
· Web viewFluid-filled monitoring systems consist of a catheter connected to a transducer via...
16
1 Hemodynamics Review Packet 2014 Hemodynamics Review 2013-2014
Transcript of · Web viewFluid-filled monitoring systems consist of a catheter connected to a transducer via...

1
Hemodynamics Review Packet
2014
Hemodynamics Review 2013-2014

2
Cardiac Cycle
Watch video on youtube.com:
Hemodynamic Monitoring Concepts by SuCollege
The Hemodynamic Profile
Afterload
Preload
Contractility
Pressures equalize between atria & ventricles at end diastole
Pressures equalize between RV & PA, as well as LA & Aorta at peak systole

3
Cardiac Output = the amount of blood ejected from the heart each minute. Cardiac Index is CO/BSA.
Stroke Volume = the volume of blood ejected from the ventricle at each beat of the heart.
CO = HR X SV
Heart Rate
Changes in HR may alter cardiac output Slight increases in HR with a constant SV will result in an increased cardiac output Rapid HR will result in decreased filling time & will decrease cardiac output Bradycardia usually results in a decreased cardiac output
SV has three components: Preload, Afterload & Contractility.
Preload = the pressure in the heart at end-diastole (just before contraction). Preload is an indicator of:
Volume of blood in the ventricles at end-diastole Degree of myocardial fiber stretch just before contraction (Starling’s Law) Compliance of ventricles (stiffness or thickness of cardiac muscle) Measured using the CVP (RAP), PAD, PAWP
Low Preload: Hypovolemia, vasodilatationHigh Preload: Hypervolemia, vasoconstriction, right CHF, pulmonary hypertension, pulmonary edemaInterventions: Fluid Resuscitation, diuretics
Afterload = the amount of resistance the ventricles must overcome to eject blood. Factors affecting afterload:
Pulmonary artery pressures Viscosity of blood Outflow valves Peripheral vasculature Measured using SVR & PVR which are calculated measurements
Factors Affecting Afterload: Ventricular outflow obstruction, arterial vasoconstriction, sympathetic nervous system, temperature
Interventions: Vasodilators, vasoconstrictors, ACE Inhibitors

4
Contractility = the force with which the ventricles contract
Measured with Stroke Index (Stroke Volume/BSA)
Factors Affecting Contractility: Scarred myocardial tissue, oxygenation, acidosis, electrolyte imbalance, cardiac ischemia, chemical or pharmacological effects, pathologic conditions
Interventions: Inotropes, beta blockers
Normal Parameters & Values
Parameters ValuesSystolic & Diastolic Blood Pressure 100-130/60-90 mmHgMean Arterial Pressure 70-105 mmHgRight Atrial Pressure (CVP) 2-6 mmHgRight Ventricular Pressure 25-30/0-8 mmHgPulmonary Artery Pressure (PA) 15-30/6-12 mmHgPulmonary Artery Occlusive Pressure (PAOP) aka Pulmonary Artery Wedge Pressure (PAWP)
4-12 mmHg
Cardiac Output/Cardiac Index 4-8 L/min/2.5-4.2 L/min/m2
Systemic Vascular Resistance 770-1500 dyne/sec/cm-5
Pulmonary Vascular Resistance 20-120 dyne/sec/cm-5
Stroke Index RVSWI 7-12g/m2/beat; LVSWI 35-85g/m2/beat
Hemodynamic Monitoring

