VonDaedelzen Et Al 2000 Lancet MAP Fall and IUGR
6
Click here to load reader
Transcript of VonDaedelzen Et Al 2000 Lancet MAP Fall and IUGR

ARTICLES
THE LANCET • Vol 355 • January 8, 2000 87
Summary
Background We investigated the relation betweenfetoplacental growth and the use of oral antihypertensivemedication to treat mild-to-moderate pregnancy hypertension.
Methods The study design was a metaregression analysis ofpublished data from randomised controlled trials. Data froma paper that was regarded as an extreme statistical outlinerwere excluded from primary analyses. The change in (group)mean arterial pressure (MAP) from enrolment to delivery wascompared with indicators of fetoplacental growth.
Findings Greater mean difference in MAP withantihypertensive therapy was associated with the birth of ahigher proportion of small-for-gestational-age (SGA) infants(slope: 0·09 [SD 0·03], r2=0·48, p=0·006, 14 trials) andlower mean birthweight significant after exclusion of datafrom another paper regarded as an extreme statisticaloutliner (slope: �14·49 [6·98] r2=0·16, p=0·049, 27). Norelation with mean placental weight was seen (slope �2·01[1·62], r2=0·15, p=0·25, 11 trials).
Interpretation Treatment-induced falls in maternal bloodpressure may adversely affect fetal growth. Given the smallmaternal benefits that are likely to be derived from therapy,new data are urgently needed to elucidate the relativematernal and fetal benefits and risks of oral antihypertensivedrug treatment of mild-to-moderate pregnancy hypertension.
Lancet 2000; 355: 87–92See Commentary page xxx
Departments of Obstetrics and Gynaecology(P von Dadelszen MRCOG, M P Ornstein MD, L A Magee FRCPC),Medicine (Prof S B Bull PhD, Prof A G Logan FRCPC, L A Magee), andPaediatrics (Prof G Koren MD), University of Toronto, Toronto,Canada
Correspondence to: Dr L A Magee, 600 University Avenue, Suite428, Toronto, Ontario, Canada M5G 1X5(e-mail: [email protected])
IntroductionHypertension complicates 10% of pregnancies,1 and isassociated with an increase in maternal morbidity andmortality, as well as in perinatal mortality, intrauterinegrowth restriction, prematurity, and complications ofprematurity (such as respiratory distress syndrome). Theexcess perinatal morbidity and mortality reflect both thefetal syndrome of pre-eclampsia (ie, fetal distress,intrauterine growth restriction) and the consequences ofdelivery due to deteriorating maternal disease.
The goal of antihypertensive treatment is to improvematernal and perinatal outcomes. Historically, there hasbeen concern that lower blood pressure will reduce theperfusion of the intervillous space of the placenta, whichdoes not autoregulate its blood flow. This is an especialconcern in disorders that are associated with placentalabnormalities, either a primary defect in placentation2 (ie,pre-eclampsia) or accelerated placental ageing3 (eg,chronic hypertension), or both.
As part of a larger meta-analysis of randomisedcontrolled trials of antihypertensive therapy for mild-to-moderate pregnancy hypertension,4 we found thatthere was a statistical trend towards an increase in small-for-gestational-age (SGA) infants among womentaking antihypertensive therapy, compared with thosewho took placebo or no therapy (odds ratio 1·31[95% CI 0·98–1·75], n=15 trials, 1782 women),irrespective of both underlying type of hypertensionand drug class. This treatment effect was,however, inconsistent in both its magnitude anddirection. A previous Cochrane review5 attributed theheterogeneity to the results of the trial by Butters andcolleagues6 that compared long-term atenolol withplacebo for chronic hypertension in pregnancy, and founda large increase in SGA infants among atenolol-treatedpatients. In that small trial, there were twopostrandomisation withdrawals from the control group forsevere hypertension, leading some,5 but not all7
researchers to discount the study’s findings and itstherapeutic implications. Other explanations for theheterogeneity among treatment trials have not beenconsidered, including the magnitude of treatment-induced falls in maternal blood pressure.
Any effect of antihypertensive therapy on fetal growthis important to clarify, because the likely maternal benefits(ie, a decrease in episodes of blood pressure>160/100–110 mm Hg) are small. A reduction inintrauterine growth velocity could certainly lead topremature iatrogenic intervention during pregnancy(resulting in prematurity-related neonatal mortality andmorbidity), neurodevelopmental abnormalities (particularlyin low-birthweight babies8), and, possibly, cardiovascularhealth problems in later life.9
Fall in mean arterial pressure and fetal growth restriction inpregnancy hypertension: a meta-analysis
P von Dadelszen, M P Ornstein, S B Bull, A G Logan, G Koren, L A Magee
Articles

We assessed the relation between the magnitude ofantihypertensive-induced falls in maternal blood pressureand fetoplacental growth by metaregression analysis. Thecontroversial data from Butters and colleagues6 wereexcluded from the primary analyses. Our study was donewithin the context of a systematic review of randomisedcontrolled trials of oral antihypertensive drugs to treatmild-to-moderate pregnancy hypertension.
