
Webinar Instructions - NCOA · Embedding CDSME Programs within Agenda • Join Ivana Krajcinovic...
35
1 A nonprofit service and advocacy organization © 2012 National Council on Aging Webinar Instructions
Transcript of Webinar Instructions - NCOA · Embedding CDSME Programs within Agenda • Join Ivana Krajcinovic...

1
A nonprofit service and advocacy organization © 2012 National Council on Aging
Webinar Instructions
2
A nonprofit service and advocacy organization © 2012 National Council on Aging
Embedding CDSME Programs within
Health Care Organizations
Agenda
• Join Ivana Krajcinovic (UNITE HERE HEALTH) and Kim
Wicklund (Group Health Cooperative) to hear first-hand from
two health care organizations that have embedded CDSME
programs into their day-to-day operations. Ivana and Kim will
share information about their implementation models, as well
as speak to recommended strategies for engaging health
care organizations.
• Q&A – All

Los Angeles & Orange County
CDSMP PILOT PROGRAM
February 2012 – February 2013
3
4
• Union health plan serving unionized hospitality workers in the US
and Canada
• Las Vegas, Atlantic City, Chicago, NYC, LA, Monterey, Pittsburgh
plus national plans
• 190,000 covered lives
• Immigrants and the working poor
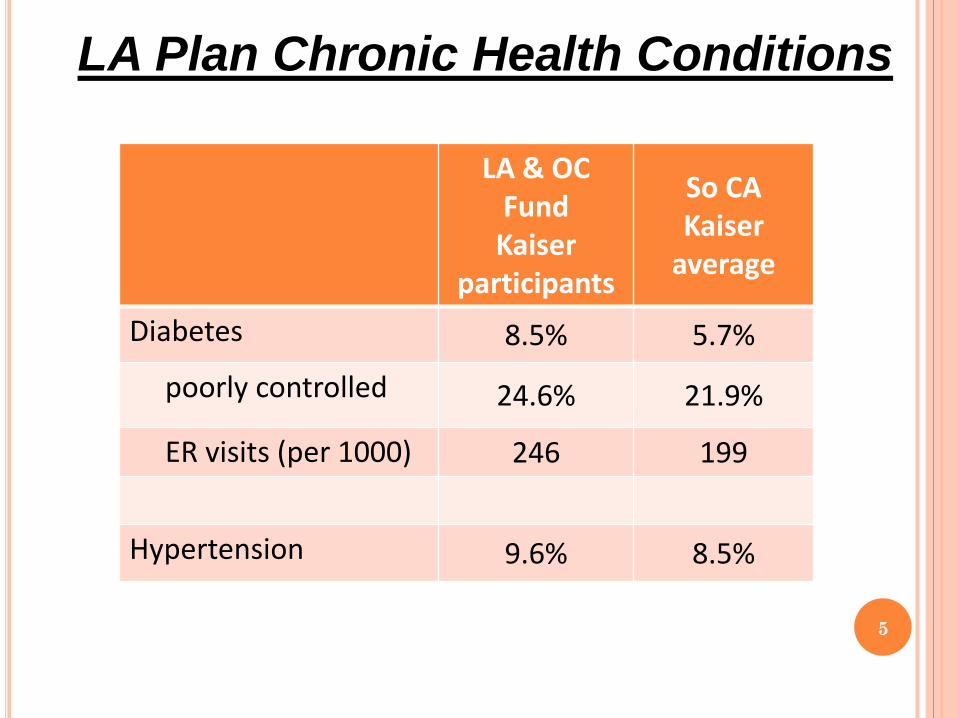
LA Plan Chronic Health Conditions
5
LA & OC Fund
Kaiser participants
So CA Kaiser
average
Diabetes 8.5% 5.7%
poorly controlled 24.6% 21.9%
ER visits (per 1000) 246 199
Hypertension 9.6% 8.5%
LA Plan Participants with 1 or more
Chronic Health Conditions
6
• 16.0% of participants
• 2,706 total participants
• 41.6% of costs
7
UHH LA and OC program
Recruitment and follow-up
Monthly meetings for graduates
Recruit volunteer leaders
Texting program (Anjna)
Graduates who come to 6 monthly meetings are eligible for up to $100/month in reimbursement for maintenance medication copays each month they attend a monthly meeting
Participation
8
At the end of the first year…. 281 entered the program
89% graduated
19 workshops in LA and Orange County
76% come to monthly meetings for graduates
9
Goals for 2nd year
Enroll an additional 500 in 35 workshops
Develop 20 trained leaders
Reduce staff
Formal evaluation (Partners in Care)
Expand program to Chicago, Las Vegas, CT and MA
10
Veroni ca

11
Veroni ca Jef f rey

12
Veroni ca l eadi ng her f i rst workshop

LESSONS LEARNED
You have more control over healthcare that you
think
Boots on the Ground
Prove that you’re serious
Leverage existing relationships
13

