Vm Prolongada Jcc 2015
7
Click here to load reader
-
Upload
cesarcampos45 -
Category
Documents
-
view
216 -
download
0
description
VM prolongada caracteristicas.
Transcript of Vm Prolongada Jcc 2015
-
Prolonged mechanical ventilation in Canadian intensive care units:A national survey,,,,
Louise Rose, RN, PhD a,b,c,d,e,f,, Robert A. Fowler, MD, MSc e,f,h, Eddy Fan, MD, PhD g,h, Ian Fraser, MD, FRCP b,David Leasa, MD, FRCP i,j, Cathy Mawdsley, RN, MSc i, Cheryl Pedersen, MSc k,Gordon Rubenfeld, MD, MSc f,h, l, On behalf of the CANuVENT group 1
Mt. Sinai Hospital, Toronto, Ontario, Canada M5G 1X5d Li Ka Shing Knowledge Institute, St. Michaels Hospital,e Department of Critical Care, Sunnybrook Health Sciencef Sunnybrook Research Institute, Toronto, Ontario, Canadag Toronto General Hospital and University Health Networh Interdepartmental Division of Critical Care Medicine, Uni Department of Critical Care, London Health Sciences Cenj University of Western Ontariok Centre for Research on Inner City Health, Li Ka Shing Knl Trauma, Emergency, and Critical Care Program, Sunnybr
Journal of Critical Care 30 (2015) 2531
etation of data: all authors.rity of the work as awhole,
Contents lists available at ScienceDirect
Journal of Critical Care
j ourna l homepage: www. jcc journa l .org Competing interests: The authors have no nancial or nonnancial competing interests to declare. Corresponding author. Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, 155 College St, Rm 276, Toronto, Ontario, Canada, M5T IP8. Tel.: +1 416 978 3492;fax: +1 416 978 8222.from inception to published article. Previous presentation: This study was presented at the 2013 European Society of Intensive Medicine Annual Scientic Meeting in Paris. Author contributions: Conception and design of the study: L.R., R.F., E.F., I.F., D.L., C.M., and G.F. Acquisition: L.R. and C.P. Analysis and interprDrafting the article or revising it critically for important intellectual content: all authors. L.R. is the guarantor of the paper, taking responsibility for the integRehabilitationIntensive careProlonged mechanical ventilation
Results: Response rate was 215 (90%) of 238 units identifying 308 patients requiring PMV on the survey dayoccupying 11% of all Canadian ventilator-capable beds. Most units (81%) used individualized plans for bothweaning and mobilization. Weaning and mobilization protocols were available in 48% and 38% of units,respectively. Of those units with protocols, only 25% reported weaning guidance specic to PMV, and 11%reported mobilization content for PMV. Only 30% of units used specialized mobility equipment. Most unitsreferred to speech language pathologists (88%); use of communication technology was infrequent (11%). Only29% routinely referred to psychiatry/psychology, and 17% had formal discharge follow-up services.Conclusions: Prolonged mechanical ventilation patients occupied 11% of Canadian acute care ventilator bedcapacity. Most units preferred an individualized approach to weaning and mobilization with considerablevariation in weaning methods, protocol availability, access to specialized rehabilitation equipment,communication technology, psychiatry, and discharge follow-up.
2014 Elsevier Inc. All rights reserved.
Funding: The work was funded by a grant from the Partnerships for Health Systems Improvement competition of the Canadian Institutes of Health Research. Institution: This work was conducted at the Centre for Research on Inner City HealthSurvey Research Unit at St. Michaels Hospital and the University of Toronto.E-mail addresses: [email protected] (L. Rose(D. Leasa), [email protected] (C. Mawdsley)
1 Reshma Amin, The Hospital for Sick Children; MoFraser, Toronto East General Hospital; Robert Fowler, SuOntario; Judy King, University of Ottawa; David Leasa, LNonoyama, University of Toronto; Jeremy Road, ProvinSunnybrook Health Sciences Centre.