MethodsAs part of a larger meta-analysis,4 MEDLINE was searched forpublished randomised controlled trials (1966–97; key words:antihypertensive agents, bedrest, hospitalisation, plasma volumeexpansion, plasma substitutes, maternal mortality, pregnancy,pregnancy complications, perinatology, neonatology, infantnewborn diseases, infant, infant mortality), Excerpta Medica(1989-92) was consulted to identify Clinical and ExperimentalHypertension in Pregnancy (now Hypertension in Pregnancy), whichwas hand-searched for 1992–97. In addition, we went throughthe references of retrieved papers, and a standard toxicologytext.10 Titles, abstracts, or photocopies of the methods ofretrieved papers were screened and data abstractedindependently by two retrievers who corroborated their findings(ie, double-checked their data and resolved disagreement throughdiscussion). The most up-to-date data were abstracted fromduplicate publications.
Inclusion criteria were: English/French language, humanpregnancy, randomised controlled trial, orally administered drugor non-drug therapy for mild-to-moderate pregnancyhypertension, and assessment of the effectiveness of maternalantihypertensive therapy or perinatal risk, or both. Seeminglyinadequate methods of randomisation (eg, randomisation byalternate allocation) were included because most reports failed todescribe the method of randomisation adequately. Trials thatadministered either placebo/no therapy or antihypertensivetherapy to controls were included, because our interest was in thetreatment-induced change in mean arterial pressure (MAP).Abstracts were excluded. Abstracted data were entered into theReview Manager Software, version 3.1 (UK CochraneCollaboration, Oxford, UK).
Trials were divided into three types as follows: chronichypertension treated throughout pregnancy; mild-to-moderate late-onset hypertension (ie, pregnancy-induced hypertension, gestationalhypertension, or chronic hypertension treated only later inpregnancy) randomised to either treatment or placebo/no therapy;and late-onset hypertension randomised to one of two active agents.
MAP, defined as diastolic blood pressure + (pulse pressure/3),was chosen as an integrated measure of perfusion pressure. Whennot reported directly, MAP was calculated from reported systolicand diastolic blood pressure, the validity of this value waschecked by use of data from studies that reported all threemeasurements (ie, MAP, systolic and diastolic blood pressure).For each trial, the change in MAP from trial entry to the lastrecord in pregnancy was calculated from treatment values; thisdefined mean differences in MAP for each trial. Therefore, apositive difference in MAP reflected a greater fall in MAP in thetreatment group than in the control group. Most trials did notreport how blood pressure was measured, or specify theKorotkoff phase used to define diastolic blood pressure.
The severity of hypertension was defined by mean atenrolment: mild (MAP 107–113 mm Hg), moderate (MAP114–129 mm Hg) or severe (MAP �130 mm Hg). Both the doseand duration of therapy were found for the groups of treatedwomen and controls. Fetal outcomes of interest were: gestationalage at delivery, SGA infants (definition recorded), mean crudebirthweight, and mean placental weight.
For quantitative meta-analysis, the summary statistic was thePeto odds ratio (defined as [O-E]/V, where O is the observednumber of events, E is the expected number of events, and V isthe exact hypergeometric variance of O).11 Calculations werebased on the fixed-effects model, which assumed that between-trial variation in outcome was due to chance alone.
The primary objective of the metaregression was to estimatethe association of treatment-induced difference in MAP withmeasures of fetoplacental growth (ie, SGA infants, birthweight,and placental weight [by mean difference between groups]), byuse of summary data from each trial. Other risk factors for poorfetoplacental growth (type of hypertension, type ofantihypertensive therapy, and difference between groups intreatment duration) were of secondary interest but could not beincluded in the regression because of the limited number of trialsthat reported these endpoints. Nonetheless, before the meta-regression, colinearity between difference in MAP and each ofthese factors was assessed by non-parametric methods12 (ie,Spearman’s, Mann-Whitney U test, or Kruskal-Wallis test, asappropriate). Lack of evidence for colinearity was taken assupport that the coefficient for difference in MAP in theregression model would remain the same (or change only slightly)irrespective of what else was included in the model.12
The metaregression was done by weighted least-squaresregression. The relation between difference in MAP and each ofthe measures of fetoplacental growth was estimated by Pearson’sr2. A p value <0·05 was considered to be significant. For the SGAoutcome, the natural logarithm of the odds ratio for a given trialwas used as the dependent variable in the regression.11 For thecontinuous outcomes (ie, birthweight and placental weight), themean difference between treatment groups was used. Each studywas weighted in the metaregression to account for the fact thatthe trials were of different size, and therefore, study-specific effectmeasures (ie, natural logarithm of the odds ratio or meandifferences) were not all measured with equal precision.12 Theweights were determined as inverse of the variance of the study-specific outcome variable.12 We weighted each data point bymultiplying both the independent (ie, difference in MAP) and thedependent variable (eg, natural logarithm of the odds ratio for agiven trial for SGA infants) by the square root of the weight.
