Welcome and introduction - Health Innovation Network...In residential care homes… • 6% increased...
86
Welcome and introduction Viv Parry Chair - Vivienne Parry OBE, health and science writer, presenter and broadcaster
Transcript of Welcome and introduction - Health Innovation Network...In residential care homes… • 6% increased...

Welcome and introduction
Viv Parry
Chair - Vivienne Parry OBE, health and science writer, presenter and broadcaster

New Care Models programme
Sir Sam Everington OBE
GP, Chair of Tower Hamlets CCG, and National Advisor at the New Care Models programme

New Care Models programme
William Roberts
National Care Homes Lead, NHS England

Our work in Sutton
13 October 2016
Chris Elliott: Chief Clinical Officer, Sutton CCGMary Hopper: Director of Quality, Sutton CCG
Sutton Homes of Care Vanguard Programme
4

Overview: The population of Sutton
1213 Care Home Beds
80 Care Homes 203,048Residents in Sutton
14166 aged 75+4450 aged 85+
£1.1M
275 people were
eligible to receive Funded Nursing Care
1770 A&E
presentations from Care Homes
1034Emergency Admissions
Health funded home care packages
Fully funded nursing home placements
£10 M
594 residents in NHS Funded
Nursing Home placements
5

Our Partners
Working in collaboration with:
• NHS England
• New Care Model Programme
• SWL Collaborative Commissioning
• Care Quality Commission
• Health Education England - South London
• Academic Health Science Networks
• Other Care Home Vanguards
Sponsored by:
The National Institute for Health and
Care Excellence (NICE)
… All our Care Homes in Sutton
6

NEW MODEL OF CARE
Inte
grat
ed C
are
Car
e S
taff
Ed
uca
tio
n a
nd
D
eve
lop
me
nt
Qu
alit
y A
ssu
ran
ce a
nd
Sa
fety
Sutton Homes of Care Vision
The vision is implemented through the 3 ‘pillars’:• Integrated Care• Care Staff Education and
Development• Quality Assurance and Safety
Our vision is to have a vibrant, high-quality care home market in Sutton delivering care that embraces the national nursing values of patient care – Care, Compassion, Competence, Communication, Courage and Commitment (the ‘6Cs’).
7

In residential care homes…
• 6% increased achievement in preferred place of death
• 78.5% increase in Sutton residents offered an advance care plan
• 10.9% increase in Sutton residents with a CMC record
• 100% of residents who died with a CMC record achieved their PPD
What we have achieved (1/2)
• 9% reduction in ambulance call outs and conveyances
• 10% - 18% reduction in A&E attendances and unplanned admissions
• 4 days reduction in length of stay in hospital
(results from preliminary evaluation of Hospital Transfer Pathway)
• Reduction of £50k in medicines costs from Nov15 to Mar16 through resident
medication reviews
8

Genuine partnership and collaborative working
(across sector) enabling more joined-up services
Enhanced communication across local health and social care
Bi monthly care home forums for care home mangers
Joint intelligence sharing across partners
Positive impact on care home staff work roles
Engagement with residents and families
Collaborative working with other five care home
Vanguards: Embedding the Enhanced Health
In Care Homes Framework into practice
What we have achieved (2/2)
9

Sutton Homes of Care
Great care is a partnership10

The Hospital Transfer Pathway
13 October 2016
Viccie Nelson: Vanguard Programme Director, Sutton CCGChristine Harger: Vanguard Quality Assurance Lead, Sutton CCG
Sutton Homes of Care Vanguard Programme
11

NEW MODEL OF CARE
Supported by three pillarsIn
tegr
ated
Car
e
Car
e S
taff
Ed
uca
tio
n a
nd
D
eve
lop
me
nt
Qu
alit
y A
ssu
ran
ce a
nd
Sa
fety
Sutton Homes of Care Vanguard Programme
An overview
12

Achievements to date:
Quality Assurance and Safety Pillar
• Joint Intelligence Group
• Quality dashboard developed
• Policy for medicines management in development
13

