WEEK 3 – PATIENT CARE ICV 113 Interventional Neuroradiology.
27
WEEK 3 – PATIENT CARE ICV 113 Interventional Neuroradiology
-
Upload
jody-greer -
Category
Documents
-
view
225 -
download
1
Transcript of WEEK 3 – PATIENT CARE ICV 113 Interventional Neuroradiology.

WEEK 3 – PATIENT CARE
ICV 113 Interventional Neuroradiology

Objectives
Week 3– Patient Care Discuss the potential neurologic complications
of Cerebral/Spinal Angiography Discuss the potential nonneurologic
complications of Cerebral/Spinal Angiography Discuss premedication for patients with
contrast reactions Discuss hydration and the Diabetic patients Discuss prevention of contrast-induced
nephropathy Discuss the importance of postprocedural
patient care

Patient Care: Remember the Following!!!
Professional Attitude
Team confidence Limit extraneous
conversation Communicate with
the patient Minimize patient
stress Never leave patient
unattended
“TIME OUT” (Correct patient? Procedure?)
Make sure pre-cath orders were followed
Allow patient to wear glasses and dentures if possible
Check for Signed Consent
04/19/23
3

What if You Were the Patient?
04/19/23
4
One of the most common complaints from patients is concerning the staff’s non-professional behaviour.
Always keep in mind the “Golden Rule” and put yourself in the patient’s shoes.
How would you like to be treated?

04/19/23
5
Dr. Morris is quoted as saying, “Many or most complications can be avoided by a methodical and systemic execution of all diagnostic studies with consistent use of simple, uncompromising, and unhurried routines.”

TWO KEY WORDS FOR ICV: ANTICIPATION AND CONSISTENCY
04/19/23
6
The text points out the importance of quick recognition of any problems before they become larger.
Always be aware of the patient and their environment, not what happened on TV last night.

Possible Causes of Complications
04/19/23
7
Below is a list of some potential causes of complications. One should look for these “red flags” prior to, during and after the angiogram.
Patient population (age, gender,etc.)
Type(s) of disease the patient has
Who referred the patient (is this procedure appropriate or would CT/MRI be better?)
Experience level of the Physician (and staff!!!)

Risk Factors for Cerebral Angiography
04/19/23
8
Patients that have/are:
History of Stroke or TIAs (Transient Ischemic Attacks)
50-70% stenotic disease in cerebral vessels
Older than 70 yrs. of age
Angiograms which require a higher volume of contrast
Angiograms that last 60 to 90 minutes or require multiple catheter exchanges
Systemic hypertension (HTN) or renal impairment
Referred for subarachnoid hemorrhage (SAH) or who are immediately postoperative

Other Procedure - Related Risks
04/19/23
9
The following are some procedure-related risks (complications) that the Physician and staff must constantly be aware of during the procedure itself.
Neurologic Complications:
Microemboli
Microbubbles
Aneurysm Rupture (if applicable)

Neurologic Complications
04/19/23
10
Neurologic complications result when pieces of plaque or other debris become dislodged from the vessel wall and travel up into the blood vessels of the brain.
Air bubble come from syringes and/or pressure-bags that have not been carefully connected so as not to have any microbubbles within the system.
Aneurysm rupture comes from careless handling and pinning of the wire(s) being used.

An Ounce of Prevention…. The Telfa Pad
04/19/23
11

Microbubbles and the Syringe
04/19/23
12
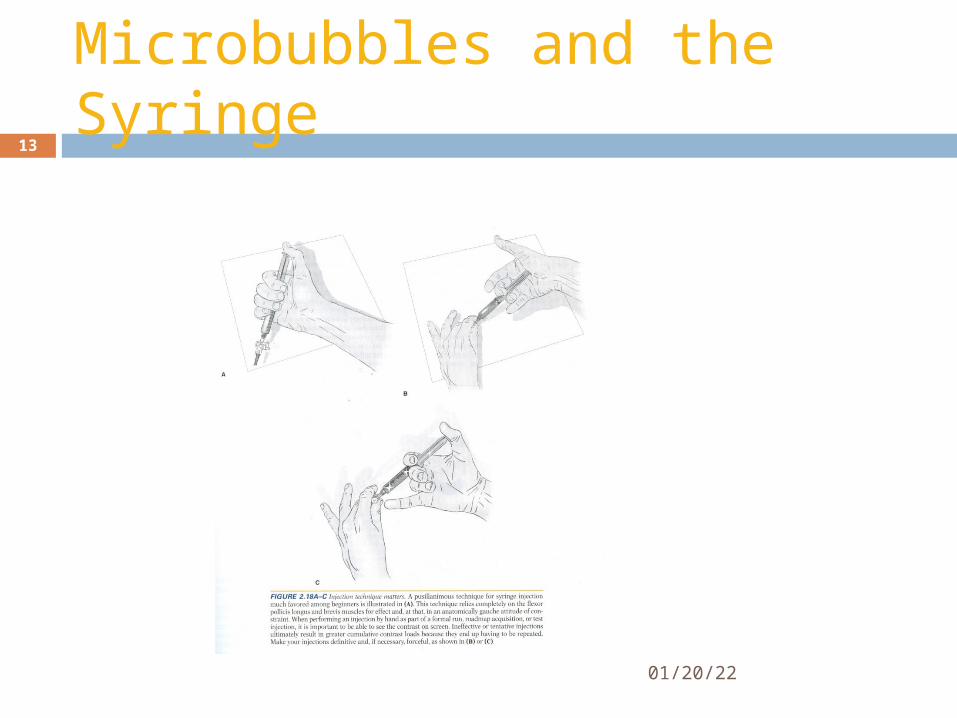
Microbubbles and the Syringe
04/19/23
13

