
October 16, 2015 Mary-Anne Doyle, MD Endocrinology and Metabolism Treatment of Diabetes.
Wendy Washington & Anne Graham Nephrology Nurse Practitioners
Eight major risk factors for CKD Diabetes
High blood pressure Age over 60 years
Smoking Obesity
Family history of kidney disease Aboriginal or Torres Strait Islander origin
Established cardiovascular disease
1 in 3 Australian adults is at increased risk of CKD due to the above risk factors!
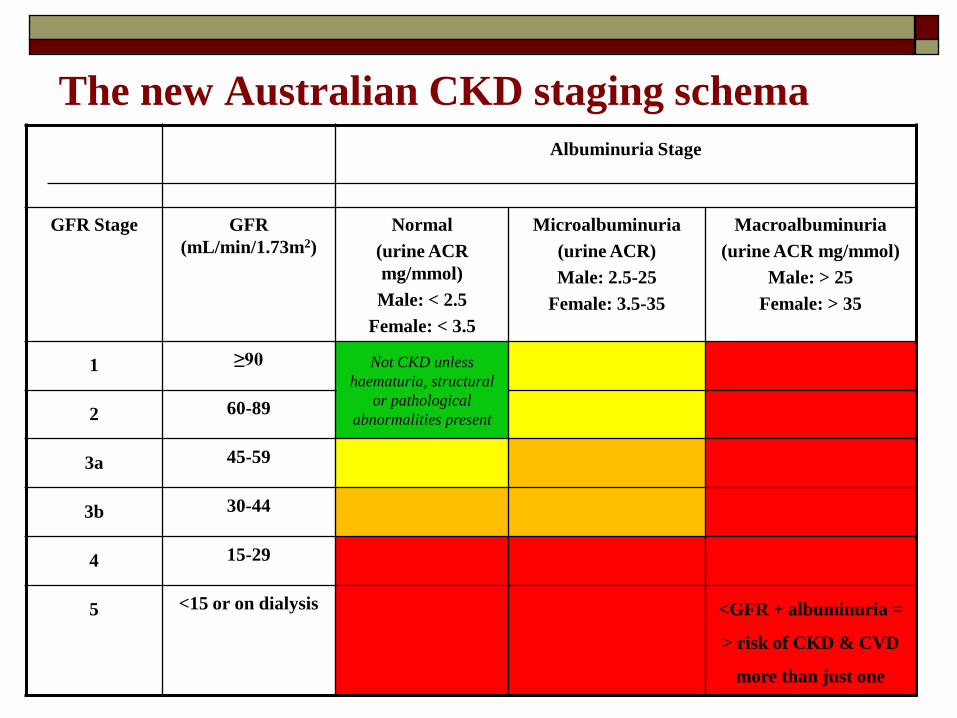
The new Australian CKD staging schema Albuminuria Stage
GFR Stage GFR (mL/min/1.73m2)
Normal (urine ACR mg/mmol) Male: < 2.5
Female: < 3.5
Microalbuminuria (urine ACR) Male: 2.5-25
Female: 3.5-35
Macroalbuminuria (urine ACR mg/mmol)
Male: > 25 Female: > 35
1 ≥90 Not CKD unless haematuria, structural
or pathological abnormalities present 2 60-89
3a 45-59
3b 30-44
4 15-29
5 <15 or on dialysis <GFR + albuminuria =
> risk of CKD & CVD
more than just one
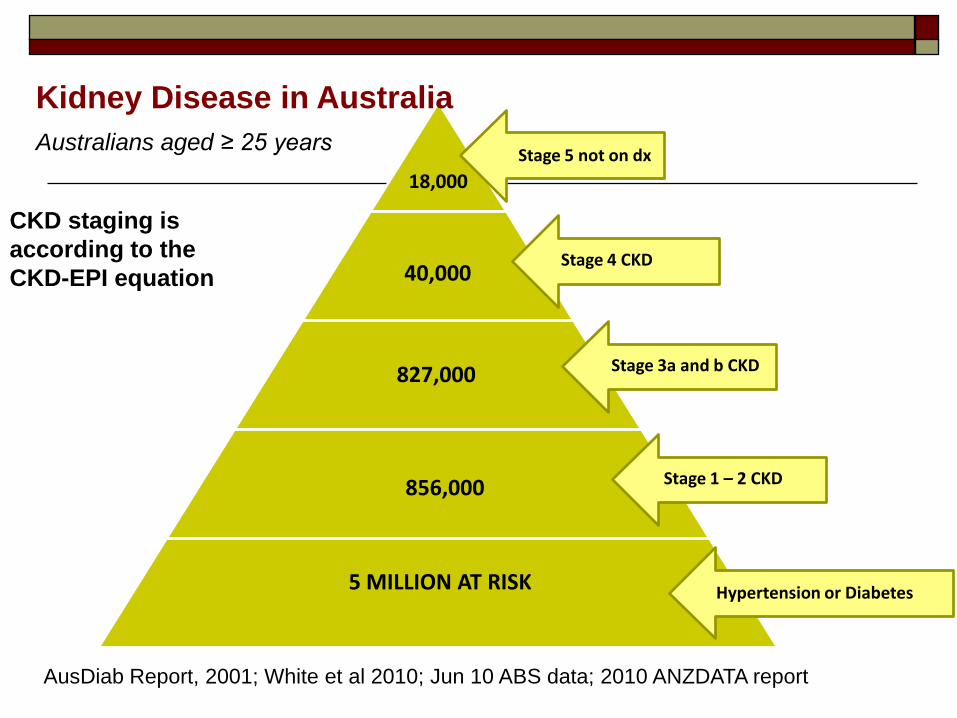
5 MILLION AT RISK
856,000
18,000
40,000
827,000
Stage 5 not on dx
Stage 4 CKD
Stage 3a and b CKD
Hypertension or Diabetes
Stage 1 – 2 CKD
Kidney Disease in Australia
