Waveform Questions-part3/Critical care Board review
14
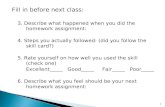
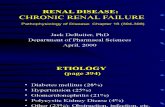
Waveform Tutorial Questions 1. The following pulmonary wedge pressure tracing and simultaneous ECG were obtained in a man with urosepsis, hypotensive and mechanically ventilated on volume assist-control mode with constant flow. What is the approximate wedge pressure? A. -4 mmHg B. 7 mmHg C. 15 mmHg D. 21 mmHg
-
Upload
azmachamberazmacare -
Category
Documents
-
view
15 -
download
0
description
CCM
Transcript of Waveform Questions-part3/Critical care Board review

Waveform Tutorial Questions 1. The following pulmonary wedge pressure tracing and simultaneous ECG were obtained in a man with urosepsis, hypotensive and mechanically ventilated on volume assist-control mode with constant flow. What is the approximate wedge pressure?
A. -4 mmHg B. 7 mmHg C. 15 mmHg D. 21 mmHg
Salma Akram

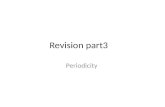
2. The following tracing was obtained from a hypotensive patient with a pulmonary artery catheter. The arrow marks a change in the pressure from the tip of the pulmonary artery catheter. What accounts for the abrupt change in the character of the waveform?
A. The catheter has migrated from the pulmonary artery back into the right ventricle B. The balloon at the tip of the catheter has burst C. The heart has suddenly failed in its ability to pump (acute systolic dysfunction) D. The balloon at the tip of the catheter has wedged
Salma Akram

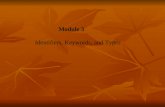
3. A 34 year old with alcoholic pancreatitis is moved to the ICU for worsening respiratory distress and hypotension. He is now intubated, sedated, and mechanically ventilated. The abdomen is diffusely tender, very distended, and firm. The extremities are cool and the capillary refill is poor. There are a few posterior lung crackles but no abnormal cardiac sounds. The ECG is normal and the urine output is < 20 mL in the past two hours. Following 1.5L normal saline a central venous catheter is placed showing a CVP = 20mmHg. An arterial catheter is placed and the following pressure is obtained:
The most appropriate management is: A. Dobutamine for severe LV dysfunction, perhaps due to alcoholic cardiomyopathy B. Norepinephrine for hypotension related to the systemic inflammatory response syndrome (SIRS) C. tPA for possible pulmonary embolus D. Intravenous fluids for hypovolemia
0
90
30
60
Salma Akram
Salma Akram
Pulse pressure variation is > 13%ppmax-ppmin/(ppmax+ppmin/2)

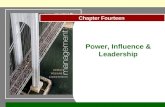
4. A 66 year old man with ischemic cardiomyopathy is admitted with cardiogenic pulmonary edema but does not require mechanical ventilation. He is awake and alert, is moderately dyspneic, has distended neck veins, and is breathing at 24 breaths/min. While inserting a pulmonary artery catheter, you notice that the right atrial pressure is elevated and does not vary with respiration. The Figure denotes the periods of inspiration and expiration. Which one of the following best explains this lack of respiratory variation? A. Right atrial pressure normally has little respiratory variation B. Reduced lung compliance due to pulmonary edema reduces the respiratory impact of respiration on pleural pressure C. The combination of cardiac dysfunction and a well-filled circulation dampens the effect of breathing on the right atrial pressure D. There is probably airflow obstruction contributing to autoPEEP
I E
Pra
Salma Akram

5. A 28 year old woman is intubated for acute respiratory failure. She is sedated, fully ventilated, and passive. The airway pressure and flow waveforms are displayed below, with the pressure in cmH2O, flow in L/s, and time in seconds. The peak value for airway pressure is elevated at 65cmH2O. The dominant contributor to this elevated airway pressure is which one of the following: A. Increased airway resistance as might be seen in asthma B. Increased autoPEEP such as due to premature emphysema C. Excessive tidal volume of greater than 1000cc D. Reduced respiratory system compliance as in lung fibrosis
Salma Akram
Salma Akram
peak-plateau should be less than 15 cwp

6. The flow and pressure waveforms in the Figure below represent which of the following modes of ventilation? A. Pressure-support ventilation B. Volume assist-control ventilation C. Pressure-control ventilation D. Volume synchronized intermittent ventilation
Salma Akram
Salma Akram
patient coughed

7. The flow and pressure waveforms in the Figure below were obtained during mechanical ventilation of a patient with ARDS. The airway pressure and flow waveforms are displayed below, with the pressure in cmH2O, flow in L/s, and time in seconds. Which one of the following sets of tidal volume (VT) and respiratory rate (RR) is closest to the settings in this patient? A. VT 450, RR 15 B. VT 450, RR 21 C. VT 650, RR 15 D. VT 650, RR 21
Salma Akram

8. A patient is ventilated with the pressure-control mode of ventilation. The Figure shows that flow rate (arrow) falls nearly linearly throughout inspiration. Which one of the following is the most important cause for this fall in flow? A. Alveolar pressure rises as the lung inflates B. Airway resistance increases throughout the breath C. The patient is generating expiratory effort D. The ventilator is programmed to decelerate the flow
Salma Akram

9. A 43 year old man is intubated for acute respiratory failure. He is sedated, fully ventilated, and passive. The airway pressure and flow waveforms are displayed below, with the pressure in cmH2O, flow in L/s, and time in seconds. The peak value for airway pressure is elevated at 40cmH2O. Which of the following diagnoses is most compatible with these waveforms? A. Status asthmaticus B. Amyotrophic lateral sclerosis C. Abdominal compartment syndrome D. Pulmonary fibrosis
Salma Akram
Salma Akram

Case 10 What is the respiratory rate in Case 10? A. 28 B. 60 C. 16 D. 10
Salma Akram


Case 11 The patient in case 11 is more tachypneic than the patient in case 10
A. True B. False
Salma Akram
Salma Akram
PSV: arrow effort not rewarded by flow

Case 12
What is the most likely explanation for the tracing in case 12? A. Respiratory distress/Tachypnea B. Autocycling C. Tachycardia D. Ventilatory circuit leak
Salma Akram

13. A 63 year old woman with AML and neutropenic fever presents with acute hypoxemic respiratory failure requiring intubation. Her ideal body weight is 65 kg. Three days into her ICU stay, the bedside nurse calls to notify you that her urine output has been less than 20 mL over each of the last 2 hours. The patient is sedated and passive on the ventilator on an assist/control mode. Her tidal volume is 650 mL. You are given the following waveform tracing:
Which of the following is true?
A. The patient will likely develop acute tubular necrosis
B. The patient should receive a one liter bolus of 0.9 NS
C. From the data presented, it is not possible to know whether the patient will respond to a fluid challenge
D. Her hypotension is more likely to respond to colloid than crystalloid, given the duration of her sepsis
Salma Akram