
Walking ability, balance and accidental falls in …136351/FULLTEXT02.pdf · Örebro Studies in...
94
Walking ability, balance and accidental falls in persons with Multiple Sclerosis
Transcript of Walking ability, balance and accidental falls in …136351/FULLTEXT02.pdf · Örebro Studies in...

Walking ability, balance and accidental fallsin persons with Multiple Sclerosis
Avh_YlvaNilsagard_K131008.indd 1 08-10-14 07.38.47

Avh_YlvaNilsagard_K131008.indd 2 08-10-14 07.38.48

Örebro Studies in Medicine 21
Ylva Nilsagård
Walking ability, balance and accidental falls
in persons with Multiple Sclerosis
Avh_YlvaNilsagard_K131008.indd 3 08-10-14 07.38.48

© Ylva Nilsagård, 2008
Title: Walking ability, balance and accidental fallsin persons with Multiple Sclerosis
Publisher: Örebro University 2008www.publications.oru.se
Editor: Heinz [email protected]
Printer: Intellecta DocuSys, V Frölunda 10/2008
issn 1652-4063isbn 978-91-7668-631-7
Avh_YlvaNilsaga ̊rd_K071008.indd 4Avh_YlvaNilsaga ̊rd_K071008.indd 4 08-10-17 13.48.0808-10-17 13.48.08

Abstract
Ylva Nilsagård (2008): Walking ability, balance and accidental falls in persons with Multiple Sclerosis. Örebro Studies in Medicine, 94 pp.
By using a pragmatic paradigm, different research methodologies were em-ployed in this thesis. MS-related symptoms may be exaggerated due to heat-sensitivity and it is supposed that cooling garments relieve the symptoms. The effects of wearing a Rehband® vest were evaluated in a sample of 42 persons with MS in a randomised controlled crossover study. Both objective and subjec-tive statistically signifi cant improvements were found when a cooled Rehband® vest was worn compared to the wearing of a room-tempered vest.
Using a repeated-measures design, 10m and 30m timed walks and Timed Up and Go were studied in 42 persons with MS. Reproducibility was investigated within and between test points. High reproducibility was found both within (r=0.97–0.98) and between measure points (r=0.91–0.93). The correlation be-tween the three tests was high (r=0.85). Differences at –23% to +40% were es-tablished as being needed to detect genuine changes. Severity of MS infl uenced the size of the differences, especially for the 30m timed walk test.
The 12-item MS Walking Scale was translated and used in a cross-sectional study. Out of 81 persons with MS, 89–96% perceived limitations in standing or walking. The internal consistency of the scale was acceptable for nine items (0.69–0.84). The concurrent validity between the 12-item MS Walking Scale and the investigated objective tests was low: Berg Balance Scale (r=–0.368**), Four Square Step Test (r=0.338**) and Timed Up and Gocognitive (r=0.319*).
A prevalence of falling was found at 63% in a longitudinal cohort study with prospectively registered falls including 76 persons with MS. The odds of falling were fi ve fold when there was a reported need of using a walking aid indoors and outdoors and by 2.5 to 15.6 times while there was disturbed pro-prioception, depending on severity. The highest sensitivity was found for the Berg Balance Scale (94%) and the highest specifi city was found for the 12-item MS Walking Scale (82%). Positive predictive values at 70–83% were found for the Berg Balance Scale, Timed Up and Gocognitive, the Four Square Step Test and the 12-item MS Walking Scale.
Finally, we explored and described factors that persons with MS perceive as related to accidental falls. A content analysis with a deductive approach was chosen. By conducting interviews, we found previously untargeted factors: divided attention, reduced muscular endurance, fatigue and heat-sensitivity. The content of the interviews also gave support to previously reported risk factors such as changes in gait pattern, walking disability, impaired proprioception and vision, and spasticity.
Key words: multiple sclerosis, cooling garment, gait, walking, balance, reliabi-lity, validity, accidental falls, prediction, ICF
Avh_YlvaNilsagard_K131008.indd 5 08-10-14 07.38.48

Avh_YlvaNilsagard_K131008.indd 6 08-10-14 07.38.48

LIST OF PUBLICATIONS This thesis is based in the following papers, which are referred to in the text by the corresponding Roman numerals:
I. Nilsagård Y, Denison E, Gunnarsson L-G. Evaluation of a single ses-sion with cooling garment for persons with multiple sclerosis – a randomized trial. Disability and Rehabilitation Assistive Technology 2006; 1(4): 225-233.
II. Nilsagård Y, Lundholm C, Gunnarsson L-G, Denison E. Clinical rele-
vance using timed walk tests and ‘timed up and go’ testing in persons with Multiple Sclerosis. Physiotherapy Research International 2007; 12(2): 105-114.
III. Nilsagård Y, Gunnarsson L-G, Denison E. Self-perceived limitations of
gait in persons with multiple sclerosis. Advances in Physiotherapy 2007; 9(3): 136-143.
IV. Nilsagård Y, Lundholm C, Denison E, Gunnarsson L-G. Predicting
accidental falls in persons with Multiple Sclerosis – a longitudinal study. Accepted 25 May 2008, Clinical Rehabilitation.
V. Nilsagård Y, Dension E, Gunnarsson L-G, Boström K. Factors per-
ceived as related to accidental falls in persons with Multiple Sclerosis. Accepted 2 October 2008, Disability and Rehabilitation.
Avh_YlvaNilsagard_K131008.indd 7 08-10-14 07.38.48

Avh_YlvaNilsagard_K131008.indd 8 08-10-14 07.38.50

LIST OF ABBREVATIONS MS Multiple Sclerosis PwMS Persons with Multiple Sclerosis EDSS Expanded Disability Status Scale ICF International Classification of Functioning, Disability and Health CNS Central Nervous System
Avh_YlvaNilsagard_K131008.indd 9 08-10-14 07.38.50

Avh_YlvaNilsagard_K131008.indd 10 08-10-14 07.38.50

Contents
1. INTRODUCTION ..................................................................... 15
1.1 Multiple Sclerosis ................................................................... 15
1.2 Expanded Disability Status Scale ............................................16
1.3.1 The International Classifi cation of Function, Disability and Health ..............................................................16
1.3.2 Structure of the ICF components, Figure A .............................17
1.4.1 Impairments ............................................................................17
1.4.2 Symptoms according to ICF core sets, Table 1 ........................19
1.5 Gait and walking ability ..........................................................19
1.6 Balance ....................................................................................20
1.7 Accidental falls ........................................................................20
1.8 Measurement of walking ability and balance ..........................21
1.9 Rehabilitation ........................................................................ 22
1.10 Physiotherapy .........................................................................22
1.11 Formulation of clinically based problems .............................. 23
2. PURPOSE ............................................................................. 25
3. MATERIAL AND METHODS .................................................27
3.1.1 Sampling .................................................................................27
3.1.2 Inclusion criteria ..................................................................... 27
3.1.3 Characteristics of the participating persons, Table 2 ...............28
3.2 Measures ................................................................................28
3.2.1 Measures at the level of Body Function and Structure .............28
3.2.1.1 Fatigue Severity Scale ..............................................................28
3.2.1.2 Modifi ed Ashworth Scale ........................................................28
3.2.1.3 Lindmark Motor Capacity Assessment, part E ........................29
3.2.1.4 Clock Drawing Test .................................................................29
3.3.1 Measures at the level of Activity and Participation ..................29
3.3.1.1 10m timed walk .......................................................................29
3.3.1.2 30m timed walk .......................................................................30
3.3.1.3 Berg Balance Scale ...................................................................30
Avh_YlvaNilsagard_K131008.indd 11 08-10-14 07.38.50

3.3.1.4 Timed Up and Go ....................................................................30
3.3.1.5 Timed Up and Gocognitive ......................................................31
3.3.1.6 Nine-Hole Peg Test ..................................................................31
3.3.1.7 Four Square Step Test ............................................................. 31
3.3.1.8 12-item MS Walking Scale .......................................................31
3.3.1.9 Static and dynamic static standing tests...................................32
3.3.1.10 Frenchay Activity Index ...........................................................32
3.4 Measures, Table 3 ....................................................................33
4. DESIGN, PROCEDURE, DATA ANALYSES ........................ 35
4.1.1 Study I .................................................................................... 35
4.2.1 Study II ...................................................................................36
4.2.2 Figure B ...................................................................................37
4.2.3 Figure C ...................................................................................37
4.3 Study III...................................................................................37
4.4.1 Study IV ..................................................................................38
4.4.2 Figure D...................................................................................41
4.5 Study V ....................................................................................42
4.6 Ethical considerations ..............................................................43
5.0 RESULTS ................................................................................ 45
5.1.1 Results, Study I ........................................................................ 45
5.1.2 Table 4 ..................................................................................... 45
5.1.3 Table 5 .....................................................................................46
5.1.4 Clinical message, Study I .........................................................47
5.2.1 Results, Study II.......................................................................47
5.2.2 Table 6 .....................................................................................47
5.2.3 Table 7 .....................................................................................47
5.2.4 Table 8 .....................................................................................47
5.2.5 Table 9 .....................................................................................48
5.2.6 Clinical message, Study II ........................................................48
5.3.1 Results, Study III .....................................................................49
5.3.2 Table 10 ...................................................................................49
5.3.3 Clinical message, Study III ......................................................50
Avh_YlvaNilsagard_K131008.indd 12 08-10-14 07.38.50

5.4.1 Results, Study IV .....................................................................50
5.4.2 Table 11 ...................................................................................50
5.4.3 Figure E ...................................................................................51
5.4.4 Table 12 ...................................................................................51
5.4.5 Table 13 ...................................................................................53
5.4.6 Table 14 ...................................................................................54
5.4.7 Figure F ................................................................................... 55
5.4.8 Figure G................................................................................... 55
5.4.9 Figure H .................................................................................. 55
5.4.10 Figure I .................................................................................... 55
5.4.11 Figure J ....................................................................................56
5.4.12 Table 15 ...................................................................................56
5.4.13 Clinical message, Study IV ......................................................57
5.5.1 Results, Study V ......................................................................57
5.5.2 Quotes .....................................................................................57
5.5.3 Figure K ...................................................................................59
5.5.4 Clinical message, Study V ........................................................60
6. DISCUSSION ..........................................................................61
6.1 Results summary .....................................................................61
6.2 Results discussion ....................................................................61
6.3 Methodological discussion ......................................................63
6.4 Future research ........................................................................67
7. CONCLUSIONS ......................................................................69
8. IMPLICATIONS ......................................................................71
9. ACKNOWLEDGEMENTS ........................................................73
10. APPENDIX ..............................................................................77
Appendix 1 EDSS ....................................................................77
Appendix 2 Berg Balance Scale .............................................. 78
Appendix 3 Timed Up and Gocognitive ................................ 79
Appendix 4 Four Square Step Test ......................................... 79
Appendix 5 12-item MS Walking Scale ...................................79
11. REFERENCES ....................................................................... 81
Avh_YlvaNilsagard_K131008.indd 13 08-10-14 07.38.50

Avh_YlvaNilsagard_K131008.indd 14 08-10-14 07.38.50
15
1. INTRODUCTION 1.1 Multiple Sclerosis Multiple Sclerosis (MS) is an autoimmune chronic disease affecting the Central Nervous System (CNS). The name originates from the multiple scars or scleroses caused by inflammatory processes in the CNS. These processes damage the mye-lin sheets and lead to disrupted or disturbed transmission of the nerve signals. In combination with the destruction of neurons, this results in loss of function.82 The myelin damage may be fully or partially restored by a remyelination process.82 MS is considered to be a primarily white matter disease but even early in the dis-ease there is involvement of grey matter20 and may later dominate the pathologi-cal progress.52
The cause of the disease development is not quite established but it is regarded to be a possible combination of hereditary, environmental, geographical and viral causes. Sweden is one of the countries with the highest incidence (5.2/100.000)147 of PwMS. A prevalence between 96/100.000152 and 154/100.000147 has been reported in Sweden, although clusters with even higher prevalence have been found.21 It is estimated that around 13.000 persons are di-agnosed with MS in Sweden150. Diagnosis is established by the Poser criteria, which requires that two separate episodes in time and location be found in the clinical examination and be verified by cerebrospinal fluid analysis or magnetic resonance imaging.120 The McDonald criteria makes it possible to diagnose MS after one episode compatible with a MS-relapse, if verified in clinical examination and supported by magnetic resonance imaging alone or in combination with cerebrospinal fluid analysis.93
The relapsing remitting form of MS, at onset, is the most common where symptoms occur for a period of time and then fully or partially regress. In time, however, the progression of the disease continues and the initially relapsing-remitting form develops into a secondary progressive phase with ongoing loss of function. A median time between 11 and 19 years to reach a secondary progres-sive phase from onset of MS has been reported.175 Around 15% are diagnosed as having a primary progressive form of MS without exacerbations.29
The individual course of MS is difficult to predict but is suggested to relate to age at onset and time for occurrence of a progressive phase.175, 176 Sever-ity of MS is commonly graded using the Expanded Disability Status Scale (EDSS)80 (Appendix 1). The median time to reach limitations corresponding to EDSS 4.0 has been estimated as eight years176 and to reach EDSS 6.0, between 20176 and 28 years.158 The median age of reaching disability scores of EDSS 4.0, 6.0 and 7.0 have been reported to be 44, 55 and 63 years, respectively.32 A benign course of MS is defined as having an EDSS score at 2-3 after 10 years of dis-ease.117, 124 Being a young woman without motor symptoms at presentation indi-cates a more benign course.33
The age of debut is commonly between 20 and 40 years with a peak reported as early as 26 to 28150 up to 30 years.29 MS, consequently, strikes in the midst of life affecting major life areas such as work and family. At least two-thirds of those affected are women.89
Around 3.500 PwMS in Sweden are treated with disease modifying treatment.150 These treatments reduce the frequency of exacerbation and are, sub-
Avh_YlvaNilsagard_K131008.indd 15 08-10-14 07.38.50

16
sequently, aimed at PwMS having relapsing-remitting MS or exacerbations within a progressive phase. However, a wide range of symptomatic treatments offers an opportunity to reduce symptoms due to MS and is available regardless of MS form. Despite promising medical development, rehabilitation interventions are still of great importance in MS care, especially since adverse effects are rare. The multiplicity of symptoms, and the impact they have on daily functioning, strongly emphasise a multidisciplinary teamwork. Both those with MS and their signifi-cant others should attract attention in MS care. 1.2. Expanded Disability Status Scale EDSS was developed to measure disability in PwMS80 and is administered by neu-rologists (Appendix 1). Changes in EDSS can be used to support clinical decisions and are frequently reported in scientific papers. The scale ranges from 0 to 10 in steps of 0.5 (except between 0 and 1). For ratings of 4.0 or lower, EDSS is based on scores from eight functional systems: pyramidal, cerebellar, brainstem, sen-sory, bowel and bladder, visual, and cerebral (mental) function. Scores above 4.0 are highly dependent on the person's ambulation status, which is a major criti-cism of the scale. It is the distance a person can actually walk (capacity) that should be rated and used. Difficulties for PwMS in correctly estimating their maximum walking distance can impact the EDSS score.36, 127 MS is graded as be-ing mild at EDSS 1.0-3.5, moderate at 4.0-5.5, severe at 6.0-9.5,149 and EDSS 10 equals death due to MS.80 1.3.1 The International Classification of Functioning, Disability and Health The comprehensive aim of ICF is to offer a standardised language and structure to describe health and health related conditions that can be used for research purposes as well as a clinical tool.173 Information is organised in two parts with each part having two components (Figure A). An attempt was made during the process of conducting this thesis to relate the performed studies to ICF. The measures used in the studies are mainly at the level of Body Function or Activity, but data was also collected at the level of Participation and for Contextual fac-tors. ICF was used as a tool when categorising the open answers given in the study-specific questionnaire where activities performed during falls were de-scribed in Study IV. ICF was used as a conceptual framework when constructing the interview guide and when coding and categorising the units of meaning as well as for presentation of the results in Study V.
Avh_YlvaNilsagard_K131008.indd 16 08-10-14 07.38.50

17
1.3.2 Figure A Structure of the components of the International Classification of Functioning, Disability and Health. 1.4.1 Impairments Depending on the site of the lesions, different symptoms occur when having MS. The symptoms vary in presence and extent between different individuals and dur-ing different time periods. Some of the symptoms are presented below. Fatigue - defined as ‘an overwhelming sense of tiredness, lack of energy and feeling of exhaustion’132 - is one of the most disabling symptoms and, in fact, the most disabling symptom in 10% to 20% of PwMS.53, 57, 79 It is commonly present in MS-populations53, 57, 72, 81, 96 and covers both physiological and psychological as-pects.178 Several possible underlying mechanisms are enlightened in a review178 such as enhanced central motor drive, impaired inhibitory circuits in the primary motor cortex, relation to the amount of diffuse axonal damage and brain atro-phy. Fatigue may be experienced both at rest and after activities and exercise. It varies over time and is predicted by depressive symptoms,83, 177 weak or moderate sense of coherence, living with a partner,177 and heat-sensitivity.83 Fatigue exagger-ates other MS symptoms and becomes more explicit at warmer environmental temperatures.53, 57, 78 Cognitive dysfunction is present in approximately 45% to 60%38 and may also be present in newly diagnosed PwMS73. The dysfunctions involve memory (re-trieval from long-term storage and working memory), speed of information proc-essing, holding and manipulating information in mind, and disability to plan, solve problems and self-monitoring.73, 129 In a longitudinal cohort study including 81 persons with newly diagnosed MS, the most affected cognitive ability was
IICF
Part 1: Functioning
and Disability
Part 2: Contextual
factors
Components of Body Function and Structure
Components of Activities and Participation
Components of Environmental
factors
Components of Personal factors
Facilitators and Barriers
Performance
Capacity
Changes in Body Function
or Structure
Avh_YlvaNilsagard_K131008.indd 17 08-10-14 07.38.50

18
noted for visual organisation.73 Cognitive dysfunction may affect work, social activities and activities in daily life.73, 129 By using screening instruments, it is possi-ble to detect cognitive dysfunction at an early stage. If dysfunctions are suspected, a neuro-psychologist may establish a neuropsychological profile to be used when planning further interventions. Spasticity is defined as ‘an inappropriate increase in velocity-dependent tonic stretch reflexes’ and is part of the upper motor neuron syndrome.91 Affecting mainly the lower limbs, it may disturb activity, positioning and resting. It is a common feature in PwMS with over 84% reporting spasticity in a cross-sectional survey128 including data for 20.380 individuals. The primarily goal with treating spasticity is to improve function or to ease care. Preferably, this can be achieved by combining patient education, physiotherapy and medication.119 Approximately half a sample of PwMS using either intrathecal baclofen treatment (n=198) or oral drugs (n=315) to treat spasticity, reported that they combine medication with physical therapy or stretching to alleviate their spasticity.128 Limb weakness is usually asymmetrically manifested in the lower extremities, al-though weakness may also appear in the upper extremities.91 Weakness was re-ported as the most frequently occurring symptom, with a reported prevalence at 80% and being present at any time by 89%.153 Evidently, impaired strength nega-tively affects movements and transfers. Proprioception and sensory touch are sensory qualities commonly impaired in PwMS, often present at onset of the disease.91 Proprioception is the ability to sense the body and the parts of the body’s mutual position and relation to each other. Sensory touch is the ability to recognise surfaces and their structure and quality, and to feel light touch. Pain is frequently listed as one of the initial symptoms reported at disease onset.91,
111 It can be divided into primary pain associated with MS lesions and secondary pain that results from disability instead of the disease process. A point prevalence at nearly 50% was reported in a systematic review.111 Within one month of as-sessment, approximately 75% reported having had pain. Risk factors reported to increase the likelihood of pain are older age, longer disease duration, and higher EDSS.89, 111 Heat-sensitivity is recognised in approximately 60-80% of PwMS61, 116, 154 and heat may aggravate several symptoms,91 possibly explained by the increased sensi-tivity to heating in demyelinated axons. For example, fatigue,53, 57, 79 muscle weak-ness and visual impairment,92 may increase in warm environments. Exposure to high temperatures was perceived as a negative extrinsic factor in a survey with 2.529 PwMS.142 Different techniques to provide cooling are used in physiotherapy and these can often be taught as self-care management. Local cooling, cold baths, cryo cuffs and cooling garments exemplify some of those techniques. Reduced symptoms due to different cooling therapies have been reported in PwMS for ataxia,1 tremor,48 fatigue,10, 22, 54, 169 walking,54, 95, 134, 169 strength,10, 22, 95 balance,10 and spasticity.54
Avh_YlvaNilsagard_K131008.indd 18 08-10-14 07.38.51

19
The above-mentioned symptoms are presented in Table 1 according to the com-prehensive ICF core set75 to illustrate the level at which they are classified. 1.4.2 Table 1 Classification of symptoms according to the comprehensive ICF core sets for MS. Symptom ICF code ICF category title Fatigue Energy and drive functions B130 Cognitive dysfunction Higher level cognitive functions
Attention functions Visuospatial perception
B164 B140 B1565
Spasticity Muscle tone B735 Limb weakness Muscle power functions B730 Proprioception Proprioceptive function B260 Light touch Touch function B265 Pain Sensation of pain B280 Heat-sensitivity Tolerance for heat and cold B5501 Affected gait pattern Gait pattern functions B770 Walking disability Walking D450 Balance Not defined ------- B: Body Function and Structure, D: Activity and Participation 1.5 Gait and walking ability Impaired gait pattern is reported as reduced speed,11, 45, 87, 130, 153, 156 reduced stride length,11, 45, 87 prolonged double limb support11, 87, deviations in muscle recruit-ment11 and gait initiation.125 The changes in gait pattern may result from abnor-mal muscle tone, limb weakness, incoordination, or disturbed proprioception. Reduced strength in hamstrings and in m. quadriceps correlates with reduced gait velocity at both comfortable and maximum speed.156 Physiotherapists analyse the gait pattern of patients in order to define the specific problem areas that need fur-ther investigation before designing and carrying out proper interventions.
Walking with a disrupted gait pattern demands more energy166 that may induce muscular fatigue or cause further increase in muscular tone. Ankle foot orthoses can be prescribed to assist dorsiflexion of the foot in order to facili-tate gait pattern. The use of these orthoses does not, however, seem to affect gait speed26, 136 but instead diminishes the self-perceived limitations in walking.123 Or-thoses assisting hip flexion seem promising since they have been reported to im-prove gait performance evaluated with a timed 25-foot walk, Timed Up and Go, and a 6-minute walk test.148 Some situations require certain levels of gait speed such as, for example, when safely crossing a street. In Stockholm, a speed at 1.2m/s is required for crossing a signalised intersection before the red light comes on, but the corresponding standard in Europe is 1.4m/s.151
Limitations in walking ability are well recognised in PwMS45, 70, 72, 91, 96 and are also present in the early course of the disease11, 87. This is reported to be the most important disability in persons with benign or moderate MS.66 Examples of limitations in walking ability are reduced walking distance, walking on a slope or uneven surface, and walking in crowds or in traffic.
Avh_YlvaNilsagard_K131008.indd 19 08-10-14 07.38.52