Australians aged ≥ 25 years
CKD staging is according to the CKD-EPI equation
AusDiab Report, 2001; White et al 2010; Jun 10 ABS data; 2010 ANZDATA report
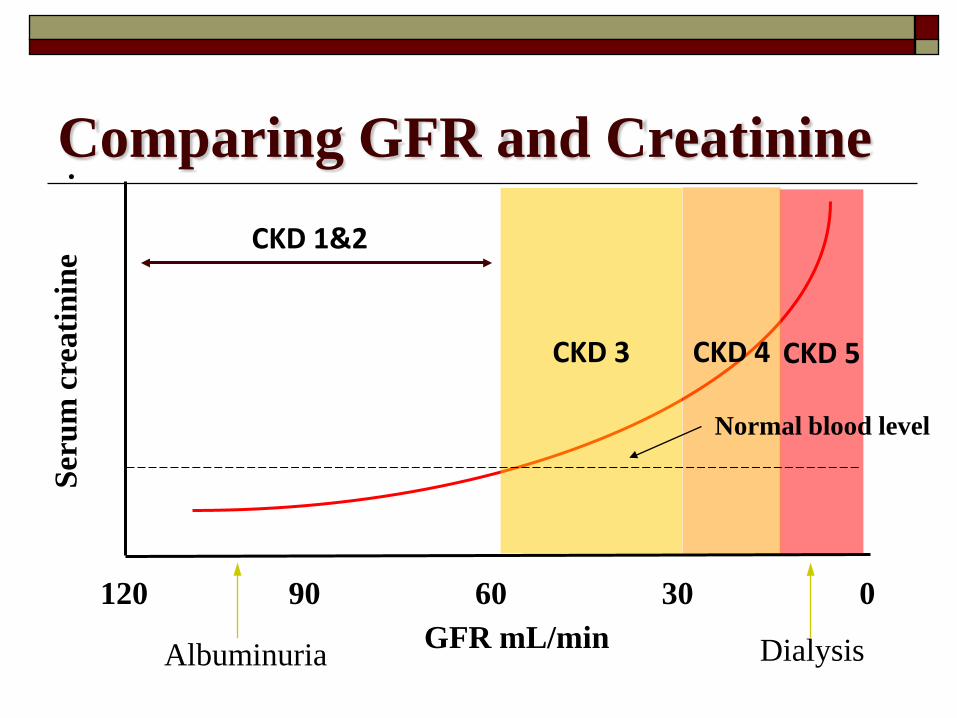
Comparing GFR and Creatinine . CKD 1&2
CKD 5
CKD 4
CKD 3
GFR mL/min Dialysis
120 90 60 30 0
Seru
m c
reat
inin
e
Albuminuria
Normal blood level
Diabetic Kidney Disease (DKD) and end-stage renal disease (ESRD ) in Australia1
DKD is now the most common cause of patients commencing dialysis in Australia (and QLD)1
DKD accounts for 35% of new ESRD patients with 90% of these Type 2 (15% non insulin) (ANZDATA - Australia and NZ)1
Five year survival for diabetics entering dialysis is only 5% compared to 20% for non-diabetics
T1DM ESRD patients have 1.77 relative risk of mortality. T2DM ESRD patients have a 1.27 relative risk of mortality
compared to non-DM patients 1. ANZDATA 2011
Chronic Kidney Disease (CKD) CKD team (North Ward) work to slow
progression, to delay or prevent dialysis. NP, dietitian, social worker 693 patients, 132 JPHS, 559 TTH Diabetes on care plan 226 (?%) 340 (61%) Proteinuria on care plan 9 78 (FERRET database)