Achievements to date:Care Staff Education and Training Pillar
Training / Education
• E-learning packages
• Classroom based training
• Bespoke interventions from link staff
• Student nurse mentorship training
underway
Summary of resources
• Concerned About A Resident poster
• Priorities ‘For Care of the Dying
Person’ poster
• Red Bag poster and film
• Reference cards, posters and film
Care Home Forums14

Achievements to date:
Integrated Care Pillar
• Care Home Support Team in place
• Pilot in 6 Nursing Homes: Health and Wellbeing Reviews
• Dementia assessment using DeAR-GP
… and …
• Hospital Transfer Pathway
15

The Hospital Transfer Pathway
16

How we achieved this (1/2)
1. Corridor conversations with partners revealed there were several issues with
the admission/discharge of residents
2. Set up a meeting with all partners involved in care providedo Care homes
o Local hospital
o Ambulance service
o CCG
3. Held “no-blame” conversations to discuss all issues in detail
4. Collaboratively proposed solutions to overcome these issues
5. Continued to work together to implement the pathway
17

How we achieved this (2/2)
Issues identified
• No standard paperwork
• Lost documents
• Loss of residents’ belongings
• Medicines disappear
• No system in place to track residents
through the hospital
• Care homes find it difficult to get
information from hospitals
• Care homes receive lots of phone calls
about the residents’ clinical ‘situation’
• Poor communication between hospitals
and care homes on discharge
• Residents staying in hospital for longer
periods than necessary
Solutions proposed
• Transfer bag
• Standard paperwork to assist
ambulance staff and A&E staff
• Baseline information about the resident
• Better communication between care
homes and hospitals at all points of the
resident’s journey
• Senior staff from care homes to visit
residents in hospital within 48 hours of
admission
18

The standardised paperwork
• CARES Handover Process
• Older Persons Assessment Form
For baseline information
• CARES Escalation Record
To capture the acute episode
• This is Me
(or equivalent)
• MAR Sheet
19

The magic of Red Bag
• 2 or 3 per home depending on size & need
• Serial number to track
• Space for name tag on front
• Spacious inside to hold change of clothes
and personal items
• Separate compartment inside to hold
glasses and visual aids, dentures, hearing
aids and other personal aids
• Sleeve on side to hold paperwork (securely
fastened with velcro)
• Includes a set of cleaning instructions
20

• Standard documentation enhances clinical decision making
• Improves residents experience
• Supports collaborative working and communication
• Alerts hospital staff that the patient comes from a care home
• Aids early discharge and involves care homes in discharge planning
National guidance
• NICE Guideline 27: Transition between inpatient hospital settings and
community or care home settings for adults with social care needs
• NICE quality standard [QS120] Medicines optimisation
• CQUIN Indicator N2: Reduction in Emergency Admissions.
Supports best practice
21

Demonstrable impact to date
• 179 residents of care homes have been tracked through our local
hospital in the last nine months
• Average length of stay with a bag was 13.4 days, compared to
17.4 days without a bag
Residents with a Red Bag have 4 days less
in hospital than those without a Red Bag
Note: Data kindly collected by Integration and Transformation
Team and Oder People Nurses at our local hospital
22

Training film and poster
https://www.youtube.com/watch?v=XoYZPXmULHE23

Perspectives
24
Short film: The red bag from a residents perspective
https://youtu.be/MP03jUtBXmA

Sutton Homes of Care
Great care is a partnership
http://www.suttonccg.nhs.uk/VANGUARD 25

@HINSouthLondon
www.hin-southlondon.org
Our Focus on Care Homes
Rebecca Jarvis
Programme Director, Health
Innovation Network

The Health Innovation Network is the
Academic Health Science Network (AHSN)
for South London, one of 15 AHSNs across
England.
We connect academics, NHS
commissioners and providers, local
authorities, patients and patient groups,
and industry in order to accelerate the
spread and adoption of innovations and
best practice, using evidence-based
research across large populations.
Working as catalysts of change across
health and social care economies,
we enable health improvements and
economic growth.
Population
3 Million
Healthcare
Workforce of
60,000+
55Member
Organisations
12South London
Boroughs

