Welcome to CobraServ - Rogers Benefit Group COBRAServ welcome.pdfManaged business solutionsfor human...
20
Welcome to CobraServ Managed business solutions for human resources and employee effectiveness
Transcript of Welcome to CobraServ - Rogers Benefit Group COBRAServ welcome.pdfManaged business solutionsfor human...

Welcome to CobraServ
Managed business solutions for human resources and employee effectiveness

Managed business solutions for human resources and employee effectiveness
WELCOME TO CobraServ
Dear CobraServ Customer:
Welcome to CobraServ - the nation’s largest COBRA compliance service. We look forward to providing you with thebest COBRA compliance administration available, to minimize your involvement in COBRA.
Members of our implementation team will be contacting you. They will review the materials in this section("Welcome to CobraServ") and the section entitled "CobraServ Forms" and discuss how CobraServ can best meet yourneeds. Our team will show you just how well they know COBRA – and will share their knowledge with you.
CobraServ does it all, from assuming administration of your COBRA continuants, to performing future billing andadjudication of eligibility, to collecting and processing all related transactions.
With CobraServ, your role is reduced to responding to 3 situations:
1 When individuals first become covered under your plan;
2 When an individual experiences a COBRA Qualifying Event;
3 If you receive a report of COBRA activity that requires response.
In this document, you will find information concerning:
• What CobraServ Does
• What the Employer Does
• Reports and Updating Your Carrier
• COBRA Compliance Requirements

WHAT CobraServ DOESE l e c t i o n s , B i l l i n g , R e p o r t i n g , A d d i t i o n a l S e r v i c e s
Elect ions• CobraServ Customer Service Representatives (CSRs) respond to all inquiries from Qualified Beneficiaries.
• CobraServ provides a toll-free hotline to continuants 24 hours-a-day, 365 days a year for premium inquiriesthrough our Interactive Voice Response (IVR) system.
• Qualified Beneficiaries can elect COBRA by phone via the IVR system; on our Website using Elect By Net; oron paper with a COBRA Election Form.
• CobraServ determines whether the elections CobraServ receives were made within the allowable 60-day period.
• CobraServ offers special status reports to employers.
• We provide an employer a toll-free hotline to call for assistance.
Bil l ing• CobraServ administers the initial 45-day and ongoing 30-day grace periods.
• Each month, CobraServ sends each continuant a detailed bill with a payment envelope and a request forongoing certification of continuant eligibility.
• CobraServ sends grace letters to those who don’t pay within eight days of the grace expiration date.
• CobraServ determines any late payments. We accept full and partial premium payments, within “Safe Harbor”.
• Checks are returned that are non-negotiable (no signature, wrong payee, etc.) if they are received byCobraServ more than 10 days before the grace period expiration date.
• Checks received less than 10 days before the grace period expiration date are also returned, and the COBRAcontinuant is given up to 10-days to correct their non-negotiable check.
• CobraServ follows up on dishonored checks.
• CobraServ archives critical documents and materials for seven years in a professional archiving facility, toresolve potential disputes.
• CobraServ sends cancellation notices to those who do not pay their premiums within the grace period.
• If you have active continuants, you will receive amonthly consolidated premium check represent-ing premiums collected from COBRA continu-ants, less the 2% administrative fee paid bythe continuant. Accompanying reportswill indicate actions to be taken, if any.
Managed business solutions for human resources and employee effectiveness

WHAT CobraServ DOES (continued)E l e c t i o n s , B i l l i n g , R e p o r t i n g , A d d i t i o n a l S e r v i c e s
Addit ional ServicesCobraServ also provides the following additional services:
• employs two different ERISA law firms to help keep your plan in compliance and to stay up-to-date oncourt cases affecting COBRA. CobraServ forms are updated as the regulations change;
• utilizes a Research Department to stay current on compliance changes and trends through subscriptions to industry publications, legislative bulletins and legal update services;
• sends conversion notices, where appropriate, in the last 90 days before COBRA reaches maximum term;
• accepts calls from providers, hospital representatives, agents, brokers or HMOs regarding coverages/eligibility;
• provides employer with mail labels for all COBRA continuants to assist in Open Enrollment communica-tions;
• handles multiple Qualifying Events (for example, termination of employment followed by divorce);
• provides ongoing customer service to all administrators and continuants.