20
Walking disability may restrict activities in daily living,44 participa-tion in social activities44, 50 and work,50 while maintained mobility facilitates per-forming activities in daily living and socialising with family and friends.50 Experi-encing difficulties with walking, as rated using the 12-item MS Walking Scale, is also related to lower levels of physical activity.99 Environmental factors such as having shops and transit stops within walking distance and accessibility to free or low-cost facilities influence the actual distance walked positively.41
1.6 Balance Balance is a complex motor skill requiring central processing of vestibular, visual and somatosensory information in order to activate the musculoskeletal system to produce coordinated eye movements, posture, stance and locomotion. The con-cept of balance has been described to cover four subdivisions of motor skills in-corporating postural control 1) on a stationary basis, 2) in voluntary movements, 3) in involuntary movements, and 4) in external perturbations.122 All of these subdivisions may be negatively affected in PwMS143 and should consequently be recognised and targeted in physiotherapeutic interventions aiming to restore bal-ance function. Different approaches have been evaluated in experimental clinical trials with reported positive effects.25, 64, 141 Balance function per se is not catego-rised in ICF but is, instead, incorporated in different activities.173
Balance is often negatively affected in PwMS55, 58, 87, 96, 114, 143 and limi-tations may be present even in the absence of clinical disability.87 Problem with balance has been reported as the most common symptom alongside walking dis-ability, followed by fatigue and bladder dysfunction.70 Forty-eight out of 58 (83%) PwMS stated that they experienced balance problem and 40 of those re-ported the problems as being constant. Another study55 reported that 82.5% of those with a progressive course of MS stated balance problems compared to 73.4% in the relapsing-remitting subgroup. Persons with a progressive form of MS seem to perform somewhat worse in balance performance tests compared to those with a relapsing-remitting form.143
The above-mentioned symptoms are presented in Table 1. 1.7 Accidental falls An accidental fall may be defined as ‘an unexpected contact with any part of the body on the ground’.157 The scientific base of knowledge concerning accidental falls in PwMS is accumulating,23, 51, 114, 145 but considering the impact falls may have in everyday life, the body of research is still rather small. PwMS are exposed to the risk of falling due to both their MS-specific symptoms and their limitations in performing activities. Attention should be paid to both individual and envi-ronmental variables, and a multidisciplinary approach is preferable. A thorough evaluation of factors disposed to falls should be undertaken to guide the interven-tions.
The reported prevalence of falls is considerable and varies between 31%145 and 57%.43 Several symptoms have been reported to be associated with falls; for example, limitation in walking and balance captured by the Equiscale,23 the need to use an assistive device when walking,23 cognitive dysfunction,51 and urinary incontinence.51 Experiencing accidental falls may result in fear of falling, which in itself can lead to activity curtailment.114
Avh_YlvaNilsagard_K131008.indd 20 08-10-14 07.38.52

21
To our knowledge, mainly data of retrospectively registered falls has, thus far, been investigated and published regarding PwMS. The participants have been asked to recall falls within different time frames: one month,27 two months,23 three months,43 six months,51 and up to one year.145 The studies most commonly rely on self-reported data, which methodologically induce a lack of control and possible presence of cognitive dysfunction must be considered.
1.8 Measurement of walking ability and balance There are many aspects to consider when choosing relevant measures. Obviously, it is vital that the measure reflects the impairments, activity limitations or partici-pation restrictions that are of interest. Effects of interventions directed at the level of Body Function and Structure may also be experienced at the level of Activity or Participation.
First of all, a measure must be reliable, and there are different types of reliability. Reproducibility describes the agreement between different observers (interrater reliability) or between observations made by one person (intrarater reliability) or by test results from separate test occasions on a patient or sample (test-retest reliability). Internal consistency is used to ensure that a measure includ-ing several items actually addresses the same underlying concept.
Secondly, a measure must be valid. Content validity determines whether the measure covers relevant or important content. Criterion validity is the correlation of a scale or a measure with a ‘gold standard’ and contains concurrent and predictive validity. When developing a measure that covers variables not di-rectly observable, the underlying theory of that specific construct can be used (construct validity). Validity can describe how closely a measure is related to an-other measure of the same construct (convergent validity) or how it is not related with a measure of a disparate construct (discriminant validity).146
The functional level of the targeted individual or sample must be taken into consideration to avoid floor and ceiling effects. When evaluating ex-pected change either originating from disease progression or regression or from effects of given interventions, measures’ responsiveness is important. Preferably, a measure should be quick and easy to administer and transferable into different environments. This facilitates repeated measurement enabling the observer to fol-low the course of disease or recovery irrespective of costly equipment or premises.
When evaluating gait pattern, thorough gait analysis requests expen-sive equipment and laboratory facilities and is often not feasible to use in clinical practice. Thus, the evaluation is often performed in the clinical situation using descriptive terms. Likewise, postural control can be quantified in laboratory con-ditions using a technological device even at the Body Function and Structure level. In clinical practice, other measures targeting Activity and Participation are often preferred. A simple way to evaluate walking ability is to measure the time to walk a certain distance at either self-selected comfortable speed or at forced speed. Walking distance and effort when walking can be evaluated using standardised tests such as the 2, 6 and 12 minute walks.19 Inexpensive and simple devices such as pedometers may be used to quantify distance covered and steps taken. Other measures reflect the subjective experiences of a certain limitation such as the 12-item MS Walking Scale that measures perceived limitations within a variety of as-pects in walking and balance demanding tasks66.
Avh_YlvaNilsagard_K131008.indd 21 08-10-14 07.38.52

22
Some measures are closely related to walking but incorporate differ-ent balance demanding tasks or basic mobility while walking. Timed Up and Go118 includes the task of rising up from a chair, walking 3m, turning, walking back and sitting down again, thus including balance performance as well as gait speed. Adding either a cognitive or a manual task sharpens the test.86, 139 Another measure is the Dynamic Gait Index that includes walking at different speeds, with head movements, walking around and over objects or climbing stairs.140 The Four Square Step Test, developed recently, requires a person to quickly step over ob-stacles in four directions.40 Measuring refined balance tasks is possible with, for example, the commonly used Berg Balance Scale.12 Evidently, accidental falls can be used to measure balance since falling is the outermost consequence of poor balance.
1.9 Rehabilitation Rehabilitation is described by the World Health Organization as a process that enables the individual to identify problems and to reach his or her optimal ability aiming to facilitate independence and social integration.174 In order to manage this, coordinated interventions supplied through a multidisciplinary approach are emphasised. The person receiving rehabilitation should take an active part in this goal-targeted and time limited process.144 This is especially important since the concordance in goal setting may differ between the PwMS and the rehabilitation team.16 The benefits of multidisciplinary rehabilitation for PwMS have been sum-marised in a systematic review.76 The evidence is considered strong with regard to inpatient rehabilitation resulting in achievements at the level of activity and par-ticipation according to the ICF. There is also strong evidence that low intensity rehabilitation conducted over a longer period of time positively affects quality of life. Although limited evidence, improvements in participation and quality of life are reported for outpatient and home-based rehabilitation. It is recommended that PwMS should undergo regular specialist evaluation to assess their needs for appropriate rehabilitation.76 Rehabilitation can also be used in conjunction with medical treatment related to exacerbations. Administrating steroids in combina-tion with multidisciplinary rehabilitation is superior in comparison with the ad-ministering of steroids in a standard neurology or day ward setting.35 1.10 Physiotherapy Limitations in walking and balance are often a cause for referral to a physiothera-pist for evaluation and intervention. Human movement throughout the lifespan is central in physiotherapy. Physiotherapists tailor interventions in order to reduce symptoms, improve or maintain function, develop strategies to manage symp-toms, supply suitable assistive technology, promote overall health, educate and inform both individuals and their significant others, and to assist the person to achieve the highest possible level of independence.144, 167 Therapeutic exercise in physiotherapy, regardless of diagnosis, is beneficial and adverse events are rare. The exercise programmes should, preferably, be individualised and targeted.155 There is strong evidence that exercise therapy can improve muscle power function, exercise tolerance functions and mobility-related activities. The evidence is moder-ate for improvements in mood and upper extremity function with exercise ther-apy compared to no exercise therapy for PwMS.126
k l d d h ff h
Avh_YlvaNilsagard_K131008.indd 22 08-10-14 07.38.53

Increasing knowledge exists regarding the positive effects that exer-
cise may have on the CNS. Exercise may enhance neurobiological processes that promote brain health in ageing and disease. Regular physical activity may mediate favourable changes in disease factors as well as in symptoms associated with MS. Several favourable mechanisms induced by exercise resulting in promotion of neuroprotection and neuroplasticity has been described.170
It is important to promote activity among PwMS since they may be less physically active than other nondiseased adults100 and since their symptoms may worsen due to low levels of physical activity.99 General recommendations for levels of physical activity have been described for PwMS.46, 113 There are a wide range of possibilities to participate in exercise despite having MS. Coaching a per-son to find accurate exercise and optimal dosage lies within the area of expertise of physiotherapists. Those with stronger self-efficacy in relation to exercise seem to show greater adherence to an exercise program.90 This challenges physiothera-pists to positively influence the persons’ beliefs in their capability to successfully carry out prescribed exercise programs. Considering the chronic course of MS, self-care management is essential; for example, PwMS need to be educated in how to economise with their energy and how to reduce negative symptoms themselves. 1.11 Formulation of clinically based problems Clinical problems were formulated that were based on the common presence of walking and balance disabilities in PwMS combined with the physiotherapists’ role in relation to these disabilities. New cooling garments had been marketed and it was felt important to evaluate whether they could be a useful self-administered intervention for PwMS to counteract the worsening of symptoms due to heat-sensitivity. The effects of a single intervention were evaluated since it was of inter-est whether it was possible to intervene instantly if exaggerated symptoms were experienced due to heat sensitivity.
Valid and reliable measures are needed to evaluate the natural course of events due to MS as well as the effects of interventions. Reliability needs to be established for each population of interest. As a clinically working physiothera-pist, questions arose regarding what measures to use and what the most suitable way to administer them were. When using measures, it is necessary to know how to interpret the gained results in terms of establishing genuine changes. To enable the use of already existing self-rating scales, these need to be translated into Swed-ish and validated.
Based on our clinical experience, accidental falls and near fall inci-dents are rather common among PwMS. Besides surveying the frequency of acci-dental falls and near fall incidents, we were interested in finding variables or measures easily collected in clinical practice that could predict falling. With predic-tive knowledge, those at risk of falling can be identified and proper measures can be taken. However, in order to tailor the interventions properly, deepened knowl-edge about which factors cause accidental falls was sought. Consequently, it be-came apparent that more knowledge would be gained directly from those who experienced falls by conducting interviews.
23

Avh_YlvaNilsagard_K131008.indd 24 08-10-14 07.38.53
25
2. PURPOSE
The comprehensive aim of this thesis was to gain more knowledge about walking ability, balance, and accidental falls in PwMS. The specific aims were to: Study I … evaluate whether primarily gait and balance were improved if
wearing a cooled Rehband® vest during a single session in compari-son with a single session with placebo treatment.
Study II … clarify the reproducibility, the smallest percentage difference
needed to be able to detect a genuine change, and the correlation re-garding the 10m and 30m timed walks and the Timed Up and Go.
Study III … describe the self-perceived walking limitations experienced by
PwMS using the Swedish translation of the 12-item MS Walking Scale and to investigate it for internal consistency and concurrent va-lidity.
Study IV … describe the frequency of falls and near fall incidents and circum-
stances of falls, investigate predictive values regarding falls for four tests and clinical variables and calculate the correlations between ret-rospective reported falls and prospectively recorded falls.
Study V … explore and describe what factors PwMS perceived as being re-
lated to accidental falls using the ICF.
Avh_YlvaNilsagard_K131008.indd 25 08-10-14 07.38.54

Avh_YlvaNilsagard_K131008.indd 26 08-10-14 07.38.54

27
3. MATERIALS AND METHODS 3.1.1 Sampling In Örebro County, adult PwMS with, roughly speaking, a remained ability to walk are cared for at the University Hospital by a team specialised in MS. The studies were directed at those within similar severity of MS as those cared for by the MS-team. Cooperation was sought with other centres caring for PwMS to ensure samples large enough for the planned studies.
Commonly, neurologists rate EDSS when performing a clinical ex-amination. The score is documented in the medical record and may be registered in the Swedish MS Registry.150 Different approaches were used when identifying eligible persons for inclusion. At the University Hospital in Örebro (Study I-IV) and the Primary Health Care district of West Östergötland County (Study III-IV), the Swedish MS Registry was used.149 At Mälar Hospital in Eskilstuna (Study I-IV), Sahlgrenska University Hospital (Study III-IV), and the Primary Health Care districts of East Östergötland County (Study III-IV), local registries, personal knowledge, and medical records were used. However, when conducting Study III-IV, EDSS scores were not available at one participating centre. This led to com-plementary assessments for six PwMS being performed for the express purpose of these studies by a neurologist from the University Hospital in Örebro (L-GG) Of those registered in the Swedish MS Registry for the year 2005-2006, EDSS was reported for 90% in Örebro County, and for 65% in Östergötland County.149 3.1.2 Inclusion criteria Purposeful samples were strived for and limits of severity of MS were based upon clinical reasoning. In order to be able to include a 30m timed walk test (which was repeated three times on each test occasion), the upper limit was set at EDSS 6.0 in Study I to II. The lower limit in Study I to II was set at EDSS 3.0 where some limi-tation of walking capacity is often present. For Study III to IV we decided to keep the upper limit but chose EDSS 3.5 as the lower limit based upon discussions on how to achieve a representative sample including both fallers and non-fallers. All persons had to be diagnosed as having MS. Specific criteria are described below for each study. Characteristics for each sample are presented in Table 2. Study I-II: Registered EDSS between 3.0 and 6.0 was required together with self-reported heat-sensitivity. Ongoing exacerbation of MS and factors preventing persons from walking 100m, such as heart or lung disease, were considered as exclusion criteria. Study III: A registered EDSS between 3.5 and 6.0 was an initial inclusion criterion, although data from three PwMS with an EDSS within 0.5 points outside these limits were allowed in the analyses. The ability to walk a minimum of 10m with bilateral support was required (excluding rollators). Exclusion criteria were those with ongoing exacerbation of MS, other physical illness preventing them from walking, or an inability to fill in the 12-item MS Walking Scale.
Avh_YlvaNilsagard_K131008.indd 27 08-10-14 07.38.54

28
Study IV: A registered EDSS between 3.5 and 6.0 was an absolute criterion and an ability to walk a minimum of 10m with bilateral support was required (excluding rollators). Exclusion criteria were major difficulties in understanding instructions or filling in the questionnaires and evident hearing or visual loss and ongoing ex-acerbation of MS. Study V: The persons were purposefully selected according to reported history of accidental falls registered in Study IV. Only an extended difficulty in understand-ing and speaking Swedish were chosen as exclusion criteria. 3.1.3 Table 2 Characteristics of the participants for the respective study. Study I-II
(n=43) Study III (n=81)
Study IV (n=76)
Study V (n=12)
Age (mean, sd) 52 (±9) 50 (±11) 50 (±10) 55(±11) Male/ female 13/30 20/61 19/57 1/11 EDSS (median) 4.0 4.5 4.5 5.5 EDSS 1-3.5 (frequency) 15 22 21 1 EDSS 4-5.5 (frequency) 18 36 35 6 EDSS 6 (frequency) 10 23 20 5 RRMS/SPMS/PPMS 22/13/8 45/27/9 40/27/9 3/9/0 RRMS: Relapsing-remitting MS; SPMS: Secondary Progressive MS; PPMS: Primary Pro-gressive MS. 3.2 Measures Measures and variables used in the studies are summarised in Table 3. A study specific questionnaire targeting Body Function and Activity and Participation was constructed for Study I. For Study II, a form was developed where near fall inci-dents, accidental falls and circumstances when falling were registered daily. Ques-tionnaires for relevant data were designed for the respective study. In addition, the measures that follow below were used. 3.2.1 Measures at the level of Body Function and Structure 3.2.1.1 Fatigue Severity Scale is a questionnaire that measures the consequences of fatigue containing nine statements (1-7 points). A score is calculated by adding all statements (9-63 points) and dividing the sum by nine.79 The person is asked to rate his or her fatigue, defined as ‘a sense of tiredness, lack of energy and total body give-out’132 Internal consistency is reported at α=0.81, test-retest reliability at r=0.8479 and the scale discriminates between PwMS and healthy controls.28 Fa-tigue Severity Scale correlates with other fatigue scales78 and has been recom-mended for clinical use when evaluating PwMS.28 3.2.1.2 Modified Ashworth Scale is an ordinal scale that allows the investigator to measure spasticity by grading the resistance of the muscles to passive stretching.18 It extends the original Ashworth Scale6 in order to increase the discreteness at the lower end of the scale by a total of six grades.18 Interrater reliability for PwMS has been investigated for muscles in the lower limbs using the Ashworth Scale109 and was found to be good ( 0.70) for the m. soleus, the m. gastrocnemius and the m.
Avh_YlvaNilsagard_K131008.indd 28 08-10-14 07.38.54

29
psoas, and between 0.36 and 0.69 for the m. quadriceps and the knee flexors. The Modified Ashworth Scale has reported an interrater reliability of the elbow flexor muscle with agreement in almost 87% of the ratings18 for persons with le-sions in the CNS. The interrater reliability for the Modified Ashworth Scale has also been investigated in a sample consisting of nine PwMS with two physiothera-pists performing the ratings. Out of 72 tested muscle groups, 55 were graded as having no increase in muscle tone in the lower limbs.112 The percentage of agree-ment was 64% for combined lower limb score but for the respective muscles, it was only significant for the left m. quadriceps. Despite the shortcomings of the scales,5 they are still widely used both in clinical practice and in research.62 Alterna-tive measures such as the patient-based MS Spasticity Scale has recently been de-veloped67 but has not yet been translated into Swedish. 3.2.1.3 Lindmark Motor Capacity Assessment, part E Two sensory qualities were measured in the lower extremities: light touch and proprioception using part E in the modified Motor Assessment Chart according to Lindmark et al.84 The chart was initially developed84 and validated85 to evaluate functional capacity after stroke, but has been used in its entirety or partially for different neurological diagnosis.45, 56, 64 Light touch was tested for the feet and leg and proprioception was measured for the big toes, ankles and knees. The scale is 3-graded (0-2) where 0 equals total loss of function, 1 equals disturbed sensation, and 2 equals normal sensation.85 3.2.1.4 Clock Drawing Test measures global cognitive function by a complex task. It involves a wide range of cognitive functions such as planning, visuospatial abilities, motor programming and execution, abstract thinking, inhibition of the tendency to be pulled by perceptual features of the stimulus and concentration and frustration tolerance.138 A paper with a pre-drawn circle is given to the person being investigated and he or she is asked to put the numbers on the clock and set the time at ‘10 past 11’. Several scoring systems have been used.138 In the present study, severity of impairment was graded between 0 and 5 giving the highest score to an intact clock.138 Deficit in motor performance does not heavily affect the per-formance and the test is considered brief enough not to induce fatigue.8, 129 The Clock Drawing Test is recommended as a screening instrument for early cognitive dysfunction.8, 129 Sensitivity for discriminating PwMS without cognitive dysfunc-tion from those cognitively impaired is reported at 93.4% and the specificity at 85.8%.8 All above measures provide ordinal data. 3.3.1 Measures at the level of Activity and Participation 3.3.1.1 The most common distance chosen both for persons with neurological and other conditions when evaluating gait velocity is 10m.59, 60 The 10m timed walk is considered to be valid, reliable, and sensitive to change161 and has been recommended for measuring disability and evaluating the effect of physiothera-peutic interventions aimed at restoring mobility in PwMS.165 Test-retest variability has been reported for the 10m timed walk in self-selected speed for PwMS.97, 165 The speed increased slightly (1.6m/min) when eight trials were conducted over the
Avh_YlvaNilsagard_K131008.indd 29 08-10-14 07.38.54