Group Health’s experience
February 19, 2013 | Kimberly Wicklund, MPH
Implementing CDSMP in an
integrated health care system

Group Health
Consumer-governed, non-profit
financing and care delivery
system founded in 1947
Mission: To design, finance and
deliver high-quality health care
623,000 members in
Washington and North Idaho
Integrated group practice: 25
medical centers
Contracted provider network:
9,000 physicians

Patient-centered care and innovation
Core values reflected in initiatives to:
Partner with patients:
Healthier lifestyles
Clinical preventive services
Chronic disease self-management
Activate and engage patients:
MyGroupHealth
Health Profile
Shared decision-making
Provide evidence-based, planned care through:
Coordinated outreach
Opportunistic care
Deliver patient-centered through medical home
Rationale for CDSMP at Group Health
Strong evidence for improved skills, self-efficacy,
outcomes
Patient centered
Low-cost intervention
Enables clinical staff to focus on complex medical
issues instead of self-management skills
Engages consumers, as well as patients

Group Health’s Model
Guiding principals
1. Strive for population impact
2. Enable equal access to CDSMP regardless of where
member gets care
3. Offer program in various ways to respond to patients’
unique needs
4. Maintain ongoing commitment to exploring new and
innovative approaches
Face-to-face CDSMP
Started in1998
58 volunteer leaders
Offered in18 medical centers
Retention: 69%
Maximum reach to date: 632 (2007)
Reach in 2012:
29 workshops
359 people
Current evaluation focus: fidelity
Web-based CDSMP
Funded by Group Health Foundation Partnership for Innovation
Partners: National Council on Aging, Stanford University, Group Health Research Institute
Goal: assess if web-based CDSMP increases uptake by members who are not using in-person program
In health plan network
Younger
473 participants
Retention: 66%
Evaluation:
Administrative data review for utilization and costs
Baseline and 6 month follow-up survey for self-reported health status, health behaviors, and utilization
Web-based CDSMP evaluation results
Expanded reach by 30%
Reached younger population– average age was 55, 10 yrs younger than face to face
Significant improvements in:
Depression
Pain
Fatigue
Health distress
Trend toward more use of primary care and less of specialty
Limited reach in health plan network
Diabetes Self-Management Program pilot
Funded by Group Health Foundation (2012)
Goal: pilot 8-10 DSMP workshops at Group Health medical centers
Actual reach:
14 workshops
208 total participants
Evaluation in process:
Survey: self-management behaviors, blood sugar
knowledge, medication management
EMR review: clinical measures, and health care utilization
DSMP pilot feedback
“Today I received my latest
blood and kidney test
results, and for the first time
in my adult life they all were
within normal ranges. My
A1c was 5.7….”
Employer pilots
Testing 3 approaches:
1. Worksite-based workshops (King County)
4 workshops in 2012- 56 employees
Retention: 87%
Gold status for documented attendance of ≥4 sessions
2. Formal reporting of participation (SHWT)
GH/SHWT reporting process for incentivizing employees
attending ≥4 sessions online or in person
3. Employee self report on participation (Group Health)
≥4 sessions in person or online for 400 wellness points

Reach 1999-2012
0
100
200
300
400
500
600
700
800
900
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Total members enrolled in Living Well with Chronic Conditions 1999 to 2012*
*2012 includes Living Well with Diabetes
Online
Total
In person