Pressure Bag Set-Up
04/19/23
14

Other Procedure - Related Risks
04/19/23
15
• Major Nonneurologic Complications:
Hematoma formation Dissection of artery Pseudoaneurysms MI (myocardial infarction) Cardiac Arrest Angina Pectoris Allergic Reactions
Pseudoaneurysm

Dissection with Thrombosis
04/19/23
16

Aneurysm Rupture
04/19/23
17
If in the unfortunate event an aneurysm is ruptured, the first course of action may be to reverse any Heparin that may have already been given.
What drug reverses the effects of Heparin?
Answer: __________?

Neurologic Complications
04/19/23
18
Minor Nonneurologic Complications:
Nausea or vomiting Bradycardia Extrasystoles Fainting Delayed hematoma after discharge from
hospital

Premedication of Patients
04/19/23
19
Many times, questions arise concerning the patient’s medications they are taking. Should they or should they not take them prior to a Cerebral Angiogram?
It’s best to refer the question to the Physician
The next slide will answer many of those questions based on many Physicians decisions.

Patient Preparation and Prescription Drugs Prior to Angiogram
04/19/23
20
Diet and Hydration (NPO prior to most procedures) Medications
1. Insulin (may take- at lower dosage)2. Glucophage (48 hrs. prior and post)3. Antihypertensives (yes)4. Diuretics (Lasix)- no5. Heparin (stopped 2-6 hrs prior)6. Warfarin (stopped 5-10 days prior)7. Lovenox ( 5-10 days by most) 8. Aspirin9. Ativan (pre-procedure sedation)

Patients with Impaired Renal Function
04/19/23
21
Prevention of Contrast-Induced Nephropathy1. Mucomyst2. Corlopam3. Sodium Bicarbonate infusion (? Under debate)4. Theophylline

Pre-Procedure CareOther Possible Issues to Address
04/19/23
22
Prophylactic Antibiotics (Possible Infection) Within 2 hours of procedure
Correction of Coagulopathies (Bleeding Disorders)

Vasovagal Response
04/19/23
23
A response generated from fear or nervousness.
Characterized by pallor, diaphoresis, nausea, and hypotension, which is frequently preceded by, or accompanied by bradycardia.
TREATMENT: fluids, Atropine, patient in Trendelenburg

Intra-Procedure Care
04/19/23
24
Hypertension (Labetalol) Bleeding (Increase Fluids ? CT) Contrast Reactions Hypoglycemia (Check Blood Sugar level) Dysrhythmias (“PULL BACK!!!”) Sepsis (Antibiotics) Seizures (Valium) Air Embolism –Use extreme caution and watch
pressure lines for any bubbles CARDIAC ARREST (Start CPR –Call Code!)

Intra-Procedure Care
04/19/23
25
Reaction to Sedatives and Analgesics
1. Nausea and Vomiting (Compazine)2. Decreased Resp. or BP (Narcan or Romazicon)

Post Procedure Care
Achieve Hemostasis Monitor puncture site Vital signs should be
monitored every 15min for 1 hour
Give post procedural instructions for closure devices (varied due to type)
04/19/23 26

References
Morris, P.P. Practical Neuroradiography, 2nd Edition, 2007
Osborn, A.G. Handbook of Neuroradiology, 2nd Edition, 1999
Bontrager, K.L. TEXTBOOK of Radiographic Positioning and Related Anatomy , 5th Edition, 2001
Snopek, A.M Fundamentals of Special Radiographic Procedures, 5th Edition, 2006
Tortorici, M.R. Fundamentals of Angiography, 1982
Various other Internet sources