30
same day.97 An individual test-retest score for gait speed tested five times on a sin-gle day showed a variability of 20 ±8%.165
Differences in procedure are reported in the scientific literature re-garding using usual or comfortable pace versus fast pace and using a dynamic versus still start. The use of usual pace and a dynamic start is more commonly reported in neurological studies and the pace significantly impacts the mean walk-ing velocity in persons with neurological conditions.60 Using a 10m distance with a static start at comfortable pace has been recommended for standardising the test procedure.59 The 10m timed walk can also be performed with a turn at 5m,164 which can be useful if evaluating persons in their homes. 3.3.1.2 The 30m timed walk at forced speed has been described as a functional test that correlates to force-platform measures in healthy persons.47 The use of a prolonged distance (30m) provides the opportunity to evaluate whether increased effort, due to longer distance and higher speed, affects the reproducibility. There is, to our knowledge, no published reliability study regarding the 30m timed walk for PwMS. 3.3.1.3 The Berg Balance Scale is a performance-based measure intended for indi-viduals with affected balance. It contains 14 items, graded from 0 to 4 points with a maximum of 56.12 High scores indicate better balance. It was based on the premise that balance is the ability to maintain an upright posture under different circumstances. The purpose of the Berg Balance Scale is to monitor functional bal-ance over time and to evaluate persons’ response to treatment and to predict falls. It addresses two dimensions of balance 1) the ability to maintain upright posture, and 2) to make appropriate adjustments for voluntary movement: narrowing the base of support, asking subjects to lean toward the edges of a base of support, and altering sensory input to manipulate degree of difficulty.49 High interrater (r=0.96) and test-retest (r=0.96) reliability has been reported in PwMS.24 A cut-off at <45 points is suggested to increase the relative risk of multiple falling during the following year with 2.7.13 When using the same cut-off in an elderly sample pre-dicting falls during six months, a sensitivity at 53% and a specificity at 92% was found17 and for persons post stroke, it predicted falls with a sensitivity at 65% and a specificity at 65%.4 This cut-off has also been used for PwMS resulting in sensitivity at 40% and specificity at 90%.27 The components of the task are cate-gorised in relation to the components of ICF in Appendix 2. 3.3.1.4 Timed Up and Go was designed to measure balance, mobility, and loco-motor performance, including the risk of falls in elderly people with balance dis-order.118 The Timed Up and Go is a development of the Get Up and Go test88 by adding a time component. Time elapsed is registered from rising from a chair, walking 3m, turning around, walking back, and sitting down. High interrater reliability has been established for persons with Parkinson disease (0.87-0.99),98 elderly medically stable persons attending a Day Geriatric Hospital (0.99)118 and for those with spinal cord injury (0.97).163 The Timed Up and Go test was further developed by adding a manual task86. By calculating the difference between Timed Up and Gomanual and Timed Up and Go, diffTUG is achieved. It is proposed that a diffTUG at 4.5s identify elderly people prone to fall,86 although less encouraging predictive ability is reported by others.4, 139
Avh_YlvaNilsagard_K131008.indd 30 08-10-14 07.38.54

31
3.3.1.5 Timed Up and Gocognitive is a development of Timed Up and Go by the ad-dition of a cognitive task; namely, subtracting 3 from a randomised number be-tween 20 and 100.139 This allows balance to be measured during a multi-task condition that may resemble everyday situations more than a single-task condi-tion does. The additive task of subtracting has also been used when measuring balance function in laboratory conditions and has been useful when classifying older persons with a mildly increased risk of falls from those without.31 Other cognitive tasks also seems valuable when identifying older persons at risk of fal-ling such as reciting alternative letters from the alphabet when walking.168 Our hypothesis was that multi-task conditions are more likely to cause accidental falls than single-task conditions and, for that reason, the Timed Up and Gocognitive was chosen for Study IV. The components of the task are categorised in relation to the components of ICF in Appendix 3. 3.3.1.6 Nine-Hole Peg Test is a performance-based measure of dexterity in the upper extremities161 recommended for PwMS.131 The person tested firstly places pegs in holes in a box and then removes them as fast as possible. After one trial attempt, the test is performed twice for both hands. A score is calculated as the mean value of the four tests. Both intrarater and interrater reliability in a MS-population is reported at 0.98 respectively.130 3.3.1.7 The Four Square Step Test is performance-based and measures the ability to quickly step over obstacles in different directions.40 Four sticks at 2.5cm height are placed on the floor at 90 degrees angles to each other. The person is asked to complete a sequence of stepping into the squares (forwards, sideways, backwards and sideways) first clockwise and then back again without touching the sticks and facing forwards, if possible. Time to complete the sequence is recorded. The Four Square Step Test is based on the knowledge that trips and slips are common rea-sons why older people fall. Interrater reliability has been reported for older people at r=0.9940 and for those with vestibular disorders at r=0.93.171 A cut-off was suggested at 12s to identify persons with vestibular disorders having one or more risk factors for falls with a sensitivity at 80% and specificity at 92%.171 In a sam-ple of community-dwelling adults (>65 years), the optimal cut-off was, instead, suggested to be 15s, giving a sensitivity at 85% and specificity at 88% for identi-fying multiple fallers.40 A correlation has been established between the Four Square Step Test and the Step test (r=-0.83) and the Timed Up and Go (r=0.88) for community-dwelling adults.40 The components of the task are categorised in relation to the components of ICF in Appendix 4. 3.3.1.8 The 12-item MS Walking Scale was developed as a patient-rated measure of walking ability.66 Twelve items were generated from patient interviews, expert opinion, and literature review. The person rates the extent to which his or her ability to walk and perform activities while standing has been affected by MS dur-ing the previous two weeks. Each item is scored on a 1 to 5 scale and a total score is generated (0-100). High scores indicate a greater impact on walking ability. The psychometric qualities are consistently reported as satisfactory.66, 94, 101 Parameters other than gait speed and distance are reflected, such as the need to use support, the need to concentrate when walking, and the ability to stand while doing things. It is considered reliable and valid.66, 94, 101 Although the 12-item MS Walking Scale
Avh_YlvaNilsagard_K131008.indd 31 08-10-14 07.38.55

32
is diagnosis-specific, it remains to have satisfactory psychometric criteria as a problem-specific scale after the removal of all MS-specific details and used upon different neurological conditions.69 The items of the scale are categorised in rela-tion to the components of ICF in Appendix 5. 3.3.1.9 Static and dynamic standing tests. The time for steady stance tests was tested using footprints taped on the floor to standardise positions, as described by Frzovic et al.: feet apart, feet together, stride stance, tandem stance and single leg stance.58 A maximum time of 90s was used since previous research investigat-ing PwMS has reported a ceiling effect using a maximum testing time of 30s for feet apart58, 143 or feet together and stride stance.58 As a test of dynamic standing balance, the Step test was chosen.65 A time limit of 15s and a 17-cm-high step were used. 3.3.1.10 The Frenchay Activity Index was originally developed for persons with stroke68 but was also found feasible for use in MS-populations.43 It is a 15-item questionnaire that mainly covers domestic chores, leisure and work-related activi-ties, and other outdoor activities. The total score ranges from zero (low) to 45 (high) frequency of activities.162 Timed Up and Go, Timed Up and Gocognitive, the Nine-Hole Peg Test, the Four Square Step Test and static and dynamic standing tests supply ratio data. The Berg Balance Scale, the 12-item MS Walking Scale, and Frenchay Activity Index are considered ordinal scales.
Avh_YlvaNilsagard_K131008.indd 32 08-10-14 07.38.55

33
3.4 Table 3 Measures used in the respective study in alphabetical order. Measures Study I Study II Study III Study IV Study V 10m timed walk 12-item MS Walking Scale 30m timed walk Berg Balance Scale Clock Drawing Test EDSS Fatigue Severity Scale Four Square Step Test Frenchay Activiy Index Modified Ashworth Scale Modified Motor Capacity Assessment, part E
Nine-Hole Peg Test One-legged stance Oral temperature Standing feet together Step test Tandem stance Timed Up and Go Timed Up and Gocognitive
Avh_YlvaNilsagard_K131008.indd 33 08-10-14 07.38.55

Avh_YlvaNilsagard_K131008.indd 34 08-10-14 07.38.55

35
4. DESIGN, PROCEDURE, MEASURES AND DATA ANALYSES 4.1.1 Study I Design A randomised crossover trial was conducted using a washout period of seven days (Figure B). Varied block sizes (Örebro: 6-12, Eskilstuna: 4-8) were used as-signing the PwMS to begin with active or placebo treatment. Active treatment consisted of wearing a cooled Rehband® vest while seated for 45min. Placebo treatment consisted of wearing a room tempered Rehband® vest instead while seated for 45min. The allocation was concealed using sealed envelopes. The inves-tigators were blinded to the intervention and an attempt to blind the participants was conducted. The allocation schedule was followed without protocol violation.
A power analysis based upon a 10m timed walk was performed us-ing an 80% power to detect an estimated clinically significant change at 2s be-tween treatments, an estimated standard deviation at 5s, and the correlation be-tween successive measurements at 0.6s. A significance level was set at 0.05. A minimum sample size was set at 42 PwMS. Forty-eight PwMS were included and randomised and 43 completed the intervention (Figure C). Procedure Participating centres were Örebro University Hospital (36 randomised/32 com-pleted) and Mälar Hospital in Eskilstuna (12 randomised/11 completed) (Figure C). The three physiotherapists who collected the data were trained to ensure strict application of the testing procedures, and a manual was available. Four measure points were used for the tests: directly before and after each period of active cool-ing or placebo, respectively. The same physiotherapist administered all tests to a given person. A stopwatch accurate to two decimal places was used in the testing. The persons sat down for at least five minutes before testing started. They were encouraged to wear comfortable shoes and the same footwear on all test occa-sions. The use of orthopaedic devices and walking aids was noted to ensure that conditions were the same on all testing occasions. Indoor and outdoor tempera-tures were measured at each measure point in order to control for environmental factors. The primary outcomes were 10m and 30m timed walk in terms of time and stride length. Furthermore, the following measures and variables were used: oral temperature, spasticity, standing balance tests, Timed Up and Go, and the Nine-Hole Peg Test. One day after either active or placebo intervention, the PwMS filled in a study specific questionnaire. In the questionnaire, the PwMS rated presence and potential changes of fatigue, spasticity, weakness, pain, diffi-culty with balance or transfers or dressing/ undressing or thinking clearly, gait disturbance, dysarthria, or over-long time to recover. The choice of included questions was based on earlier findings regarding subjective experiences after us-ing a cooling garment.54 Furthermore, their general experience of wearing the vest was evaluated using a Visual Analogue Scale 0-100mm, as was the time when they experienced any possible effects from the intervention. Statistical procedure The analysis was performed using the differences within-persons (the measures after treatment minus baseline values).2 Mainly non-parametric methods were
Avh_YlvaNilsagard_K131008.indd 35 08-10-14 07.38.55

36
chosen due the fact that data was not normally distributed. The Mann Whitney U-test was used to perform calculations of periodic, carry over and treatment ef-fects for the primary outcomes including the objective variables. Analysis of peri-odic effect compares potential differences between the periods for the two groups. If there is no such difference present, we expect the mean differences between the periods in the two groups to be equal but have an opposite sign. The treatment periodic or carry over effect evaluates if there is any interaction between the par-ticipants’ mean values for the two treatment conditions. Treatment periodic effect or carry over effect was absent in all but two objective variables. Therefore all values were used in the analysis of treatment effect for the objective variables and for Visual Analogue Scale (VAS). Wilcoxon signed ranks tests were used for analysis of the study specific questionnaire, performing simple comparison of treatments. A paired t-test was used to analyse temperatures indoors and out-doors. 4.2.1 Study II Design A repeated measures design was used including three measure points. The PwMS were randomised into two groups with two different time schedules (Figure B). Data obtained from Study I was used. The group starting with the placebo con-tributed with two measure points at baseline with 45min between and one meas-ure point seven days thereafter with 45min between. The group starting with ac-tive treatment in Study I contributed with one measure point at baseline and two measure points seven days later. Procedure Participating centres were Örebro University Hospital and Mälar Hospital in Eskilstuna (Figure C). The 10m timed walk test at a self-selected speed was per-formed from a still start behind a starting line. Time was registered from when the command ‘Go’ was given, until the persons passed a second line. The test was performed three consecutive times, generating a total of 387 values. For Timed Up and Go, a 47 cm-high chair with arm and back supports was used. The dis-tance was marked with tape on the floor and a cone marked the turning point. The persons were encouraged to walk as quickly as was consistent with safety. After one trial attempt, Timed Up and Go was performed twice, generating a to-tal of 258 values. The 30m timed walk test at a forced speed was performed three consecutive times, generating a total of 387 values. Statistical procedure Reproducibility was evaluated within a single measure point as well as between three different measure points, and the correlation between the three different tests was calculated. Since the distribution of data was skewed, all calculations were performed using log-transformed data.
Intra class correlation is the correlation between two measurements (single rating or mean value of ratings) on the same target.137 The combined col-lected data was analysed so the effect of the data collector contributed to the variability of the ratings. Intra class correlation2,1 was used since it penalises sys-tematic errors when analysing repeated measures within the same occasion, when
Avh_YlvaNilsagard_K131008.indd 36 08-10-14 07.38.55

37
repeating the measuring after one week, and to compare the first value to the mean value. Intra class correlation1,1 was used to assess the correlation between the 10m and 30m timed walk and Timed Up and Go.
If measurement error is present, the difference between two meas-urements may be caused by this error and not by actual difference in perform-ance. To determine a genuine change in performance, quantification of the small-est percentage difference has been developed.9 Since data was not normally dis-tributed, the smallest real ratio was instead calculated.
4.2.2 Figure B Schedule for active treatment with cooled vest 45min, placebo 45min with a room-tempered vest, the four test occasions in Study I, and for the three measure points used in Study II (shaded). 4.2.3 Figure C
Flowchart Study I-II.
4.3 Study III Design A cross sectional design with data gathered at one point from a convenience sam-ple was used. Eighty-two PwMS were included and 81 were analysed (Figure D).
82 eligible PwMS were sent a letter of invitation 16 were not subjectively
heat-sensitive
17 declined participation 1 was unable to be
contacted48 were randomised
5 dropped out during the study
43 were analysed
Placebo 22 ˚C
Placebo 22 ˚C
Active -20 ˚C
Active -20 ˚C
7 days washout
7 days washout
Group II
Group I 4
44 33
33 22
2
11
11
Avh_YlvaNilsagard_K131008.indd 37 08-10-14 07.38.56

38
Procedure Participating centres were Örebro University Hospital, Mälar Hospital in Eskilstuna, Sahlgrenska University Hospital in Gothenburg and the Primary Health Care districts of West and East Östergötland County. The test procedure was implemented and performed at the respective unit involving seven physio-therapists trained for securing accordance of the test procedure. The Berg Balance Scale, Timed Up and Gocognitive and the Four Square Step Test were performed in a randomised order. One practice trial was performed for the Four Square Step Test and Timed Up and Gocognitive followed by two performances, and the best values were used in further calculations. The 12-item MS Walking Scale was completed at the end of the session. Statistical procedure Kendall’s tau coefficient was used for calculations of 1) correlations between the 12-item MS Walking Scale (S) and Timed Up and Gocognitive, the Berg Balance Scale and the Four Square Step Test, 2) correlations between specific items, and 3) cor-relations between Timed Up and Gocognitive, the Berg Balance Scale and the Four Square Step Test. Kendalls tau measures the degree of correspondence between two rankings with the hypothesis being that there is no correlation between the rankings of the respective scale. Two-tailed tests are used since the correlation can be either negative (high values in one scale correlates with low values on another scale) or positive (the scales have the same direction).2
Internal consistency measures if each item in a scale measures the same concept and was calculated using Cronbach’s alpha. The coefficient ranges from 0 (the items in the scale have no correlation with each other) and 1 (perfect correlation). When comparing groups, alpha coefficients at 0.7 to 0.8 are consid-ered sufficient, but when evaluating individuals, values at 0.9 are recommended.14 4.4.1 Study IV Design A longitudinal cohort design was conducted with prospectively collected data for accidental falls during twelve weeks involving five units. Seventy-six PwMS com-pleted the study (Figure D) and were analysed. Procedure Participating centres were Örebro University Hospital, Mälar Hospital in Eskilstuna, Sahlgrenska University Hospital and Primary Health Care districts of West and East Östergötland County. The PwMS were tested on one occasion at the respective unit involving seven physiotherapists trained for securing accor-dance of the test procedure. Information was collected on age, gender, height, weight, history of falling, fear of falling, avoiding activities due to fear of falling, use of assistive devices for walking or transferring, urinary incontinence and medication. Medications were later classified (L-GG) for possible side effects e.g., dizziness, tiredness or reduced blood pressure. The test procedure included ex-amination of sensory touch, proprioception and spasticity all in the lower ex-tremities, fatigue and cognition.
The Berg Balance Scale, Timed Up and Gocognitive and the Four Square Step Test were performed in a randomised order in blocks of six within each cen-
Avh_YlvaNilsagard_K131008.indd 38 08-10-14 07.38.56

39
tre using a computerised random-number generator. One practice trial was per-formed for the Four Square Step Test and Timed Up and Gocognitive followed by two performances and the best values were used in further calculations. A ran-dom-number table was used for the numbers chosen in the Timed Up and Gocogni-
tive. The 12-item MS Walking Scale was completed at the end of the session. Daily self-registry of falls and near fall incidents followed during twelve weeks. Every fortnight, data for two weeks were sent to one of the authors (YN) who made reminder phone calls if the data did not return in the scheduled time. In order to describe the circumstances when falling, pre-categorised alternatives and one open alternative ‘other’ were used. After completion of the twelve weeks, a fol-low-up telephone call was made. The PwMS were then asked to recall the number of actual falls during the twelve-week period to investigate the correlation be-tween actual falls and retrospective falls. Statistical procedure Spearman’s rho was calculated to assess agreement between prospectively col-lected data and retrospectively reported data for accidental falls during the study period of twelve weeks and between the number of falls and near fall incidents.2 The variables were ranked and then correlated. Spearman’s correlation was used since data was not normally distributed.
Since established cut-offs for the respective test or variables investi-gated were not available for PwMS, they were chosen in order to maximise the sum of sensitivity and specificity for calculation of predictive values. The percent-age of correctly identified fallers and non-fallers were reported as sensitivity and specificity. The Youden Index was calculated (sensitivity + specificity –1).
Positive predictive value is the proportion of persons with test results above (below for Berg Balance Scale) the cut-off that are correctly classified as fallers. Negative predicted value is the proportion of persons with test results be-low (above for Berg Balance Scale) the cut-offs that are correctly classified as non-fallers.3
The likelihood ratios summarises how many times more (or less) likely a person that experiences accidental falls has test results worse or equal to the cut-offs. Likelihood ratios above 10 or below 0.1 are considered strong.37 The ratio describes the probability of a specific test result in, for example, fallers to the probability in non-fallers63. Positive likelihood ratio is the ratio of the propor-tion of fallers correctly classified as fallers divided by the proportion of non-fallers incorrectly classified as fallers. Positive likelihood ratio is calculated as sen-sitivity/(specificity-1) and shows how much the odds increase for being a faller with a positive test result. Negative likelihood ratio is the ratio of the proportion of fallers incorrectly classified as fallers divided by the proportion of non-fallers correctly classified, and is calculated as (1-sensitivity)/specificity.63
Simple logistic regression analysis was used to identify clinical vari-ables related to falls (as they would be potential confounders) and for the investi-gated measures. Multiple logistic regression analysis was used to evaluate the test effect while adjusting for the clinical variables found to be significantly related to falling. Odds are a way of describing the ratio of the probability that the event of interest occurs to the probability that it does not.15
Avh_YlvaNilsagard_K131008.indd 39 08-10-14 07.38.57

40
Nagelkerke’s R2 was used as a measure of explanatory value for comparisons between the tests and the clinical variables.103 It is a measure of the proportion of variance explained by the regression model (Table 12).
Avh_YlvaNilsagard_K131008.indd 40 08-10-14 07.38.57

41
4.4.2 Figure D Flowchart Study III-IV.
82 PwMS included and tested
4 PwMS were excluded due to violation of inclusion criteria (EDSS, age)
2 PwMS dropped out directly at study start
81 PwMS were finally analysed in Study III
76 PwMS were finally included in Study IV
1 excluded due to violation of inclusion criteria (age)
Avh_YlvaNilsagard_K131008.indd 41 08-10-14 07.38.57
42
4.5 Study V Design A qualitative content analysis with a mainly deductive approach was used to ana-lyse the text material achieved by the interviews.42 The ICF173 was used as a framework both to create an interview guide and to analyse data. Nineteen PwMS had reported at least one fall during a twelve-week period (Study IV). Since then, one had died and two had moved outside the county. Four persons declined participation due to personal reasons. Consequently, data from twelve PwMS living in Örebro County were gathered during semi-structured interviews. Procedure Before the interviews, background data was collected including the Frenchay Ac-tivity Index.68 The interviews were conducted by one of the authors (YN). The interview guide was derived from the ICF’s domains and the focus was repeatedly placed on falls. The focus of the interviews was the individual’s perception of which factors they thought either prevented or triggered accidental falls. Loca-tions of the interviews were voluntary. Of twelve persons, nine were interviewed in their homes and three at Örebro University Hospital. The opening question was: “You were invited to participate since you have reported experiencing falls. Can you please tell me as much as possible about the circumstances when you fall?“ The interviews took 30 to 60min, were tape-recorded and transcribed ver-batim. The transcribed interviews were analysed in the steps described below. NVivo software121 was used as support. Data analyses The following steps were taken during the analyses of the interviews:
1. The transcribed interviews were read in their entirety to obtain an overall picture.
2. Categories were created and defined inductively, independently of ICF, us-ing a pilot interview in order to ensure that statements, which might not fit ICF critera and thereby impede the validity of the results, would not be missed.
3. The categorisation of the statements in the pilot interview was discussed with a co-author (KB), resulting in refined categories. The ongoing inter-views were then coded and new nodes were created when needed and defi-nitions were refined.
4. The created categories were matched with ICF, resulting in further analysis where some existing categories were merged or divided in order to match ICF definitions. Each category was, thus, named and defined according to the ICF. The categories were placed into the ICF model, and relationships within the model were considered. The statements in each category were concentrated into a running text and several quotes were initially chosen to illustrate the categories. The texts of the separate categories were then reread in several steps, moving back and forth between the text and the output of the content analysis, checking for consistency in coding. From earlier selected quotes, those reflecting the categories content the most were finally chosen.
Avh_YlvaNilsagard_K131008.indd 42 08-10-14 07.38.57