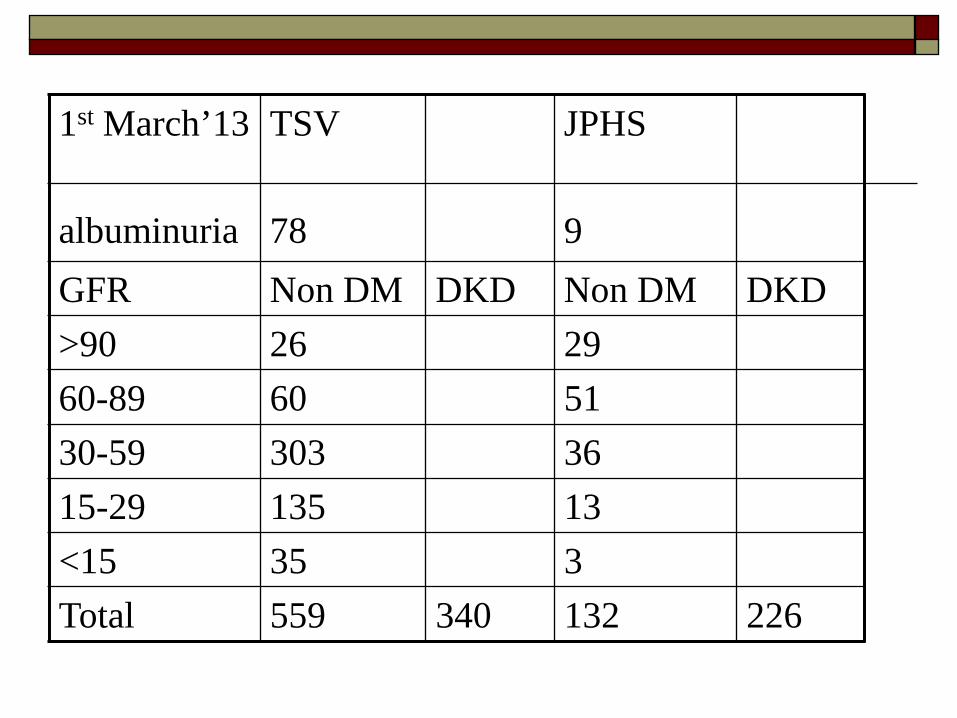
1st March’13 albuminuria
TSV 78
JPHS 9
GFR Non DM DKD Non DM DKD >90 26 29 60-89 60 51 30-59 303 36 15-29 135 13 <15 35 3 Total 559 340 132 226
Principal goals of CKD management
Self Management of chronic conditions to slow progression Reduction of cardiovascular and kidney risk factors Early detection and management of CKD complications Avoid nephrotoxic medications Ensure all medication doses are appropriate for stage of CKD Manage contributing cause Timely referral to a Nephrologist (GFR<30 or <60 if DKD) Discuss by Stage 4 re dialysis, transplant, conservative care If planning haemodialysis, AVF creation at eGFR 15 Home dialysis has best outcomes
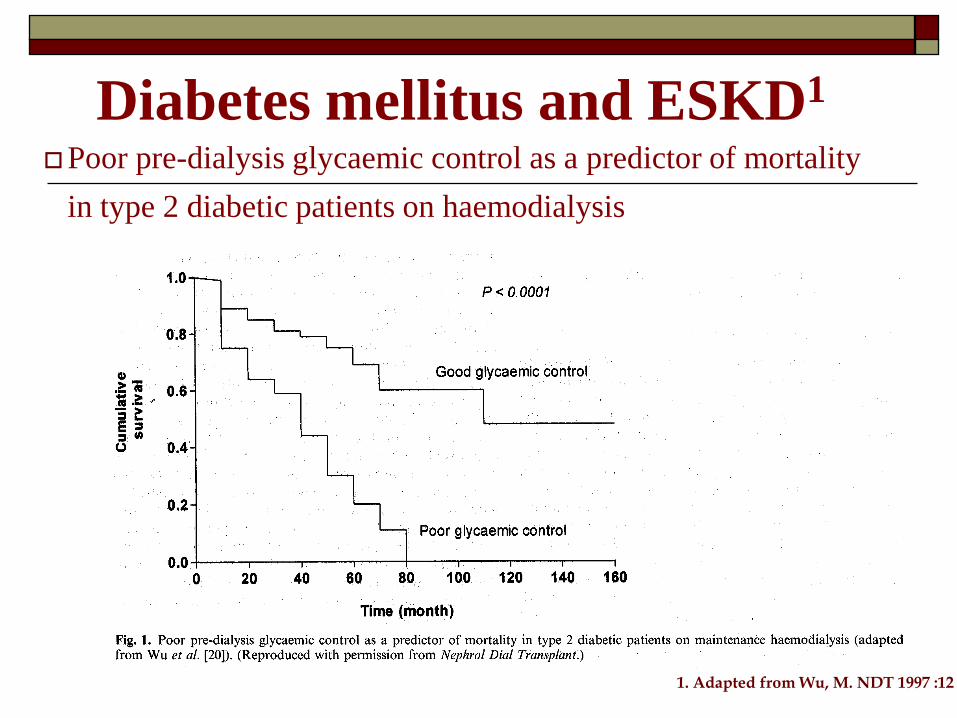
Diabetes mellitus and ESKD1 Poor pre-dialysis glycaemic control as a predictor of mortality
in type 2 diabetic patients on haemodialysis
1. Adapted from Wu, M. NDT 1997 :12

KHA – Diabetic Kidney Disease Major Cause of Kidney Failure - March 2010
Research shows 27% of people commencing dialysis did not see a
Nephrologist until < three months prior to their kidneys failing.