Together with our members we have prioritised health challenges for our local
communities…
Clinical Themes Cross-cutting themes
Patient &
Public
Involvemen
…creating clinical and cross-cutting themes, with patient and public involvement
running throughout all of our programmes.
Diabetes
Dementia
Musculoskeletal
Alcohol
Economic Growth
Technology & Information
Digital Health
Patient Experience
Education & TrainingAtrial Fibrillation
Patient Safety

www.hin-southlondon.org | @HINSouthLondon
Why focus on care homes?
• 70-80% of residents are living
with dementia
• One third of people living with dementia
• Estimated 9000 people in south London
• Negative press
• High annual staff turnover
• Low pay
• Poor access to training and development

www.hin-southlondon.org | @HINSouthLondon
Care homes in south London
356CARE HOMES
for older people
12,760BEDS
>100CARE HOME
PROVIDERS

www.hin-southlondon.org | @HINSouthLondon
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Kingston upon Thames
Sutton
Croydon
Bexley
Bromley
Merton
Greenwich
Wandsworth
Richmond upon Thames
Lambeth
Lewisham
Southwark
LA funded placements Self funded/vacant beds
Proportion
of Local
Authority
funded
placements
in each
Borough

www.hin-southlondon.org | @HINSouthLondon
Aashna House
in Lambeth
Care homes in south London

www.hin-southlondon.org | @HINSouthLondon
Care homes in south London

www.hin-southlondon.org | @HINSouthLondon
Morden College
in Greenwich
Care homes in south London

www.hin-southlondon.org | @HINSouthLondon
South London Care Homes Network
• Engage the sector in the work of the HIN
and our members
• Disseminate innovation and best practice
• Share information about local, national and
legal requirements
• Communicate a positive image and
reputation of the sector
• Find out about local and national
initiatives for workforce development
and research
• Network with others from the sector
and with industry

www.hin-southlondon.org | @HINSouthLondon
https://vimeo.com/185712372/59992645ce

www.hin-southlondon.org | @HINSouthLondon
Care Homes leads network
• Contracts monitoring teams
• CCG & Local Authority
Commissioners
• Care home liaison teams
• Quality improvement teams

www.hin-southlondon.org | @HINSouthLondon
HIN projects with Care Homes
• DeAR-GP: Detecting dementia
in care homes
• Barbara’s Story – dementia
awareness training
• My Catheter Passport –
promoting good catheter care

Working with Sutton Homes of Care
Spreading
the Red Bag
across
south
London

www.hin-southlondon.org | @HINSouthLondon
Thank you

Panel Q&A session• Sir Sam Everington OBE
• William Roberts
• Chris Elliott
• Mary Hopper
• Viccie Nelson
• Christine Harger
• Rebecca Jarvis

Workshops: Morning session
Option Part 1 Part 2 Location
1 Family Perception of Care Audit: St Christopher’s
Hospice
Increasing resident engagement and inclusion through
democratic participation: NDTi (National Development
Team for Inclusion)
Lil Patrick (Third
Floor)
2 Southwark Care Homes Enhanced GP Service and
Multi-Disciplinary Team
The future of collaborative working across care and
education providers enabling the delivery of bespoke,
high quality higher apprenticeship: Greenwich and
Bexley Community Hospice
Max Nasatyr (Third
Floor)
3 Better Together: An Integrated Approach to Enable
Active Residents in Care Homes (ARCH): St Georges
University Hospitals NHS Foundation Trust
DeAR-GP- Dementia Assessment and Referral to GP:
Health Innovation Network
South Bank room 1
4 Making Mealtimes Matter: Bromley Healthcare CIC The Behaviour and Communication Support Service
(BACSS): South West London St. Georges Mental Health
NHS Trust
Fred Miller (Third
Floor)
5 In the Garden: Spare Tyre Theatre Company South Bank room 2
(LG Floor)

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Innovations in Telemedicine and the Digital Care Hub– learning from a Care Homes Vanguard
Rachel BinksNurse Consultant – Digital & Acute CareAiredale NHS Foundation Trust