43
5. The categories were then ranked according to the number of informants having reflected upon issues related to each node and upon the amount of paragraphs coded for the separate nodes.
6. The matrix coding queries- function121 was used to investigate potential differences or similarities depending on attribute variables such as type of MS, and whether living in an apartment or in a house, living alone or liv-ing with a partner.
All steps of the analytic procedure were continuously discussed with a co-author until consensus was reached (KB).
4.6 Ethical considerations Ethical approval and advisory opinion was obtained for the included studies from the Regional Ethics committee in Uppsala. Participation in the studies was volun-tary and written informed consent was received. The choice to participate or not in the studies did not affect the access to care of the participants and they were informed of their right to terminate their participation at any time.
Avh_YlvaNilsagard_K131008.indd 43 08-10-14 07.38.57

Avh_YlvaNilsagard_K131008.indd 44 08-10-14 07.38.57
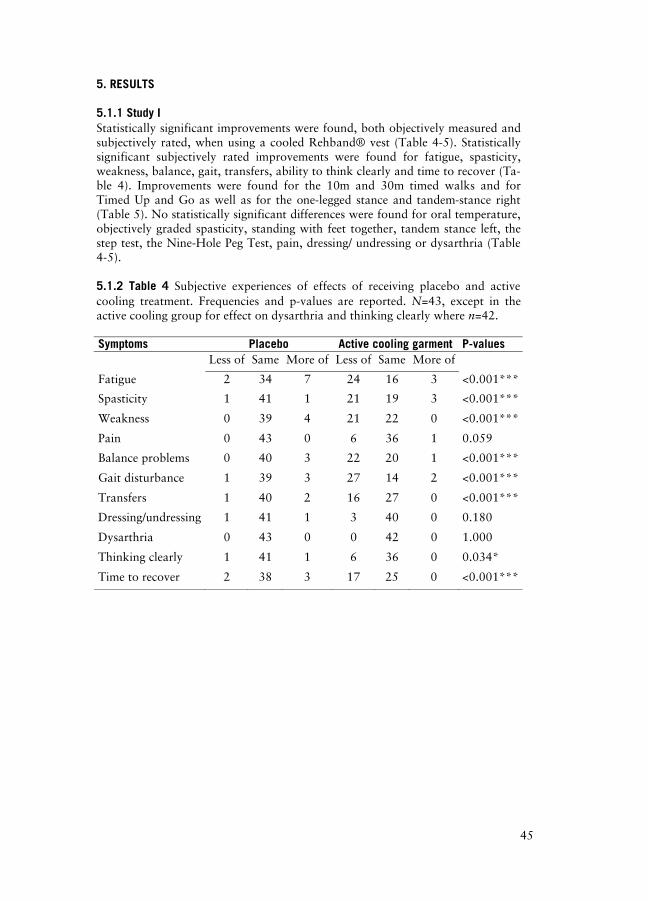
45
5. RESULTS 5.1.1 Study I Statistically significant improvements were found, both objectively measured and subjectively rated, when using a cooled Rehband® vest (Table 4-5). Statistically significant subjectively rated improvements were found for fatigue, spasticity, weakness, balance, gait, transfers, ability to think clearly and time to recover (Ta-ble 4). Improvements were found for the 10m and 30m timed walks and for Timed Up and Go as well as for the one-legged stance and tandem-stance right (Table 5). No statistically significant differences were found for oral temperature, objectively graded spasticity, standing with feet together, tandem stance left, the step test, the Nine-Hole Peg Test, pain, dressing/ undressing or dysarthria (Table 4-5). 5.1.2 Table 4 Subjective experiences of effects of receiving placebo and active cooling treatment. Frequencies and p-values are reported. N=43, except in the active cooling group for effect on dysarthria and thinking clearly where n=42.
Symptoms Placebo Active cooling garment P-values Less of Same More of Less of Same More of
Fatigue 2 34 7 24 16 3 <0.001***
Spasticity 1 41 1 21 19 3 <0.001***
Weakness 0 39 4 21 22 0 <0.001***
Pain 0 43 0 6 36 1 0.059
Balance problems 0 40 3 22 20 1 <0.001***
Gait disturbance 1 39 3 27 14 2 <0.001***
Transfers 1 40 2 16 27 0 <0.001***
Dressing/undressing 1 41 1 3 40 0 0.180
Dysarthria 0 43 0 0 42 0 1.000
Thinking clearly 1 41 1 6 36 0 0.034*
Time to recover 2 38 3 17 25 0 <0.001***
Avh_YlvaNilsagard_K131008.indd 45 08-10-14 07.38.57

46
5.1.3 Table 5 Differences between post placebo and baseline values, and for post-active treatment and baseline values. Medians and inter-quartile ranges (25-75 %) are given together with p-values. N=43 except for oral temperature where n=42. Variables Placebo Active treatment P-values
10m timed walk (s) 0.12 (-0.18 - 0.61) -0.30 (-1.01 - 0.12) 0.001***
10m timed walk (steps) 0.17 (-0.17 - 0.67) -0.50 (-0.83 - 0.08) <0.001***
30m timed walk (s) 0.38 (-0.26 - 1.43) -0.71 (-1.93 - 0.40) <0.001***
30m timed walk (steps) 0.67 (0.17 - 2.38) -1.00 (-1.92 - 0.17) <0.001***
Oral temperature (˚C) 0.00 (-0.10 - 0.15) -0.05 (-0.20 - 0.12) 0.426
Modified Ashworth 0.00 (-0.50 - 0.62) -0.50 (-1.25 - 0.50) 0.296
Standing, feet together (s) 0.00 (0.00 - 0.00) 0.00 (0.00 - 0.00) 0.720
Tandem stance, right (s) -1.74 (-10.10 - 0.00) 0.31 (-1.06 - 4.06) 0.025*
Tandem stance, left (s) -0.93 (-3.86 - 0.19) 0.20 (-0.66 - 3.52) 0.055
One-leg stance, right (s) -1.14 (-3.75 - 0.30) 0.14 (-1.00 - 1.02) 0.003**
One-leg stance, left (s) -0.01 (-1.10 - 0.52) 1.36 (-0.81 - 3.11) 0.045*
Step test, right (steps) 0.25 (-0.50 - 1.00) 0.50 (-0.25 - 0.75) 0.990
Step test, left (steps) 0.00 (-0.12 - 0.62) 0.50 (-0.50 - 1.00) 0.720
Timed Up and Go (s) 0.15 (-0.48 - 0.90) -0.54 (-1.43 - 0.22) 0.003**
Nine- Hole Peg Test score 0.32 (-2.95 - 2.83) -0.25 (-2.85 - 2.57) 0.990
Avh_YlvaNilsagard_K131008.indd 46 08-10-14 07.38.58

47
5.1.4 Clinical message - Study I Objective and subjective effects were found when wearing the Rehband vest® in-dicating clinically relevant results likely to have a positive effect on everyday life and thus encourage an active life-style. 5.2.1 Study II The reproducibility of the 10m and 30m timed walk tests and Timed Up and Go was very high. An intra class correlation coefficient at 0.97-0.98 was found within a single measure point. The corresponding coefficient between measure points was 0.91-0.93 (Table 6). Comparisons between first attempts, mean values of timed gait tests and best value of Timed Up and Go as calculated using Intra Class Cor-relation1,1 revealed correlations at 0.99 to 1.0 (Table 7). These results were pro-duced independently of EDSS above 4.0 or not. 5.2.2 Table 6 Test retest results as calculated with Intra Class Correlation2,1
pre-sented at a 95% confidence interval, using the results of the first attempt at the respective measure point. 30m timed walk 10m timed walk Timed Up and Go Total 0.93 (0.89 0.96) 0.92 (0.86 0.95) 0.91 (0.83 0.95) EDSS 3.0-4.0 0.96 (0.92 0.98) 0.87 (0.74 0.94) 0.84 (0.66 0.93) EDSS 4.5-6.0 0.89 (0.77 0.95) 0.91 (0.82 0.96) 0.88 (0.76 0.95) 5.2.3 Table 7 Comparisons between first attempts; mean values of timed gait tests and best value of Timed Up and Go as calculated with Intra Class Correlation2, 1
presented at a 95% confidence interval. 30m timed walk 10m timed walk Timed Up and Go Total 1.00 (0.99 1.0) 0.99 (0.95 1.0) 0.99 (0.93 1.0) EDSS 3.0-4.0 0.99 (0.98 1.0) 0.98 (0.77 1.0) 0.96 (0.69 0.99) EDSS 4.5-6.0 1.00 (0.99 1.0) 0.98 (0.96 1.0) 1.00 (0.98 1.0) To be able to detect a genuine change, an improvement of –23% to –29% or a deterioration of +30% to +40% is needed (Table 8). However, the size of this change differed depending on EDSS. For less severely affected persons (EDSS 3.0-4.0), a smaller percentage increase or decrease was required, especially for the 30m timed walk in comparison with more severely disabled persons. 5.2.4 Table 8 The smallest percentage difference required for detecting a genuine change is presented for the 10m and 30m timed walk tests and for Timed Up and Go. The first attempts from the two baseline sessions were used. 30m timed walk 10m timed walk Timed Up and Go Total 29 / +40 23 / +30 24 / +31 EDSS 3.0-4.0 14 / +17 23 / +29 21 / +27 EDSS 4.5-6.0 38 / +60 25 / +33 27 / +36
Avh_YlvaNilsagard_K131008.indd 47 08-10-14 07.38.58

48
The correlation between all the three measures was high (0.85) (Table 9). The correlation between the timed walk tests and Timed Up and Go was lower for those with EDSS 3.0-4.0 compared to those with EDSS 4.5-6.0 5.2.5 Table 9 Correlations between the test results as calculated with Intra Class Correlation1,1 presented at a 95% confidence interval. Values from the first at-tempt in the first testing session were used. All tests 30m / 10m 30m / TUG 10m / TUG Total 0.85
(0.76 0.91) 0.85
(0.74 0.92) 0.85
(0.74 0.92) 0.83
(0.71 0.91) EDSS 3.0-4.0 0.76
(0.59 0.88) 0.85
(0.69 0.93) 0.72
(0.45 0.87) 0.70
(0.42 0.86) EDSS 4.5-6.0 0.83
(0.67 0.92) 0.81
(0.56 0.92) 0.83
(0.61 0.93) 0.85
(0.66 0.94) TUG: Timed Up and Go 5.2.6 Clinical message – Study II Due to the high correlations, the choice of using only one measure and using only one attempt seems sufficient. Severity of MS (EDSS) is of importance when esti-mating the smallest real ratio needed to establish a genuine change, especially if using the 30m timed walk test.
Avh_YlvaNilsagard_K131008.indd 48 08-10-14 07.38.58

49
5.3.1 Study III Walking ability was rated as limited in a majority of the investigated persons. Apart from perceived reduction in gait speed and distance, the qualitative aspects of walking were perceived as being limited (Table 10). 5.3.2 Table 10 Median (M) and interquartile range (25-75%), frequency distribu-tion and percentage reported for the items in the MS Walking Scale: n=81, except for item 6 where n=80. Item 1- 12 Not at
all =1
A little
=2
Mode- rately
=3
Quite a bit =4
Extre-mely =5
1. Limited your ability to walk? M=4 (3-4)
7 (8.6)
12 (14.8)
15 (18.5)
34 (42)
13 (16)
2. Limited your ability to run? M=5 (5-5)
3 (3.7)
2 (2.5)
2 (2.5)
7 (8.6)
67 (82.7)
3. Limited your ability to climb up and down stairs? M=4 (3-4)
6 (7.4)
9 (11.1)
20 (24.7)
28 (34.6)
18 (22.2)
4. Made standing while doing things more difficult? M=3 (2-4)
9 (11.1)
19 (23.5)
22 (27.2)
22 (27.2)
9 (11.1)
5. Limited your balance when standing or walking? M=3 (3-4)
4 (4.9)
9 (11.1)
30 (37)
27 (33.3)
11 (13.6)
6. Limited how far you are able to walk? M=4 (4-5)
4 (5.0)
6 (7.5)
9 (11.3)
29 (36.3)
32 (40.0)
7. Increased the effort needed for you to walk? M=4 (3-5)
5 (6.2)
8 (9.9)
12 (14.8)
33 (40.7)
23 (28.4)
8. Made it necessary for you to use sup-port when walking indoors? M=3 (2-4)
17 (21.0)
16 (19.8)
17 (21.0)
15 (18.5)
16 (19.8)
9. Made it necessary for you to use sup-port when walking outdoors? M=4 (1-5)
22 (27.2)
5 (6.2)
8 (9.9)
19 (23.5)
27 (33.3)
10. Slowed down your walking? M=4 (2-5)
8 (9.9)
13 (16.0)
6 (7.4)
24 (29.6)
30 (37.0)
11. Affected how smoothly you walk? M=4 (3-5)
5 (6.2)
9 (11.1)
13 (16.0)
18 (22.2)
36 (44.4)
12. Made you concentrate on your walking? M=4 (3-5)
6 (7.4)
5 (6.2)
15 (18.5)
25 (30.9)
30 (37.0)
The internal consistency was acceptable for nine of the twelve items (0.69-0.84) Lower values were obtained for items regarding abilities to run, to climb up and down stairs and standing activities (0.56-0.62).
The correlations calculated between the 12-item MS Walking Scale and the investigated objective tests were low; the Berg Balance Scale (r=-0.368), Timed Up and Gocognitive (r=0.319) and the Four Square Step Test (r=0.338). This was also the case between different items of the 12-item MS Walking Scale and test results from Timed Up and Gocognitive, the Four Square Step Test or items from the Berg Balance Scale (r=-0.184 – 0.385).
Avh_YlvaNilsagard_K131008.indd 49 08-10-14 07.38.58

50
5.3.3 Clinical message – Study III The 12-item MS Walking Scale captures several aspects of perceived limitations in walking ability among PwMS and can be used for clinical and research purposes. The scale provides complementary information to the Berg Balance Scale, Timed Up and Gocognitive and the Four Square Step Test. 5.4.1 Study IV Forty-eight persons (63%) reported a total of 270 accidental falls during a twelve- week period and 2.352 near fall incidents. Most falls occurred during the afternoon when performing daily activities (Table 11). Two persons reported hav-ing a fracture as a consequence of falling during the study period. 5.4.2 Table 11 Circumstances and frequency of reported activities when falling; n=270. Circumstance Frequency % Time Morning
Afternoon Evening Night Missing or unclear data
69 94 51 7 49
31 43 23 3
Self-perceived fatigue
Not at all As usual Somewhat more than usual Much more than usual Missing or unclear data
24 86 89 23 48
11 39 40 10
Being in a hurry
Not at all As usual Somewhat more than usual Much more than usual Missing or unclear data
103 81 48 1 37
44 35 21 <1
Reported activities
Personal hygiene Working in the kitchen Cleaning indoors Working outdoors Physical activities/ leisure pursuit Other activities Missing or unclear data
19 31 24 24 63 57 52
9 14 11 11 29 26
Avh_YlvaNilsagard_K131008.indd 50 08-10-14 07.38.59

Sum of falls and sum of near fall incidents were moderately correlated at r=0.57. The correlation between retrospectively and prospectively collected data regarding falls was r=0.82 (Figure E). 5.4.3 Figure E
0
5
10
15
20
25
30
35
40
45
0 5 10 15 20 25 30 35
Prospectively reported falls
Retro
spec
tivel
y re
porte
d fa
lls
Correlation (r=0.82) between retrospectively recalled falls and registered falls; n=61. EDSS, spasticity, use of walking aid and proprioception differed significantly between fallers and non-fallers (Table 12). When adjusting for these variables, the measures were not significantly related to falling (Table 13). 5.4.4 Table 12 Possible effect modifying clinical variables. Self-reported data Non-fallers
n=28 Fallers n=48
Odds Ratio (95% CI)
R2
Age, years (mean, range) 50 (32-75) 50 (25-71) 1.00 (0.96; 1.05)
0.000
Body Mass Index, kg/m2, (median, range)
24 (18-33) 24 (18-36) 1.02 (0.91; 1.16)
0.003
EDSS (median, range) 4.0 (3.0-6.0) 5.0 (3.5-6.0) 1.99 (1.22; 3.40)
0.133
Fatigue Severity Scale (Median, Range)
6.5 (1.9-9.0) 6.5 (1.7-9.0) 0.98 (0.77; 1.25)
0.000
Spasticity (median, range) 2.0 (0-14) 4.0 (0-28) 1.14 (1.02; 1.31)
0.089
Gender, Male 6 (21) 13 (27) 1.36 (0.46; 4.37)
0.005
History of falling 12 (43) 29 (60) 2.04 (0.80; 5.34)
0.066
Urinary incontinence 17 (61) 32 (67) 1.08 (0.41; 2.80)
0.000
51

52
Self-reported data Non-fallers n=28
Fallers n=48
Odds Ratio (95% CI)
RR22
Cognitive dysfunction 9 (32) 21 (44) 0.99 (0.65; 1.46) 0.000 Medication with potential side-effects1
18 (64) 33 (69) 1.22 (0.45; 3.27) 0.003
MS type Relapsing remitting
17 (61) 23 (48) Ref 0.022
Secondary progressive
8 (29) 19 (40) 1.76 (0.63; 5.13)
Primary pro-gressive
3 (11) 6 (12) 1.48 (0.34; 7.79)
Fear of falling
No 9 (32) 22 (46) 0.95 (0.57; 1.58)3 0.001
Some
11 (39) 12 (25)
Moderate 8 (29) 10 (21) Extreme 0 (0) 4 (8) Avoidance Never 8 (29) 15 (31) 1.04 (0.66; 1.65)3 0.001 Seldom 7 (25) 11 (23) Sometimes 11 (39) 15 (31) Often 2 (7) 7 (15) Walking aid None 9 (32) 4 (8) 2.27 (1.23; 4.37)2 0.120 Indoors or
outdoors 5 (18) 8 (17)
Both indoors and outdoors
14 (50) 36 (75)
Disturbed superficial touch
Feet 12 (43) 25 (52) 1.45 (0.57; 3.76) 0.011
Leg 11 (39) 26 (54) 1.83 (0.72; 4.81) 0.028 Disturbed propriocep-tion
No 14 (50) 10 (21) 2.50 (1.36; 5.12)2 0.158
Big toes 12 (43) 21 (44) Ankles 0 (0) 11 (23) Knees 2 (7) 6 (12)
Descriptive statistics and odds ratios for falling reported with 95% confidence intervals. Frequencies (%) are given unless otherwise stated. 1Fatigue, dizziness and/or reduced blood pressure; 2Odds ratio for each step of the ordinal scale; R2: Nagelkerke
Avh_
Yl
vaNilsagard_K131008.indd 52 08-10-14 07.38.59
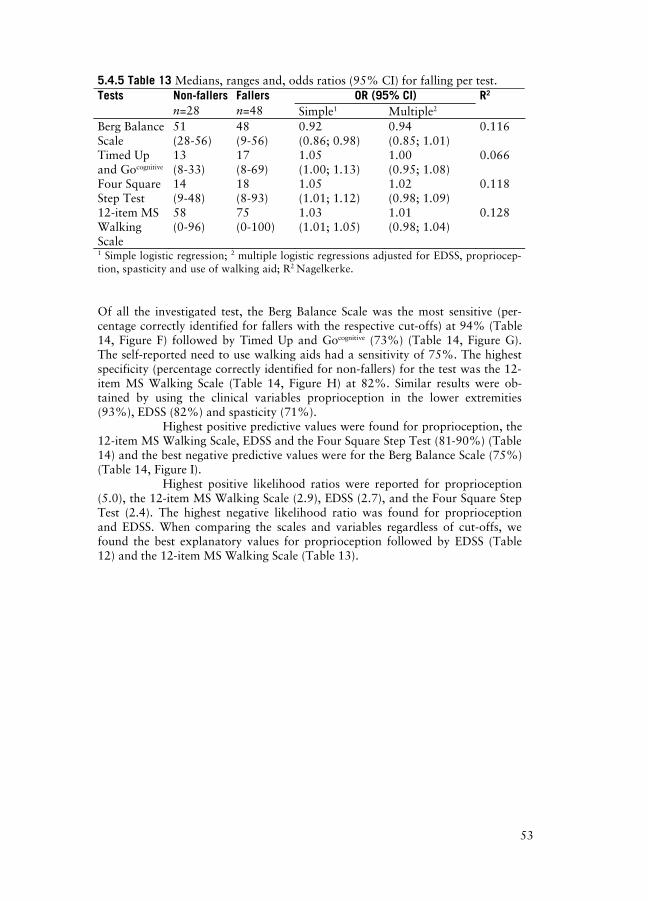
53
5.4.5 Table 13 Medians, ranges and, odds ratios (95% CI) for falling per test. OR (95% CI) Tests Non-fallers
n=28 Fallers n=48 Simple1 Multiple2
R2
Berg Balance Scale
51 (28-56)
48 (9-56)
0.92 (0.86; 0.98)
0.94 (0.85; 1.01)
0.116
Timed Up and Gocognitive
13 (8-33)
17 (8-69)
1.05 (1.00; 1.13)
1.00 (0.95; 1.08)
0.066
Four Square Step Test
14 (9-48)
18 (8-93)
1.05 (1.01; 1.12)
1.02 (0.98; 1.09)
0.118
12-item MS Walking Scale
58 (0-96)
75 (0-100)
1.03 (1.01; 1.05)
1.01 (0.98; 1.04)
0.128
1 Simple logistic regression; 2 multiple logistic regressions adjusted for EDSS, propriocep-tion, spasticity and use of walking aid; R2 Nagelkerke. Of all the investigated test, the Berg Balance Scale was the most sensitive (per-centage correctly identified for fallers with the respective cut-offs) at 94% (Table 14, Figure F) followed by Timed Up and Gocognitive (73%) (Table 14, Figure G). The self-reported need to use walking aids had a sensitivity of 75%. The highest specificity (percentage correctly identified for non-fallers) for the test was the 12-item MS Walking Scale (Table 14, Figure H) at 82%. Similar results were ob-tained by using the clinical variables proprioception in the lower extremities (93%), EDSS (82%) and spasticity (71%).
Highest positive predictive values were found for proprioception, the 12-item MS Walking Scale, EDSS and the Four Square Step Test (81-90%) (Table 14) and the best negative predictive values were for the Berg Balance Scale (75%) (Table 14, Figure I).
Highest positive likelihood ratios were reported for proprioception (5.0), the 12-item MS Walking Scale (2.9), EDSS (2.7), and the Four Square Step Test (2.4). The highest negative likelihood ratio was found for proprioception and EDSS. When comparing the scales and variables regardless of cut-offs, we found the best explanatory values for proprioception followed by EDSS (Table 12) and the 12-item MS Walking Scale (Table 13).
Avh_YlvaNilsagard_K131008.indd 53 08-10-14 07.39.00