http://dx.doi.org/10.1016/j.jcrc.2014.07.0230883-9441/ 2014 Elsevier Inc. All rights reserved.April to November 2012. Weekly telephone and e-mail reminders were sent for 6 weeks.WeaningMobilizationa b s t r a c ta r t i c l e i n f o
Keywords:Mechanical ventilation
Background: We sought to describe prevalence and care practices for patients experiencing prolongedmechanical ventilation (PMV), dened as ventilation for 21 or more consecutive days and medical stability.Methods: We provided the survey to eligible units via secure Web link to a nominated unit champion fromToronto, Ontario, Canada M5B 1W8s Centre, Toronto, Ontario, Canada M4N 3M5M4N 3M5
k, Toronto, Ontario, Canada M5G 2C4iversity of Toronto, Toronto, Ontario, Canada, M5G 2C4tre, London, Ontario, Canada N6G 2V4
owledge Institute, St. Michaels Hospital, Toronto, Ontario, Canada M5B 1W8ook Health Sciences Centre, Toronto, Ontario, Canada M4N 3M5Lawrence S. Bloomberg Faculty of Nursing, University of Toronb Provincial Centre of Weaning Excellence/Prolonged Ventilationcto, Toronto, Ontario, Canada M5T 1P8Weaning Centre, Toronto East General Hospital, Toronto, Ontario, Canada M4C 3E7a), [email protected] (R.A. Fowler), [email protected] (E. Fan), [email protected] (I. Fraser), [email protected], [email protected] (C. Pedersen), [email protected] (G. Rubenfeld).nica Avendano, West Park Healthcare Centre; Sandra Dial, Montreal Chest Institute; Eddy Fan, Mount Sinai Hospital; Iannnybrook Health Sciences Centre; Roger Goldstein, West Park Healthcare Centre; Sherri Katz, Childrens Hospital of Easternondon Health Sciences Centre; Cathy Mawdsley, London Health Sciences Centre; Douglas McKim, Ottawa Hospital; Mikacial Respiratory Outreach Program, Vancouver Coastal Health; Louise Rose, University of Toronto; Gordon Rubenfeld,
-
26 L. Rose et al. / Journal of Critical Care 30 (2015) 25311. Introduction
Population aging, increasing morbidity, and scientic and techno-logical advances prolonging life mean that the number of patientsrequiring prolonged mechanical ventilation (PMV) continues to rise,resulting in insufcient intensive care unit (ICU) capacity to delivercare [1-3]. International reports indicate that PMV patients accountfor a minority, ranging from 4% to 30% depending on the denitionused, of all mechanically ventilated patients but consume 40% of ICUbed days and 50% of costs [1,4-6]. Substantial variability exists in thedenition of PMV, with ventilation duration ranging frommore than 6hours [7] to more than 29 days [8]. Another common denition istracheostomy placement and ventilation for 96 hours or more basedon diagnosis-related group coding [9]. Awareness of epidemiologicaltrends for mechanical ventilation is important as there are signicantnancial and resource implications for health care systems andorganizations. Costs to the health care system continue afterdischarge, with hospital readmission rates up to 70% reported [10].
The costs of PMV are not only nancial; long-term physical andpsychologic consequences impose substantial symptom burden andaffect patient and family quality of life [11-13]. Prolonged mechanicalventilation signals a need to change the primary focus of care fromacute resuscitation and stabilization to rehabilitation and long-termcare planning. However, the interprofessional rehabilitative approachneeded to reduce unnecessary prolongation of ventilator dependenceand to optimize mobility, communication, nutritional status, andpsychologic well-being is not consistent across ICUs [14].
No national Canadian data dene resource requirements and caredelivery for patients experiencing PMV. Our objectives were todescribe PMV prevalence and specic care practices includingweaning, mobilization, communication, swallowing, psychologicsupport, discharge barriers, and follow-up.
2. Methods
2.1. Study design and sample
We conducted an exploratory cross-sectional survey. Prolongedmechanical ventilation was dened as ventilation for 21 or moreconsecutive days and medical stability as recommended by theNational Association for Medical Direction of Respiratory Care [15].Medical stability was dened as no ongoing need for vasopressors/inotropes and resolution of the initial reason for ICU admission.Eligible units comprised ICUs, high-dependency units, weaningcenters, and other acute care units with ventilator capacity providingcare to PMV patients within the preceding 12 months. In theCanadian context, ICUs are categorized as level III, capable ofproviding the highest level of care, whereas level II and I ICUsgenerally provide support for patients with single organ failure orshort-term ventilation. High-dependency units serve as an interme-diate level of care either as a step up from the ward or a step downfrom the ICU. Weaning units either accept patients from within theinstitution they are located or may service as a regional referral unit.We excluded units with no invasive ventilation capacity, thoseproviding only short-term ventilation or long-term institutionalcare, and neonatal ICUs. We identied eligible units using an existinginventory of Canadian ICU capacity (Rob Fowler, 2011) and snowballreferrals. Units were screened by telephone to conrm eligibility,seek agreement for questionnaire completion, and to identify asurvey champion.
2.2. Questionnaire development
We contracted an independent survey unit (http://www.stmichaelshospital.com/crich/sru/) to manage questionnaire devel-opment, administration, and data collection. Informed by an elec-tronic database search (1990-2010) of literature relevant to PMV, 10team members representing medicine, nursing, respiratory, andphysical therapy generated questionnaire domains, items, andresponse formats, which were then iteratively rened. A Web-basedquestionnaire was programed using Snap Professional Software(snapsurveys.com, London, United Kingdom) and distributed to 7international PMV experts to pilot. Experts assessed for comprehen-siveness, redundancy, clarity, face validity, time to complete, andnumber of people to gather required information.
After further renement based on pilot testing, the nal question-naire comprised 8 domains: unit characteristics, patient characteris-tics on day survey completed and if available in a database during thepreceding 12months, clinical practices, equipment, funding and costs,liaison and transitions, patient follow-up, and perceptions of care. Tofacilitate recruitment in Francophone provinces, the questionnairewas professionally translated by Access Alliance.