Managed business solutions for human resources and employee effectiveness
OVERVIEW OF EMPLOYER RESPONSIBILITIES
Init ia l Notice of COBRA RightsWhenever a new employee or a spouse or a dependent child first becomes covered under the group health plan,he and/or she must be provided an Initial Notification of COBRA Rights. A sample Initial Notice of COBRA Rightsis included in your COBRA Compliance Implementation Kit.
New Qual ifying EventsAny of the following events that would cause an employee, spouse or dependent to lose coverage under thegroup health plan is considered a COBRA Qualifying Event:
• Termination of the employee’s employment for any reason other than gross misconduct (layoff, resignation,retirement, etc.)
• Employee’s reduction of hours
• Death of the covered employee
• Divorce or legal separation from the covered employee
• Dependent child of the covered employee ceasing to meet eligibility requirements under the Group Health Plan
• Covered employee/retiree becomes entitled to Medicare
• Retiree or retiree’s spouse or child loses coverage within one (1) year before or after the commencement ofproceedings of the sponsoring employer under Title II (bankruptcy), United States Code.
An individual who loses coverage under the group health plan because of a Qualifying Event is a QualifiedBeneficiary.
1. When a Qualifying Event causes an employee or a dependent to lose coverage under the group health plan,you must mail a COBRA Notification Form to the Qualified Beneficiary within fourteen (14) days of theQualifying Event; even if the Qualified Beneficiary tells you he or she does not want continuation coverage.The Department of Labor has indicated the best method of delivery to the Qualified Beneficiary is by proper-ly addressed First-Class Mail.
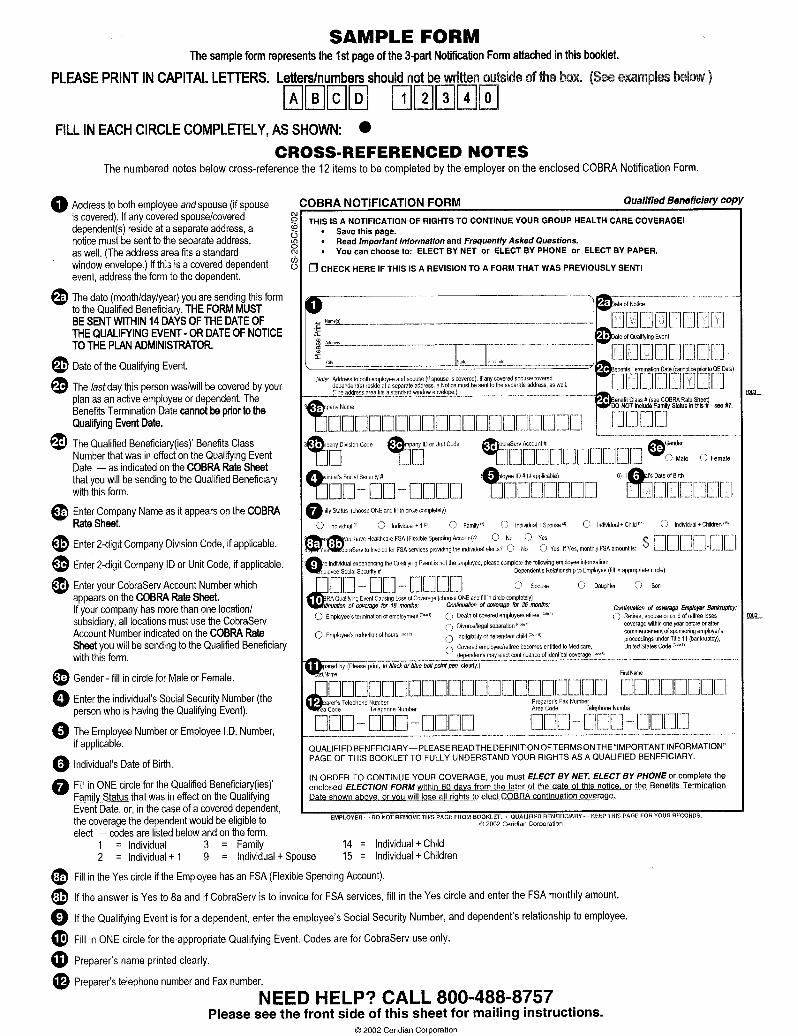
2. Remove the top page of the COBRA Notification and Election Booklet. Complete the COBRA NotificationForm as indicated on the first page of the booklet, "Employer Instructions" and on the "Sample Form" page ofthe booklet.
3. Remove the blue-bordered and pink-bordered copies of the COBRA Notification Form from the booklet.Within fourteen (14) days of the Qualifying Event, mail all remaining pages via First- Class Mail, togetherwith a copy of the COBRA Rate Sheet, to the Qualified Beneficiary and spouse by name, and eligible depend-ents, if covered under the group health plan to their last- known home address (i.e., John Smith and MarySmith and Eligible Dependents).
4. Mail the blue bordered COBRA Notification Form to CobraServ within 14 days of the Qualifying Event.Please, DO NOT FAX the form to us.
5. Retain the pink-bordered "Employer Copy" of the form for your records.
6. Terminate this person from your group insurance plan, effective as of the "Benefits Termination Date."
If you have any questions regarding the Initial Notice or if you need assistance in completing the COBRANotification Form, please call CobraServ Client Services at 800/488-8757. We also have a separate toll-free dedi-cated COBRA continuant line, 800/877-7994.

WHAT TO DO WITH REPORTSParticipant Update, Monthly Participant Status,Premium Distribution Reports
Reports / Carr ier UpdatingCobraServ will send you reports of:
• COBRA continuants electing COBRA and paying the first premium;
• dependents being added or dropped;
• continuants being cancelled.
Your role is to review these reports, and report the addition, termination or dependent change to the appropriate carrier(s).
Descript ion of the Reports
• Participant Update Reports are generated by CobraServ and sent to the employer providing detail of contin-uants who make the initial COBRA premium payment, cancellations, or change of their dependents’ status.These reports are sent on a daily or weekly basis and provide you with the information needed to updateyour carrier.
• Once a month, the employer receives the Monthly Participant Status Report from CobraServ and aPremium Distribution Report summarizing all activity for the previous month and a consolidated check forthe premiums collected, less the 2% administrative fee paid by the continuant.
The next three pages will provide you some sample reports.
Managed business solutions for human resources and employee effectiveness
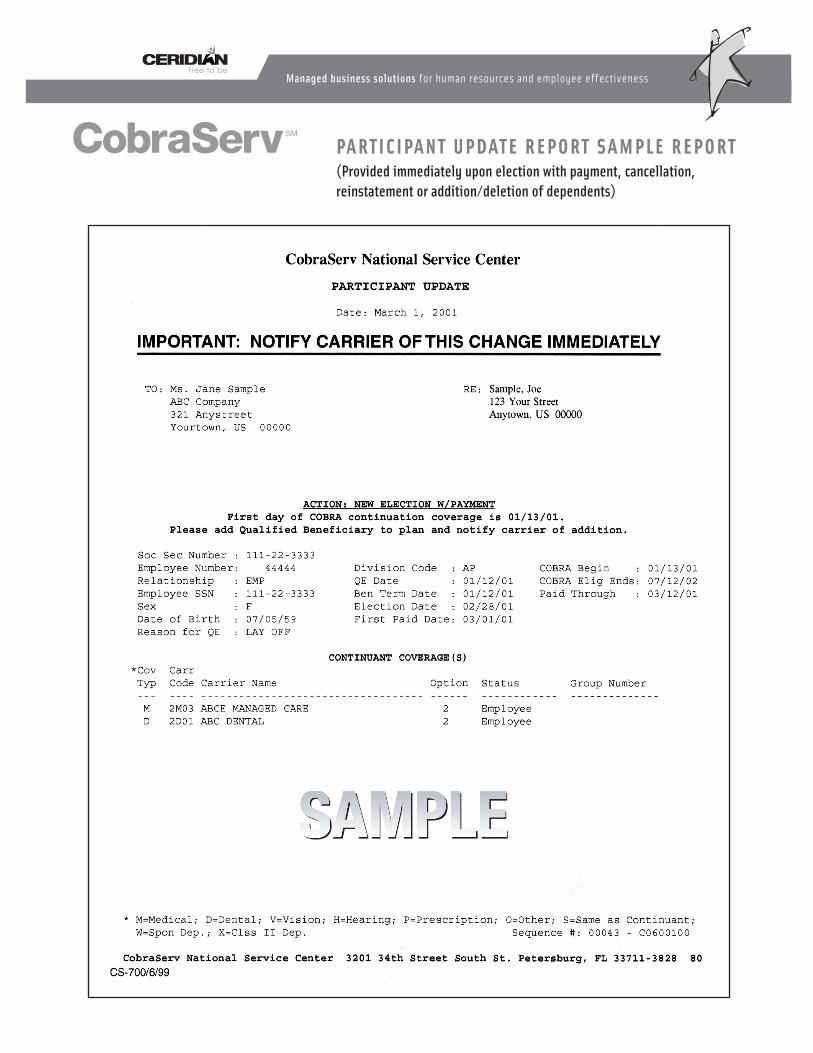
PARTICIPANT UPDATE REPORT SAMPLE REPORT(Provided immediately upon election with payment, cancellation, reinstatement or addition/deletion of dependents)
Managed business solutions for human resources and employee effectiveness