54
5.4
.6 T
able
14
A
ccu
racy
of
the
pred
icti
on o
f fa
lls.
Avh_YlvaNilsagard_K131008.indd 54 08-10-14 07.39.00

55
5.4.7 Figure F
The Berg Balance Scale correctly identified 94% of those who fell in our sample using a cut-off at 55points (sensitivity). 5.4.8 Figure G
Timed Up and Gocognitive correctly identified 73% of the fallers using a cut-off at 13.6s (sensitivity). 5.4.9 Figure H
82% of the persons scoring below the cut-off at 75 on the 12-item MS Walking were correctly identified as non-fallers (specificity). 5.4.10 Figure I
Percentages of those with a test result worse than the respective cut-off and that actually fell during the study period (positive predictive values).
Berg Bal-ance Scale
55p
Timed Up and Gocognitive
13.6s
Four Square Step test
16.9s
12-item MS Walking
Scale 75
Avh_YlvaNilsagard_K131008.indd 55 08-10-14 07.39.00

56
The odds for falling are presented for the 1st to 4th quartile (Figure J) with the re-spective cut-offs (Table 15). In general, the worse performance of the tests, the greater the odds of falling. 5.4.11 Figure J
0
1
2
3
4
5
6
7
8
9
FSST BBS TUG MSWS EDSS
Odd
s fo
r fa
lling
1st quartile
2nd quartile
3rd quartile
4th quartile
Odds for falling divided into quartiles for the respective scale and EDSS. For exact val-ues, see table 15. FSST: Four Square Step test; BBS: Berg Balance Scale; TUG: Timed Up and Gocognitive; MSWS: 12-item MS Walking Scale. 5.4.12 Table 15 Odds for falling divided into quartiles for the respective scales and EDSS shown in Figure J. Tests 1st
quartile 2nd
quartile 3rd
quartile 4th
quartile Four Square Step Test (s) -12 12.1-17 17.1-24 24.1 Berg Balance Scale (p) 9-41 42-49 50-53 54-56 Timed Up and Gocognitive (s) -12.0 12.1-15.2 15.3-21.4 21.5-69.4 12-item MS Walking Scale (score) -49 50-67 68-81 82-100 EDSS 3-3.5 4-4.5 5-5.5 6
Avh_YlvaNilsagard_K131008.indd 56 08-10-14 07.39.01

57
5.4.13 Clinical message – Study IV The Berg Balance Scale identified the highest proportion of fallers and the 12-item MS Walking scale identified the highest proportion of non-fallers. If a PwMS has disturbed proprioception or spasticity in the lower limbs, reports a need to use a walking aid both indoors and outdoors increasing the odds of falling, a risk analysis should be performed considering the increased odds of falling. If a PwMS: * scores 55points or less on the Berg Balance Scale, the probability that he or she will fall is 70%. * scores 75 or more on the 12-item MS Walking Scale, the probability that he or she will fall is 83%. * needs 16.9s or more to complete the Four Square Step Test, the probability that he or she will fall is 81%. * needs 13.6s or more to complete the Timed Up and Gocognitive, the probability that he or she will fall is 73%. 5.5.1 Study V The persons described factors perceived as risk factors for accidental falls not previously established in MS populations in relation to falls. Those factors were divided attention, reduced muscular endurance, fatigue and heat-sensitivity. 5.5.2 Quotes:
”So it’s easy to walk and think about something else and look at some-thing else. Yes, when I come across something that gets in the way,.. maybe it’s someone who talks to me, getting in the way, or anything really, … I find it difficult to walk and get wobbly… because I’m not just concentrating on walking.”
”Falling … I do that more when I’m physically tired.”
”I’ve never fallen in the forenoon or rather it happens more in the eve-ning because by then I’ve used up all my energy and I can’t manage to stand on my legs any longer. ”
”Yes, I can’t bear heat so it’s really… well, … I can’t deal with it the same as I manage during the winter… because the heat just exhausts me more than anything else…. Oh, while I’m thinking about it, I’ve noticed that I’ve often got problems with cramp and I get it much more in the summer. ”
In addition, previously reported risk factors such as changed gait pattern, limited walking ability, impaired proprioception, seeing and, spasticity were described. Walking, recreation and leisure, maintaining and changing body position, lifting or carrying, taking care of the home, washing of the body, moving around, pre-paring meals and housekeeping were limited.
Avh_YlvaNilsagard_K131008.indd 57 08-10-14 07.39.01

58
”Yes, it’s really hard if I come across a mass of people; yes, so it is, … but I wouldn’t manage without the sticks (Nordic walking poles). In any case, sometimes you don’t even think you’ll come across a mass of folk that you might have to jostle your way through”.
”It’s things like when I’m standing, washing my face,… as soon as I shut my eyes mainly .. that’s when I fall.”
”I can’t lift heavy pots. I don’t bring hot food to the table. ”
”So we don’t have guests so often - and if you don’t invite some people to your house you don’t get invited out very much. This has become something I just can’t do. ”
Having access to supportive persons and using assistive device were considered to reduce falls. Unsuitable physical environment and climate conditions were con-sidered to induce falls. Several preventative strategies were described to partially compensate for the impairments, limitations and restrictions. The ability to use adequate preventing strategies and to adapt to the life situation was described and classified as personal factors (Figure K).
”It means an awful lot, so it does. It’s not just support, it’s mental support too…- that you have someone with you that knows you’re a bit wobbly and doesn’t question it.”
”… because if I stumble a little or something like that, my sticks (Nordic walking poles) get me steady again”.
”I walk near walls. It’s quiet good because you’ve always got some-thing there close by. You really need to take it very carefully with everything at home. It’s a bit harder outside but I walk all the time and watch the ground properly. ”
”Even though it’s hard, I need to figure all these things out myself. It doesn’t matter what others say you should do about this or that, you’ve got to let it mature, allow it… I guess it’s first and foremost not just to feel: ‘I’m so lazy since I haven’t done more than this” … but rather it’s an achievement that I’ve managed to do this. Al-though it’s taken many years!”
Avh_YlvaNilsagard_K131008.indd 58 08-10-14 07.39.01
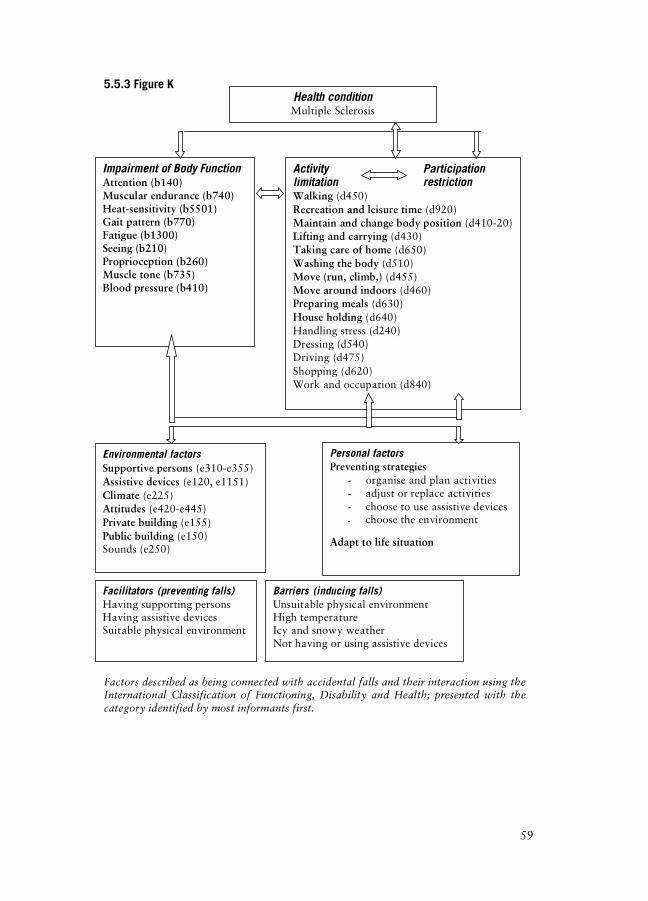
59
5.5.3 Figure K Factors described as being connected with accidental falls and their interaction using the International Classification of Functioning, Disability and Health; presented with the category identified by most informants first.
Impairment of Body Function Attention (b140) Muscular endurance (b740) Heat-sensitivity (b5501) Gait pattern (b770) Fatigue (b1300) Seeing (b210) Proprioception (b260) Muscle tone (b735) Blood pressure (b410)
Activity Participation limitation restriction Walking (d450) Recreation and leisure time (d920) Maintain and change body position (d410-20) Lifting and carrying (d430) Taking care of home (d650) Washing the body (d510) Move (run, climb,) (d455) Move around indoors (d460) Preparing meals (d630) House holding (d640) Handling stress (d240) Dressing (d540) Driving (d475) Shopping (d620) Work and occupation (d840)
Environmental factors Supportive persons (e310-e355) Assistive devices (e120, e1151) Climate (e225) Attitudes (e420-e445) Private building (e155) Public building (e150) Sounds (e250)
Personal factors Preventing strategies
- organise and plan activities - adjust or replace activities - choose to use assistive devices - choose the environment
Adapt to life situation
Barriers (inducing falls) Unsuitable physical environment High temperature Icy and snowy weather Not having or using assistive devices
Facilitators (preventing falls) Having supporting persons Having assistive devices Suitable physical environment
Health condition Multiple Sclerosis
Avh_YlvaNilsagard_K131008.indd 59 08-10-14 07.39.01

60
5.5.4 Clinical message – Study V With the knowledge of what factors PwMS perceive as being related to accidental falls, physiotherapists may tailor interventions to decrease the risk of falling. The interventions may be directed at all levels of the ICF and include, for example, hands-on treatment, physical exercise, task-specific training, prescription of assis-tive devices, information and education. By taking advantage of the different pro-fessional expertise in a MS-team, all aspects can be scrutinised. This message was given by one person at the end of Study IV illustrating some of the factors perceived as being related to falls:
” Hi!
Now 12 weeks have gone and I’m sending my last correspondence to you. This time has been useful for me (hope it’s also been the same for you). This time has got me thinking about why I fall.
I’ve come to the conclusion that I shouldn’t be in such a hurry or lose concentration when I’ve been still for a longer time because that’s when I get so stiff. I also need to think about lifting my feet properly so that I don’t stumble on the edge of the rug or something like that. I shouldn’t turn my head too fast either when I’m mov-ing around otherwise I’ll fall flat.
Greetings from 302”
Avh_YlvaNilsagard_K131008.indd 60 08-10-14 07.39.02

61
6. GENERAL DISCUSSION AND IMPLICATIONS 6.1 Results summary Working as a physiotherapist in a team caring for PwMS raises many clinical questions. Increased knowledge within a few areas of interest has been gained by conducting the studies within this thesis, although much research remains to be done. This is a summary of our findings.
We suggest using cooling garments as a self-administered intervention where adverse events are unlikely to occur and that heat-sensitive PwMS may benefit from.105 When using timed 10m or 30m walking tests or Timed Up and Go, one attempt is sufficient, and in most cases, one of the tests can be chosen to save both time and energy. We present limits for establishing a genuine change for Timed Up and Go and for the 10m and 30m timed walk tests. If a person walks 30% slower in the 10m or 30m timed walk tests or performs the Timed Up and Go at a 40% slower rate, a genuine deterioration is established. A genuine im-provement is established when the PwMS (EDSS 3.0-6.0) walks 23-29% faster when performing the investigated tests.104
By using the 12-item MS Walking Scale, different self-perceived as-pects of walking limitations are captured.66 Limitations in walking were stated by the majority (89-96%) of the investigated sample (EDSS 3.5-6.0). The need to use support was stated by 73% when walking indoors and by 79% when walking outdoors. The scale seems to capture aspects other than the Berg Balance Scale, Timed Up and Gocognitive and the Four Square Step Test do, since concurrent validity was not established between the 12-item MS Walking Scale and these tests.107 The scale may contribute with valuable information since it reflects the subjective per-spective of the limitations.
We found a prevalence of falls at 63% that indicates the importance of recognising and intervening against falls in PwMS (EDSS 3.5-6.0). Two hun-dred and seventy falls and 2.352 near fall incidents were reported. In the investi-gated sample, the Berg Balance Scale had the highest sensitivity (9 %) followed by reported use of a walking aid indoors and outdoors (75%) and Timed Up and Go (73%). The highest specificity was found for loss of proprioception (93%), the 12-item MS Walking Scale (82%), EDSS (82%) and the Four Square Step Test (75%). Loss of proprioception (90%), the 12-item MS Walking Scale, EDSS and the Four Square Step Test (81-83%) presented the best positive predicted values. Negative predictive values were, in general, lower than the positive values, with the excep-tion of the Berg Balance Scale (75%).108 The PwMS identified variables not earlier targeted in research as being the cause of falls in MS populations. This applies to divided attention, reduced muscular endurance, fatigue and heat-sensitivity.106 6.2 Results discussion The actual differences in time achieved at group level in performance between post placebo and baseline values and post active treatment and baseline values when wearing a Rehband® cooling garment may be scrutinised for clinical relevance. For example, for the 10m and 30m timed walk, the difference was highly statisti-cally significant but the difference was only 0.42s and 1.09s, respectively. The largest time differences were found for tandem stance right (2s) and for one legged stance right (2.28s) between the different conditions. We argue that since the ob-
Avh_YlvaNilsagard_K131008.indd 61 08-10-14 07.39.02
4

62
jectively measured improvements are in parity with those subjectively rated, these differences were also clinically relevant. Improvements in walking after the use of a cooling garment have also been reported in other studies.34, 54, 134
Walking speed is often used as a clinical measure as well as in re-search to evaluate interventions or to determine changes in functional status. The findings in Study II are in line with otherwise published research.74, 77, 133, 165 For the 10m timed walk, a difference at approximately 20-30% is considered as a genuine change104, 165; similar to that reported for a 25-foot timed walk at 20%.74, 77, 133 With a longer distance, such as the 30m timed walk, larger differences are needed (29-40%) and seem to vary depending on the severity of MS.104 A test retest reli-ability for 10m timed walk at approximately r=0.91-0.92 seems plausible when evaluating PwMS.104, 112
The mean walking speed of the investigated PwMS in Study I and II was 1.15-1.17 m/s104, 105, which is markedly slow. The following reference values have been reported for healthy persons aged 20 to 69 years: women walking at self-selected speed 1.54–1.35m/s7 or 1.24-1.16 m/s110 and for men 1.59-1.47m/s7 or 1.23-1.28 m/s.110 Reference values for a fast walking speed are reported as 1.63-1.64s for men and 1.69-1.56s for women. Likewise, the time to complete Timed Up and Go was longer (mean value 12.5-13.9s) for the PwMS compared to that of published normative values (mean value 5.31-7.24s) for healthy persons aged 20-69.71
The relevance of using walking speed as an outcome variable of an intervention may be questioned. To walk faster may in fact be a compensatory strategy for a person with balance problems. On the other hand, to walk slower may be a successful adjustment in order to gain more control over movements and possibly prevent evolvement of additional spasticity. Other aspects of walk-ing may, therefore, be of interest to evaluate.
The 12-item MS Walking Scale addresses limitations in running, stair climbing, balance, walking distance, effort when walking, the need to use support or assistive device, smoothness in walking and the need to concentrate when walking.66 The use of patient-based measures may help capture limitations possi-bly not reflected by objective measures. The internal consistency for items rating limitations in running, climbing stairs and, standing while doing something, was not satisfactory. Better values could possibly be obtained if investigating a sample without restrictions regarding EDSS, since the original scale was developed to include all PwMS regardless of EDSS; although those unable to walk at all will just tick a box indicating this on the form. It could also be argued that the item that has the limitations of standing activities should be dismissed since the scale measures limitations in walking ability. The remaining nine items all had an alpha coefficient around 0.7 but below 0.9. Consequently, the scale is primarily rec-ommended for use at group level. The scale has been revised by withdrawing all MS-specific terms and tested in a population consisting of different neurological diseases with promising results.69
The prevalence of accidental falls was found to be 63%, which is higher than previously reported.23, 27, 43, 51, 145 There are also some disparities for the predictive value of some variables compared to that reported by Finlayson et al.51 where we found no significant association with falling for gender, presence of bladder incontinence, medication intake, or fear of falling. However, we found
Avh_YlvaNilsagard_K131008.indd 62 08-10-14 07.39.02
63
an association for spasticity that was opposite to the findings of Cattaneo et al.23 Unambiguous agreement is found for the association between the need to use walking aids and accidental falls.27, 108, 145 If detecting those prone to falls is more important than detecting those who are not prone, proprioception measured by the modified Motor Capacity Assessment, part E was the most promising vari-able, followed by 12-item MS Walking Scale in the investigated sample. All inves-tigated tests, proprioception, spasticity, the need for using of walking aids, and EDSS had positive predictive values that exceeded the prevalence of falling at 63%. Two persons reported having had a fracture during the study period, and fractures are the most commonly reported injury after experiencing a fall, at least for PwMS aged 55-94 years.115
Frequency of falling among healthy persons in the age corresponding to that of the sample in Study IV is not published, to our knowledge. A fall fre-quency at 27% within one year for elderly persons ( 65 years) is reported, which is lower than that found for PwMS.23, 43, 51, 145 6.3 Methodological discussion This thesis includes PwMS with limitations for registered EDSS. Thus, the gener-alisability of the findings should be considered for persons or samples with simi-lar severity of MS. By using a multi-centre approach in Study I-IV, sufficient sam-ple sizes were achieved and the generalisation of the results were also reinforced by having participants from five different centres. The distribution of gender in the respective studies were, with the exception of Study V, in parity with the es-timated ratio of at least 2:130 with more women affected than men.
A general weakness of the studies is that EDSS was mainly achieved from medical records or registries instead of rated at the time for the test occa-sions. It is possible that the actual EDSS has changed in either direction for an individual since it was last registered. It could be suggested that where there is a more active progression in MS, a more frequent contact with the neurologist can be expected, thereby giving an updated EDSS, whilst with a more sedentary course of MS, longer periods of time may have elapsed since the latest rating of the EDSS score. However, it is most probable that the EDSS could be somewhat higher than earlier registered for the total study group due to the time factor and the progressive feature of the disease. Neurologists at the respective unit did the ratings primarily. Agreement between raters on the EDSS has been reported to be 69%.135 It is uncertain as to whether or not these above mentioned aspects inflict the results.
Besides being used as an inclusion criterion and as a descriptive vari-able of the samples, EDSS was used in the analyses in Study II and IV. A distinc-tion between those having a more severe MS within the study group depending on EDSS was used for calculations of test-retest reliability, correlation between tests, and when calculating the smallest percentage difference to detect a genuine change for timed walk tests and Timed Up and Go.104 EDSS was also used for calculations of predictive values for accidental falls.108
The recruitment of study participants in some centres was facilitated by the use of the Swedish MS Registry.149 Since registration is voluntary, the grade of coverage is not perfect. Those registered were easily identified as eligible for
Avh_YlvaNilsagard_K131008.indd 63 08-10-14 07.39.02

64
participation. Otherwise, local registries personal knowledge of the patient was crucial for identification.
The measures used in the studies reflect both objective and subjective perspectives of PwMS. Only the 12-item MS Walking Scale66 is patient-specific. The other measures used are symptom or task specific, and some of them have been recommended when evaluating PwMS: Fatigue Severity Scale28, the Clock Drawing Test8, 129, the 10m timed walk test165 and the Nine-Hole Peg Test.131 The ceiling effect found using the Berg Balance Scale is noteworthy when evaluating PwMS (EDSS 3.5-6.0), since the cut-off for predictive values was close to the maximum score (55/56p).
The chosen measures targeted Body Function and Structure, and Ac-tivities and Participation according to the ICF.173 The Berg Balance Scale, Timed Up and Go, Timed Up and Gocognitive and the Four Square Step Test are classified by their developers as being performance-based.12, 118, 139 They can be used in dif-ferent settings and environments i.e., rehabilitation units, acute care, Primary Health Care, the patient’s home, and so on. However, according to the definitions of the ICF,173 they do not measure performance but rather capacity.
Average daily steps taken may measure the level of physical activity, and for PwMS who walked either with or without a cane, the average daily steps measured by pedometer ranged from 1.190 to 19.473 with an average of 5.887 steps per day,41, 160 which is considered to be low active.159 Information of daily estimated walking distance was asked for in Study IV since it was believed that persons with a more active lifestyle were more exposed to the risk of falling. A more sedentary life style could, on the contrary, be a result of having experienced falls. Unfortunately, there were major difficulties for the PwMS to estimate their walking distance, which became apparent both from phone calls and the filled in forms. Thus, we had to exclude walking distance in the analyses. The difficulties in estimating one’s maximum walking distance are confirmed by others. Overestima-tion is reported at 43-47% and underestimation at 36-37%.36, 127 Ringel reported that only 21% of 100 PwMS made accurate estimations of the maximum walking distance.127 Créange et al. measured the correlation between patients’ estimation of their maximal walking distance and the distance measured by a global positioning system odometer. Although a statistically significant correlation was found at r=0.41, the error (objective minus subjective walking capacity) ranged from –6.419m to +3.950m.36 The capacity of walking also differs within the sub samples of PwMS according to their EDSS. PwMS with an EDSS score at 3.5-4.0 have been reported to have a maximum walking distance between 2.310m and 670m in a study by Creange et al., while the corresponding distance for those with EDSS 5.5-6.0 ranged from 1.850m to 468m.36 It is a challenge to find relevant and accurate measures for performance. Suggestions within the area of walking are, for exam-ple, pedometers.
Randomised controlled trials are preferred when evaluating interven-tions. Power calculations are performed to ensure the inclusion of a sufficient number of participants to answer the research questions. By predetermining the sample size, type II errors can be avoided. In Study I, it was not considered possi-ble to reach the estimated sample size if conducting a parallel group design, so a randomised crossover design was chosen instead. The within-subject comparison in crossover analyses is considered to be an advantage. It is important to establish
Avh_YlvaNilsagard_K131008.indd 64 08-10-14 07.39.02