2.3. Questionnaire administration
We provided the online questionnaire (see online supplement) viasecure Web link to the self-nominated survey champion from April toNovember 2012. Survey champions comprising unit directors, nursemanagers, physicians, senior registered nurses (RNs), or respiratorytherapists (RTs) were directed to complete a 1-time assessment ofpatient prevalence before survey return and to request assistancewith questionnaire completion from relevant interprofessional teammembers. Weekly telephone and e-mail reminders were sent for 6weeks, with a nal reminder in October. Telephone contact alsoenabled centers to clarify questionnaire items. The questionnaire wasadministered to blocks of 40 units to enable meticulous follow-up.
2.4. Ethical considerations
Research ethics boards of the University of Toronto (no. 26199)and St. Michaels Hospital approved the study. Participation wasvoluntary and consent implied by questionnaire return.
2.5. Statistical analyses
We examined results using descriptive statistics including theSharpiro-Wilk test for normality. We summarized continuousvariables using means and SDs or medians and interquartile rangesdepending on the data distribution and categorical variables usingfrequencies, proportions, and 95% condence intervals (CIs). Becauseof missing responses, denominators vary. We compared patientdemographics and clinical practices in ICUs with non-ICUs using 2
tests. Analyses were conducted using SPSS 22 (IBM, Armonk, NY).
3. Results
We screened 450 units of which 212 were ineligible. Reasons forineligibility comprised 101 (48%) of 212 had no invasive ventilationcapacity, 65 (31%) of 212 had only short-term ventilation capacity, 34(16%) of 212were PMV capable but had no patients in past 12months,11 (5%) of 212 were neonatal ICUs, and 1 (0.5%) of 212 was a long-term ventilation unit. We received 215 evaluable surveys (90%response rate) of which 203 (94%) contributed data on more than50% of items, and an additional 12 (6%) provided unit data only.
3.1. Unit characteristics
Most units (152/215, 71%)were level III [16] adult ICUswithmixedpopulations using a 1:1 nurse/patient ratio (Table 1). We identied3317 physical beds in participating units of which 2710 (82%) wereventilator capable, 2919 ICU beds with 2553 (87%) ventilator capable,and 398 non-ICU beds with 157 (39%) ventilator capable (Table 2).
-
Lightwriters (TobyChurchill, Cambridge, United Kingdom) wasinfrequent (23/201, 11%). Use of tracheostomy tubes and speakingvalves enabling vocalization was relatively common: 143 (71%) of 201units used Passy-Muir valves; 130 (65%) of 201, cufess tubes; 106(53%) of 201, fenestrated tubes; and 53 (26%) of 201, speaking tubes
Dieticians performed swallowing assessment in 56 (29%) of 195units and speech language pathologists in 175 (90%) of 193Techniques to assess safe swallowing comprised oral reex clinicaexamination (131/179, 73%), trial swallow with soft feed (130/17973%), videouoroscopic evaluation (modied barium swallow; 105/179, 59%), laryngeal reex clinical examination (101/179, 56%), triaswallow with colored liquid (96/179, 54%), and beroptic endoscopicevaluation (27/179, 15%). Nitrogen balance wasmeasured in 88 (51%)of 175 units, prealbumin in 124 (67%) of 184, and zinc porphyrins in43 (25%) of 174.
N600 beds 26 (12)Unit typeLevel III ICUb 152 (71)Level II and I ICUb 45 (21)Weaning unit 8 (4)Step-up/step-down unit 4 (2)Otherc 6 (3)Unit populationAdult only 170 (79)Combined adult and pediatric 28 (13)Pediatric only 17 (8)ICU specialtyd
MSICU 85 (43)MSTICU 61 (31)MSTICU + CS 21 (10)MSICU + CS 8 (4)CVS only 8 (4)MICU 5 (2)Othere 9 (4)Nurse/patient ratio in ICUs for all ventilated patients1:1 116 (59)1:2 58 (29)1:1 or 1:2 depending on acuity 17 (9)1:2 or 1:3 depending on acuity 3 (2)Otherf 3 (2)
MSICU, medical/surgical ICU; MSTICU, medical/surgical/trauma ICU; CS, cardiacsurgery; CVS, cardiovascular surgery; MICU, medical ICU; STICU, surgical trauma ICUCCU, coronary care unit; SICU, surgical ICU.Percentage may exceed 100 due to rounding.
a New Brunswick, Newfoundland, Nova Scotia, and Prince Edward Island.b Level III ICUs are capable of providing the highest level of care; level II and I ICUs
generally provide support for patients with single organ failure or short-term ventilationc Other comprises the following ventilator-capable units: adult acute medical uni
(4), pediatric acute medical unit (1), and spinal unit (1).d Not reported by 1 unit.e Other comprises STICU (3), MICU + CVS (2), neurosurgical ICU (2), CCU (4), SICU
(1), and burns ICU (1).f Other comprises 1:1 to 1:3 depending on acuity (1); ratio is usually 1:3, 1 intubated
and 2 nonintubated (1); not described (1).