Managed business solutions for human resources and employee effectiveness
PARTICIPANT STATUS SAMPLE REPORT(Provided monthly)

Managed business solutions for human resources and employee effectiveness
PREMIUM DISTRIBUTION SAMPLE REPORT(Provided monthly)
SAMPLE MONTHLY PREMIUM REIMBURSEMENT
Managed business solutions for human resources and employee effectiveness
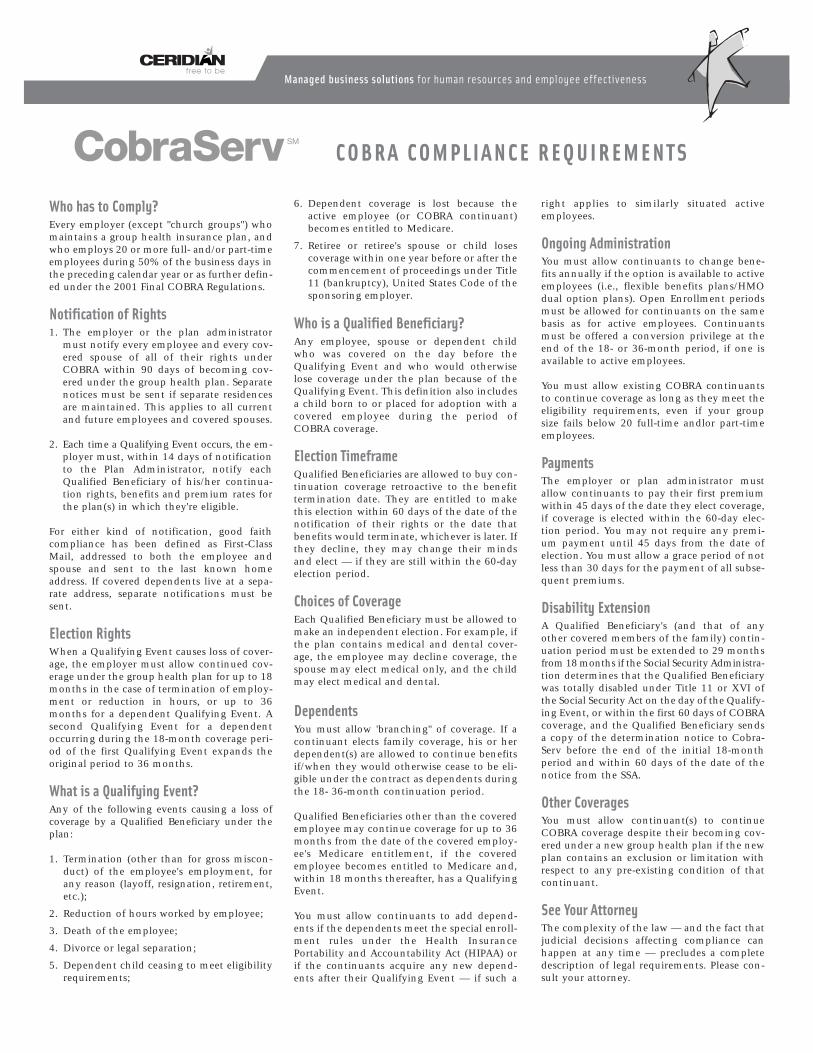
COBRA COMPLIANCE REQUIREMENTS
Who has to Comply?Every employer (except "church groups") whomaintains a group health insurance plan, andwho employs 20 or more full- and/or part-timeemployees during 50% of the business days inthe preceding calendar year or as further defin-ed under the 2001 Final COBRA Regulations.
Notification of Rights1. The employer or the plan administrator
must notify every employee and every cov-ered spouse of all of their rights underCOBRA within 90 days of becoming cov-ered under the group health plan. Separatenotices must be sent if separate residencesare maintained. This applies to all currentand future employees and covered spouses.
2. Each time a Qualifying Event occurs, the em-ployer must, within 14 days of notificationto the Plan Administrator, notify eachQualified Beneficiary of his/her continua-tion rights, benefits and premium rates forthe plan(s) in which they're eligible.
For either kind of notification, good faithcompliance has been defined as First-ClassMail, addressed to both the employee andspouse and sent to the last known homeaddress. If covered dependents live at a sepa-rate address, separate notifications must besent.
Election RightsWhen a Qualifying Event causes loss of cover-age, the employer must allow continued cov-erage under the group health plan for up to 18months in the case of termination of employ-ment or reduction in hours, or up to 36months for a dependent Qualifying Event. Asecond Qualifying Event for a dependentoccurring during the 18-month coverage peri-od of the first Qualifying Event expands theoriginal period to 36 months.
What is a Qualifying Event?Any of the following events causing a loss ofcoverage by a Qualified Beneficiary under theplan:
1. Termination (other than for gross miscon-duct) of the employee's employment, forany reason (layoff, resignation, retirement,etc.);
2. Reduction of hours worked by employee;
3. Death of the employee;
4. Divorce or legal separation;
5. Dependent child ceasing to meet eligibilityrequirements;
6. Dependent coverage is lost because theactive employee (or COBRA continuant)becomes entitled to Medicare.
7. Retiree or retiree's spouse or child losescoverage within one year before or after thecommencement of proceedings under Title11 (bankruptcy), United States Code of thesponsoring employer.
Who is a Qualified Beneficiary?Any employee, spouse or dependent childwho was covered on the day before theQualifying Event and who would otherwiselose coverage under the plan because of theQualifying Event. This definition also includesa child born to or placed for adoption with acovered employee during the period ofCOBRA coverage.
Election TimeframeQualified Beneficiaries are allowed to buy con-tinuation coverage retroactive to the benefittermination date. They are entitled to makethis election within 60 days of the date of thenotification of their rights or the date thatbenefits would terminate, whichever is later. Ifthey decline, they may change their mindsand elect — if they are still within the 60-dayelection period.
Choices of CoverageEach Qualified Beneficiary must be allowed tomake an independent election. For example, ifthe plan contains medical and dental cover-age, the employee may decline coverage, thespouse may elect medical only, and the childmay elect medical and dental.
DependentsYou must allow 'branching" of coverage. If acontinuant elects family coverage, his or herdependent(s) are allowed to continue benefitsif/when they would otherwise cease to be eli-gible under the contract as dependents duringthe 18- 36-month continuation period.
Qualified Beneficiaries other than the coveredemployee may continue coverage for up to 36months from the date of the covered employ-ee's Medicare entitlement, if the coveredemployee becomes entitled to Medicare and,within 18 months thereafter, has a QualifyingEvent.
You must allow continuants to add depend-ents if the dependents meet the special enroll-ment rules under the Health InsurancePortability and Accountability Act (HIPAA) orif the continuants acquire any new depend-ents after their Qualifying Event — if such a
right applies to similarly situated activeemployees.
Ongoing AdministrationYou must allow continuants to change bene-fits annually if the option is available to activeemployees (i.e., flexible benefits plans/HMOdual option plans). Open Enrollment periodsmust be allowed for continuants on the samebasis as for active employees. Continuantsmust be offered a conversion privilege at theend of the 18- or 36-month period, if one isavailable to active employees.
You must allow existing COBRA continuantsto continue coverage as long as they meet theeligibility requirements, even if your groupsize fails below 20 full-time andlor part-timeemployees.
PaymentsThe employer or plan administrator mustallow continuants to pay their first premiumwithin 45 days of the date they elect coverage,if coverage is elected within the 60-day elec-tion period. You may not require any premi-um payment until 45 days from the date ofelection. You must allow a grace period of notless than 30 days for the payment of all subse-quent premiums.
Disability ExtensionA Qualified Beneficiary's (and that of anyother covered members of the family) contin-uation period must be extended to 29 monthsfrom 18 months if the Social Security Administra-tion determines that the Qualified Beneficiarywas totally disabled under Title 11 or XVI ofthe Social Security Act on the day of the Qualify-ing Event, or within the first 60 days of COBRAcoverage, and the Qualified Beneficiary sendsa copy of the determination notice to Cobra-Serv before the end of the initial 18-monthperiod and within 60 days of the date of thenotice from the SSA.
Other CoveragesYou must allow continuant(s) to continueCOBRA coverage despite their becoming cov-ered under a new group health plan if the newplan contains an exclusion or limitation withrespect to any pre-existing condition of thatcontinuant.
See Your AttorneyThe complexity of the law — and the fact thatjudicial decisions affecting compliance canhappen at any time — precludes a completedescription of legal requirements. Please con-sult your attorney.