To be conservative,13 we omitted the data of Butters andcolleagues6 from the primary analysis. This trial was identified tobe a statistical outlier (by our work and by others). However, wealso did a sensitivity analysis in which data from the paper byButters and colleagues were included, and both non-parametric(Spearman’s)12 and parametric (Pearson’s r) methods were used.Secondary analyses included the relation between other riskfactors for poor fetoplacental growth and measures of that growth.
Results45 randomised controlled trials (41 publications)14–53 wereidentified that randomly allocated 3773 women withmild-to-moderate pregnancy hypertension to oral anti-hypertensive treatment. Seven trials (six publications)6, 14–18
randomised women with chronic hypertension to therapyor placebo/no therapy. A further 38 trials randomlyallocated women with late-onset hypertension toantihypertensive therapy or either placebo/no therapy (15trials),19–33 or other antihypertensive therapy (23 trials, 20publications).34–53
The drugs used in these trials were: methyldopa (doserange 500–4000 mg/day); �-blockers—acebutolol(400–1200 mg/day), atenolol (50–200 mg/day), labetalol(200–2400 mg/day), metoprolol (50–300 mg/day),oxprenolol (80–640 mg/day), pindolol (10–25 mg/day),propranolol (30–160 mg/day); thiazide diuretics—bendrofluazide (5–10 mg/day), chlorothiazide (1·0 g/day),hydrochlorthiazide (50 mg/day); ketanserin (20–80mg/day); hydralazine (25–200 mg/day); calcium-channelblockers—isradipine (5 mg/day), nicardipine (600mg/day), nifedipine (40–120 mg/day), verapamil(360–480 mg/day); and clonidine (150–1200 �g/day).Only the dosing rage was reported for each trial. For drugversus drug trials, �-blockers were always theexperimental intervention, and methyldopa was alwaysthe control or standard treatment.
ARTICLES
88 THE LANCET • Vol 355 • January 8, 2000

In terms of quality, 12 (27%) of 45 randomisedcontrolled trials described adequate allocation conceal-ment, 40 (89%) described successful randomisation bybalanced baseline maternal characteristics betweengroups, and 13 (29%) described adequate outcome-assessment masking. There was no apparent impact ofthese factors on trial outcomes (data not presented).
No collinearity was detected between mean differencein MAP and either mean difference in treatment durationof antihypertensive therapy (Spearman’s �=0·10, p=0·68,19 trials) or mean total duration of therapy in theexperimental group of antihypertensive versus placebo/notherapy trials (�=0·10, p=0·84, eight trials). The median(range) duration of therapy for all trials was 8·0(1·87–27·5) weeks, and all women were treated during thethird trimester.
Mean difference in MAP did not differ between trialsthat enrolled women with chronic hypertension
(5·34 [�2·00 to 19·00] mm Hg, six trials) or late-onsethypertension (0·70 [�13·00 to 15·76], p=0·27, 23 trials).There was a trend towards greater treatment-inducedmean difference in MAP among trials that administeredplacebo/no therapy to controls: �-blockers versusplacebo/no therapy (5·93 [1·33–7·99] mm Hg, seventrials), other antihypertensives versus placebo/no therapy(5·02 [�2·00 to 19·00] mm Hg, six trials), �-blockerversus other antihypertensive therapy (1·35 [�13·00 to15·76] mm Hg, 12 trials), or other antihypertensive versusother antihypertensive (–0·30 [�2·00 to 1·73], p=0·05,four trials).
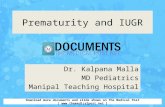
15 trials (13 publications)6,15,16,24,25,27,29,31,35,37,45,46,53 thatrandomly allocated treatment to 1587 women, describedboth mean blood pressure control and the proportion ofSGA infants. All but five trials defined SGA asbirthweight below 10th centile for gestational age, withappropriate tables: three trials (two publications16,27) didnot define SGA (but the author of one publication16 withtwo trials has routinely used below 10th centile forgestational age in other publications), one used below 5thcentile for gestational age,35 and another used below 250in Usher’s curve.45 Greater treatment-induced meandifference in MAP was associated with a higherproportion of SGA infants (figure 1); results are presentedby type of hypertension and treatment of control group forclarity. With the paper by Butters and colleagues6
excluded, the slope was 0·09 (SE 0·03; r2=0·48, p=0·006).With the inclusion of the paper by Butters andcolleagues,6 the slope of the linear-regression line was thesame by non-parametric analyses (0·09 [0·04], p=0·01) orparametric analyses (0·09 [0·04], p=0·065). The latterwas not significant, due to expansion of the SE of theregression coefficient.