27L. Rose et al. / Journal of Critical Care 30 (2015) 2531We identied 308 PMV patients occupying 11% of the 2710 ventilator-capable beds. Based on the 2011 Canadian census population [17], theestimated prevalence of PMV is 0.92/100 000 population. Of the 206sites providing PMV patient data on the survey day, 78 (38%) had nopatients, 87 (42%) had 1 to 2, 19 (14%) had 3 to 5, and 12 (6%) hadmore than 5 PMV patients.
3.2. Patient characteristics
Characteristics of PMV patients are shown in Table 3. Sepsis oracute lung injury as the primary reason for PMV were more commonin ICU patients, whereas neuromuscular disease and spinal cord injurywere more frequent indications in non-ICU patients. Rates of chronicobstructive pulmonary disease, neurologic insult, and ICU-acquiredweakness were similar as was age distribution. Patients with chronicneurologic conditions comprised 36% of the study population andoccupied 4% (95% CI, 3%-5%) of ventilator-capable ICU beds. Althoughmost patients (188/308, 61%) had received ventilation for 21 days ormore but less than 3 months, 55 (18%) of 308 had received ventilationfor 6 months or more. More patients had been ventilated for 6 monthsor more in non-ICUs (P=10.002). Of the 18 non-ICUs and 197 ICUs, 6(17%) and 39 (14%) maintained a database of PMV comprising 486patients admitted in the preceding 12 months: 419 (86%) of 486 fromICUs and 67 (14%) of 486 from non-ICUs.
3.3. Clinical practices
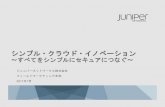
3.3.1. Weaning and mobilizationMost units reported using a variety of weaning methods for PMV
patients with progressive pressure support reduction being the mostcommon (165/198, 83%) (Fig. 1). Physicians determined weaningmethods in most units (179/194, 92%). Respiratory therapists and RNswere reported to inuence selection of weaning method in 146 (77%)of 190 and 58 (36%) of 162 sites, respectively. Eleven sites (6%)indicated that selection was dependent on patient characteristics; 4(2%) reported that weaning in their unit was guided by a protocol, butsome physicians elected not to use it; and 2 (1%) indicated thatweaning was a team approach. Few units (75/194, 39%) transitionedPMV patients to a different ventilator.
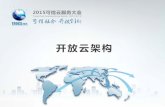
Most units (161/198, 81%) used individualized plans for PMVpatients for weaning and mobilization. Weaning protocolswere available in 95 (48%) of 198 units, although only 24 (25%) of95 reported protocolized guidance specic to PMV patients.Mobilization protocols were available in 75 (38%) of 198 units;only 22 (11%) of 75 units reported PMV-specic content. Airwayclearance strategies such as lung volume recruitment (breathstacking), manually assisted cough, and mechanical cough assistdevices were used in 134 (68%), 102 (52%), and 55 (28%) sites,respectively. Despite 141 (71%) of 198 sites indicating earlymobility was a priority commenced within 3 days of admission,only 60 (31%) of 196 units reported access to specialized mobilityequipment (Fig. 2). Availability of protocols with PMV-speciccontent was similar in ICUs and non-ICUs as was access tospecialized mobility equipment, mechanical cough assist devices,and use of lung volume recruitment. Manually assisted cough wasused more commonly in non-ICUs (P = .02). Only 18 (9%) of 191sites indicated that they used serial objective measures of musclestrength such as dynamometry or the Medical Research Councilscale for grading muscle strength.
3.3.2. Communication and swallowingMost units (179/201, 90%) used traditional communication tools
such as alphabet/word/picture/writing boards and had access tospeech language pathologists (172/196, 88%); use of other commu-nication technology such as iPads (Apple Inc, Cupertino, CA), DynaVoxcommunication augmentation devices (DynaVox, Pittsburgh, PA), and.