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Telecare
Telecoaching
Telemonitoring
Teleconsultation
Digital Health

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
A system designed by default
Some people seem to do quite well without waiting for healthcare support…

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Teleconsultation Prison health care
Care at home
Nursing & residential care
Supporting end of life patients
24/7 clinical hub
improving patient experience
changing patient flow
reducing costs
Electronic shared recordconnecting primary & secondary care now
connecting whole health & social care economy tomorrow
right care today

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
right time – care anywhere

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
right place - replicable model
475 Nursing/Residential Care Homes + 50 in implementation
Supporting > 14,000 residents
NEWCASTLE
LEEDS
MANCHESTER
BIRMINGHAM
LONDON

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Provide, safe, effective high standards of care
To support residents to stay at home
Support residents/nurses/
carers in the planning
and delivery of care
Escalate to community
teams out of hours
Aims of the service

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Gold Line
GP Triage
Intermediate Care Hub
Acute Care Team
Single Point of Access
Complex Care Team
Other services delivered from the digital care hub
Shared record
Registered practitioners
Visual contact

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
http://www.health.org.uk/gold-line
http://www.airedale-trust.nhs.uk/services/telemedicine/
Video insight into our telemedicine and Gold Line Service

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
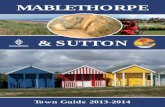
Data from End of Life Care Profiles PHE and district wide reporting (CSU)
National data England 2013
AWC 2013 Bradford District 2013
Bradford City 2013
GSF/Gold LineYear 2013/14
All deaths in hospital
48.3 36.0 45.9 50.4 14%
All deaths at home
22.4 20.1 24.5 23.1 41%
All deaths in care homes
21.6 33.2 19.0 19.7 22%
All deaths in hospice
5.5% 8.8 8.3 4.6 23%

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Call sheet

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
ReportingNursing Homes
Residential Homes
Day Current Month
Last Month
% Variance
YTD Day Current Month
Last Month
% Variance
YTD
Monday 128 85 51% ↑ 213 Monday 194 153 27% ↑ 347
Tuesday 117 74 58% ↑ 191 Tuesday 174 121 44% ↑ 295
Wednesday 83 83 0 ↔ 166 Wednesday 152 121 26% ↑ 273
Thursday 76 79 4% ↓ 155 Thursday 128 104 23% ↑ 232
Friday 88 108 19% ↓ 196 Friday 145 160 9% ↓ 305
Saturday 106 107 1% ↓ 213 Saturday 153 174 12% ↓ 327
Sunday 110 76 45% ↑ 186 Sunday 197 108 82% ↑ 305 Time Current
MonthLast
Month%
VarianceYTD Time Current
MonthLast
Month%
VarianceYTD
Morning 295 255 16% ↑ 550 Morning 456 379 20% ↑ 835
Afternoon 413 357 16% ↑ 770 Afternoon 687 562 22% ↑ 1,249
Hours Current Month
Last Month
% Variance
YTD Hours Current Month
Last Month
% Variance
YTD
In Hours 344 329 5% ↑ 673 In Hours 466 419 11% ↑ 885
Out Of Hours 364 283 29% ↑ 647 Out Of Hours 677 522 30% ↑ 1,199
Total 708 612 1143 941