Analysis according to the type of hypertension waspossible only for the late-onset hypertension groups, sincethere were only three chronic hypertension trials (apartfrom that of Butters and colleagues). The subgroupresults were similar to those overall, whether controls weretreated with placebo/no therapy (slope 0·12 [0·05],p=0·12, five trials) or antihypertensive drug therapy (slope0·21 [0·07], p=0·04, six trials). There was no associationbetween mean difference in duration of therapy and thelog odds of SGA infants (p=0·92, ten trials). Mean totaltreatment duration for treatment group ofantihypertensive treatment versus placebo/no therapytrials was also not significantly related to the log odds ofan SGA infant (p=0·30, seven trials).
27 trials (25 publications)14–16,24,25,27,29–32,35–37,39,41–43,46–48,50–53
randomly allocating treatment to 2305 women, describedboth mean blood pressure control and mean birthweight.Treatment-induced mean difference in MAP was notsignificantly associated with lower mean birthweight(figure 2). However, the data point from the trial byJannet and colleagues48 (which did not report theincidence of SGA infants) was an extreme statisticaloutlier, and was excluded from the sensitivity analysis. Bythe use of weighted non-parametric Spearman’sregression,12 a significant relation was demonstrated(slope:�14·49 [6·98], r2=0·16, p=0·049), such that overthe range of reported mean difference in MAP, a10 mm Hg fall in MAP was associated with a 145 gdecrease in birthweight. Just 16% of the variation in meanbirthweight between groups could be explained by thedifferential fall in MAP between treatment and controlgroups, and three trials (two18,22 in this analysis) reported
ARTICLES
THE LANCET • Vol 355 • January 8, 2000 89
3
Nat
ural
loga
rithm
odd
sra
tio (
SG
A)
2
1
0
–1
–2–5·0 –2·5 0 –2·5 5·0 7·5 10·0
Difference in MAP (mm Hg)
Chronic hypertension (drug vs placebo) Late-onset hypertension (drug vs placebo) Late-onset hypertension (drug vs drug)
Butters andcolleagues
500
250
0
Difference in MAP (mm Hg)–1
5·0–1
2·0–1
0·0–7
·5–5
·0–2
·5 0 2·5 5·0 7·510·0
12·515·0
17·5
–250
–500
–750
–1000
Chronic hypertension (drug vs placebo) Late-onset hypertension (drug vs placebo) Late-onset hypertension (drug vs drug)
Jannet andcolleagues
Butters andcolleagues
Mea
n di
ffer
ence
inbi
rthw
eigh
t (g
)
Figure 1: Relation between fall in MAP and proportion of SGAinfantsSpearman’s �=0·69 (p=0·007) without Butters and colleagues’ trial,6
�=0·64 (p=0·01) with that trial.
Figure 2: Relation between fall in MAP and low birthweightSpearman’s �=�0·46 (p=0·021) without both outlier trials;6,48 �=�0·31(p=0·122) with both outlier trials; �=0·44 (p=0·025) without trial ofJannet and colleagues;48 �=�0·30 (p=0·14) without trial of Butters andcolleagues.6

significant differences in gestational age at delivery. Withinclusion of Butters and colleagues’ trial6 (and exclusionof that of Jannet and colleagues48), the slope of the linear-regression line did not change by either non-parametricanalyses (�14·06 [9·18], p=0·02) or parametric analyses(�14·06 [9·18], p=0·14); however, inclusion of Jannetand colleagues (and exclusion of that of Butters andcolleagues) shows that the relation was dependent onomitting this trial (slope: �3·84 [6·54], p=0·14 [non-parametric], p=0·56 [parametric]). There are nomethodological problems in the trial of Jannet andcolleagues (women randomly assigned metoprolol ornicardipine) that could explain the marked disparity in itsresults.
Analysis by type of hypertension and antihypertensivetreatment showed non-significant inverse relationsbetween difference in MAP and mean birthweight:chronic hypertension (slope �18·60 [20·91], p=0·44, fivetrials), late-onset hypertension with placebo/no therapy ofcontrols (�16·69 [11·66], p=0·23, six trials), and late-onset hypertension with antihypertensive therapy ofcontrols (�17·47 [15·27], p=0·27, 14 trials). There wasno association between either mean difference in durationof therapy (p=0·60, 19 trials) or mean total duration oftherapy among the treatment group of drugs versusplacebo/no therapy trials (p=0·34, nine trials).