.l,
l
;
.tTable 1Site characteristics
Characteristic (n =215 ventilator-capable units) n (%)
ProvinceOntario 75 (35)Quebec 47 (22)British Columbia 25 (12)Atlantic provincesa 24 (11)Alberta 19 (9)Manitoba 13 (6)Saskatchewan 11 (5)Northwest Territories 1 (0.5)Hospital sizeb100 beds 22 (10)100-199 beds 46 (21)200-399 beds 82 (38)400-599 beds 39 (18)
-
3.3.3. Assessment and management of symptoms, psychologic issues, andpsychosocial issues
Use of objective anxiety measures for PMV patients was reported by44 (23%) of 192 units; however, 22 (50%) of 44 described delirium,
Table 2Bed numbers
n = 215 units Responding units Total physical beds Physical beds/unita Tot
Overall 215 3317 12 (8-20) 271ICUs 197 2919 12 (8-20) 255Non-ICUsc 18 398 25 (6-37) 157Pediatric 17 307 16 (9-24) 277ProvinceOntario 75 1312 16 (10-23) 115Quebec 47 684 11 (11-18) 648British Columbia 25 357 11 (9-20) 247Alberta 19 329 16 (10-22) 279Manitoba 13 215 12 (7-26) 96Saskatchewan 11 183 10 (6-36) 73Nova Scotia 9 79 8 (7-11) 65New Brunswick 7 69 8 (6-12) 67Newfoundland 6 67 10 (8-15) 65Prince Edward Island 2 18 9 (2-) 11Northwest Territories 1 4 - 2
a Median (interquartile range) beds per unit.b Number (%) of ventilator beds occupied by PMV patients on day of survey.c Non-ICUs include weaning centers, high-dependency units, and other acute care units
Table 3Patient characteristics
Characteristic, n (%) Overall(n = 308)
ICUs(n = 272)
Non-ICUsa
(n = 36)
Primary reason for PMVSepsis/multiorgan failure 61 (20) 58 (21) 3 (8)NMD 50 (16) 41 (15) 9 (25)COPD 37 (12) 32 (12) 5 (14)Neurologic insult 30 (10) 28 (10) 2 (6)ICU-acquired weakness 26 (8) 22 (8) 4 (11)Spinal cord injury 24 (8) 14 (5) 10 (28)ARDS/ALI 17 (6) 17 (6)
28 L. Rose et al. / Journal of Critical Care 30 (2015) 2531Central hypoventilation syndrome 8 (3) 7 (3) 1 (3)Postcardiac surgery 7 (2) 7 (3) Unknown 6 (2) 6 (2) Trauma 3 (1) 3 (1) Otherb 26 (8) 24 (9) 2 (6)
Not reported 13 (4) 13 (5) Age categories, y0-16 28 (9) 26 (10) 2 (6)17-29 16 (5) 13 (5) 3 (8)30-64 94 (31) 82 (30) 12 (22)65-79 120 (39) 105 (39) 15 (42)80 38 (12) 34 (13) 4 (11)Not reported 12 (4) 12 (4) Duration of ventilation21 d to b2 mo 142 (46) 132 (49) 10 (28)2 to b3 mo 46 (15) 39 (14) 7 (19)3 to b6 mo 42 (14) 36 (13) 6 (17)6 mo to b1 y 29 (9) 23 (8) 6 (17)1 y 26 (8) 19 (7) 7 (19)Unknown 2 (1) 2 (1) Not reported 21 (7) 21 (8)
NMD, neuromuscular disease; COPD, chronic obstructive pulmonary disease; ARDS,acute respiratory distress syndrome; ALI, acute lung injury.Percentage may exceed 100 due to rounding.
a Non-ICUs include weaning centers, high-dependency units, and other acute careunits capable of providing ventilation to medically stable patients.
b Other: chest wall restriction (2), post-transplantation (2), cardiomyopathy(2), pancreatitis (1), severe bronchopulmonary dysplasia (1), hypophosphatasia,tetralogy of fallot (1), severe congestive heart failure (1), chronic bronchiectasis(1), pneumonia (1), third degree heart block and severe delirium (1), mediastinal mass(1), persistent chylothorax (1), failure to thrive (1), thromboendarterectomy (1), burn(1), respiratory failure (1), necrotizing fasciitis (1), not dened (5).sedation, or pain assessment tools. Eight units used the Faces AnxietyScale [18]; 1 offered patients a choice of the Faces Anxiety Scale, State-Trait Anxiety Inventory [19], or a visual analog scale for anxiety [20]; and1 used the modied COMFORT Scale [21]. Eleven sites did not describethe tool used. An objective measure of dyspnea was used by 11 (6%) of193 units; 7 identied use of the modied Borg scale [22].
Psychiatric/psychologic/counseling services were available forpatients in 153 (77%) of 198 units and for families in 88 (45%) of195 units; 44 (29%) of 153 reported routinely referred PMV patients.Most units (146/196, 74%) held regular family meetings, although themost commonly reported frequency was on an as needed basis (66,45%). Weekly meetings were conducted by 42 units (29%); theremainder conducted biweekly, monthly, or bimonthly meetings.Access to palliative care specialists and ethicists was reported by 139(73%) of 191 and 131 (69%) of 191, respectively.