65
the time for the washout period between interventions to eliminate a carry over effect. Seven days were chosen since it seemed most unlikely that any effect of the cooling garment could be sustained for this long and since it seemed practically possible for the participants to visit the Department of Physiotherapy at this in-terval.
Blinding of the patient and the person who measures the effect, as well as of the person that provides the intervention, is considered to be important so as not to transfer any expectations of the effect. To achieve successful blinding of the patients is often problematic when evaluating rehabilitative or physio-therapeutic interventions. It might also be difficult to identify and differentiate the different supposedly beneficial components within, for example, physiotherapy.172 Blinding of the patient was strived for in Study I105 by not giving any information with regard to whether or not the garment was cooled at the respective session. The success rate of the blinding could have been measured but was not since it was considered that it might possibly draw unnecessary attention to the different temperatures provided. The problem with obtaining accurate blinding of the pa-tients is a weakness of this study. A repeated measure design was used in Study II104 that investigated the 10m and 30m timed walk and Timed Up and Go. The timed walk tests were measured three times on each occasion, and the Timed Up and Go was measured twice since this was compatible with standard procedure in clinical practice. When measuring the time to walk a certain distance at either ‘self-selected speed’ or at ‘forced speed’, the actual choice of speed is left to the person performing the tests. It is possible that walking at ‘self-selected speed’ is a distinguishing feature in an individual and, therefore, unlikely to change easily. Timed walk tests are, however, commonly used for a vast number of diagnoses. The repeatability of the tests is important to be aware of since it guides both how many repetitions we chose to measure and how we interpret the results. The translation process of the 12-item MS Walking Scale followed the steps outlined by Streiner & Norman.146 The participants filled in the scale after having performed the Berg Balance Test, the Four Square Step Test and Timed Up and Gocognitive in a randomised order. By filling in the scale while super-vised by a physiotherapist, certain clarification or help with reading the questions could be given if needed.
The objective measures were chosen for different reasons. Together they cover several aspects of balance function. The Berg Balance Scale12 is com-monly used and familiar to physiotherapists working with persons with neuro-logical diagnoses in general. The Four Square Step Test40 is a rather new test that provides information of ability of rapidly stepping over obstacles. It does not re-quire extensive equipment and is quickly administered. The Timed Up and Gocogni-
tive139 requires divided attention and, therefore, seems highly interesting when evaluating PwMS. The measures and separate items or subcomponents of the measures seemed relevant when validating the 12-item MS Walking Scale. A longitudinal cohort study with prospectively collected falls was conducted to evaluate the predictive values of four measures and clinical vari-ables.108 The major criticism of the study is that no predetermined cut-off values were used. A power calculation was initially performed using the Berg Balance Scale with a 95% confidence interval and a cut-off at 45 of 56 points. It was be-
Avh_YlvaNilsagard_K131008.indd 65 08-10-14 07.39.03
66
lieved that 75% of the study population would have 45 points and 25% 46, and it was assumed that 20% with 46 points would fall at least once in 3 months. If 60% with 45 fell, there would be a need for 68 persons to reach 80% power. By considering a dropout rate of 20%, 82 PwMS were to be included. However, since defined cut-offs were not available when planning the study, we later decided to create cut-offs to maximise the sum of the sensitivity and the specificity. Thus, the analyses were not performed according to the initial power calculation. Instead, MS-specific cut-offs are presented for future research and clinical practise. It was believed that the impairments of Body Function and Struc-ture, as well as the limitations of Activities and Participation, were different in PwMS compared to previously investigated populations for whom the cut-offs had been established earlier. Cut-offs must be determined for separate popula-tions as reflected by the different cut-offs suggested for the Four Square Step Test: 12s for persons with vestibular disorders,171 15s for community-dwelling adults over 65 years,40 and 24s for persons with unilateral transtibial amputation.39 The cut-off we present at 55 points for the Berg Balance Scale is close to that reported as being most optimal (54 points) for community-dwelling people in a prospective study.102
Daily registration of accidental falls was asked for but it was not possible to control the compliance to this instruction. It is also possible that the participants interpreted the definition of ‘near fall incident’ in different ways de-spite the provided definitions. Actual falls are more likely to be interpreted in a similar way between the participants but the reporting of falls was also collected by self-registration. A qualitative content analysis design with mainly deductive approach was chosen to study factors perceived as related to accidental falls in PwMS.106 Using the ICF173 when designing the interview guide and coding the data governed the choice of using a deductive approach. A manifest analysis seemed appropriate due to the focus and perspective of the research question. A description of the obvious components of the communication was strived for, rather than interpret-ing the underlying meaning of the text. The use of a framework supplying stan-dardised operational definitions was believed to increase the reliability. Interviews seemed appropriate resulting in richer data compared to, for example, question-naires. The fact that the informants were aware that the interviewer was a physio-therapist might be seen as either strength or a weakness. It could be argued that persons reveal specific information to a physiotherapist depending on previous experience gained in earlier professional meetings. On the other hand, good knowledge of the symptoms when having MS could be advantageous. The com-puter software NVivo121 was used during the analytic procedure and this facili-tated moving back and forth from the entirety of the text to the categories.
An effort was made to relate the conducted studies to ICF in order to facilitate communication. The ICF is based on a biopsychosocial model and offers a standardised language and framework to describe health and health related is-sues.173 Differentiation between activities and participation was, however, not strived for during the analyses. To be able to do this, there must be an explicit purpose to enable the researcher to account for that aspect throughout the study. Our intention was to explore and describe factors perceived as related to acciden-tal falls rather than the consequences of experiencing accidental falls. Limitations
Avh_YlvaNilsagard_K131008.indd 66 08-10-14 07.39.03

67
in activities may or may not restrict participation depending on environmental factors such as the use or non-use of assistive device, which, in turn, can be re-lated to personal factors such as coping strategies. A limitation may restrict one person but not another person. Health can be seen as a successful identification and management of limits and possibilities of the different parts of ICF, and ICF can, thus, be an effective tool in Health Care. 6.4 Future research The effect of wearing a cooled Rehband® vests was tested with the persons rest-ing.105 From a physiotherapeutic perspective, it would be most interesting to evaluate the effects of using the vests in combination with exercise. It is possible that the exercise tolerance may be enhanced by using a cooling garment while training.
The Swedish translation of the 12-item MS Walking Scale107 could be modified and evaluated in persons with different neurological diagnoses, as was done with the original version by Holland et al.69 Further evaluation of validity and reliability could also be conducted both for the original scale66 and for the generic version.69
Since the cut-offs in Study IV108 were based on the same data as was used for the evaluation of the predictive abilities of the scales, further research is needed to verify them. Preferably, such studies should use prospectively collected data for falls to eliminate the risk of recall bias.
Measures capturing those factors not earlier targeted in MS popula-tion in relation to falls could be used in future clinical practice as well as when planning intervention studies of falls i.e., divided attention, muscular endurance, fatigue and heat-sensitivity. To develop and evaluate a fall-chart based on the obtained knowledge is challenging.
The results from Study IV108 and V106 reveal that several things may cause accidental falls. This calls for tailored interventions targeting several com-ponents of the ICF, which can be provided tentatively by professional expertise within MS-teams.
Avh_YlvaNilsagard_K131008.indd 67 08-10-14 07.39.03

Avh_YlvaNilsagard_K131008.indd 68 08-10-14 07.39.03

7. CONCLUSIONS Walking and balance ability are often affected when having MS, and these and other disabilities may be exaggerated by heat. For those experiencing heat- sensitivity, the use of Rehband® cooling garments may provide positive effects on everyday life.
In clinical praxis and for research purposes, the 10m and 30m timed walk and Timed Up and Go may be used to objectively measure walking ability. When evaluating PwMS (EDSS 3.0-6.5), it is sufficient to choose one of the meas-ures since the correlations are high; it is also sufficient to use just one attempt since the reproducibility is high. To establish a genuine change, a smallest percent-age difference at approximately –23% or +31% for the 10m timed walk and Timed Up and Go is needed. The smallest percentage difference needed to detect a genuine change in the 30m timed walk test differed depending on the severity of MS. With EDSS ≤4, the difference should exceed –14% or +17% compared to -38% or +60% with an EDSS >4.
The 12-item MS Walking Scale provides supplementary information regarding qualitative components in walking limitations that are common in PwMS. The scale is translated into Swedish and is available for clinical and re-search purposes.
Accidental falls and near fall incidents occur rather commonly in PwMS (EDSS 3.5-6.0). Several clinical variables and measures can contribute to identify those at risk of falling. Penetrating the need to use assistive devices, de-termining the EDSS score, testing proprioception and spasticity, and using objec-tive and subjective measures will provide help when identifying possible fallers.
Additional knowledge about what may cause accidental falls was achieved by data derived directly from those who fell. Attention was brought to the importance of factors such as divided attention, muscular endurance, fatigue and heat-sensitivity.
69

Avh_YlvaNilsagard_K131008.indd 70 08-10-14 07.39.03

71
8. IMPLICATIONS
There is some evidence that the use of a cooled Rehband® vest has positive ef-fects at group level. The vests are used in clinical practice for PwMS cared for at the hospital. The purpose may be to achieve a general effect of the cooling or to tolerate exercise better. Different vests are lent out for a test period to those that are interested in buying them. In Örebro County, a cooling garment is, unfortu-nately, not considered as a free assistive device.
In clinical practice, we have reduced the trials to one for the 10m timed walk and the Timed Up and Go. Values of smallest percentage differences needed to evaluate whether a genuine change is established. This information can be used to evaluate changes in performance and provide information used in the decision process for initiation medical or physiotherapeutic measures, and to evaluate treatments of medical and physiotherapeutic character. The Swedish translation of the 12-item MS Walking Scale is seen as a complement to objective measures when evaluating walking. The patient com-pletes the scale either at home before the visit to the clinic or during the visit. Checklists including predictive variables can be produced to supply more information regarding who is, and who is not, at risk of accidental falls. This improves the possibility for identifying those at risk. The additional informa-tion regarding factors and situations that cause or prevent falls can be used to survey the problem and when planning and conducting interventions.
Avh_YlvaNilsagard_K131008.indd 71 08-10-14 07.39.03

Avh_YlvaNilsagard_K131008.indd 72 08-10-14 07.39.04

9. ACKNOWLEDGEMENTS I would like to express my sincere gratitude to everyone who contributed in their own different way so that this thesis could be submitted. Special thanks are due to: All the people with MS who generously contributed their time to make this thesis possible. My supervisors who have been enormously engaged and perceptive in the work for this thesis. Throughout the journey, you have guided me through method discussions, manuscript writing and searching for grants. Your accessibility for both big and small questions has been fantastic! Your patience is admirable and your knowledge is greatly desired. You are all very good role models as supervi-sors. Associate Professor Lars-Gunnar Gunnarsson, Department of Occupational and Environmental Medicine, Örebro University Hospital, my main supervisor, for his great generosity with knowledge, time for supervision, constant encouragement and help in finding a workplace in which to carry out the work. Memorable Lars-Gunnar comment: “Give me the name and the personal identity numbers of the patients in question and I can fix my time to estimate the EDSS of those who are lacking it.” Associate Professor Eva Denison, Department of Caring and Public Health Sci-ences, Mälardalen University, my co-supervisor for lightning quick responses to all my questions, interesting and fruitful discussions and also extremely wise viewpoints viewed from an admirable holistic perspective. Memorable Eva com-ment: “It looks good but …..your tables seems to be numbered in a somewhat adventurous order.” Katrin Boström, Strategic planning officer, Department of Health and Medical Services, Örebro, method supervisor in Study V who, with an evident anchoring in clinical reality and a great interest in the stories of the informants, has guided me in the anguishes of the qualitative world. Memorable Katrin comment: “Of course it can be so… although… now you’re thinking like a physiotherapist again.” You who are within the mystical world of statistics for your consistently pleasant treatment and your efforts to assist with everything from messed up computer matrices to interpretation of data. Professor Lennart Bodin, Research and Development Unit, Statistics and Epide-miology, Örebro University Hospital, for your patient and tireless supervision in statistics as well as decisive views about planning and analysis of Study 1. Anders Magnuson, Research and Development Unit, Statistics and Epidemiology, Örebro University Hospital, for assistance with randomising in Studies I-III. Research Assistant, Ing-liss Bryngelsson, Department of Occupational and Environmental Medicine, Örebro University Hospital, for your help with the analyses for Study I. Scott Montgomery, Research and Development Unit, Statistics and Epidemiol-
73

74
ogy, for your viewpoints about the planning of Study IV as well as for assistance in translating the 12-item MS Walking Scale. Cecilia Lundholm, Department of Medical Epidemiology and Biostatistics, the Karolinska Institute whose co-authorship in Studies II and IV has contributed considerably to raising the quality of the studies. The physiotherapists who so willingly and competently contributed with partici-pants for the studies. Helena Tholin (Department for Physiotherapy, Örebro Uni-versity Hospital) och Malin Yderfors (NeuroRehab, Mälar Hospital, Eskilstuna) for collecting data for Studies I-IV. Emelie Blixt and Monica Svensson (Rehab Väst, Motala), Monica Johansson (Rehab Öst, Norrköping), and Erik Kristersson (Sahlgrenska University Hospital, Göteborg) for collection of data for Studies III-IV). Eivor Zaring, Marianne Bodström and Ulla Eriksson, Department for Physio-therapy, Örebro University Hospital, and Birgitta Axelsson Mälardalen Hospital for dealing with the cooling vests as well as collecting the study specific records in Study I. Without your positive attitude, the study wouldn’t have been possible to conduct. The Department of Occupational and Environmental Medicine, Örebro Univer-sity Hospital for the opportunity to have my own office while I was working on my thesis; an invaluable support which brought with it the possibility of concen-trated work without which the time to complete the thesis would have been lengthened considerably. A special thanks is due to Carl-Göran Ohlson for con-tinual happy and supportive cheering! Marie Hårding, former Director for the Department of Physiotherapy, Örebro University Hospital, for inspiring and visionary leadership as well as the encour-agement once upon a time to begin to walk the road leading to PhD studies. Åsa Andersson, Departmental Head of Physiotherapy, the Department of Geriat-rics, Örebro University Hospital who, during my time there made it easier for me to continue to follow the track towards my doctorate degree. Kerstin Bergström, Head of the Department of Physiotherapy, Örebro University Hospital who immediately connected to my idea of PhD studies and for all the practical help. Lillemor Nilsson, Department of Physiotherapy, who has taken care of my work-leave applications as well as my bills and research accounts. My fantastic colleagues and friends in the MS team: - you are an eternal source of inspiration! To work together with you is incredibly stimulating. Margareta Samuelsson, former Departmental Head and Björn Lindvall, current Head for the Department of Neurology, Örebro University Hospital for a positive attitude to the conducting of the studies, as well as Marie Lokander for assistance with dealing with the MS-register.
Avh_YlvaNils
ag
ard_K131008.indd 74 08-10-14 07.39.04

75
My research colleagues within physiotherapy: Ann Hammer, Anette Forsberg and Ulrika Einarsson, who knew exactly when encouragement was needed (manu-scripts turned down, broken photocopier, unbelievably filled diaries etc.) and in an absolutely special insightful way could give it. Birgitta Lindmark, Professor of Physiotherapy, Department of Neuroscience, Sec-tion of Physiotherapy, Uppsala University who through her personal engagement during previous studies has inspired continued research. Former and present physiotherapists in the Neuro Group at Örebro University Hospital. You are all, in different ways, a valuable part of my everyday life, which I really appreciate. Carita Hele Öist who, with her great knowledge, generously introduced me to working as a physiotherapist within neurology and gave me tools in my efforts to improve my clinical work. Kerstin Forsberg who was instrumental in getting me work as a private practising physiotherapist at Örebro Rehab Centre for a couple of years. All my colleagues in the Centre for Assessment of Medical Technology in Örebro (CAMTÖ), especially Georg Lohse and Christina Holmdahl. Margareta Landin, Medical Library, USÖ, for your quick, energetic and tireless assistance over the years! Margareta Möller, the Health Care Sciences Research Centre, Örebro, whose generous attitude facilitated the practical questions in Study V, and Maria Ek-holm who printed out the interviews. For financial support, the Research Committee (ÖLL), the Department of Physio-therapy (USÖ), CAMTÖ, LSR Neurology Section, LSR Memorial Fund and Nyckelfonden (Research Foundation). Also you who are all extra super special: My Söderström-Bergdahl for a lasting and warm friendship for over 43 years; and all of you others who I gratefully count as my friends. You know who you are! All my ”stable” friends and pony parents in whose company I always feel good, with whom I can gather strength and energy and who offer a lovely contrast to my work and my studies. My parents, Gull and Per Gunnvald, for a safe, secure and loving upbringing where everything is possible if you’re willing to work at it. You have facilitated and made my academic journey possible through your constant encouragement and through the tons of practical help that you have given with such generosity as a matter of course, which I value enormously!
Avh_YlvaNilsagard_K131008.indd 75 08-10-14 07.39.04

76
Karin, my beloved sister. I wish you were here! My everyday hero and life companion, Lars, who has read (?) all (?) my articles… Thank you for your full support when I had the yearning to learn more! Your ability to cope with a periodically tired and stressed wife is simply world-class! Our wonderful daughters Filippa and Wilma who just through being there has enriched my life in a totally indescribable way! If only you knew how glad and proud I am to be your mamma!
Avh_YlvaNilsagard_K131008.indd 76 08-10-14 07.39.04
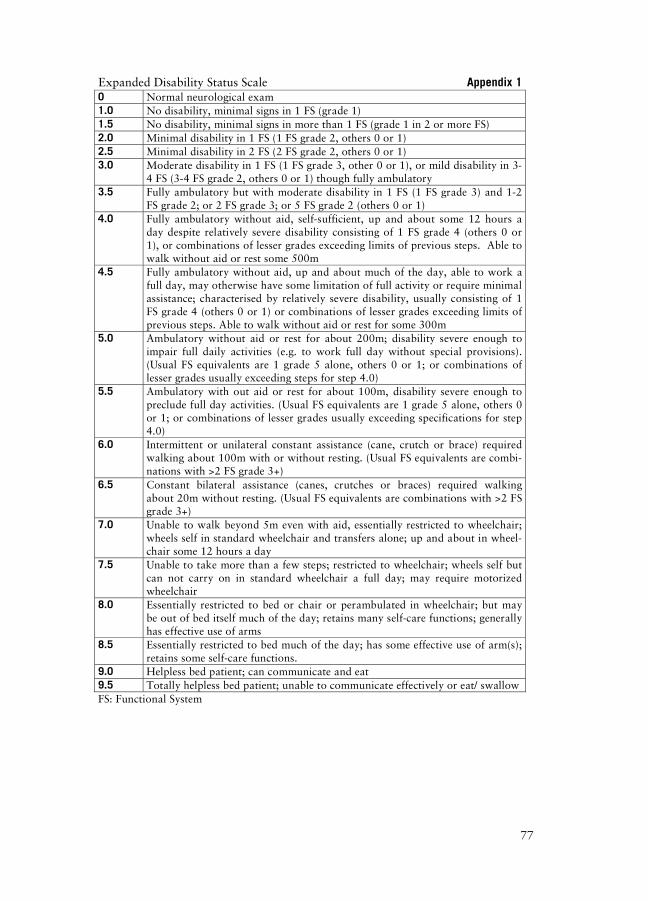
77
Expanded Disability Status Scale Appendix 1 0 Normal neurological exam 1.0 No disability, minimal signs in 1 FS (grade 1) 1.5 No disability, minimal signs in more than 1 FS (grade 1 in 2 or more FS) 2.0 Minimal disability in 1 FS (1 FS grade 2, others 0 or 1) 2.5 Minimal disability in 2 FS (2 FS grade 2, others 0 or 1) 3.0 Moderate disability in 1 FS (1 FS grade 3, other 0 or 1), or mild disability in 3-
4 FS (3-4 FS grade 2, others 0 or 1) though fully ambulatory 3.5 Fully ambulatory but with moderate disability in 1 FS (1 FS grade 3) and 1-2
FS grade 2; or 2 FS grade 3; or 5 FS grade 2 (others 0 or 1) 4.0 Fully ambulatory without aid, self-sufficient, up and about some 12 hours a
day despite relatively severe disability consisting of 1 FS grade 4 (others 0 or 1), or combinations of lesser grades exceeding limits of previous steps. Able to walk without aid or rest some 500m
4.5 Fully ambulatory without aid, up and about much of the day, able to work a full day, may otherwise have some limitation of full activity or require minimal assistance; characterised by relatively severe disability, usually consisting of 1 FS grade 4 (others 0 or 1) or combinations of lesser grades exceeding limits of previous steps. Able to walk without aid or rest for some 300m
5.0 Ambulatory without aid or rest for about 200m; disability severe enough to impair full daily activities (e.g. to work full day without special provisions). (Usual FS equivalents are 1 grade 5 alone, others 0 or 1; or combinations of lesser grades usually exceeding steps for step 4.0)
5.5 Ambulatory with out aid or rest for about 100m, disability severe enough to preclude full day activities. (Usual FS equivalents are 1 grade 5 alone, others 0 or 1; or combinations of lesser grades usually exceeding specifications for step 4.0)
6.0 Intermittent or unilateral constant assistance (cane, crutch or brace) required walking about 100m with or without resting. (Usual FS equivalents are combi-nations with >2 FS grade 3+)
6.5 Constant bilateral assistance (canes, crutches or braces) required walking about 20m without resting. (Usual FS equivalents are combinations with >2 FS grade 3+)
7.0 Unable to walk beyond 5m even with aid, essentially restricted to wheelchair; wheels self in standard wheelchair and transfers alone; up and about in wheel-chair some 12 hours a day
7.5 Unable to take more than a few steps; restricted to wheelchair; wheels self but can not carry on in standard wheelchair a full day; may require motorized wheelchair
8.0 Essentially restricted to bed or chair or perambulated in wheelchair; but may be out of bed itself much of the day; retains many self-care functions; generally has effective use of arms
8.5 Essentially restricted to bed much of the day; has some effective use of arm(s); retains some self-care functions.
9.0 Helpless bed patient; can communicate and eat 9.5 Totally helpless bed patient; unable to communicate effectively or eat/ swallow FS: Functional System
Avh_YlvaNilsagard_K131008.indd 77 08-10-14 07.39.05