Learn more online at www.ceridian.com/myceridian
Best in class solutions. Extraordinary expertise. Provenservice for thousands of companies around the world.Ceridian frees your company to maximize your human,financial and technological resources and get themfocused on what’s really important – your business.
Ceridian 3201 34th Street South St. Petersburg, FL 33711 www.ceridian.com/myceridian
©2003 Ceridian Corporation. All rights reserved.Printed in USA MP-030625 CAP
M A N A G E D B U S I N E S S S O L U T I O N S

ORIGINAL—EMPLOYEE COPY—EMPLOYERCS-306/2/02SAL © 2002 Ceridian Corporation
RETAIN THIS NOTICE WITHYOUR INSURANCE PAPERS
*VERY IMPORTANT NOTICE*
INITIAL NOTICE OF COBRA RIGHTS
A federal law known as COBRA (Consolidated Omnibus BudgetReconciliation Act of 1985 as amended) requires most employers sponsor-ing group health plans to notify all of their employees, including newly-hired, current and previous employees (and their dependents) of theirrights to “continuation” health care coverage in the event they would losecoverage due to certain events called “Qualifying Events.” This notice is theemployer’s fulfillment of this obligation. If you, your spouse or dependentchild(ren) are or become participants in the above employer’s group healthplan(s), it is important to understand your ongoing rights and obligationsunder the continuation of coverage provisions of COBRA. This summary ofrights should be reviewed by both you and your spouse (if applicable),retained with other benefits documents, and referred to in the event that anyaction is required on your part.
If you, your spouse or dependent child(ren) should lose coverageunder the above employer’s group health plan(s) due to a “QualifyingEvent” (listed below), you may be entitled to elect temporary continuationof health care coverage (“continuation coverage”) at group rates. It isimportant that your sponsoring employer have your current address.Notification of a Qualifying Event should one occur, will be sent to your lastknown address at the time of the event. The following summary ofinformation concerning COBRA outlines the procedures which should befollowed if or when a Qualifying Event occurs.
If you are an employee of the employer designated in the “EM-PLOYER” box above and are covered by its group health plan, you havea right to elect continuation coverage if you lose your group health coveragebecause of a reduction in your hours of employment or the termination ofyour employment (for reasons other than gross misconduct).
If you are the covered spouse of the above covered employee, youhave the right to elect continuation coverage for yourself if you lose grouphealth coverage for any of the following reasons:
(1) The death of your spouse;(2) The termination of your spouse’s employment (for reasons
other than gross misconduct) or reduction in your spouse’shours of employment;
(3) Divorce or legal separation from your spouse; or(4) Your spouse becomes entitled to Medicare.If you are a covered dependent child of the above employee, you
have the right to elect continuation coverage if you lose group healthcoverage for any of the following reasons:
(1) The death of the employee;(2) The termination of the employee’s employment (for reasons
other than gross misconduct) or a reduction in theemployee’s hours of employment;
(3) Parents' divorce or legal separation;(4) Employee becomes entitled to Medicare; or(5) The dependent ceases to be a “dependent child” under the
terms of the plan(s).You also have a right to elect continuation coverage if you are
covered under the plan as a retiree or spouse or child of a retiree, and losecoverage within one year before or after the commencement of proceed-ings under Title 11 (bankruptcy), United States Code.
Under the law, the employee (or a covered dependent) has theresponsibility to inform the above named employer of a divorce, legalseparation, or a child losing dependent status under the plan if any ofthese events would cause a loss of coverage. This notification mustbe made within 60 days after the date of the Qualifying Event, or thedate on which coverage would end under the plan because of theevent, whichever is later. The notice must be in writing, and should besent to the contact person or department of the employer indicated onthis form. If notice is not timely made, rights to continue coverage willterminate. In situations where a covered employee discontinuescoverage of a spouse in anticipation of a divorce or legal separation,your sponsoring employer, who received timely notification, is re-quired to make COBRA continuation coverage available effectivefrom the date of the divorce or legal separation (but not prior to thatdate). If you need help acting on behalf of an incompetent beneficiary,please contact the employer indicated for assistance.
When the employer is notified that a Qualifying Event has happened,it will in turn notify you that you have the right to elect continuationcoverage. Under the law, you have 60 days from the date you would losecoverage because of one of the events described above, or 60 days fromthe date of the employer’s notice of your right to elect continuationcoverage (whichever is later) to elect continuation coverage. If you makea timely election, coverage will become effective on the day after coveragewould otherwise be terminated. Note: Some states offer financial aid tohelp certain individuals pay for COBRA coverage. Contact yourappropriate state agency regarding availability and eligibility re-quirements. Additionally, under certain circumstances, COBRA cover-age may be paid with pre-tax dollars from a cafeteria plan underSection 125.
If you do not timely elect continuation coverage, your group healthinsurance coverage will terminate in accordance with the provisionsoutlined in your employer’s plan.
If you elect continuation coverage, your coverage will be identical tothe coverage provided under the plan to similarly situated employees andtheir family members. The law requires that you be afforded the opportu-nity to maintain continuation coverage for 36 months from the date of theQualifying Event, unless coverage was lost because of a termination ofemployment or a reduction in hours. In that case, the required continuationcoverage period is 18 months measured from the Qualifying Event date.The 18-month period may be extended to 29 months for disabled QualifiedBeneficiaries under certain circumstances, as described on the reverseside of this notice.
However, the law also provides that continuation coverage may endprior to the expiration of the 18-, 29- or 36-month period described aboveif any one of the following occurs:
• The Qualified Beneficiary fails to pay the required premium in atimely manner;
• The Qualified Beneficiary first becomes, after the date of election,
Continued on next page
Contact Person/Department:NAME PHONE
EMPLOYER (employer completes both address sections)
FROM:
NAME
ADDRESS
CITY/ST/ZIP
DATE:TO:

CS-306/2/02SAL © 2002 Ceridian CorporationORIGINAL—EMPLOYEE COPY—EMPLOYER
entitled to Medicare;• The employer/former employer no longer provides group health
coverage to any of its employees;• The Qualified Beneficiary first becomes, after the date of election,
covered under another group health plan (as an employee orotherwise) which does not contain any exclusion or limitation withrespect to any preexisting condition of the Qualified Beneficiary.
You do not have to show that you are insurable to choose continuationcoverage. However, continuation coverage under COBRA is providedsubject to your eligibility for coverage under the plan. The employerreserves the right to terminate your continuation coverage retroactively ifyou are determined to be ineligible.
Under the law, you may have to pay all or part of the premium for yourcontinuation coverage. Your employer may charge you up to 102% of theapplicable premium for your continuation coverage. The law also says that,at the end of the 18-month, 29-month or 36-month continuation coverageperiod, you must be allowed to enroll in an individual conversion healthplan if one is provided under the terms of the employer’s group healthplan. In addition, under the Health Insurance Portability & AccountabilityAct (HIPAA, 1996), in certain circumstances, such as when you exhaustCOBRA coverage, you may have the right to buy individual health coveragewith no pre-existing condition exclusion without having to give evidence ofgood health.
Once your continuation coverage terminates for any reason, it cannotbe reinstated.
Please notify the contact person or department indicated in theEMPLOYER box on the front side of this notice if:
• you have any questions about this material;• you have a change in marital status, or you, your spouse, or
eligible covered dependent has a change of address.Also, if your spouse or any covered child resides at a different address,please notify the employer in writing, so that a separate notice may be sent.
COBRA Questions and Answers
A) Who is a Qualified Beneficiary?A Qualified Beneficiary is any employee, former employee, or spouse ordependent child of an employee or former employee, who was coveredunder the employer’s group health plan on the day before the QualifyingEvent. The definition also includes a child born to or placed for adoption witha covered employee during the period of COBRA coverage.
B) What is a Qualifying Event?A Qualifying Event is any of the following events which would cause anemployee, former employee, covered spouse or covered dependent childto lose coverage under the employer’s group health plan. These eventsinclude:
a) with respect to a Qualified Beneficiary, an employee’s terminationof employment (includes voluntary resignation and involuntarytermination, except when termination is due to gross misconduct),retirement, or layoff;
b) with respect to a Qualified Beneficiary, an employee’s reduction ofwork hours (includes work stoppage, strike, or employee beginsleave of absence);
c) with respect to a Qualified Beneficiary other than the employee,death of a covered employee;
d) with respect to a Qualified Beneficiary other than the employee,divorce or legal separation from a covered employee;
e) with respect to a Qualified Beneficiary other than the employee, a
INITIAL NOTICE OF COBRA RIGHTS (continued)
dependent child’s loss of eligibility due to the plan’s eligibilitydefinitions;
f) with respect to a Qualified Beneficiary other than the employee,an employee becoming entitled to Medicare.
g) with respect to a retiree or spouse or child of a retiree, loss ofcoverage within one year before or after the sponsoringemployer’s commencement of proceedings under Title 11(bankruptcy), United States Code.
C) How long may coverage be continued?If the Qualifying Event is either “(a)” or “(b)” in question B above, coveragemay be continued for up to 18 months,* which is measured from the dateof the Qualifying Event. For Qualified Beneficiaries other than the coveredemployee, coverage may be continued for: (i) up to 36 months from anyother Qualifying Event, which is measured from the date of the originalQualifying Event, or, (ii) up to 36 months measured from the date of thecovered employee's Medicare entitlement, if the covered employee be-comes entitled to Medicare and, within 18 months thereafter, has aQualifying Event (either "(a)" or "(b)" in question B above). However,continuation coverage may end prior to the expiration of the 18-, 29- or36-month period, as described on the reverse side of this notice.
*Note: A Qualified Beneficiary who is determined under Title II orXVI of the Social Security Act, to have been disabled at the time ofa Qualifying Event or within the first 60 days of COBRA coveragedescribed in “(a)” or “(b)” in question B above may be eligible tocontinue coverage for an additional 11 months (29 months total).In order to obtain this extension of coverage, the Qualified Benefi-ciary must provide the employer with the written determination ofdisability from the Social Security Administration within 60 days ofthe date of the determination of disability by the Social SecurityAdministration and prior to the end of the 18-month continuationperiod. The employer can charge up to 150% of the applicablepremium during the 11-month disability extension. If coverage isextended to 29 months, coverage will cease upon a final determi-nation that the Qualified Beneficiary is no longer disabled. Thedisabled individual must notify the Employer within 30 days of anyfinal determination that he or she is no longer disabled.