KHA shows only 8.4% of the general population in surveys identifies Diabetes as a cause of kidney disease.
People can lose 90% of their kidney function with no symptoms.
Combined this with a major community information gap over the link
between Type 2 Diabetes and kidney failure.
Screening is simple- Quarterly Blood pressure check
Annual blood and urine (albuminuria, ACR and creatinine)
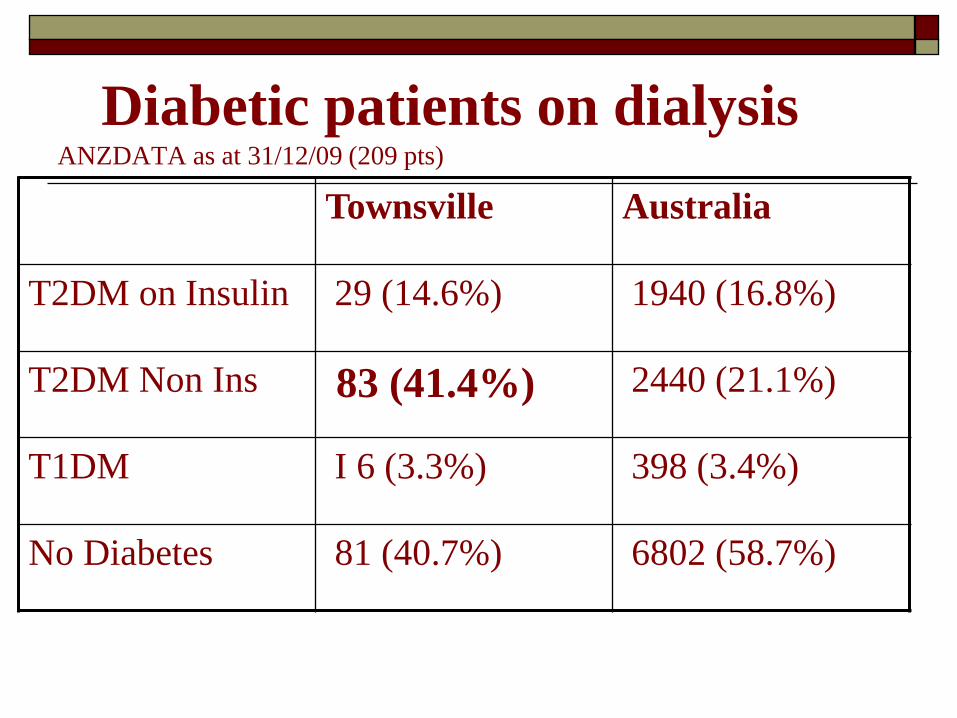
Diabetic patients on dialysis ANZDATA as at 31/12/09 (209 pts)
Townsville Australia
T2DM on Insulin 29 (14.6%) 1940 (16.8%)
T2DM Non Ins 83 (41.4%) 2440 (21.1%)
T1DM I 6 (3.3%) 398 (3.4%)
No Diabetes 81 (40.7%) 6802 (58.7%)
Renal Replacement Therapy
18,999 (474 per million) people received renal replacement therapy at 31st December 2010.