7
Appendix 2 Berg Balance Scale Items ICF
codes Explanations to codes
1: ‘Stand up. Try not to use your hands as support’
d4103 To sit down and rise up from sitting
2: ‘Stand for 2 minutes without sup-port’
d4154 To maintain a standing position
3: ‘Sit with your arms crossed for 2 minutes’
d4153 To maintain a sitting position
4: ‘Sit down’ d4104 To take and leave standing position or change position from standing such as sit-ting.
5: ‘Move from one chair to another and back, use your hands as little as possible’
d4200 Transfer in sitting without changing the body position
6: ‘Close your eyes and stand still for 10 seconds’
b260, b235 d4154
Proprioceptive function Vestibular balance function Maintain standing position
7: ‘Put your feet together and stand still without support’
d415 To maintain a body position
8: ‘Lift your arm to 90 degrees. Ex-tend your fingers and lean forward as far as you can’
d4452 d4106
To use hands and arms to reach out, touch (and grip) something To adjust and change the distribution of body weight in standing
9: ‘Pick up the shoe on the floor in front of you’
d430 d4105
Lift and carry objects To lean the body downwards or sideways such as when bending and reaching for something
10: ‘Twist and look directly behind your left shoulder. Repeat to the right’
d4
Transfers
11: ‘Turn 360 degrees. Stop. Turn 360 degrees in the other direction’
d4 Transfers
12: ‘Put your feet alternately at the stool. Keep on until each foot touched the stool 4 times’
d4
Transfers
13: ‘Put one foot directly in front of the other. If you can’t place it there, try to put it so that your heel on the forward foot is in front of the other foot’s toes’
d4104 d415
To intake or leave standing position Maintain body position
14: ‘Stand on one leg as long as you are able to without support’
d4104 d415
To intake or leave standing position Maintain body position
8
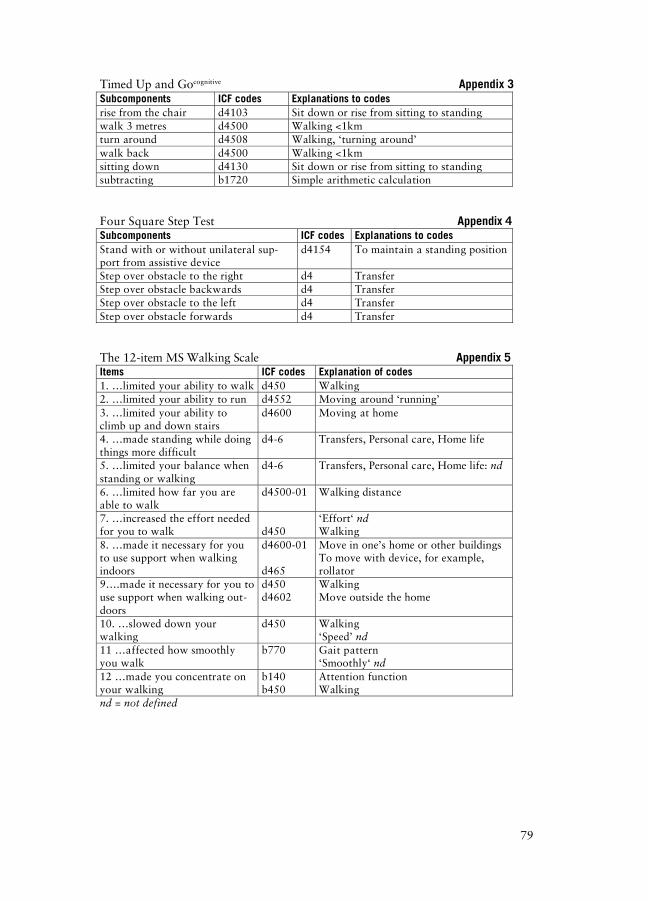
79
Timed Up and Gocognitive Appendix 3Subcomponents ICF codes Explanations to codes rise from the chair d4103 Sit down or rise from sitting to standing walk 3 metres d4500 Walking <1km turn around d4508 Walking, ‘turning around’ walk back d4500 Walking <1km sitting down d4130 Sit down or rise from sitting to standing subtracting b1720 Simple arithmetic calculation
Four Square Step Test Appendix 4Subcomponents ICF codes Explanations to codes Stand with or without unilateral sup-port from assistive device
d4154 To maintain a standing position
Step over obstacle to the right d4 Transfer Step over obstacle backwards d4 Transfer Step over obstacle to the left d4 Transfer Step over obstacle forwards d4 Transfer The 12-item MS Walking Scale Appendix 5Items ICF codes Explanation of codes 1. …limited your ability to walk d450 Walking 2. …limited your ability to run d4552 Moving around ‘running’ 3. …limited your ability to climb up and down stairs
d4600 Moving at home
4. …made standing while doing things more difficult
d4-6 Transfers, Personal care, Home life
5. …limited your balance when standing or walking
d4-6 Transfers, Personal care, Home life: nd
6. …limited how far you are able to walk
d4500-01 Walking distance
7. …increased the effort needed for you to walk
d450
‘Effort‘ nd Walking
8. …made it necessary for you to use support when walking indoors
d4600-01 d465
Move in one’s home or other buildings To move with device, for example, rollator
9….made it necessary for you to use support when walking out-doors
d450 d4602
Walking Move outside the home
10. …slowed down your walking
d450 Walking ‘Speed’ nd
11 …affected how smoothly you walk
b770 Gait pattern ‘Smoothly‘ nd
12 …made you concentrate on your walking
b140 b450
Attention function Walking
nd = not defined
Avh_YlvaNilsagard_K131008.indd 79 08-10-14 07.39.05

Avh_YlvaNilsagard_K131008.indd 80 08-10-14 07.39.06

81
10. REFERENCES 1. Albrecht H, Schwecht M, Pollmann W, Parag D, Erasmus LP, Konig N.
[Local ice application in therapy of kinetic limb ataxia. Clinical assess-ment of positive treatment effects in patients with multiple sclerosis]. Nervenarzt 1998;69(12):1066-73.
2. Altman DG. Practical statistics for medical research. London: Chapman and Hall; 1991.
3. Altman DG, Bland JM. Diagnostic tests 2: Predictive values. British Medical Journal 1994;309(6947):102.
4. Andersson AG, Kamwendo K, Seiger A, Appelros P. How to identify po-tential fallers in a stroke unit: validity indexes of 4 test methods. Journal of Rehabilitation Medicine 2006;38(3):186-91.
5. Ansari NN, Naghdi S, Moammeri H, Jalaie S. Ashworth Scales are unre-liable for the assessment of muscle spasticity. Physiotherapy Theory & Practice 2006;22(3):119-25.
6. Ashworth B. PRELIMINARY TRIAL OF CARISOPRODOL IN MULTIPLE SCLEROSIS. Practitioner 1964;192:540-2.
7. Auvinet B, Berrut G, Touzard C, Moutel L, Collet N, Chaleil D, Barrey E. Reference data for normal subjects obtained with an accelerometric de-vice. Gait and Posture 2002;16(2):124-34.
8. Barak Y, Lavie M, Achiron A. Screening for early cognitive impairment in multiple sclerosis patients using the clock drawing test. Journal of Clinical Neuroscience 2002;9(6):629-32.
9. Beckerman H, Roebroeck ME, Lankhorst GJ, Becher JG, Bezemer PD, Verbeek AL. Smallest real difference, a link between reproducibility and responsiveness. Quality of Life Research 2001;10(7):571-8.
10. Beenakker EA, Oparina TI, Hartgring A, Teelken A, Arutjunyan AV, De Keyser J. Cooling garment treatment in MS: clinical improvement and decrease in leukocyte NO production. Neurology 2001;57(5):892-4.
11. Benedetti MG, Piperno R, Simoncini L, Bonato P, Tonini A, Giannini S. Gait abnormalities in minimally impaired multiple sclerosis patients. Mul-tiple Sclerosis 1999;5(5):363-8.
12. Berg K, Wood-Dauphinee S, Williams JI, Gayton D. Measuring balance in the elderly: preliminary development of an instrument. Physiotherapy Canada 1989;41(6):304-11.
Avh_YlvaNilsagard_K131008.indd 81 08-10-14 07.39.06
82
13. Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Canadian Journal of Public Health. Revue Canadienne de Sante Publique 1992;83(2):S7-11.
14. Bland JM, Altman DG. Cronbach's alpha. British Medical Jorunal1997;314(7080):572.
15. Bland JM, Altman DG. Statistics notes. The odds ratio. British Medical Journal 2000;320(7247):1468.
16. Bloom LF, Lapierre NM, Wilson KG, Curran D, DeForge DA, Blackmer J. Concordance in goal setting between patients with multiple sclerosis and their rehabilitation team. American Journal of Physical Medicine and Re-habilitation 2006;85(10):807-13.
17. Bogle Thorbahn LD, Newton RA. Use of the Berg Balance Test to predict falls in elderly persons. Physical Therapy 1996;76(6):576-83.
18. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Physical Therapy 1987;67(2):206-7.
19. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. British Medical Jour-nal (Clinical Research Ed.) 1982;284(6329):1607-8.
20. Calabrese M, Atzori M, Bernardi V, Morra A, Romualdi C, Rinaldi L, McAuliffe MJ, Barachino L, Perini P, Fischl B, Battistin L, Gallo P. Corti-cal atrophy is relevant in multiple sclerosis at clinical onset. Journal of Neurology 2007;254(9):1212-20.
21. Callander M, Landtblom AM. A cluster of multiple sclerosis cases in Lysvik in the Swedish county of Varmland. Acta Neurologica Scandi-navica 2004;110(1):14-22.
22. Capello E, Gardella M, Leandri M, Abbruzzese G, Minatel C, Tartaglione A, Battaglia M, Mancardi GL. Lowering body temperature with a cooling suit as symptomatic treatment for thermosensitive multiple sclerosis pa-tients. Italian Journal of Neurological Sciences 1995;16(8):533-9.
23. Cattaneo D, De Nuzzo C, Fascia T, Macalli M, Pisoni I, Cardini R. Risks of falls in subjects with multiple sclerosis. Archives of Physical Medicine and Rehabilitation 2002;83(6):864-7.
24. Cattaneo D, Jonsdottir J, Repetti S. Reliability of four scales on balance disorders in persons with multiple sclerosis. Disability and Rehabilitation2007;29(24):1920-5.
25. Cattaneo D, Jonsdottir J, Zocchi M, Regola A. Effects of balance exer-cises on people with multiple sclerosis: a pilot study. Clinical Rehabilita-tion 2007;21(9):771-81.
Avh_YlvaNilsagard_K131008.indd 82 08-10-14 07.39.06
83
26. Cattaneo D, Marazzini F, Crippa A, Cardini R. Do static or dynamic AFOs improve balance? Clinical Rehabilitation 2002;16(8):894-9.
27. Cattaneo D, Regola A, Meotti M. Validity of six balance disorders scales in persons with multiple sclerosis. Disability and Rehabilitation2006;28(12):789-95.
28. Chipchase SY, Lincoln NB, Radford KA. Measuring fatigue in people with multiple sclerosis. Disability and Rehabilitation 2003;25(14):778-84.
29. Compston A, Confavreux C. The distribution of multiple sclerosis. In: McAlpine D, Matthews WB, editors. McAlpine's Multiple sclerosis. 2nd ed. Edinburgh: Churchill Livingstone; 1991. p. 71-111.
30. Compston A, Wekerle H. The genetics of multiple sclerosis. In: McAlpine D, Matthews WB, editors. McAlpine's Multiple sclerosis. 2nd ed. Edin-burgh: Churchill Livingstone; 1991. p. 113-81.
31. Condron JE, Hill KD. Reliability and validity of a dual-task force platform assessment of balance performance: effect of age, balance impairment, and cognitive task. Journal of the American Geriatrics Society2002;50(1):157-62.
32. Confavreux C, Vukusic S. Age at disability milestones in multiple sclero-sis. Brain 2006;129(Pt 3):595-605.
33. Costelloe L, Thompson A, Walsh C, Tubridy N, Hutchinson M. Long term clinical relevance of criteria for designating Multiple Sclerosis as benign after ten years of disease. Journal of Neurology, Neurosurgery and Psy-chiatry 2008.
34. Coyle PK, Krupp LB, Doscher C, Deng Z, Milazzo A. Clinical and immu-nological effects of cooling in multiple sclerosis. Journal of Neurologic Rehabilitation 1996;10(1):9-15.
35. Craig J, Young CA, Ennis M, Baker G, Boggild M. A randomised con-trolled trial comparing rehabilitation against standard therapy in multiple sclerosis patients receiving intravenous steroid treatment. Journal of Neurology, Neurosurgery and Psychiatry 2003;74(9):1225-30.
36. Creange A, Serre I, Levasseur M, Audry D, Nineb A, Boerio D, Moreau T, Maison P. Walking capacities in multiple sclerosis measured by global positioning system odometer. Multiple Sclerosis 2007;13(2):220-3.
37. Deeks JJ, Altman DG. Diagnostic tests 4: likelihood ratios. British Medi-cal Journal 2004;329(7458):168-9.
38. DeSousa EA, Albert RH, Kalman B. Cognitive impairments in multiple sclerosis: a review. American Journal of Alzheimer's Disease & Other Dementias 2002;17(1):23-9.
Avh_YlvaNilsagard_K131008.indd 83 08-10-14 07.39.06
84
39. Dite W, Connor HJ, Curtis HC. Clinical identification of multiple fall risk early after unilateral transtibial amputation. Archives of Physical Medicine and Rehabilitation 2007;88(1):109-14.
40. Dite W, Temple VA. A clinical test of stepping and change of direction to identify multiple falling older adults. Archives of Physical Medicine and Rehabilitation 2002;83(11):1566-71.
41. Doerksen SE, Motl RW, McAuley E. Environmental correlates of physical activity in multiple sclerosis: A cross-sectional study. International Jour-nal of Behavioural Nutrition and Physical Activity 2007;4:49.
42. Downe-Wamboldt B. Content analysis: method, applications, and issues. Health Care for Women International 1992;13(3):313-21.
43. Einarsson U, Gottberg K, Fredrikson S, Bergendal G, von Koch L, Holm-qvist LW. Multiple sclerosis in Stockholm County. A pilot study exploring the feasibility of assessment of impairment, disability and handicap by home visits. Clinical Rehabilitation 2003;17(3):294-303.
44. Einarsson U, Gottberg K, Fredrikson S, von Koch L, Holmqvist LW. Ac-tivities of daily living and social activities in people with multiple sclerosis in Stockholm County. Clinical Rehabilitation 2006;20(6):543-51.
45. Einarsson U, Gottberg K, von Koch L, Fredrikson S, Ytterberg C, Jin YP, Andersson M, Holmqvist LW. Cognitive and motor function in people with multiple sclerosis in Stockholm County. Multiple Sclerosis2006;12(3):340-53.
46. Einarsson U, Hillert J. Multipel skleros. In: FYSS 2008 : fysisk aktivitet i sjukdomsprevention och sjukdomsbehandling. Stockholm: Statens folk-hälsoinstitut; 2008. p. 424-40.
47. Ekdahl C, Jarnlo GB, Andersson SI. Standing balance in healthy sub-jects: evaluation of a quantitative test battery on a force platform. Scan-dinavian Journal of Rehabilitation Medicine 1989;21(4):187-95.
48. Feys P, Helsen W, Liu X, Mooren D, Albrecht H, Nuttin B, Ketelaer P. Effects of peripheral cooling on intention tremor in multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2005;76(3):373-9.
49. Finch E. Physical rehabilitation outcome measures : a guide to enhanced clinical decision making. 2. ed. Hamilton, Ontario: Decker; 2002.
50. Finlayson M, van Denend T. Experiencing the loss of mobility: perspec-tives of older adults with MS. Disability and Rehabilitation2003;25(20):1168-80.
51. Finlayson ML, Peterson EW, Cho CC. Risk factors for falling among people aged 45 to 90 years with multiple sclerosis. Archives of Physical Medicine and Rehabilitation 2006;87(9):1274-9.
Avh_YlvaNilsagard_K131008.indd 84 08-10-14 07.39.07
85
52. Fisher E, Lee JC, Nakamura K, Rudick RA. Gray matter atrophy in multi-ple sclerosis: A longitudinal study. Annals of Neurology 2008;25:25.
53. Fisk JD, Pontefract A, Ritvo PG, Archibald CJ, Murray TJ. The impact of fatigue on patients with multiple sclerosis. Canadian Journal of Neuro-logical Sciences 1994;21(1):9-14.
54. Flensner G, Lindencrona C. The cooling-suit: case studies of its influence on fatigue among eight individuals with multiple sclerosis. Journal of Ad-vanced Nursing 2002;37(6):541-50.
55. Ford HL, Gerry E, Johnson MH, Tennant A. Health status and quality of life of people with multiple sclerosis. Disability and Rehabilitation2001;23(12):516-21.
56. Forsberg A, Press R, Einarsson U, de Pedro-Cuesta J, Holmqvist LW. Disability and health-related quality of life in Guillain-Barre syndrome dur-ing the first two years after onset: a prospective study. Clinical Rehabili-tation 2005;19(8):900-9.
57. Freal JE, Kraft GH, Coryell JK. Symptomatic fatigue in multiple sclerosis. Archives of Physical Medicine and Rehabilitation 1984;65(3):135-8.
58. Frzovic D, Morris ME, Vowels L. Clinical tests of standing balance: per-formance of persons with multiple sclerosis. Archives of Physical Medi-cine and Rehabilitation 2000;81(2):215-21.
59. Graham JE, Ostir GV, Fisher SR, Ottenbacher KJ. Assessing walking speed in clinical research: a systematic review. Journal of Evaluation in Clinical Practice 2008.
60. Graham JE, Ostir GV, Kuo YF, Fisher SR, Ottenbacher KJ. Relationship between test methodology and mean velocity in timed walk tests: a re-view. Archives of Physical Medicine and Rehabilitation 2008;89(5):865-72.
61. Guthrie TC, Nelson DA. Influence of temperature changes on multiple sclerosis: critical review of mechanisms and research potential. Journal of the Neurological Sciences 1995;129(1):1-8.
62. Haigh R, Tennant A, Biering-Sorensen F, Grimby G, Marincek C, Phillips S, Ring H, Tesio L, Thonnard JL. The use of outcome measures in physical medicine and rehabilitation within Europe. Journal of Rehabilita-tion Medicine 2001;33(6):273-8.
63. Halkin A, Reichman J, Schwaber M, Paltiel O, Brezis M. Likelihood ra-tios: getting diagnostic testing into perspective. QJM 1998;91(4):247-58.
64. Hammer A, Nilsagard Y, Forsberg A, Pepa H, Skargren E, Oberg B. Evaluation of therapeutic riding (Sweden)/hippotherapy (United States). A single-subject experimental design study replicated in eleven patients
Avh_YlvaNilsagard_K131008.indd 85 08-10-14 07.39.07