3.3.4. Discharge and follow-upTable 4 lists discharge options available to unit for PMV patients
requiring long-term ventilation. Most commonly perceived barriers totransition to either weaning or long-term ventilation units were lackof beds and prolongedwaiting lists (Fig. 3). Most commonly perceived
al ventilator-capable beds Ventilator-capable beds/unita PMV beds,b n (%, 95% CI)
0 10 (6-18) 308 (11, 10-13)3 10 (7-18) 272 (11, 10-12)
4 (4-10) 36 (23, 17-30)15 (8-23) 30 (11, 8-15)
7 15 (8-20) 148 (13, 11-15)10 (8-16) 69 (11, 9-13)9 (5-15) 20 (8, 5-12)
14 (8-21) 25 (9, 6-13)5 (4-10) 16 (17, 11-26)6 (4-10) 10 (14, 8-23)8 (5-10) 4 (6, 2-15)8 (6-12) 4 (6, 2-15)
10 (7-15) 11 (17, 10-28)6 (3-) 1 (9, 2-38)
capable of providing ventilation to medically stable patients.barriers to transition to the community were lack of a transitionprogram and insufcient paid caregivers and caregiver hours (Fig. 4).Formal follow-up services were reported by only 34 units (17%).Various models of follow-up were described, with the most frequent(12/34, 35%) conducted by a team composed of a physician, RN, andRT and within 1 month of hospital discharge.
4. Discussion
This is the rst study to document acute care bed occupancy bypatients ventilated for 21 days or more and considered medicallystable across Canada and to explore stated clinical practices specic toPMV patients. We found that patients who potentially could betransferred to an alternate care location occupied 11% of ventilator-capable acute care beds. Availability of protocols to guideweaning andmobilization was variable, with guidance specic to management ofthese complex clinical processes for PMV patients lacking. Unitsreported limited access to specialized equipment for rehabilitationincluding exercise, mobility, and communication devices; infrequentuse of objectivemeasures of anxiety and dyspnea; and limited referralto psychologic services. Lack of beds and long wait lists for alternatecare locations were frequent barriers to institutional transition; lack of
-
ts e
29L. Rose et al. / Journal of Critical Care 30 (2015) 2531transition programs and paid caregiver hours were frequent barriersto community discharge.
Comparison of our estimate of PMV prevalence with othercountries is problematic due to few multicenter or national studiesdescribing prevalence dened as 21 days or more and variation in thedenominator. However, our estimate of PMV prevalence appearslower than those previously reported in the United States or Taiwan,both countries with reimbursement plans that trigger transfer to alower acuity facility [23,24]. A 2006 point-prevalence survey of 58respiratory care managers in Massachusetts estimated PMV preva-lence of 3.7/100 000 population [25]. In 2004 and 2005, a Taiwanesenational administrative database identied 30 000 PMV patientsequivalent to 0.13% of the total population [24]. Lone and Walsh [5],again using an administrative database (2002-2006), reported thatPMV incidence in 3 Scottish hospitals was 6.3/100 ventilated patients.
We found that most units preferred an individualized approach toweaning and mobilization but considerable variation in weaningmethods, protocol availability, and access to specialized rehabilitationequipment. Consensus recommendations for PMV weaning [15]include integration of nonphysician-implemented protocols and useof daily, progressively lengthening, unassisted breathing trials.Evidence concerning weaning protocols suggests reduced ventilationduration [26]; however, few studies include patients ventilated for 21days or more. Jubran et al [27] recently demonstrated a substantialreduction in ventilation duration comparing 2 protocolized ap-proaches: pressure support ventilation and daily tracheostomy trials.
Early mobilization of ventilated patients increases the likelihood ofregaining functional independence [28]. Although mobilization in
Fig. 1. Weaning methods for patienpatients ventilated 21 days or more cannot be considered early, it isintegral to rehabilitation and frequently requires access to specialized
Fig. 2. Specialized mobility equipment (n = 198 units).equipment. Limited availability of mobilization protocols and equip-ment found in our survey indicates an area for institutional reviewand further knowledge translation. In addition, few units reportedusing objective measures for anxiety and dyspnea or routine referralto psychiatry despite anxiety, depression, and posttraumatic distresssyndrome being prevalent among PMV patients both during and afterweaning [29-31] and depressive symptoms being a risk factor forimpaired physical function [32].
Our data indicate that many units had limited discharge optionsfor patients requiring specialized weaning services or lower careintensity. Unlike other health care systems, in Canada, there are nopolicy initiatives or nancial incentives to transfer patients out of ICU,and facilities such as long-term acute care hospitals in the UnitedStates [23] and respiratory intermediate care units in Taiwan [33] andsome European countries [34] either do not exist or are extremelylimited. Such facilities have lower stafng ratios and have been shownto reduce readmission rates and health care costs [35]. In addition, forpatients requiring long-term ventilation, only half of our sample hadaccess to long-term care or community placements, and those unitswith access considered bed availability and prolonged wait lists assignicantbarriers. In contemporaneous surveys,we identied a further428 patients equivalent to 1.3/100 000 population in institutionsproviding long-term care [36] and 4334 individuals living at home andrequiring ventilation giving an estimated prevalence of 12.9/100 000population [37]. These ndings provide useful information for healthpolicy decision making and health care resource allocation.
Study strengths are rigorous development and meticulous surveyfollow-up resulting in a 90% response rate and data that are
xperiencing PMV (n = 198 units).representative of acute care units across Canada. Limitations arethose of surveys describing reported as opposed to actual clinicalpractices, whereby participants may provide an inaccurate reectionof actual practice based on inadequate knowledge or social desirabil-ity bias. Although we identied PMV prevalence, we were unable todetermine incidence as few units maintained a database withthis information.