Of these, 8,409 (474 per million) had a functioning kidney transplant and
10,590 (459 per million) receiving dialysis and 1208 (2151 per million) were Aboriginal or Torres Strait Islanders
A clear vision of Starting dialysis
Townsville Patient Treatment Options
Transplant – PAH only after extensive workup Hospital Haemodialysis at TTH Satellite Haemodialysis at:
Home Hill Mt Isa Palm Island North Ward Community Campus
Home: Haemodialysis, CAPD, APD Visiting every 3/4 months; contact monthly
Transplantation Transplant is a treatment, not a cure. Organ
failure and rejection can happen at any time. Medication Forever
Only Qld transplant unit is PAH, Brisbane With Diabetes, aim for combined Pancreas
and Kidney – only Sydney or Melbourne Problems are damage to other organs and
vessels from diabetes may prevent this option
Goals of Dialysis
Remove waste products (urea, creatinine) Remove some toxins Balance electrolytes Replenish bicarbonate (acid base balance) Remove excess water
Haemodialysis regimens Intermittent haemodialysis (3x/wk): Incenter,
Satellite, home. (usually 5 hours) Daily dialysis – done at home. Nocturnal slow dialysis is the best (at home). Haemofiltration, replacement of all the
electrolyte fluid with new
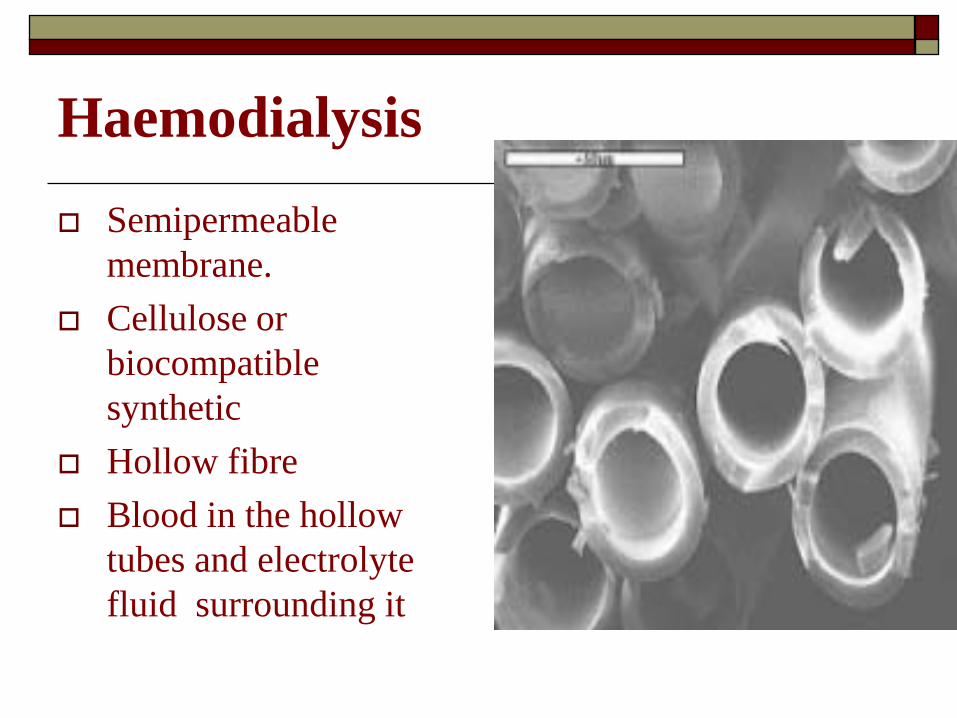
