS Total Score by sagittal balance by surgical approach• well balanced least disabled, fused short of sacrum did best• very imbalance (VP) most disabled and worse off if not fused to sacrum
SF-12v2 / SRS Total Score by Subluxation
• significant subluxation (++,+) more improvement than no subluxation
SF-12v2 PCS / SRS Total score by Osteotomy Status
• patients with osteotomy had lower baseline scores •At 2 years f/u, patients with an osteotomy had higher scores

Follow-up data
• When is improvement clinically significant ?
– Set a bar of 10-point increase in SRS score• From 100pt. Scale
– Assumption of patient perceived improvement• Minimal Clinically Important Difference
– Berven et al.
Adult Scoliosis: Thoracolumbar / Lumbar Deformity

Met Ten-Point SRS Improvement Criterion by Year and Gender
62%
100%
69%
100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Female Male
Gender
Pe
rce
nt
Me
eti
ng
Cri
teri
on
One Year
Two Year
Minimum 10 point SRS instrument improvement

Met Ten-Point SRS Improvement Criterion by Year and Lordosis Modifier
57%
67%
100%
61%
78%
100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
A - marked lordosis B - moderate lordosis C - No lordosis present
Lordosis Modifier
Pe
rce
nt
Me
eti
ng
Cri
teri
on
One Year
Two Year
Minimum 10 point SRS instrument improvement
Loss of lumbar lordosis…greater likelihood of clinical success

Met Ten-Point SRS Improvement Criterion by Year and Sagittal Balance Modifier
60%
73%
63%64%
73%
88%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Under 40 40 to 95 96 and Greater
Sagittal Balance Modifier
Pe
rce
nt
Me
eti
ng
Cri
teri
on
One Year
Two Year
Minimum 10 point SRS instrument improvement
At 2-yr follow up:greater imbalance patients more likely to have successful outcome

Met Ten-Point SRS Improvement Criterion by Year and Osteotomy
59%
73%
66%
80%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No Osteotomy Performed Osteotomy Performed
Osteotomy
Pe
rce
nt
Me
eti
ng
Cri
teri
on
One Year
Two Year
Minimum 10 point SRS instrument improvement
Patients having osteotomies more likely to have successful outcome

Met Ten-Point SRS Improvement Criterion by Year and Baseline SF-12 PCS
83%
67%
58%
44%
92%
78%
58%
44%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Under 25 25 to Under 35 35 to Under 45 45 and Higher
Baseline SF-12 PCS
Pe
rce
nt
Me
eti
ng
Cri
teri
on
One Year
Two Year
Minimum 10 point SRS instrument improvement
Patients with lower baseline scores more likely to achieve significant improvement

Can we predict who will have successful surgery ?
How can we select the best patients for surgery ?(and how to optimize the chances of a successful outcome)
When to operate on Adult Scoliosis patients and when to say No

Predictive Models
– Gender
– Age
– Apical Modifier
– Lordosis Modifier
– Subluxation Modifier
– Sagittal Balance
– Surgical Approach– Osteotomy– Fixation to Sacrum– SF-12v2 Physical Component Summary
– SF-12v2 Mental Component Summary
– SRS Total Score – Oswestry Disability Index
Outcome ?

Strength of Predictive Models
Outcome Score
(meeting the
MCID threshold)
% Correct Classification by
Model
Area Under ROC Curve (.80 and above
is considered good discrimination)
% of Surgical Cases Failing to Meet
Criterion
SRS Pain 81.1% .864 39.5%
SRS Appearance 75.4% .838 33.3%
SRS
Pain and Appearance
78.1% .845 53.5%
SF-12v2 PCS 77.9% .862 47.6%
Models to predict Clinical Improvement with Surgery

Follow-up data: Conclusions
The winners– Greater disability at start (SRS, ODI, SF-12)– Male– Subluxation >6mm– Lost lumbar lordosis <400
– Osteotomy
Who benefits least• minimal baseline disability (SRS, ODI, SF-12)
• No subluxation, no marked sagittal imbalance • Good lordosis, >400
• Lack of osteotomy

How can we select the best patients for surgery ?(and how to optimize the chances of a successful outcome)
When to operate on Adult Scoliosis patients and when to say No
SRS, ODI, SF-12
Regional deformity
Focal deformity
Surgical approachosteotomy
Global sagittal balance
apex
gender

+
SRSODISF-12/36
Refine Classification
Predictive outcomes model
Treatment Algorithm
Adult Scoliosis / Deformity: next steps

Thank you….














![MBA Curriculum JOINT DEGREES Course # Course Name MD/MBA ...med.fau.edu/admissions/MD-MBA-and-MD-MHA-Joint-Degree-Progra… · the restrictions on when the MBA portion can be satisfied.]](https://static.fdocuments.net/doc/165x107/5fc073d90fc3557c8c161765/mba-curriculum-joint-degrees-course-course-name-mdmba-medfaueduadmissionsmd-mba-and-md-mha-joint-degree-progra.jpg)