86
with multiple sclerosis. Physiotherapy Theory & Practice 2005;21(1):51-77.
65. Hill KD, Bernhardt J, McGann AM, Maltese D, Berkovits D. A new test of dynamic standing balance for stroke patients: reliability, validity and comparison with healthy elderly. Physiotherapy Canada 1996;48(4):257-62.
66. Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ. Measuring the impact of MS on walking ability: the 12-Item MS Walking Scale (MSWS-12). Neurology 2003;60(1):31-6.
67. Hobart JC, Riazi A, Thompson AJ, Styles IM, Ingram W, Vickery PJ, Warner M, Fox PJ, Zajicek JP. Getting the measure of spasticity in multi-ple sclerosis: the Multiple Sclerosis Spasticity Scale (MSSS-88). Brain2006;129(Pt 1):224-34.
68. Holbrook M, Skilbeck CE. An activities index for use with stroke patients. Age and Ageing 1983;12(2):166-70.
69. Holland A, O'Connor RJ, Thompson AJ, Playford ED, Hobart JC. Talking the talk on walking the walk: a 12-item generic walking scale suitable for neurological conditions? Journal of Neurology 2006;253(12):1594-602.
70. Isaksson AK, Ahlstrom G, Gunnarsson LG. Quality of life and impairment in patients with multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2005;76(1):64-9.
71. Isles RC, Choy NL, Steer M, Nitz JC. Normal values of balance tests in women aged 20-80. Journal of the American Geriatrics Society2004;52(8):1367-72.
72. Johansson S, Ytterberg C, Claesson IM, Lindberg J, Hillert J, Andersson M, Widen Holmqvist L, von Koch L. High concurrent presence of disabil-ity in multiple sclerosis. Associations with perceived health. Journal of Neurology 2007;254(6):767-73.
73. Jonsson A, Andresen J, Storr L, Tscherning T, Soelberg Sorensen P, Ravnborg M. Cognitive impairment in newly diagnosed multiple sclerosis patients: a 4-year follow-up study. Journal of the Neurological Sciences2006;245(1-2):77-85.
74. Kaufman M, Moyer D, Norton J. The significant change for the Timed 25-foot Walk in the multiple sclerosis functional composite. Multiple Sclero-sis 2000;6(4):286-90.
75. Khan F, Pallant JF. Use of the International Classification of Functioning, Disability and Health (ICF) to identify preliminary comprehensive and brief core sets for multiple sclerosis. Disability and Rehabilitation2007;29(3):205-13.
Avh_YlvaNilsagard_K131008.indd 86 08-10-14 07.39.07
87
76. Khan F, Turner-Stokes L, Ng L, Kilpatrick T. Multidisciplinary rehabilita-tion for adults with multiple sclerosis. Cochrane Database of Systematic Reviews 2007(2):CD006036.
77. Kragt JJ, van der Linden FA, Nielsen JM, Uitdehaag BM, Polman CH. Clinical impact of 20% worsening on Timed 25-foot Walk and 9-hole Peg Test in multiple sclerosis. Multiple Sclerosis 2006;12(5):594-8.
78. Krupp LB. Fatigue in multiple sclerosis: definition, pathophysiology and treatment. CNS Drugs 2003;17(4):225-34.
79. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Archives of Neurology 1989;46(10):1121-3.
80. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an ex-panded disability status scale (EDSS). Neurology 1983;33(11):1444-52.
81. Landtblom AM, Flensner G, Callander M, Stawiarz L. [The Swedish MS registry points out an important clinical problem: physical and psycho-logical fatigue is a main symptom in multiple sclerosis]. Lakartidningen2004;101(44):3456-7.
82. Lassmann H, Wekerle H. The pathology of multiple sclerosis. In: McAlpine D, Matthews WB, editors. McAlpine's Multiple sclerosis. 2nd ed. Edinburgh: Churchill Livingstone; 1991. p. 557-99.
83. Lerdal A, Celius EG, Krupp L, Dahl AA. A prospective study of patterns of fatigue in multiple sclerosis. European Journal of Neurology2007;14(12):1338-43.
84. Lindmark B, Hamrin E. Evaluation of functional capacity after stroke as a basis for active intervention. Presentation of a modified chart for motor capacity assessment and its reliability. Scandinavian Journal of Rehabili-tation Medicine 1988;20(3):103-9.
85. Lindmark B, Hamrin E. Evaluation of functional capacity after stroke as a basis for active intervention. Validation of a modified chart for motor ca-pacity assessment. Scandinavian Journal of Rehabilitation Medicine1988;20(3):111-5.
86. Lundin-Olsson L, Nyberg L, Gustafson Y. Attention, frailty, and falls: the effect of a manual task on basic mobility. Journal of the American Geriat-rics Society 1998;46(6):758-61.
87. Martin CL, Phillips BA, Kilpatrick TJ, Butzkueven H, Tubridy N, McDonald E, Galea MP. Gait and balance impairment in early multiple sclerosis in the absence of clinical disability. Multiple Sclerosis 2006;12(5):620-8.
88. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the "get-up and go" test. Archives of Physical Medicine and Rehabilitation1986;67(6):387-9.
Avh_YlvaNilsagard_K131008.indd 87 08-10-14 07.39.08

88
89. McAlpine D, Matthews WB, editors. McAlpine's Multiple sclerosis. 2. ed. Edinburgh: Churchill Livingstone; 1991.
90. McAuley E, Morris KS, Doerksen SE, Motl RW, Liang H, White SM, Wo-jcicki TR, Rosengren K. Effects of change in physical activity on physical function limitations in older women: mediating roles of physical function performance and self-efficacy. Journal of the American Geriatrics Society2007;55(12):1967-73.
91. McDonald I, Compston A. The clinical feature and diagnosis of multiple sclerosis. In: McAlpine D, Matthews WB, editors. McAlpine's Multiple sclerosis. 2nd ed. Edinburgh: Churchill Livingstone; 1991. p. 287-346.
92. McDonald I, Compston A. The genetics of multiple sclerosis. In: McAlpine D, Mathiowetz WB, editors. McAlpine's Multiple sclerosis. 2nd
ed. Edinburgh: Churchill Livingstone; 1991. p. 113-81.
93. McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, McFarland HF, Paty DW, Polman CH, Reingold SC, Sandberg-Wollheim M, Sibley W, Thompson A, van den Noort S, Weinshenker BY, Wolinsky JS. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. An-nals of Neurology 2001;50(1):121-7.
94. McGuigan C, Hutchinson M. Confirming the validity and responsiveness of the Multiple Sclerosis Walking Scale-12 (MSWS-12). Neurology2004;62(11):2103-5.
95. Meyer-Heim A, Rothmaier M, Weder M, Kool J, Schenk P, Kesselring J. Advanced lightweight cooling-garment technology: functional improve-ments in thermosensitive patients with multiple sclerosis. Multiple Sclero-sis 2007;13(2):232-7.
96. Minden SL, Frankel D, Hadden L, Perloffp J, Srinath KP, Hoaglin DC. The Sonya Slifka Longitudinal Multiple Sclerosis Study: methods and sample characteristics. Multiple Sclerosis 2006;12(1):24-38.
97. Morris ME, Cantwell C, Vowels L, Dodd K. Changes in gait and fatigue from morning to afternoon in people with multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2002;72(3):361-5.
98. Morris S, Morris ME, Iansek R. Reliability of measurements obtained with the Timed "Up & Go" test in people with Parkinson disease. Physical Therapy 2001;81(2):810-8.
99. Motl RW, Arnett PA, Smith MM, Barwick FH, Ahlstrom B, Stover EJ. Worsening of symptoms is associated with lower physical activity levels in individuals with multiple sclerosis. Multiple Sclerosis 2008;14(1):140-2.
100. Motl RW, McAuley E, Snook EM. Physical activity and multiple sclerosis: a meta-analysis. Multiple Sclerosis 2005;11(4):459-63.
Avh_YlvaNilsagard_K131008.indd 88 08-10-14 07.39.08

89
101. Motl RW, Snook EM. Confirmation and extension of the validity of the Multiple Sclerosis Walking Scale-12 (MSWS-12). Journal of the Neuro-logical Sciences 2008;268(1-2):69-73.
102. Muir SW, Berg K, Chesworth B, Speechley M. Use of the Berg Balance Scale for predicting multiple falls in community-dwelling elderly people: a prospective study. Physical Therapy 2008;88(4):449-59; discussion 60-1.
103. Nagelkerke NJD. A note on a general definition of the coefficient of de-termination. Biometrika 1991;78(3):691-2.
104. Nilsagard Y, Lundholm C, Gunnarsson LG, Dcnison E. Clinical relevance using timed walk tests and 'timed up and go' testing in persons with mul-tiple sclerosis. Physiotherapy Research International 2007;12(2):105-14.
105. Nilsagård Y, Denison E, Gunnarsson L-G. Evaluation of a single session with cooling garment for persons with multiple sclerosis - a randomized trial. Disability and Rehabilitation: Assistive Technology, 2006;1(4):225 - 33.
106. Nilsagård Y, Denison E, Gunnarsson L-G, Boström K. Factors perceived as related to accidental falls in persons with Multiple Sclerosis. Disabilityand Rehabilitation [submitted 3 March 2008].
107. Nilsagård Y, Gunnarsson L, Denison E. Self-perceived limitations of gait in persons with multiple sclerosis. Advances in Physiotherapy2007;9(3):136-43.
108. Nilsagård Y, Lundholm C, Denison E, Gunnarsson L-G. Predicting acci-dental falls in persons with Multiple Sclerosis - a longitudinal study. Clini-cal Rehabilitation [accepted 25 May 2008].
109. Nuyens G, De Weerdt W, Ketelaer P, Feys H, De Wold L, Hantson L, Nieuwboer A, Spaepen A, Carton H. Inter-rater reliability of the Ashworth scale in multiple sclerosis. Clinical Rehabilitation 1994;8(4):286-92.
110. Oberg T, Karsznia A, Oberg K. Basic gait parameters: reference data for normal subjects, 10-79 years of age. Journal of Rehabilitation Research and Development 1993;30(2):210-23.
111. O'Connor A B, Schwid SR, Herrmann DN, Markman JD, Dworkin RH. Pain associated with multiple sclerosis: Systematic review and proposed classification. Pain 2007;8:8.
112. Paltamaa J, West H, Sarasoja T, Wikstrom J, Malkia E. Reliability of physical functioning measures in ambulatory subjects with MS. Physio-therapy Research International 2005;10(2):93-109.
113. Petajan JH, White AT. Recommendations for physical activity in patients with multiple sclerosis. Sports Medicine 1999;27(3):179-91.
Avh_YlvaNilsagard_K131008.indd 89 08-10-14 07.39.09

90
114. Peterson EW, Cho CC, Finlayson ML. Fear of falling and associated ac-tivity curtailment among middle aged and older adults with multiple scle-rosis. Multiple Sclerosis 2007;13(9):1168-75.
115. Peterson EW, Cho CC, von Koch L, Finlayson ML. Injurious falls among middle aged and older adults with multiple sclerosis. Archives of Physical Medicine and Rehabilitation 2008;89(6):1031-7.
116. Petrilli S, Durufle A, Nicolas B, Robineau S, Kerdoncuff V, Le Tallec H, Lassalle A, Gallien P. [Influence of temperature changes on clinical symptoms in multiple sclerosis: an epidemiologic study]. Annales de Ré-adaptation et de Médecine Physique 2004;47(5):204-8.
117. Pittock SJ, McClelland RL, Mayr WT, Jorgensen NW, Weinshenker BG, Noseworthy J, Rodriguez M. Clinical implications of benign multiple scle-rosis: a 20-year population-based follow-up study. Annals of Neurology2004;56(2):303-6.
118. Podsiadlo D, Richardson S. The timed "Up & Go": a test of basic func-tional mobility for frail elderly persons. Journal of the American Geriatrics Society 1991;39(2):142-8.
119. Polman CH, Thompson AJ, Murray TJ, McDonald WI. Multiple sclerosis : the guide to treatment and management. 5th ed. New York: Demos; 2001.
120. Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC, Johnson KP, Sibley WA, Silberberg DH, Tourtellotte WW. New diagnos-tic criteria for multiple sclerosis: guidelines for research protocols. Annals of Neurology 1983;13(3):227-31.
121. QSR International. NVivo 7 [computer software]; 2005.
122. Ragnarsdottir M. The concept of balance. Physiotherapy 1996;82(6):368-75.
123. Ramdharry GM, Marsden JF, Day BL, Thompson AJ. De-stabilizing and training effects of foot orthoses in multiple sclerosis. Multiple Sclerosis2006;12(2):219-26.
124. Ramsaransing GS, De Keyser J. Benign course in multiple sclerosis: a review. Acta Neurologica Scandinavica 2006;113(6):359-69.
125. Remelius JG, Hamill J, Kent-Braun J, Van Emmerik RE. Gait initiation in multiple sclerosis. Motor Control 2008;12(2):93-108.
126. Rietberg MB, Brooks D, Uitdehaag BM, Kwakkel G. Exercise therapy for multiple sclerosis. Cochrane Database of Systematic Reviews2005(1):CD003980.
Avh_YlvaNilsagard_K131008.indd 90 08-10-14 07.39.09

91
127. Ringel I, Zettl UK. Estimates of the walking distance in multiple sclerosis patients and their effect on the EDSS. Journal of Neurology2006;253(5):666-7.
128. Rizzo MA, Hadjimichael OC, Preiningerova J, Vollmer TL. Prevalence and treatment of spasticity reported by multiple sclerosis patients. Multi-ple Sclerosis 2004;10(5):589-95.
129. Rogers JM, Panegyres PK. Cognitive impairment in multiple sclerosis: evidence-based analysis and recommendations. Journal of Clinical Neu-roscience 2007;14(10):919-27.
130. Rosti-Otajarvi E, Hamalainen P, Koivisto K, Hokkanen L. The reliability of the MSFC and its components. Acta Neurologica Scandinavica2008;117(6):421-7.
131. Rudick R, Antel J, Confavreux C, Cutter G, Ellison G, Fischer J, Lublin F, Miller A, Petkau J, Rao S, Reingold S, Syndulko K, Thompson A, Wallenberg J, Weinshenker B, Willoughby E. Recommendations from the National Multiple Sclerosis Society Clinical Outcomes Assessment Task Force. Annals of Neurology 1997;42(3):379-82.
132. Schwartz JE, Jandorf L, Krupp LB. The measurement of fatigue: a new instrument. Journal of Psychosomatic Research 1993;37(7):753-62.
133. Schwid SR, Goodman AD, McDermott MP, Bever CF, Cook SD. Quanti-tative functional measures in MS: what is a reliable change? Neurology2002;58(8):1294-6.
134. Schwid SR, Petrie MD, Murray R, Leitch J, Bowen J, Alquist A, Pelligrino R, Roberts A, Harper-Bennie J, Milan MD, Guisado R, Luna B, Mont-gomery L, Lamparter R, Ku YT, Lee H, Goldwater D, Cutter G, Webbon B. A randomized controlled study of the acute and chronic effects of cool-ing therapy for MS. Neurology 2003;60(12):1955-60.
135. Sharrack B, Hughes RA, Soudain S, Dunn G. The psychometric proper-ties of clinical rating scales used in multiple sclerosis. Brain 1999;122 ( Pt 1):141-59.
136. Sheffler LR, Hennessey MT, Knutson JS, Naples GG, Chae J. Functional effect of an ankle foot orthosis on gait in multiple sclerosis: a pilot study. American Journal of Physical Medicine and Rehabilitation 2008;87(1):26-32.
137. Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing rater re-liability. Psychological Bulletin 1979;86(2):420-8.
138. Shulman KI. Clock-drawing: is it the ideal cognitive screening test? Inter-national Journal of Geriatric Psychiatry 2000;15(6):548-61.
Avh_YlvaNilsagard_K131008.indd 91 08-10-14 07.39.10
92
139. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Physical Therapy 2000;80(9):896-903.
140. Shumway-Cook A, Woollacott MH. Motor control : theory and practical applications. Baltimore: Williams & Wilkins; 1995.
141. Silkwood-Sherer D, Warmbier H. Effects of hippotherapy on postural sta-bility, in persons with multiple sclerosis: a pilot study. Journal of Neu-rologic Physical Therapy 2007;31(2):77-84.
142. Simmons RD, Ponsonby AL, van der Mei IA, Sheridan P. What affects your MS? Responses to an anonymous, Internet-based epidemiological survey. Multiple Sclerosis 2004;10(2):202-11.
143. Soyuer F, Mirza M, Erkorkmaz U. Balance performance in three forms of multiple sclerosis. Neurological Research 2006;28(5):555-62.
144. Stevenson VL, Playford ED. Rehabilitation and MS. International MS Journal 2007;14(3):85-92.
145. Stolze H, Klebe S, Zechlin C, Baecker C, Friege L, Deuschl G. Falls in frequent neurological diseases--prevalence, risk factors and aetiology. Journal of Neurology 2004;251(1):79-84.
146. Streiner DL, Norman GR. Health measurement scales : a practical guide to their development and use. 2. ed. Oxford: Oxford University Press; 1995.
147. Sundstrom P, Nystrom L, Forsgren L. Incidence (1988-97) and preva-lence (1997) of multiple sclerosis in Vasterbotten County in northern Sweden. Journal of Neurology, Neurosurgery and Psychiatry2003;74(1):29-32.
148. Sutliff MH, Naft JM, Stough DK, Lee JC, Arrigain SS, Bethoux FA. Effi-cacy and safety of a hip flexion assist orthosis in ambulatory multiple sclerosis patients. Archives of Physical Medicine and Rehabilitation2008;89(8):1611-7.
149. Swedish Multiple Sclerosis Registry. [Internet]. 2006 [cited 2007 Apr 26]. Available from: http://www.ms.reg.net.se.
150. Swedish Multiple Sclerosis Registry. [Internet]. 2007 [cited 2008 May 13]. Available from: http://www.ms.reg.net.se.
151. Swedish Road Administration. övergångsställen [Internet]. 2004 [cited 2005 9 Dec]. Available from:
http://www.vv.se/templates/page3____14290.aspx?quicksearchquery=VU-94.
152. Svenningsson A, Runmarker B, Lycke J, Andersen O. Incidence of MS during two fifteen-year periods in the Gothenburg region of Sweden. Acta Neurologica Scandinavica 1990;82(3):161-8.
Avh_YlvaNilsagard_K131008.indd 92 08-10-14 07.39.10

93
153. Swingler RJ, Compston DA. The morbidity of multiple sclerosis. Quarterly Journal of Medicine 1992;83(300):325-37.
154. Syndulko K, Jafari M, Woldanski A, Baumhefner RW, Tourtellotte WW. Effects of temperature in multiple sclerosis: a review of the literature. Journal of Neurologic Rehabilitation 1996;10(1):23-34.
155. Taylor NF, Dodd KJ, Shields N, Bruder A. Therapeutic exercise in physiotherapy practice is beneficial: a summary of systematic reviews 2002-2005. Australian Journal of Physiotherapy 2007;53(1):7-16.
156. Thoumie P, Lamotte D, Cantalloube S, Faucher M, Amarenco G. Motor determinants of gait in 100 ambulatory patients with multiple sclerosis. Multiple Sclerosis 2005;11(4):485-91.
157. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. New England Journal of Medicine1988;319(26):1701-7.
158. Tremlett H, Paty D, Devonshire V. Disability progression in multiple scle-rosis is slower than previously reported. Neurology 2006;66(2):172-7.
159. Tudor-Locke C, Bassett DR, Jr. How many steps/day are enough? Pre-liminary pedometer indices for public health. Sports Medicine2004;34(1):1-8.
160. Tudor-Locke C, Hatano Y, Pangrazi RP, Kang M. Revisiting "how many steps are enough?" Medicine and Science in Sports and Exercise2008;40(7 Suppl):S537-43.
161. Wade DT. Measurement in neurological rehabilitation. Oxford: Oxford Univ. Press; 1992.
162. Wade DT, Legh-Smith J, Langton Hewer R. Social activities after stroke: measurement and natural history using the Frenchay Activities Index. In-ternational Rehabilitation Medicine 1985;7(4):176-81.
163. van Hedel HJ, Wirz M, Dietz V. Assessing walking ability in subjects with spinal cord injury: validity and reliability of 3 walking tests. Archives of Physical Medicine and Rehabilitation 2005;86(2):190-6.
164. van Herk IE, Arendzen JH, Rispens P. Ten-metre walk, with or without a turn? Clinical Rehabilitation 1998;12(1):30-5.
165. Vaney C, Blaurock H, Gattlen B, Meisels C. Assessing mobility in multi-ple sclerosis using the Rivermead Mobility Index and gait speed. ClinicalRehabilitation 1996;10(3):216-26.
166. Waters RL, Mulroy S. The energy expenditure of normal and pathologic gait. Gait and Posture 1999;9(3):207-31.
Avh_YlvaNilsagard_K131008.indd 93 08-10-14 07.39.10

94
167. WCPT. World Confederation for Physical Therapy DoPT. [Internet]. Lon-don, UK; 2007 [cited 2008 2 June]. Available from: wcpt.org/policies/position/index.php.
168. Verghese J, Buschke H, Viola L, Katz M, Hall C, Kuslansky G, Lipton R. Validity of divided attention tasks in predicting falls in older individuals: a preliminary study. Journal of the American Geriatrics Society2002;50(9):1572-6.
169. White AT, Wilson TE, Davis SL, Petajan JH. Effect of precooling on physical performance in multiple sclerosis. Multiple Sclerosis2000;6(3):176-80.
170. White LJ, Castellano V. Exercise and brain health - implications for mul-tiple sclerosis : part 1 - neuronal growth factors. Sports Medicine2008;38(2):91-100.
171. Whitney SL, Marchetti GF, Morris LO, Sparto PJ. The reliability and valid-ity of the Four Square Step Test for people with balance deficits secon-dary to a vestibular disorder. Archives of Physical Medicine and Rehabili-tation 2007;88(1):99-104.
172. Wiles C. Physiotherapy and related activities in multiple sclerosis. Multi-ple Sclerosis 2008;14(7):863-71.
173. World Health Organization. International classification of functioning, dis-ability and health (ICF). Geneva: World Health Organization; 2001.
174. World Health Organization. [Internet]. 2008 [cited 2008 May 13]. Avail-able from: http://www.who.int/topics/rehabilitation/en/.
175. Vukusic S, Confavreux C. Prognostic factors for progression of disability in the secondary progressive phase of multiple sclerosis. Journal of the Neurological Sciences 2003;206(2):135-7.
176. Vukusic S, Confavreux C. Natural history of multiple sclerosis: risk fac-tors and prognostic indicators. Current Opinion in Neurology2007;20(3):269-74.
177. Ytterberg C, Johansson S, Holmqvist LW, Koch LV. Longitudinal varia-tions and predictors of increased perceived impact of multiple sclerosis, a two-year study. Journal of the Neurological Sciences 2008.
178. Zwarts MJ, Bleijenberg G, van Engelen BG. Clinical neurophysiology of fatigue. Clinical Neurophysiology 2008;119(1):2-10.
Avh_YlvaNilsagard_K131008.indd 94 08-10-14 07.39.11

![Walking-Working Surfaces.ppt [Read-Only] - …chemicalstrategies.org/.../walking_working_surfaces.pdf · OSHA Office of Training and Education 21 Summary Slips, trips, and falls constitute](https://static.fdocuments.net/doc/165x107/5b7754217f8b9ad3338ced38/walking-working-read-only-chemicalstrategiesorgwalkingworkingsurfacespdf.jpg)
