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Reason for callNursing Homes Residential Home
Purpose Current Last % Variance YTD Current Last % Variance YTD
Advance Plan/DNAR 0 0 0 ↔ 0 0 0 0 ↔ 0
Agitation/Confusion 0 0 0 ↔ 0 0 0 0 ↔ 0
Anxiety 1 4 75% ↓ 5 8 11 27% ↓ 19
Bowel concerns 0 0 0 ↔ 0 1 0 100% ↑ 1
Breathing difficulties 18 14 29% ↑ 32 31 17 82% ↑ 48
Catheter concern 12 10 20% ↑ 22 26 22 18% ↑ 48
Cerebral event 1 0 100% ↑ 1 0 0 0 ↔ 0
Chest infection 75 65 15% ↑ 140 68 46 48% ↑ 114
Chest pain 2 0 100% ↑ 2 7 9 22% ↓ 16
Death 0 0 0 ↔ 0 0 0 0 ↔ 0
Dehydration 12 6 100% ↑ 18 24 7 243% ↑ 31
Emotional distress 7 4 75% ↑ 11 6 8 25% ↓ 14
EOL Symptoms 0 0 0 ↔ 0 0 0 0 ↔ 0
Eye Infection (eye) 8 9 11% ↓ 17 21 7 200% ↑ 28
Falls 49 31 58% ↑ 80 119 91 31% ↑ 210
General Deterioration 0 0 0 ↔ 0 0 0 0 ↔ 0
Head Injury 0 0 0 ↔ 0 0 0 0 ↔ 0
Medication issue 0 0 0 ↔ 0 1 0 100% ↑ 1
Nausea 4 1 300% ↑ 5 6 5 20% ↑ 11
Other 239 197 21% ↑ 436 398 251 59% ↑ 649
Pain Management 39 24 63% ↑ 63 68 50 36% ↑ 118
Seizure 5 5 0 ↔ 10 10 3 233% ↑ 13
Skin complaints 86 25 244% ↑ 111 106 86 23% ↑ 192
UTI (suspected) 68 41 66% ↑ 109 109 76 43% ↑ 185
Vomiting 13 10 30% ↑ 23 18 10 80% ↑ 28
Wound care 11 5 120% ↑ 16 17 30 43% ↓ 47

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Outcome of calls
Nursing Homes Residential Homes
Referral Current Month
Last Month
% Variance YTDCurrent Month
Last Month
% Variance YTD
collaborative care team 0 1 100% ↓ 1 0 3 100% ↓ 3
community matron 2 3 33% ↓ 5 4 12 67% ↓ 16
district nurse 12 5 140% ↑ 17 60 72 17% ↓ 132
palliative care service 0 1 100% ↓ 1 0 0 0 ↔ 0
palliative care physician 0 0 0 ↔ 0 0 1 100% ↓ 1
Referral to social services 0 1 100% ↓ 1 0 0 0 ↔ 0
Referral to GP 224 204 10% ↑ 428 258 223 16% ↑ 481
GP out of hours service 170 115 48% ↑ 285 209 152 38% ↑ 361
Intention (would have) Current Month
Last Month
% Variance YTDCurrent Month
Last Month
% Variance YTD
called their GP 509 342 49% ↑ 851 721 509 42% ↑ 1,230
attended A&E or called an ambulance 56 38 47% ↑ 94 85 68 25% ↑ 153
contacted community nursing 8 9 11% ↓ 17 69 58 19% ↑ 127
Not have contacted an alternative healthcare provider
20 6 233% ↑ 26 32 18 78% ↑ 50
Not applicable 57 56 2% ↑ 113 137 76 80% ↑ 213
Outcome Current Month
Last Month
% Variance YTDCurrent Month
Last Month
% Variance YTD
Patient remained in place of residence 618 527 17% ↑ 1,145 1,018 779 31% ↑ 1,797
Ambulance request for patient 83 65 28% ↑ 148 123 110 12% ↑ 233
Hospital notified of death 7 2 250% ↑ 9 9 9 0 ↔ 18

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
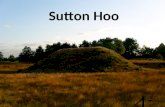
What would you have done?
0
50
100
150
200
250
300
350
W/C
07
/12
/20
15
W/C
14
/12
/20
15
W/C
21
/12
/20
15
W/C
28
/12
/20
15
W/C
04
/01
/20
16
W/C
11
/01
/20
16
W/C
18
/01
/20
16
W/C
25
/01
/20
16
W/C
01
/02
/20
16
W/C
08
/02
/20
16
W/C
15
/02
/20
16
W/C
22
/02
/20
16
W/C
29
/02
/20
16
W/C
07
/03
/20
16
W/C
14
/03
/20
16
Called an ambulance
Contacted a GP
Contacted a community nurse
Done nothing
Question not asked (follow upetc)