Haemodialysis Semipermeable
membrane. Cellulose or
biocompatible synthetic
Hollow fibre Blood in the hollow
tubes and electrolyte fluid surrounding it
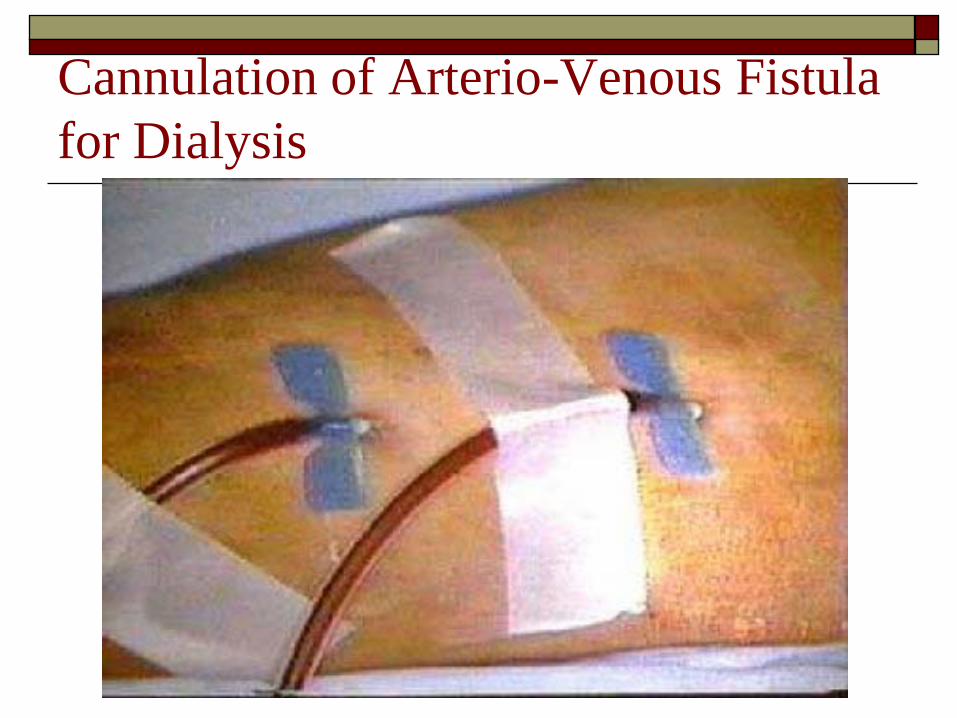
Cannulation of Arterio-Venous Fistula for Dialysis
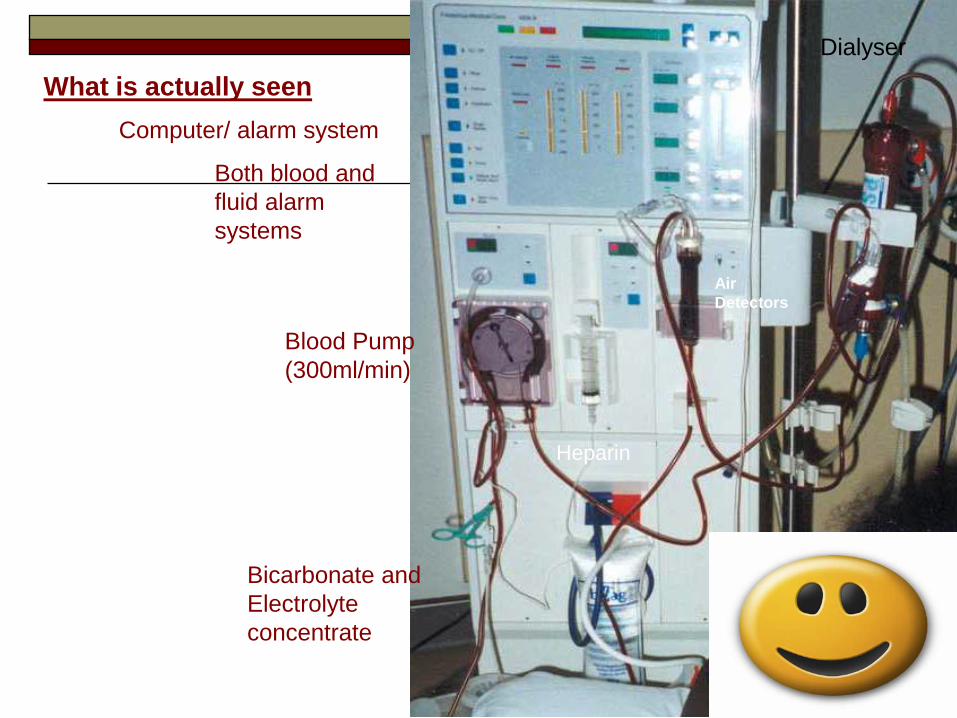
What is actually seen Computer/ alarm system
Both blood and fluid alarm systems
Blood Pump (300ml/min)
Dialyser
Bicarbonate and Electrolyte concentrate
Heparin
Air Detectors
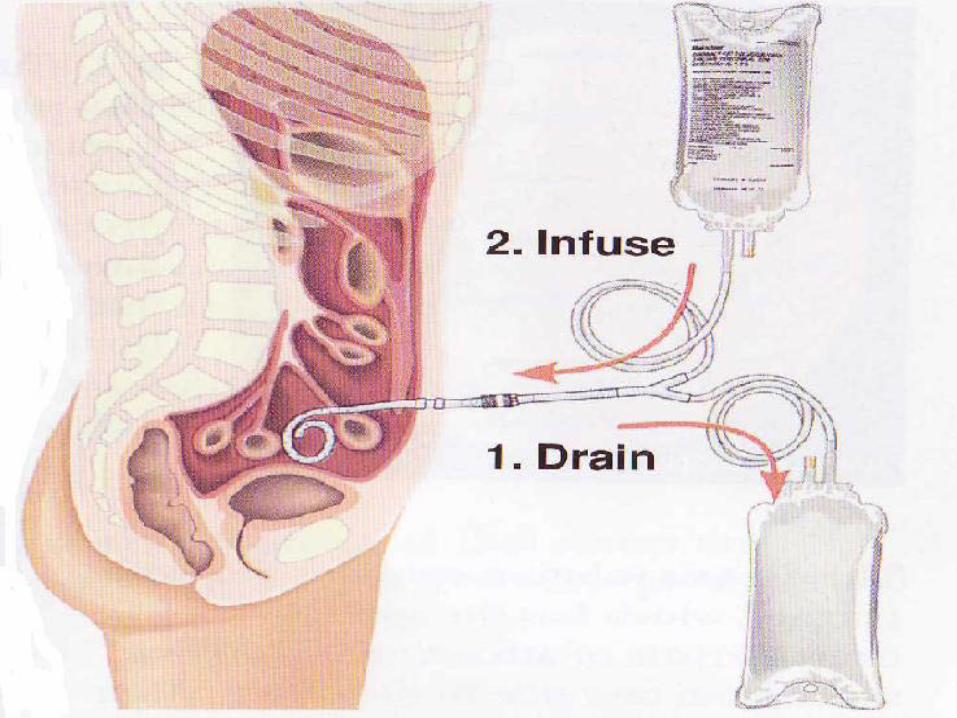
PERITONEAL DIALYSIS Continuous Ambulatory Peritoneal dialysis (C.A.P.D)
Automated Peritoneal Dialysis (A.P.D) where machine does it overnight so you have days free
DIANEAL Dianeal uses Glucose to produce an osmotic
gradient which moves extracellular fluid into the peritoneal cavity, to remove excess fluid no longer excreted by Kidneys.
The higher the strength of glucose, the greater the fluid loss 0.55%; 1.5%; 2.5%; 4.25%
The least Glucose load = 3 bags 1.5% dextrose And 1.5% glucose is 83mmol of Glucose = Increased insulin requirement (may be overnight)
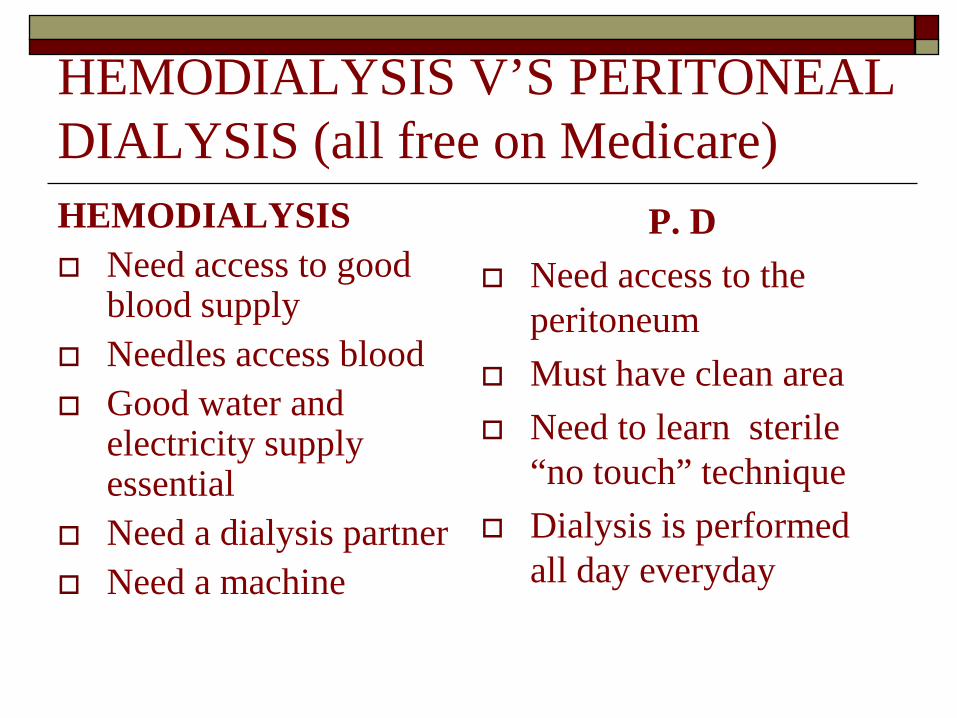
HEMODIALYSIS V’S PERITONEAL DIALYSIS (all free on Medicare) HEMODIALYSIS Need access to good
blood supply Needles access blood Good water and