11 trials (ten publications)14,16,25,31,32,36,41,47,48,50 randomlyallocating treatment to 1119 women, reported both meanblood pressure control and mean placental weight. Nosignificant relation was seen between mean difference inMAP and mean placental weight (p=0·25, 11 trials).Subgroup analysis was possible only for the late-onsethypertension trials that compared two antihypertensivedrugs; no significant relation was found (p=0·47, sixtrials). There was no significant association between meandifference in duration of therapy and mean placentalweight (p=0·88, nine trials).
DiscussionBy meta-analysis, we investigated the apparentheterogeneity of the influence of oral antihypertensivetreatment on the odds ratio for delivering an SGA infant.Despite exclusion of the trial6 by Butters and colleagues,we found a relation between mean treatment-induced fallsin MAP and impaired fetal growth, as assessed bybirthweight corrected for gestational age (usually definedas <10th centile). This relation could not be explained bytype of hypertension, type of antihypertensive agent, ormean duration of therapy, since none of these were relatedto mean difference in MAP.
A puzzling finding is that antihypertensive therapy wasassociated with poor fetal growth, whereas the duration ofthat therapy was not. The mean difference in treatmentduration between groups was very small, and could notexplain the difference in fetal growth between groups,overall. However, even among placebo/no therapycontrolled trials, the mean total duration of therapy didnot relate to fetal growth; in this analysis, all women weretreated for a median of 10·3 weeks, and a minimum of 3·3weeks in the third trimester. Possibly antihypertensivetreatment during this period of greatest fetal growthvelocity is most important.
That antihypertensive therapy may adversely affectintrauterine fetal growth is a clinically important finding.The exclusion of the trial by Butters and colleagues fromthe analysis increases the clinical impact, given the
concerns expressed about this small trial withmethodological problems.
No relation between mean difference in MAP andcrude mean birthweight was seen, when we excluded onlythe trial by Butters and colleagues. However, two of thetrials in the analysis found a significant difference ingestational age at delivery, which is the most importantdeterminant of birthweight. In addition, the trial by Jannetand colleagues48 was a statistical outlier in finding a muchgreater difference in both fall in MAP and birthweightbetween groups, for reasons that were unexplained by trialdesign or type of antihypertensive (ie, nicardipine vsmetoprolol); with exclusion of this trial, we still showed asignificant relation between mean difference in MAP andmean birthweight, Over the reported range of fall in MAP,a 10 mm Hg fall was associated with a 145 g decrease inmean birthweight. However, this post-hoc analysis mustbe viewed with caution. No relation was seen betweenmean difference in MAP and mean placental weight.
Previously, �-blockers have been singled out as beingthe class of antihypertensive associated with an increasedrisk of poor fetal growth.54 However, the influence of MAPon the odds ratio for SGA infants appeared to beunrelated to the type of antihypertensive treatment. It isunlikely that different classes of antihypertensivemedication, with differing modes of pharmacologicalaction, would have consistent fetoplacental toxic effectsand, consequently, cause reduced fetal growth. Morelikely is that the observed effect on fetal growth wasrelated to uteroplacental perfusion abnormalities, but thisconjecture remains unproven.
Certainly, vasoactive medication could influence fetalgrowth. This could be a directly toxic pharmacologicaleffect, affecting metabolism within the fetoplacental unitor the transfer of nutrients across the placenta. Reducedperfusion pressure within the intervillous space couldsimilarly affect both the placenta and the fetussymmetrically, or, in the face of abnormal placentation,differentially; we could neither exclude nor confirm anassociated abnormality of placental growth, given that fallin MAP and placental weight were not related. Areduction in intervillous perfusion may also causesufficient stress to accelerate fetal pulmonary maturation.This mechanism would be consistent with the previouslyobserved treatment-induced decrease in respiratorydistress syndrome in a previously published meta-analysis,5 as well as our previous meta-analysis.4 Fetusessubjected to in-utero stress are less likely than thosewithout such stress to develop respiratory distresssyndrome,55,56 when delivered in good condition. Althoughthe observed reduction in intrauterine growth velocitymay be associated with improved neonatal outcome (ie,respiratory distress syndrome), there are concerns thatsuch an adverse intrauterine environment could bothincrease the risk of iatrogenic antenatal and intrapartuminterventions and lead to an excess of health problems inadulthood.9
This metaregression is limited in several ways. Thisanalysis was restricted to published randomised controlledtrials, augmented by results published only in theCochrane reviews after personal communication with thetrialists; this leaves analysis open to both publication biasand the file drawer effect. Not all trials reported thecovariates of interest (principally blood pressure) or allfetal outcomes of interest (principally, the proportion ofSGA infants). Use of averages of covariates measured in
ARTICLES
90 THE LANCET • Vol 355 • January 8, 2000

the individual patient (eg, difference in MAP) must bedone with caution because they may not adequatelyreflect important between-patient, within-trialdifferences.57 The practice of omitting data from trials thatare statistical outliers has been recommended by some13
but not all authorities.12 Finally, meta-analyses andmetaregressions are, by their nature, observational andretrospective. Therefore, they should only be consideredhypothesis-generating, and a prelude to a randomisedcontrolled trial.58
In summary, the implications of the observed impact ofthe treatment-induced fall in blood pressure on fetalgrowth must be considered seriously. Women are unlikelyto suffer from either acute or chronic deleterious effects,over the 9 months of pregnancy, from blood pressuresthat are below 170/110 mm Hg.59,60 At present, we cannotbe sure of the impact that antihypertensive treatment formild-to-moderate pregnancy hypertension may have onperinatal outcomes. New data from clinical trials areneeded.