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
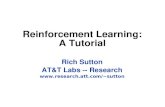
Actual GP referrals
0%
10%
20%
30%
40%
50%
60%
70%
80%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb
Referred toOOH GP %
Referred toIn Hours GP%
Referred GP(both In &Out of Hours) %

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Clinical assessment by Hub nurse
Onward refer if required to HCP for home visit
Request prescription
GP surgery informed by NHS secure mail
GP triage

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
"Of all the changes in the 15 years I have been working this is the greatest change which has reduced workload I can remember. I don't mind the extra "late" duty doc visit as this is more than made up in the drop in other visits. A big thank you to all involved."
GP feedback

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
“The innovation that telemedicine promises is not just doing the same thing remotely that used to be done face to face, but awakening us to the many things that we thought required face to face contact, but actually do not.”
David D Asch MD, MBA, Perelman School of Medicine, University of Pennsylvania
Innovation potential

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Support for care home staff using the VTR
Support for DNs and community teams – do they need to attend?
Overview and clinical support of care home staff developing enhanced roles
Remote outpatient clinics
Remote training and clinical support

E n h a n c e d h e a l t h i n c a r e h o m e s
Airedale and Partners
Enhanced Health in Care Homes Vanguard
Technology Enabled Health – the art of the possible…
Questions

Workshops: Afternoon session
Option First presenter Second presenter Location
1 Namaste Care: To Honour the Spirit Within: Ebury
Court Care Home
The role of the OT within the Mental Health Care Home
Intervention team (MHCHIT) to promote activity
engagement in care homes: South London and Maudsley
NHS Foundation Trust
Max Nasatyr (Third
Floor)
2 Southwark Care Homes Enhanced GP Service and
Multi-Disciplinary Team
The future of collaborative working across care and
education providers enabling the delivery of bespoke,
high quality higher apprenticeship
Lil Patrick (Third
Floor)
3 Care homes: Implementing, sustaining and
evidencing the delivery of quality end of life care: St
Christopher's Hospice
An Innovative Integrated Model of Care for Nursing
Homes: The Royal Marsden NHS Foundation Trust
South Bank room 1
4 RADIQL (Reminiscence Arts and Dementia Impact on
Quality of Life): measurably improving the
Wellbeing of older people with dementia in
residential
care homes: Age Exchange
Reducing loneliness in care homes through trained
volunteers: Embracing Age
Fred Miller (Third
Floor)
5 In the Garden: Spare Tyre Theatre Company South Bank room 2
(LG Floor)

NHS Sunderland and Whzan delivering
best practice in care home telehealth
13th October 2016
Rachael Forbister
Telehealth Lead, Sunderland CCG
John Cooling
Chairman, Solcom Ltd

Contents
• The Care Model
• Case Example: Improving Care in Care Homes
• How we did it
• Expected Outcomes
• The Challenges
• Whzan
• Isle Of Wight
• Next steps

The Care Model
@ATBSunderland

Case Example: Improving Care in Care Homes
Complex healthcare needs, multiple long termconditions
Skills within residential care homes not
necessarily sufficient
Communication challenges between providers
Residents currently do not have equitable access to healthcare which can lead to hospital admissions
The need to improve early detection of acute illness in residents
Provides care closer to home to improve patient experience

• What is NEWS
• NEWS is the National Early Warning Score• Ensures a standardised means of identifying and
responding to deteriorating or acutely ill patients in the community and in-hospital setting.
• Simple scoring system using 6 physiological measurements
• Determines an overall score which is risk rated• Provides a continuous record of the patient
physiological status throughout.• More effective handover to other Health Care
professionals i.e. GP’s, OOH’s, community nurses, ambulance and Acute hospital staff.

• What It means to Care Homes
• Aids recognition of clinical deterioration• Standardises acute illness assessment in
the community care setting• Enable communication to other HCP’s
using a common language• Defines appropriate level of on-going care
required.• Supports professional/clinical leadership
within homes• Promotes collaborative working with other
external healthcare colleagues

How we did it!