D) What coverage(s) may be continued?Qualified Beneficiaries may continue only those group health coveragesthat were in effect on the day before the Qualifying Event.
E) Can Qualified Beneficiaries make separate coverage elections?Yes, Qualified Beneficiaries may make separate elections. Each QualifiedBeneficiary may choose any benefit coverage for which he or she iseligible. If Qualified Beneficiaries wish to make independent elections,they must complete separate election forms. Parents or guardians mayelect coverage on behalf of minor dependent children.
F) How much will it cost me to continue coverage under COBRA?The cost to continue coverage is the applicable group premium rate forcoverage elected, plus an administration fee, if applicable. Premium rates(including administration fees where applicable) should be provided to youat the time of a Qualifying Event. These rates are subject to change.
G) When does COBRA coverage begin?COBRA continuation coverage begins on the day after the date thatcoverage would otherwise terminate under the plan, only if the electionform is sent within the allotted time period and all other eligibility require-ments are satisfied.

1a) FROM: (COMPANY)
1b) Plan Code (Division Code) Company Code (Unit Code)
(If applicable, refer to the Client Rate Report for the one character or two characters required [alpha and/or numeric] to complete above.)
2) CobraServ Account # (indicated on the Client Rate report for location or subsidiary)
3) Please be advised that the following is currently on COBRA continuation.
(Check one box only.) ❑ (E)mployee ❑ (D)ependent
4) Social Security Number of Qualified Beneficiary
5a) Name of COBRA continuant (last, first, mi)
5b) Street (include apartment number)
5c) City
5d) State 5e) Zip Code
6) Home Phone # (if available)
7) Employee Number (if applicable)
8) Date of Birth 9) Gender (check one)
10) Marital Status (Check one box only.)
11) If the above individual in box #5 is a dependent of an employee/formeremployee, please complete the following:Employee Name (last, first, mi) _______________________________________
Employee SSN
Dependent’s Relationship to Employee ___________________________
12) Qualifying Event Date
13) Last day of pre-COBRA Coverage (cannot be prior to Qualifying Event Date)
14) First premium due-date for which CobraServ is to begin billing.
15) COBRA Qualifying Event that caused loss of coverage (check one)Continuation of coverage for 18 months:❑ Employee’s termination of employment (Code 1)
(includes voluntary resignation, involuntary termination (except when due to grossmisconduct), retirement, layoff, or leave of absence)
❑ Employee’s reduction in work hours (includes work stoppage or strike) (Code 2)
Continuation of coverage for 36 months:❑ Death of covered employee /retiree (Code 3) ❑ Ineligibility of dependent child (Code 6)
❑ Divorce/legal separation (Code 4) ❑ Retiree, spouse or child of retiree loses❑ Covered employee/retiree becomes coverage within one year before or after
entitled to Medicare; dependents commencement of proceedingsmay elect continuance of identical under Title 11 (bankruptcy) Unitedcoverage (Code 5) States Code (Code 7)
16) If employee, does he/she have a health care Flexible Spending Account (FSA)?
❑ (N)o ❑ (Y)es If Yes, MONTHLY contribution $___________________
17) Benefits Class (Refer to Client Rate Report for Code)
18) Check the current plan code coverages. CobraServ administers only plancode coverage options that are permitted by your plan or carrier.(Check one box only.)❑ 1 = Individual ❑ 9 = Individual + Spouse❑ 2 = Individual + 1 ❑ 14 = Individual + Child❑ 3 = Family ❑ 15 = Individual + Children
19) Has the continuant been approved for an additional 11-month disabilityextension? ❑ (N)o ❑ (Y)es
20) If the COBRA continuant has dependents covered, please complete thefollowing. If names are not available, please indicate “N/A.”
Dependent Name (first, last, mi)
Date of Birth (month/day/year)
Gender(check one) ❑ (M)ale ❑ (F)emale
Social Security Number — —
Relationship to employee Qualified Beneficiary ❑
Dependent Name (first, last, mi)
Date of Birth (month/day/year)
Gender check one) ❑ (M)ale ❑ (F)emale
Social Security Number — —
Relationship to employee Qualified Beneficiary ❑
Dependent Name (first, last, mi)
Date of Birth (month/day/year)
Gender (check one) ❑ (M)ale ❑ (F)emale
Social Security Number — —
Relationship to employee Qualified Beneficiary ❑
Prepared By:Name: (Print) ________________________________________________
Date:
Phone #:
Fax #:
❑ (M)ale ❑ (F)emale
❑ (S)ingle ❑ (M)arried ❑ (W)idowed ❑ (D)ivorced
COBRA Continuant Takeover Form(For transferring current COBRA continuants to CobraServ)
CS
-614
/6/0
0CA
P ❑ ORIGINAL NOTICE If FAXED, do not mail copy.
❑ REVISION . . . to a form that was previously sent.
PLEASE CHECKONE BOX ➥
□ □ □ □
□□□□□□□□M M D D Y Y Y Y
□□□□□□□□□□□□— —
□□□□□□□□□□□— —
□□□□□□□□M M D D Y Y Y Y
□□□□□□□□M M D D Y Y Y Y
□□□□□□□□□□□— —
□□□□□□□□M M D D Y Y Y Y
□□□□□□□□□□□□— —
□□□□□□□□M M D D Y Y Y Y
□□□□□□□□□□□□— —
CobraServ National Service Center • 3201 34th Street South • St. Petersburg, Florida 33711-3828 • 800/488-8757 • Fax: 727/865-3648© 2000 Ceridian Corporation
INSTRUCTIONS: Please type or print, IN BLACK OR BLUE INK, clearly.• Fill out just one form per family unit (Qualified Beneficiary and dependents).• Use this form to report existing COBRA continuants who will be transferred
to CobraServ.• Please do not use this form to report new Qualifying Events. Use the Qualifying
Event Notification Form.COMPLETE THIS FORM AND RETURN IT TO:
CobraServ National Service Center, P.O. Box 534066, St. Petersburg, FL 33747-4066Telephone: 800/488-8757 • Fax: 727/865-3648