Recruitment
Strategies
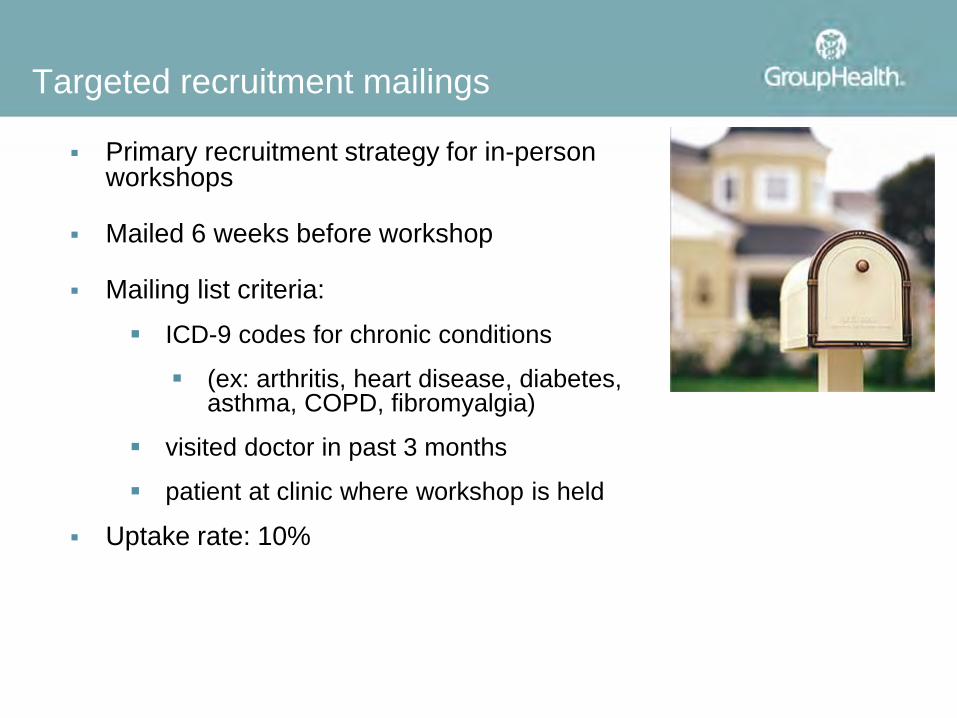
Targeted recruitment mailings
Primary recruitment strategy for in-person workshops
Mailed 6 weeks before workshop
Mailing list criteria:
ICD-9 codes for chronic conditions
(ex: arthritis, heart disease, diabetes, asthma, COPD, fibromyalgia)
visited doctor in past 3 months
patient at clinic where workshop is held
Uptake rate: 10%
Embed in provider tools and workflow
Provider can order brochure to be mailed to patient directly from electronic medical record (EMR)
Insert messages into After Visit Summary from EMR
Point of care prompts in EMR to encourage referrals
Clinic-based champions encourage referrals in team huddles and emails
Built into medical home as a standardized referral
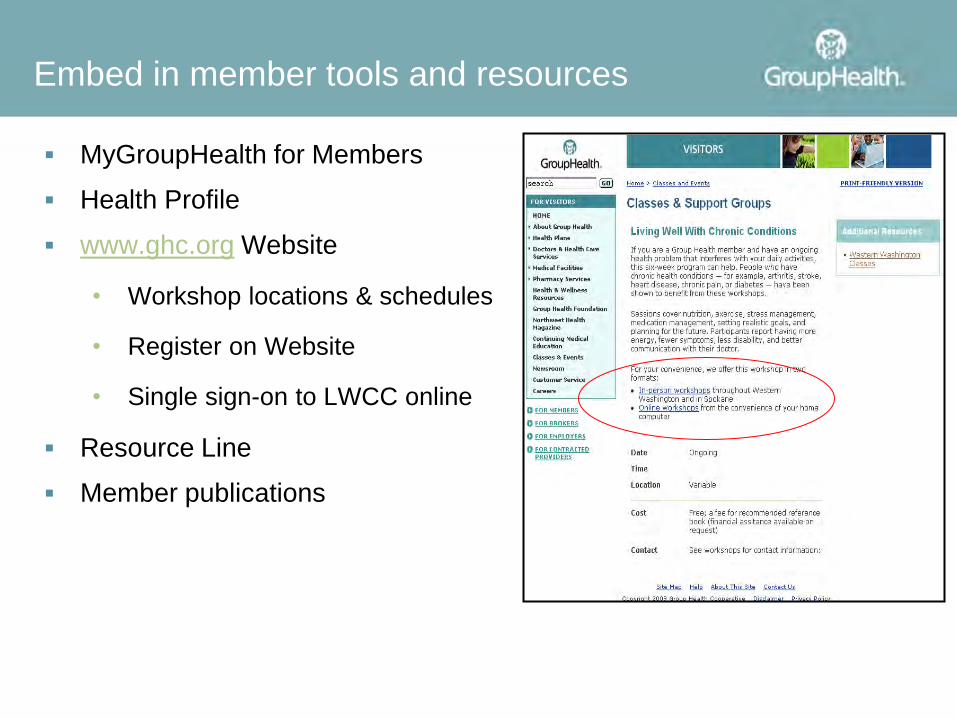
Embed in member tools and resources
MyGroupHealth for Members
Health Profile
www.ghc.org Website
• Workshop locations & schedules
• Register on Website
• Single sign-on to LWCC online
Resource Line
Member publications
Lessons learned and
conclusions
Lessons Learned
Getting buy-in
Involve leadership. Share targets, performance, improvement processes and impact with them to keep them engaged.
Clarify how CDSMP supports strategic goals.
Involve employers
Recruitment through clinics
Make referrals easy and systematic
Embed referrals into standard workflow
Use multiple awareness-raising and recruitment strategies
Look beyond the doc- champions in the clinic are often medical assistants, social workers, clinic manager, nutritionist, or nurse
Keep raising awareness in the midst of competing priorities

Lessons Learned
Roles for community partners
Partner with other organizations to expand reach and share resources and expertise
Collaborate on leader recruitment, training, sharing
Share and standardize best practices and tools
Centralize and share workshop schedules
Develop feedback and reporting processes

Current challenges and next steps
Recruiting leaders in underserved areas
Integrating more closely with clinical care
Coordinating with community organizations to expand
reach into our contracted network
Creating opportunities for “SMS light”
35
A nonprofit service and advocacy organization © 2012 National Council on Aging
Q&A
www.ncoa.org


