ContributorsP von Dadelszen, M P Ornstein, and L A Magee were responsible for thedata abstraction and statistical analyses (meta-analysis and meta-regression). A G Logan and G Koren aided in the design of the stidy andacted as content experts in the fields of hypertension and perinatalmorbidity, respectively. S B Bull aided in the statistical analysis.P von Dadelszen and L A Magee wrote the manuscript.
AcknowledgmentsThis work was supported by the Physicians’ Services Incorporated and aneducational grant from the Department of Medicine, Mount SinaiHospital, Toronto, Canada. S B Bull and A G Logan are senior scientistsof the Samuel Lunenfeld Research Institute of Mount Sinai Hospital,Toronto. G Koren is the CIBC World Market Children’s MiracleFoundation Chair in child health research, Hospital for Sick Children,Toronto, Canada.
References1 National High Blood Pressure Education Program Working Group.
Report on high blood pressure in pregnancy. Am J Obstet Gynecol1990; 163: 1691–712.
2 Khong TY, de Wolf F, Robertson WB, Brosens I. Inadequatematernal vascular response to placentation in pregnancies complicatedby pre-eclampsia and by small-for-gestational-age infants. Br J ObstetGynaecol 1986; 93: 1049–59.
3 Zuspan FP, O’Shaughnessy RW. Maternal physiology and diseases:chronic hypertension in pregnancy. In: Pitkin RM, Zlatnik FJ, ed.Yearbook of obstetrics and gynecology. Chicago: Yearbook MedicalPublishers, 1979: 11.
4 Magee LA, Ornstein MP, von Dadelszen P. Clinical review:management of mild to moderate pregnancy hypertension. BMJ 1999;318: 1332–36.
5 Collins R, Duley L. Any antihypertensive therapy for pregnancyhypertension. In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP,eds. Pregnancy and childbirth module. In Cochrane Library review no04426, Cochrane Collaboration, April 21. Oxford: Update Software,1994.
6 Butters L, Kennedy S, Rubin PC. Atenolol in essential hypertensionduring pregnancy. BMJ 1990; 301: 587–89.
7 Redman CWG. Controlled trials of antihypertensive drugs inpregnancy. Am J Kidney Dis 1991; 17: 149–53.
8 Tyson JE, Kennedy K, Broyles S, Rosenfeld CR. The small forgestational age infant: accelerated or delayed pulmonary maturation?Increased or decreased survival? Pediatrics 1995; 95: 534–38.
9 Barker DJ. The Wellcome Lecture, 1994. The fetal origins of adultdisease. Proc R Soc Lond B Biol Sci 1995; 262: 37–43.
10 Briggs GG, Freeman RK, Yaffe SK, eds. Drugs in pregnancy andlactation: a reference guide to fetal and neonatal risk, 4th edn.Baltimore: Williams & Wilkins, 1994.
11 Fleiss JL. The statistical basis of meta-analysis. Stat Method Med Res1993; 2: 121–45.
12 Berlin JA, Antman EM. Advantages and limitations of metaanalyticregressions of clinical trials data. Online J Curr Clin Trials 1994;3 (document no 132).
13 Greenland S. A critical look at some popular meta-analytic methods.Am J Epidemiol 1994; 140: 290–301.
14 Sibai BM, Grossman RA, Grossman HG. Effects of diuretics in
plasma volume in pregnancies with long-term hypertension. Am JObstet Gynaecol 1984; 150: 831–35.
15 Arias F, Zamora J. Antihypertensive treatment and pregnancyoutcome in patients with mild chronic hypertension. Obstet Gynecol1978; 53: 489–94.
16 Sibai BM, Mabie WC, Shamsa F, Villar MA, Anderson GD. Acomparison of no medication versus methyldopa or labetalol inchronic hypertension during pregnancy. Am J Obstet Gynecol 1990;162: 960–67.
17 Weitz C, Khouzami V, Maxwell K, Johnson JWC. Treatment ofhypertension in pregnancy with methyldopa: a randomized doubleblind study. Int J Gynaecol Obstet 1987; 25: 35–40.
18 Steyn DW, Odendaal HJ. Randomised controlled trial of ketanserinand aspirin in prevention of pre-eclampsia. Lancet 1997; 350:1267–71.