Table 4Discharge options for PMV patients requiring ongoing ventilation
Care venues (n = 167) n (%)
Long-term ventilation unit external to institution 90 (54)Home ventilation training services 85 (51)Specialized weaning unit external to institution 52 (31)Community-assisted living placements 41 (25)Floor/ward with ventilator capacity within own institution 39 (23)Specialized weaning unit within own institution 19 (11)High-dependency/step-down unit with ventilator capacity 17 (10)
-
nati
30 L. Rose et al. / Journal of Critical Care 30 (2015) 2531Fig. 3. Perceived barriers to transition to alter5. Conclusions
Using a point-prevalence survey, we found that PMV patientsoccupied 11% of Canadian acute care ventilator bed capacity. Despiteevidence of their efcacy, availability of weaning and mobilityprotocols was variable, and guidance specic to PMV patients wasuncommon. Few centers used objective measures of anxiety anddyspnea, routinely referred to psychologic services, or had establishedfollow-up services. Limited discharge options and signicant dis-charge barriers require consideration in health policy decisionmakingand health care resource allocation.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.jcrc.2014.07.023.
References
[1] Carson SS. Outcomes of prolonged mechanical ventilation. Curr Opin Crit Care2006;12:40511.
[2] Zilberberg MD, de Wit M, Shorr AF. Accuracy of previous estimates for adultprolonged acute mechanical ventilation volume in 2020: Update using 2000-2008data. Crit Care Med 2012;40:1820.
[3] Cox CE, Carson SS, Holmes GM, Howard A, Carey TS. Increase in tracheostomy forprolonged mechanical ventilation in North Carolina, 1993-2002. Crit Care Med2004;32:221926.
[4] Iregui M, Malen J, Tutleur P, Lynch J, Holtzman M, Kollef M. Determinants ofoutcome for patients admitted to a long-term ventilator unit. South Med J 2002;95:3107.
Fig. 4. Perceived barriers to trave venues for weaning/long-term placement.[5] Lone N, Walsh T. Prolonged mechanical ventilation in critically ill patients:epidemiology, outcomes and modelling the potential cost consequences ofestablishing a regional weaning unit. Crit Care 2011;15:R102.
[6] Clark P, Lettieri C. Clinical model for predicting prolonged mechanical ventilation.J Crit Care 2013;28:880.e17.
[7] Faenza S, Ravaglia MS, Cimatti M, Dante A, Spedicato S, Labate AMM. Analysis ofthe causal factors of prolonged mechanical ventilation after orthotopic livertransplant. Transplant Proc 2006;38:11314.
[8] Gracey DR, Naessens HM, Krishan I, Marsh HM. Hospital and posthospital survivalin patients mechanically ventilated for more than 29 days. Chest 1992;101:2114.
[9] Cox CE, Carson SS, Govert JA, Chelluri L, Sanders GD. An economic evaluation ofprolonged mechanical ventilation. Crit Care Med 2007;35:191827.
[10] Douglas S, Daly B, Brennan P, Gordon N, Uthis P. Hospital readmission among long-term ventilator patients. Chest 2001;120:127886.
[11] Euteneuer S, Windisch W, Suchi S, Kohler D, Jones P, Schonhofer B. Health-relatedquality of life in patients with chronic respiratory failure after long-termmechanical ventilation. Respir Med 2006;100:47786.
[12] Nelson J, Meier D, Litke A, Natale D, Siegel R, Morrison R. The symptom burden ofchronic critical illness. Crit Care Med 2004;32:152734.
[13] Cox CE, Martinu T, Sathy SJ, Clay AS, Chia J, Gray AL, et al. Expectations andoutcomes of prolonged mechanical ventilation. Crit Care Med 2009;37:288894.
[14] Scheinhorn DJ, Hassenpug MS, Votto JJ, Chao DC, Epstein SK, Doig GS, et al.Ventilator-dependent survivors of catastrophic illness transferred to 23 long-term care hospitals for weaning from prolonged mechanical ventilation. Chest2007;131:7684.
[15] MacIntyre NR, Epstein SK, Carson S, Scheinhorn D, Christopher K, Muldoon S.Management of patients requiring prolonged mechanical ventilation: report of aNAMDRC consensus conference. Chest 2005;128:393754.
[16] Hill A, Fan E, Stewart T, Sibbald W, Nauenberg E, Lawless B, Bennett J, Martin C.Critical care services in Ontario: a survey-based assessment of current and futureresource needs. Can J Anaesth 2009;56:2917.
[17] Statistics Canada. 2011 Census prole. Accessed on 28th Feb 2014 from http://www12.statcan.gc.ca/census-recensement/index-eng.cfm.
[18] McKinley S, Coote K, Stein-Parbury J. Development and testing of a Faces Scale forthe assessment of anxiety in critically ill patients. J Adv Nurs 2003;41:739.