Reduction in 111 and 999 calls
Reduction in A&E visits and emergency admissions
Improved early detection of acutely unwell residents
Sharing of clinical information across all providers
Promotes collaborative working with providers
Improved safety and quality of information on handover
Expected Outcomes

The Challenges!
Standard tools
Engagement
Cultural change
Scale and Sustainability
Scope Creep!
Interoperability

Whzan TELEHEALTH
Established 1998.
On the Isle of Wight.
Specialists in Internet of Things.
Bespoke software / system creators for pharmaceutical, health and nuclear industries.
Telehealth system created in 2010 with NHS South Central
Specialists in telehealth monitoring of LTCs and elderly care at home and in homes.
Winners of 2016 HSJ Best Value in Telehealth with NHS Sunderland.
A little bit about Solcom LTD & Whzan Telehealth

Whzan TELEHEALTH
JV between Local Authority and NHS Acute Trust, St Mary’s
Included within the programme, IW integrated care hub. 999/111 aware of residents and patients who are being monitored.
GPs on board.
Delivered by “Equipment Services” department. Thus maintaining a cost effective overview of the resident needs and provide backup.
Isle of Wight care home experience

Whzan TELEHEALTH
Improved patient safety and care by early detection of changes in condition using NEWS, MUST, Abbey Pain.
Improved outcomes for residents, happier for longer
Reductions in calls to 999, OOH and A&E.
Reductions in hospital stay, so important for elderly to avoid further deterioration in mobility and health.
Increased family involvement and comfort.
Monitoring is taken to the resident.
Care Home monitoring objectives

Whzan TELEHEALTH
Get all possible parties onside, as per Rachael.
Appreciate care home culture as being risk averse.
Review care home protocols, is 999 a default position?
Develop relationship with care home owner as well as Registered Managers, improves roll out.
Include local ambulance service within the proposal to improve care home protocols.
Training of care home staff. NEWS and MUST, a very positive deal here!
Determine who is deemed to be management of the care home and who is accepting responsibility. Inform care home GP.
Delivering an installation, issues.

Whzan TELEHEALTH
The Whzan tablet application can be used to collect the readings of a resident and present them as a chart so a visiting clinician can see the trends.
Care workers are empowered as Whzan will lead them through assessments (e.g. NEWS) and show the results on a green/amber/red screen.
Set the alert parameters of a resident so that readings are consistent with their historic condition.
The information can be shared with clinicians, or viewed on a patient portal.
Data reports, exports and links to other system are available. can be uploaded to the patient record…..if……EMIS, System One co-operate! However, they will try to charge you!!
Information and Data, definitely NOT the tricky bit.

Whzan TELEHEALTH
Engage with the care home owner and manager.
Inform the local GP.
Work with the protocols, but keep in mind this is about improved safety and appropriate use of primary and secondary care.
Roll out slowly, with sufficient Whzan tablets, e.g. a system per floor in a care home.
Present early to care home staff and let them train on the equipment to understand how easy it is to use. Encourage them to take their own readings.
Let the family know there is something new for improved safety.
Setting up

Whzan TELEHEALTH
Homes need about 2/3 weeks to get used to something new.
Carers take about 10 minutes to learn how to use Whzan.
NEWS limits get adjusted for patients who have abnormal symptoms
Almost all residents welcome this new form of care, it gives them comfort, reduces anxiety.
Remind users to recharge the system overnight!
Ask for feedback, Whzan development is based on it.
Medication changes are common in the first few weeks.
IW report one admission or ambulance saved per care home per week.
Our experience

Whzan TELEHEALTH
Enhancements, just ask and we’ll deliver.
Enhancements are shared with whole user group.
They come for free and can be remotely installed.
NHS users share their protocol documents.
Extra features to make life easier with a step down facility….”Whzan lité”.
Where to next?

Contact details and question time?
• Rachael Forbister
• @Rforbister
• John Cooling

Closing remarks
Viv Parry
Chair - Vivienne Parry OBE, health and
science writer, presenter and broadcaster

Thank you!
Presentations:
www.hin-southlondon.org/clinical-areas/dementia/resources