TRANSFERRING CURRENT COBRA CONTINUANTS TO COBRASERVINSTRUCTIONS FOR COMPLETING
COBRASERV CONTINUANT TAKEOVER FORM (ON REVERSE SIDE)(USE ONE FORM PER FAMILY UNIT)
This form is only needed if you have current COBRA Continuants to be transferred toCobraServ. One form should be completed for each family unit and sent to:
CobraServ National Service Center, P.O. Box 534066, St. Petersburg, FL 33747-4066
Number 1: Enter your company name. If we haveset up your account to report bydivision or unit, enter division or regioncode and company ID or unit code.
Number 2: Enter your company’s CobraServAccount Number.
Number 3: Check appropriate box to indicatewhether Continuant is an employee ordependent. (Check one box only.)
Number 4: Enter the Continuant’s complete nine-digit Social Security Number.
Number 5: Enter Continuant’s complete name(last, first, middle initial) and completemailing address (street, city, state andZip Code).
Number 6: Enter Continuant’s home phonenumber, including area code, ifavailable.
Number 7: If the Continuant is an employee who hasan employee ID number, enter it here.
Number 8: Continuant’s date of birth.(month, day, year).
Number 9: Check appropriate box to indicate theContinuant’s Gender (Male or Female).
Number 10: Check appropriate box to indicatemarital status of Continuant.
Number 11: If the Continuant is a dependent of anemployee or former employee, enteremployee’s complete name (last,first, middle initial), employee’s nine-digit Social Security Number, andContinuant’s relationship to employee.
Number 12: Enter the month, day and year of theQualifying Event.
Number 13: Enter the LAST DAY (month, day, year) ofthe Continuant’s pre-COBRA coverage.
Number 14: Enter the FIRST PREMIUM DUE DATE forwhich CobraServ is to begin billing.
Number 15: Check appropriate box (check onebox only) to indicate the type ofQualifying Event. “Employee’s terminationof employment” includes voluntaryresignation, involuntary termination(except for termination due to grossmisconduct), retirement, layoff, or leave ofabsence.“ Employee’s reduction inhours” includes work stoppage (strike).
Number 16: If the employee has a health careFlexible Spending Account (FSA), check“Yes” and indicate his or her monthlycontribution.
Number 17: Refer to your COBRA Rate Sheet andenter the CobraServ Benefits Classindicating the coverage in effect forthis individual.
Number 18: Indicate coverage by checking the boxof the appropriate plan code. Yourcarrier may not use some of the choicesindicated: check the choice thatcorresponds to the status assigned thisindividual by your carrier.
Number 19: Check appropriate box (Yes or No) toindicate whether the Continuant hasbeen approved for an 11-monthdisability extension.
Number 20: Provide information if the Continuanthas dependents covered, and indicatewhether the individual is a QualifiedBeneficiary and was covered under thegroup health plan at the time of the originalQualifying Event or was born to or placedfor adoption with a covered employeeduring the period of COBRA coverage.
PLEASE BE SURE TO COMPLETE ALL ITEMS AND TO SIGN AND DATE FORM.INCOMPLETE FORMS WILL BE RETURNED FOR COMPLETION.
CobraServ National Service Center3201 34th Street South
St. Petersburg, Florida 33711-3828800/488-8757 • Fax: 727/865-3648CS-614/6/00CAP © 2000 Ceridian Corporation