19 Menzies DN. Controlled trial of chlorothiazide in treatment of earlypre-eclampsia. BMJ 1964; 1: 739–42.
20 Leather HM, Baker P, Humphreys DM, Chadd MA. A controlledtrial of hypotensive agents in hypertension in pregnancy. Lancet 1968;ii: 488–90.
21 Redman CWG, Beilin LJ, Bonnar J. Ounsted MK. Fetal outcome intrial of antihypertensive treatment in pregnancy. Lancet 1976; ii:753–56.
22 Rubin PC, Butters L, Clark DM, et al. Placebo-controlled trial ofatenolol in treatment of pregnancy-associated hypertension. Lancet1983; i: 431–34.
23 Cruickshank DJ, Robertson AA, Campbell DM, MacGillivray I.Maternal obstetric outcome measured in a randomised controlledstudy of labetalol in the treatment of hypertension in pregnancy.Clin Exp Hypertens Pregn 1991; B10: 333–44.
24 Pickles CJ, Symonds EM, Broughton Pipkin F. The fetal outcome in arandomized double-blind controlled trial of labetalol versus placebo inpregnancy-induced hypertension. Br J Obstet Gynaecol 1989; 96:38–43.
25 Sibai BM, Gonzales AR, Mabie WC, Moretti M. A comparison oflabetalol plus hospitalization versus hospitalization alone in themanagement of preeclampsia remote from term. Obstet Gynecol 1987;70: 323–27.
26 Walker JJ, Crooks A, Erwin L, Calder AA. Labetalol in pregnancy-induced hypertension: fetal and maternal effects. In Reily A,Symonds EM, eds, International Congress Series 591. Amsterdam:Excerpta Medica, 1982: 148–60.
27 Hogstedt S, Lindberg B, Lindeberg S, Ludviksson K. Effect ofmetoprolol on fetal heart rate patterns during pregnancy and delivery.Clin Exp Hypertens Pregn 1984; B3: 152.
28 Wichman K, Ryden G, Karlberg BE. A placebo controlled trial ofmetoprolol in the treatment of hypertension in pregnancy. Scand J LabInvest 1984; 169: 90–95.
29 Plouin PF, Breart G, Llado J, et al. A randomised comparison of earlywith consecutive use of antihypertensive drugs in the management ofpregnancy-induced hypertension. Br J Obstet Gynaecol 1990; 97:134–41.
30 Bott-Kanner G, Hirsch M, Friedman S, et al. Antihypertensivetherapy in the management of hypertension in pregnancy—a clinicaldouble-blind study of pindolol. Clin Exp Hypertens Pregn 1992; B11:207–20.
31 Sibai BM, Barton JR, Akl S, Sarinoglu C, Mercer BM. A randomizedprospective comparison of nifedipine and bed rest versus bed restalone in the management of preeclampsia remote from term. Am JObstet Gynecol 1992; 167: 879–84.
32 Wide-Swensson DH, Ingemarsson I, Lunell NO, et al. Calciumchannel blockade (isradipine) in treatment of hypertension inpregnancy: a randomized placebo-controlled study. Am J ObstetGynecol 1995; 173: 872–78.
33 Phippard AF, Fischer WE, Horvath JS, et al. Early blood pressurecontrol improves pregnancy outcome in primigravid women with mildhypertension. Med J Aust 1991; 154: 378–82.
34 Lardoux H, Blazquez G, Leperlier E, Gerard J. Essai overt,comparatif, avec tirage au sort pour le traitement de l’HTA gravidiquemoderée: methyldopa, acebutolol, labetalol. Arch Mal Coeur 1988; 81:(suppl HTA): 137–40.
35 Plouin PF, Breart G, Maillard F, Papiernik E, Relier JP, for theLabetalol Methyldopa Study group. Comparison of antihypertensiveefficacy and perinatal safety of labetalol and methyldopa in thetreatment of hypertension in pregnancy: a randomized controlled trial.Br J Obstet Gynaecol 1988; 95: 868–79.
36 Lamming GD, Broughton Pipkin F, Symonds EM. Comparison of thealpha and beta blocking drug, labetalol, and methyldopa in thetreatment of moderate and severe pregnancy-induced hypertension.Clin Exp Hypertens Pregn 1980; A2: 865–95.
37 Redman CWG.A controlled trial of the treatment of hypertension inpregnancy: labetalol compared with methyldopa. InternationalCongress Series 591 Amsterdam: Excerpta Medica 1978: 101–10.
ARTICLES
THE LANCET • Vol 355 • January 8, 2000 91

38 El-Qarmalawi AM, Morsy AH, Al-Fadly A, Obeid A, Hashem M.Labetalol vs methyldopa in the treatment of pregnancy-inducedhypertension. Int J Gynaecol Obstet 1995; 49: 125–30.