5
The pulmonary artery catheter (Swan-Ganz) with its different waveforms as it travels through the heart.
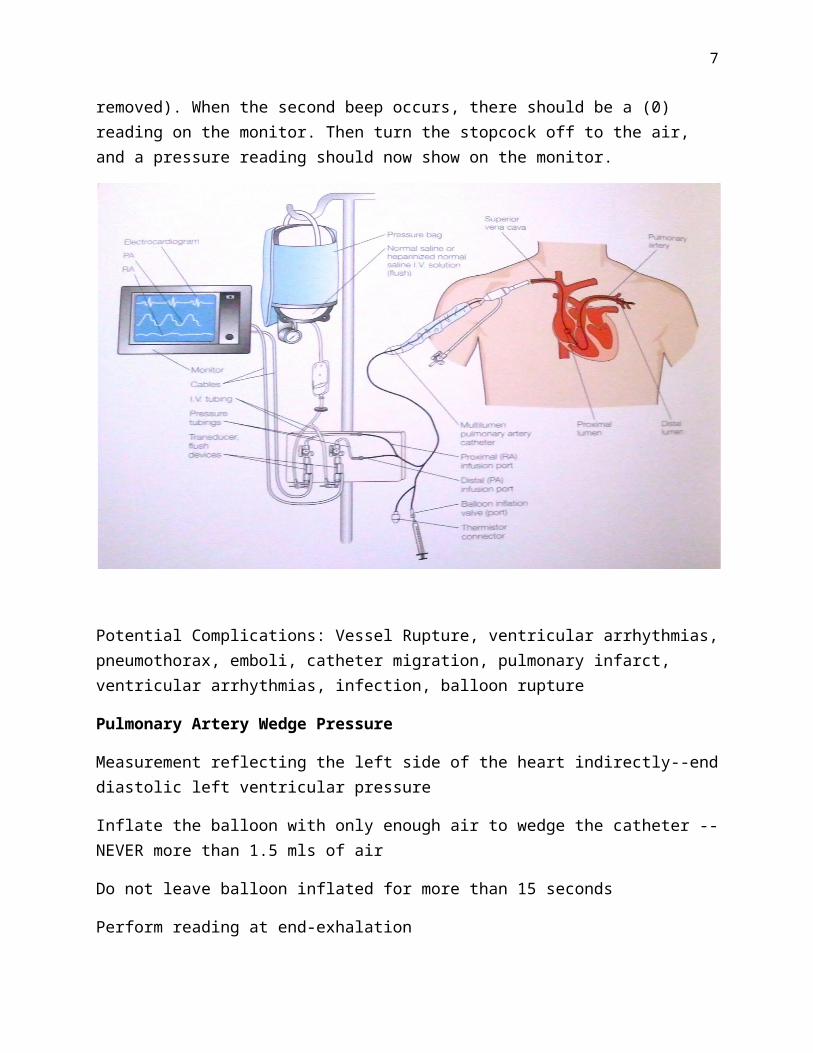
Fluid-filled monitoring systems consist of a catheter connected to a transducer via a system of stopcocks & tubing. A pressure transducer is a device that changes varying physiologic pressures into an electrical signal displayed on the monitor.
The air-fluid interface aka the zeroing stopcock must be leveled to the patient’s phlebostatic axis (4th intercostal space, mid-axillary line). If the stopcock is above the axis, an artificially low reading will be displayed; if it is below the axis, an artificially high number will be displayed.
To zero the lines, the air-fluid interface stopcock must be opened to air (off to the patient), and then the zero button on the monitor is pressed. (Be sure any unvented stopcocks have been removed). When the second beep occurs, there should be a (0) reading on the monitor. Then turn the stopcock off to the air, and a pressure reading should now show on the monitor.

6
Potential Complications: Vessel Rupture, ventricular arrhythmias, pneumothorax, emboli, catheter migration, pulmonary infarct, ventricular arrhythmias, infection, balloon rupture
Pulmonary Artery Wedge Pressure
Measurement reflecting the left side of the heart indirectly--end diastolic left ventricular pressure
Inflate the balloon with only enough air to wedge the catheter -- NEVER more than 1.5 mls of air
Do not leave balloon inflated for more than 15 seconds
Perform reading at end-exhalation
Allow passive deflation of the balloon
Some physicians do not use the wedge as pulmonary problems can affect the wedge reading
The wedge pressure can give us an indication of fluid volume status
7
Increased PAWP: Left sided heart failure, mitral stenosis or insufficiency, tamponade, overwedging (too much air in balloon), high PEEP
Decreased PAWP: Hypovolemia
Cardiac output
Measured by thermodilution--a thermistor at the end of the catheter measures temperature changes when injectate passes over the thermistor and displays this temperature change as a curve on the monitor
5 mLs of Normal Saline should be injected over 4 seconds through the distal port of the catheter (CVP or blue port) at end-expiration
At least 3 measurements should be taken and averaged to ensure accuracy
Factors that may affect CO: Irregular heart rhythms & varying rates, septal defects, sensor malfunction, tricuspid regurgitation
FICK Formula—may be used if CO is invalid.
(SaO2-SvO2) X 1.36 X Hgb=x Ex: Hgb: 11.5, SaO2 98%, SvO2 62%.
125/x= y (98-62) X 1.36 X 11.5 = 563.04
y X 10= CI 125/563.04 = .222
.222 X 10 = 2.22
Troubleshooting
Dampened Waveform: Air bubble or clot in system, kink or knot in system, small leak in system, decreased fluid or pressure in pressure bag
No waveform: transducer not open to catheter, clotted catheter tip, large leak in system (loose connections)
Right Ventricular Waveform: Catheter migration. Assess for ectopy. May need to pull back catheter until RA waveform is seen
Continuous PAWP waveform: Catheter is wedged. Deflate balloon, open to air, reposition patient. If doesn’t work, pull back catheter 1-2mm to achieve resumption of PA waveform