electricity supply essential
Need a dialysis partner Need a machine
P. D Need access to the
peritoneum Must have clean area Need to learn sterile
“no touch” technique Dialysis is performed
all day everyday
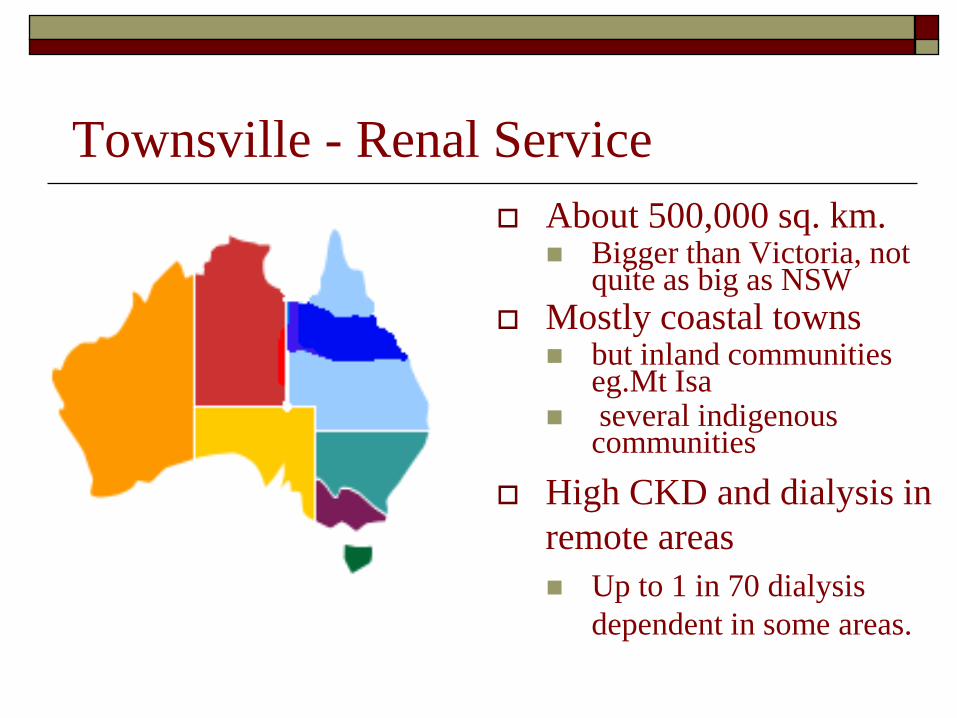
Townsville - Renal Service About 500,000 sq. km.
Bigger than Victoria, not quite as big as NSW
Mostly coastal towns but inland communities
eg.Mt Isa several indigenous
communities High CKD and dialysis in
remote areas Up to 1 in 70 dialysis
dependent in some areas.
Townsville reality Townsville has approx 230 Dialysis Clients
attached to its service > 50% have Diabetic Kidney Disease 78 are on home dialysis, so back in their own
homes and communities (spending between 2 weeks to 2 years stuck in Townsville)
Current QH policy aims for minimum 40% clients on Home dialysis with a 50% target.
Those Not at Home We have 3 rural or remote Satellite dialysis
units but all clients start in Townsville and all return here if problems
16 in Mt Isa Unit 3 in Joyce Palmer Palm Island Unit 12 in Home Hill Unit The other 125 dialyse at TTH or North Ward.
The 125 in Townsville 53% are ATSI 34% come from rural and remote areas
That number has been about 1/3 for several years Mt Isa and surrounds, 31 clients so ¾ of those
inc Mornington Island, Doomadgee, Burketown….. Flinders Highway -Charters Towers to Richmond Palm Island, Magnetic Island Bruce Highway Cardwell to Burdekin or Bowen.
Added impact of CKD Having CKD does not mean other things go
away. Still worry about feet, eyes, heart ….. Pill burden is higher than non CKD as
addition of medications for CKD if it worsens; may change after every blood test.
Changing insulin or oral agents required
Psychosocial Impact Coping with chronic illness –anxiety,
depression Haemodialysis is at least 5 hours every
second day. Isolated in TSV when you need most support Usually unable to attend important events;
births, birthdays, weddings, sorry business. Distance home, expensive and few flights
Take home message CKD prevention or slowing progression is possible
from preventable causes. BGL and BP control Referral to CKD team and Nephrologists earlier Combined Pancreas- Kidney transplant if suitable. If dialysis inevitable - home dialysis best outcomes
(long slow nocturnal Hd = same as transplant) PD first maintains residual renal function longer,
then home nocturnal Haemodialysis
New Edition! now
available at www.kcat.org.au
Further Resources…
CKD Management in General Practice
2012 Guidelines booklet


