39 Oumachigui A, Verghese M, Balachander J. A comparative evaluationof metoprolol and methyldopa in the management of pregnancy-induced hypertension. Ind Heart J 1992; 44: 39–41.
40 Gallery EDM, Ross MR, Gyory AZ. Antihypertensive treatment inpregnancy: analysis of different responses to oxprenolol andmethyldopa. BMJ 1985; 291: 563–66.
41 Fidler J, Smith V, Fayers P, de Swiet M. Randomised controlledcomparative study of methyldopa and oxprenolol in treatment ofhypertension in pregnancy. BMJ 1983; 286: 1927–30.
42 Ellenbogen A, Jaschevatzky O, Davidson A, Anderman S,Grunstein S. Management of pregnancy-induced hypertension withpindolol: comparative study with methyldopa. Int J Gynaecol Onstet1986; 24: 3–7.
43 Livingstone I, Craswell PW, Bevan EB. Propranolol in pregnancy;three year prospective study. Clin Exp Hypertens Pregn 1983; B2:341–50.
44 Hjertberg R, Faxelius G, Lagercrantz H. Neonatal adaption inhypertensive pregnancy—a study of labetalol vs hydralazine treatment.J Perinat Med 1993; 21: 69–75.
45 Rosenfeld JB. Antihypertensive therapy in the management ofhypertensio in pregnancy—a clinical double-blind study of pindolol.Clin Exp Hypertens Pregn 1992; B11: 207–20.
46 Paran E, Holzberg G, Mazor M, Zmora E, Insler V. �-adrenergicblocking agents in the treatment of pregnancy-induced hypertension.Int J Pharmacol Ther 1995; 33: 119–23.
47 Montan S, Ingemarsson I, Marsal K, Sjoberg NO. Randomisedcontrolled trial of atenolol and pindolol in human pregnancy: effectson fetal haemodynamics. BMJ 1992; 304: 946–49.
48 Jannet D, Carbonne B, Sebban E, Milliez J. Nicardipine versusmetoprolol in the treatment of hypertension during pregnancy: arandomized comparative trial. Obstet Gynecol 1994; 84: 354–59.
49 Marlettini MG, Crippa S, Morelli-Labate AM, Contarini A,Orlandi C. Randomized comparison of calcium antagonists and
beta-blockers in the treatment of pregnancy-induced hypertension.Curr Ther Res 1990; 45: 684–94.
50 Montan S, Anandakumar C, Arulkumaran A, Ingemarsson I,Ratnam SS. Randomised controlled trial of methyldopa and israpidinein preeclampsia—effects on uteroplacental and fetal hemodynamics.J Perinat Med 1996; 24: 177–84.
51 Wide-Swensson D, Montan S, Arulkumaran S, Ingemarsson I,Ratnam SS. Effect of methyldopa and isradipine in fetal heart ratepattern assessed by computerized cardiotocography in humanpregnancy. Am J Obstet Gynecol 1993; 169: 1581–85.
52 Voto LS, Zin C, Neira J, Lapidus AM, Margulies M. Ketanserin versus�-methyldopa in the treatment of hypertension during pregnancy: apreliminary report. J Cardiovasc Pharmacol 1987; 10: S101–03.
53 Horvath JS, Phippard A, Korda A, Henderson-Smart DJ, Child A,Tiller DJ. Clonidine hydrochloride—a safe and effectiveantihypertensive agent in pregnancy. Obstetrics 1985; 66: 634–38.
54 Rey E, LeLorier J, Burgess E, Lange IR, Leduc L. Report of CanadianHypertension Society Consensus Conference: 3. Pharmacologictreatment of hypertensive disorders of pregnancy. CMAJ 1997; 157:1245–54.
55 Ley D, Wide-Swensson D, Lindroth M, Svenningsen N, Marsal K.Respiratory distress syndrome in infants with impaired intrauterinegrowth. Acta Paediatr 1997; 86: 1090–96.
56 Cooper PA, Sandler DL, Simchowitz ID, Galpin JS. Effects ofsuboptimal intra-uterine growth on preterm infants between 30 and 32weeks’ gestation. S Afr Med J 1997; 87: 314–18.
57 Lau J, Ioannidis JPA, Schmid CH. Quantitative synthesis in systemicreviews. Ann Intern Med 1997; 127: 820–26.
58 Borzak S, Ridker PM. Discordance between meta-analyses and large-scale randomized, controlled trials. Ann Intern Med 1995; 123: 873–77.
59 Sibai BH. Treatment of hypertension in pregnant women. N Engl JMed 1996; 335: 257–65.
60 Redman CWG. Hypertension in pregnancy. In: de Swiet M, ed.Medical disorders in obstetric practice, 3rd edn. Oxford: Blackwell,1995: 182–225.
ARTICLES
92 THE LANCET • Vol 355 • January 8, 2000