8
Swan Ganz Catheter
Waveform Analysis
Pulmonary Artery Pressure (PAP)
Central Venous Pressure (CVP aka Right Atrial Pressure RAP)
Pulmonary Artery Wedge Pressure (PAWP) aka Occlusive Pressure (PAOP)
Cardiac Output

9
Drip Chart & the Effects on Afterload, Heart Rate & Contractility

10
Key: small arrow indicates minimal effect; double arrows indicate strong effect; blank = no effect
Common Hemodynamic Drips
Drug SVR HR Cardiac Output
Milrinone (primacor)
Levophed (norepinephrine)
Epinephrine
Dobutrex (dobutamine)
Cardene (nicardipine)
Dopamine
Phenylephrine (neosynephrine)
Vasopressin
Nipride (nitroprusside)
Nitroglycerin

11
Vasopressors act by stimulating alpha or beta receptors or both.
Physiology:
Alpha 1 Receptors: Arteries, arterioles, veins
Alpha 2 Receptors: GI tract
Beta 1 Receptors: Heart
Beta 2 Receptors: Skeletal muscle, blood vessels, coronary arteries, bronchial smooth muscle
Contractility Enhancement
Dobutamine (Dobutrex)◦ Stimulates alpha 1, beta 1, beta 2◦ Mix: Premixed 250 mg/250 mls D5W & 500mg/250mls◦ Dosing: Start 2-5 mcg/kg/min. May titrate if ordered by physician. Max 20
mcg/kg/min.
Milrinone (Primacor)◦ Increases contractility, vasodilates◦ Mix: Premixed◦ Dosing: 0.375 mcg/kg/min-0.75 mcg/kg/min
Increase Afterload
Dopamine◦ Stimulates alpha 1, beta 1◦ Mix: Premixed 400 mg/250 mls ◦ Dosing: Dosed in mcg/kg/min. Titrate to prescribed parameters (Max: 20
mcg/kg/min)
Epinephrine◦ Stimulates alpha 1, alpha 2, beta 1, beta 2◦ Mix: 4 mg/250 ml NS or D5◦ Dosing: Dosed in mcg/kg/min. Titrate to prescribed parameters.
Norepinephrine (Levophed)◦ Stimulates alpha 1 & 2, beta 1
12
◦ Mix: 4 mg/250 ml D5W (NOT NS) ◦ Dosed in mcg/min or mcg/kg/min. Titrate to prescribed parameters (Max: 3
mcg/kg/min)
Phenylephrine (Neosynephrine)◦ Stimulates alpa 1, alpha 2 (good choice if tachycardic)◦ Mix: 10 mg/250 ml NS◦ Dosing: Dosed as mcg/min. Titrate to prescribed parameters (Max: 8
mcg/kg/min)
Vasopressin◦ Stimulates vasopressin receptors found in arterial smooth muscle and renal
tubules◦ Mix: 20 mg/100 ml NS◦ Dosing: 0.01 to 0.04 units/minute. Titrate to prescribed parameters.
Decrease Afterload & Preload
Nitroglycerin◦ Dilates arteries & veins◦ Mix: 40 mg/250 mls ◦ Dosing: Dosed in mcg/min or mcg/kg/min. Titrate to prescribed parameters.
Nitroprusside (Nipride)◦ Peripheral vasodilatation ◦ Mix: 50 mg/250 mls D5◦ Dosing: Dosed as mcg/kg/min. Titrate to prescribed parameters. Max 10
mcg/kg/min◦ Monitor for cyanide toxicity. Protect from light
Nicardipine (Cardene)◦ Arterial Vasodilatation ◦ Mix: Premix 50 mg/250 mls D5W ◦ Dosing: Initial 5 mg/hour. Titrate up by 2.5 mg/hour every 5-15 minutes until
desired effect is achieved. Max 15 mg/hour
Decrease Preload

13
Furosemide (Lasix)◦ Dosing: 20-80 mg IVP. May be given as continuous infusion◦ Monitor urine output & serum potassium (K)
Bumetadine (Bumex)◦ Dosing: 0.5-1 mg IVP. May be given as continuous infusion◦ Monitor urine output & serum potassium (K)


