[19] Marteau T, Bekker H. The development of a six-item short-form of the statescale of the Spielberger State-Trait Anxiety Inventory (STAI). Br J Clin Psychol1992;31:3016.
nsition to the community.
-
[20] Davey H, Barratt A, Butow P, Deeks J. A one-item question with a Likert or VisualAnalog Scale adequatelly measured current anxiety. J Clin Epidemiol 2007;60:35660.
[21] Ambuel B, Hamlett K, Marx C, Blumer J. Assessing distress in pediatric intensivecare environments: the COMFORT scale. J Pediatr Psychol 1992;17:95109.
[22] Borg G. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14:37781.
[23] Cox C, Carson S. Medical and economic implications of prolonged mechanicalventilation and expedited post-acute care. Semin Respir Crit Care Med 2012;33:35761.
[24] Lu HM, Chen L, Wang JD, Hung MC, Lin MS, Yan YH, et al. Outcomes of prolongedmechanic ventilation: a discrimination model based on longitudinal healthinsurance and death certicate data. BMC Health Serv Res 2012;12:100.
[25] Divo MJ, Murray S, Cortopassi F, Celli BR. Prolonged mechanical ventilation inMassachusetts: the 2006 prevalence survey. Respir Care 2010;55:16938.
[26] Blackwood B, Alderdice F, Burns K, Cardwell C, Lavery G, O'Halloran P. Protocolizedversusnon-protocolizedweaning for reducing thedurationofmechanical ventilationin critically ill adult patients. Cochrane Database Syst Rev 2010;5:CD006904.
[27] Jubran A, Grant B, Duffner L, Collins E, Lanuza D, Hoffman L, et al. Effect of pressuresupport vs unassisted breathing through a tracheostomy collar on weaningduration in patients requiring prolonged mechanical ventilation: a randomizedtrial. JAMA 2013;309:6717.
[28] Schweickert W, Pohlman M, Pohlman A, Nigos C, Pawlik A, Esbrook C, et al. Earlyphysical and occupational therapy in mechanically ventilated, critically illpatients: a randomised controlled trial. Lancet 2009;373:187482.
[29] Jubran A, Lawm G, Kelly J, Duffner L, Duffner L, Gungor G, et al. Depressivedisorders during weaning from prolonged mechanical ventilation. Intensive CareMed 2010;36:82835.
[30] Jubran A, Lawm G, Duffner L, Collins E, Lanuza D, Hoffman L, et al. Post-traumaticstress disorder after weaning from prolonged mechanical ventilation. IntensiveCare Med 2010;36:20307.
[31] Tate J, Devito Dabbs A, Hoffman L, Milbrandt E, Happ MB. Anxiety and agitation inmechanically ventilated patients. Qual Health Res 2012;22:15773.
[32] Bienvenu O, Colantuoni E, Mendez-Tellez P, Dinglas V, Shanholtz C, Husain N, et al.Depressive symptoms and impaired physical function after acute lung injury: a 2-year longitudinal study. Am J Respir Crit Care Med 2012;185:51724.
[33] Liu C, Chu C, Chen W, Cheng W, Shih C, Tsai Y, et al. Impact of Taiwan's IntegratedProspective Payment Program on prolonged mechanical ventilation: a six-yearnationwide study. Respir Care 2013;58:67682.
[34] Corrado A, Roussos C, Ambrosino N, Confalonieri M, Cuvelier A, Elliott M, et al.Respiratory intermediate care units: a European survey. Eur Respir J 2002;20:134350.
[35] Kahn JM,Werner RM, David G, Ten Have TR, Benson NM, Asch DA. Effectiveness oflong-term acute care hospitalization in elderly patients with chronic criticalillness. Med Care 2013;51:410.
[36] Rose L, Leasa D, McKim D, NonoyamaM, AvendanoM, Goldstein R for the CANuVENTgroup. Provision of institutional care for long-termmechanical ventilation in Canada: anational survey. Am J Respir Crit Care Med 2014;189:A5372.
[37] L. Rose, D.McKim, S. Katz, D. Leasa,M.Nonoyama, C. Pedersen, et al., HomeMechanicalVentilation in Canada: A National Survey. Respiratory Care [under review]
31L. Rose et al. / Journal of Critical Care 30 (2015) 2531
Prolonged mechanical ventilation in Canadian intensive care units: A national survey1. Introduction2. Methods2.1. Study design and sample2.2. Questionnaire development2.3. Questionnaire administration2.4. Ethical considerations2.5. Statistical analyses
3. Results3.1. Unit characteristics3.2. Patient characteristics3.3. Clinical practices3.3.1. Weaning and mobilization3.3.2. Communication and swallowing3.3.3. Assessment and management of symptoms, psychologic issues, and psychosocial issues3.3.4. Discharge and follow-up
4. Discussion5. ConclusionsAppendix A. Supplementary dataReferences