COBRA PROCEDURES MANUALOutlining the policies and procedures followed by our organization
in the fulfillment of COBRA requirements.
This document is supplied solely for the purpose of assisting you in organizing documentation ofyour internal COBRA administration practices. To the extent that any of the information contained in
this document is inconsistent with IRS requirements, IRS requirements will govern in all cases.We suggest that you have this document reviewed by your accountant and/or attorney.
OUR COBRA ADMINISTRATION PROCEDURES:OUR COBRA ADMINISTRATION SYSTEM:COBRA administration functions are performed jointly by our organization andCobraServ, a national COBRA compliance administrator.(Within our organization, COBRA functions are handledby:________________________
Our CobraServ contact is: Client Services DepartmentCobraServ National Service Center3201 34th Street SouthSt. Petersburg, Florida 33711-3828Phone: 800/488-8757
CobraServ will provide all documentation related to the administrative functions it hasperformed on our behalf if requested in connection with an IRS audit.OUR PROCEDURES — Initial Notification of COBRA Rights (check box(es) that apply):
(Internal person responsible:_________________________________________)
Each time an employee and/or spouse becomes covered under our plan, they are notifiedof their COBRA rights as follows:
CobraServ sends an Initial Notice of COBRA Rights Form, based upon theDepartment of Labor Model Notice, via First Class Mail with proof of mailingaddressed to the employee and spouse at the last known home address. Ifspouse resides at a different address, notices are sent to both addresses. Proofof mailing is archived for 7 years.We send a copy of CobraServ-provided Initial Notice of COBRA Rights Form#CS-306 via First Class Mail addressed to the employee and spouse at the lastknown home address. If spouse resides at a different address, notices are sentto both addresses. We retain a copy of this form, which includes addresseeinformation and date sent, on file for 7 years for our records.We send a reproduction of the Initial Notice of COBRA Rights Form, based uponthe Department of Labor Model Notice, via First Class Mail addressed to theemployee and spouse at the last known home address. If spouse resides at adifferent address, notices are sent to both addresses. We retain copies of thesenotices for _____ years, and store them__________________________(location).

All of our currently-covered employees and spouses have been properly providedwith an Initial Notice of COBRA Rights. We retain copies of these notices for_____ years, and store them __________________________(location).
OUR PROCEDURES — COBRA Qualifying Event Notifications:
(Internal person responsible:_________________________________________)Each time an employee or dependent has a “Qualifying Event,” we perform the followingprocedures:
1. Remove the top page entitled “Employer Instructions.”2. Fill out COBRA Notification page of the of multi-part COBRA Notification/Election
booklet #CS-205C.3. Address it to both employee and spouse, if spouse is covered, at their last
known home address (form is designed for a standard window envelope).4. Enclose a copy of the COBRA Rate Sheet applicable to the recipient.5. Retain the pink banded copy of the form for our files, and send the blue banded
copy to CobraServ (which they retain in archive for seven years).6. Mail the Notification/Election booklet via First Class Mail within 14 days of the
Qualifying Event and retain proof of mailing.7. Terminate the person from our group insurance plan.CobraServ handles all subsequent administration related to the Qualifying Event.
OUR PROCEDURES — Billing/Collecting/Ongoing Eligibility Adjudication:
(Internal person responsible:_________________________________________)
1. CobraServ handles receipt, adjudication and processing of COBRA elections,and also handles all of our COBRA premium billing and collecting.
2. CobraServ sends us a Participant Status Update report each time a COBRAcontinuant elects and pays the first premium, a dependent is added or dropped,or a continuant is cancelled.
3. We use this report to update our carrier on COBRA continuants.4. Once a month, CobraServ sends us a complete summary of our COBRA activity
for the previous month, together with a check for the premiums collected.5. We check this report against our own records to verify that all proper COBRA
administrative activities have taken place. We also forward premium paymentsdirectly to the applicable insurance carrier.
OUR PROCEDURES — Maintaining copies of standard form letters sent toQualified Beneficiaries regarding continuation coverage.(Forms specified by the IRS as required for audit purposes should be attached tothis document. NOTE: Forms used by CobraServ for such communications duringthe period in which CobraServ services were in effect will be provided byCobraServ when requested at the time of audit.)

(Internal person responsible:_________________________________________)
FORMS ATTACHED (check applicable items):Forms used prior to utilization of CobraServ administration services.Non-CobraServ forms currently in use.Current version of CobraServ forms have been requested (at time of audit only).
OUR INTERNAL AUDIT PROCEDURES RELATED TO COBRA:Following are the audit procedures we use to ensure that all aspects of COBRAcompliance are being properly administered. (Auditing of CobraServ-performedfunctions is accomplished by reconciling our internal COBRA records with reportsprovided by CobraServ as COBRA-related activities occur, and monthly summaryreports.)Listed below are the COBRA administration functions, the person responsible forauditing them, the audit method, and the audit timeframe.
Function Audited by Audit Method & Frequency
Sending of Initial Notices tonewly-coveredemployees and spouses
Qualifying Event Discovery
Sending of Qualifying Event Noticeswith Rate Sheets
Reconciling internal records ofCOBRA activities with reports providedby CobraServ
Adding or deleting persons to/fromthe group health plan in response toCOBRA status communicatedby CobraServ

COPIES OF ALL GROUP HEALTH PLANS:Accompanying this document are copies of all group health plans in force forour organization. (Check this box as complete after you have attached copies of allof your group health plans, to include policy, Summary Plan Description, and allamendments and riders.)
DETAILS PERTAINING TO ANY PAST REQUEST FOR CONTINUED COVERAGE AND/ORPENDING LAWSUITS RELATING TO COBRA COVERAGE:
Accompanying this document are records of past requests for continuedcoverage and details of pending lawsuits (including pleadings, complaints,answers, etc.) relating to COBRA coverage. (NOTE: CobraServ keeps copiesof all request letters and correspondence related to requests for continuedcoverage, and will make them available upon request at the time of audit.)
(Check this box as complete after you have attached copies of all items requested.)
MAINTENANCE OF RECORDS:Accompanying this document is information concerning all employees whohave left our employment during the current and 6 preceding tax years. If wecover any independent contractors under our group health plans, a similarlist for them is provided.*
(Check this box as complete after you have attached the lists requested.)
Information to include:a) Nameb) Addressc) Marital Statusd) Health plan selected, and whether such plan covered the family or just
the employee.e) Dental plan selected, and whether such plan covered the family or just
the employee.f) Date of termination from the company.g) Date that COBRA Continuation Coverage was made available to the
terminated employee.h) Date that COBRA Continuation Coverage was made available to the spouse
and/or dependents of the terminated employee.i) With regard to items (g) and (h), was this notice written or oral?j) With regard to items (g) and (h), was a separate notice given to each party?k) With regard to items (g) and (h), was the notice hand delivered or mailed?l) Was COBRA Continuation Coverage accepted or rejected by the employee
and/or spouse.m) Was the termination of the employee voluntary or involuntary?
*NOTE: The Pink banded copies of form CS-205C provide the majority of information required.
CS-802/8/02 CAP © 2002 Ceridian