Vaccines in immunocompromised children - Slideset by Professor Kathryn Edwards
Upload
waididCategory
view
259download
0

Immunocompromised persons vary:
Nature of immunodeficiency
Degree of immunosuppression
Response to immunization
Susceptibility to infection
Vaccine safety and vaccine efficacy
Vaccine benefit
Recommandations
Pro Cons

Heterogeneous group of immunodeficiency
Wide spectrum of clinical manifestations
Caused by >200 known single gene mutations leading to defects of innate
and/or adaptive immunity
Predisposition to autoimmunity and malignancies
Increased susceptibility to infections that influences the final prognosis
Combined immunodeficiencies with/without
associated or syndromic features
Predominantly antibody deficiencies (50%)
Diseases of immune dysregulation
Congenital defects of phagocyte number,
function, or both
Defects in innate immunity
Autoinflammatory disorders
Complement deficiencies

1 10 100
Incidence
Prevalence Europe: 41,401- 638,015
North America: 19,464- 299,947
Worldwide: 390,546- 6,018,593
Europe: 76,148
North America: 35,799
Worldwide: 718,326
5.6/100,000*
*The number of PID patients are estimated from the
prevalence datafor Australian registry
**The number of PID patients are estimated from the
prevalence reported for the US telephone survey
Age (y) Incidence World N (%) Europe (%) North America (%)
0-4 21.9 139,886 (18.8) 8,757 (10.4) 5,183 (13.1)
5-14 7.2 87,338 (11.8) 5,356 (6.4) 3,223 (8.2)
15-24 9.7 117,679 (15.9) 8,862 (10.5) 4,652 (11.8)
25-49 6.8 166,499 (22.4) 18,182 (21.6) 8,014 (20.3)
50-74 15.2 189,772 (25.6) 31,901 (37.9) 13,941 (35.3)
>75 12.7 40,762 (5.5) 11,173 (13.3) 4,438 (11.2)
86/100,000**
Bousfiha AA et al., 2013
Joshi A et al., 2011
10.2-10.4/100,000*y

Principi N & Esposito S, 2014
Type of PID Type of infectious
risk
Recommended vaccines Contraindicated vaccines
Phagocytic cell defects Bacterial and fungal
infections
Inactivated vaccines Live attenuated bacterial vaccines in
chronic granulomatous disease.
Live attenuated viral and bacterial
vaccines in leucocyte adhesion deficiency
and cytotoxic granule-release defect.
Complement deficiencies Bacterial infections All (probably effective) None
TLR and IL-12/IFN-
gamma signalling
pathway defects.
Viral infections (HSV)
Bacterial infections(Non-tuberculous
Mycobacteria, non-
typhoidal Salmonella)
Inactivated vaccines Live attenuated should be given after
evaluating immune system efficiency
Minor antibody
deficiencies (IgA
deficiency, IgG subclass
deficiency, SPAD, ATS)
Viral infections(Enterovirus)
Bacterial infections
All None
Major antibody
deficiencies (X-linked
agammaglobulinemia,
CVI, ataxia-telangiectasia
DiGeorge syndrome,
Wiskott–Aldrich
syndrome)
Viral, bacterial and
fungal infections
Inactivated influenza
vaccines and vaccines
based on bacterial
polysaccharides
Live attenuated vaccines (except to
MMRV in ptz with CD4 ≥ 500 cells/ L,
CD8 ≥200 cells/ L and a normal mitogen
response or with CD4 cells/L ≥25%)

Natural Age Extremes: Prematury and Old age
Acquired Human immunodeficiency virus (HIV) infection/AIDS
Cancer (particularly hematopoietic and lymphoid malignancies)
Metabolic diseases
Malnutrition
Asplenia
Protein-losing enteropathy
…
Iatrogenic Radiation
Immunosuppressive medication therapy (cyclosporine,
dacarbazine, amphotericin B, antithyroid agents, chloramphenicol,
chloroquine, interferons, penicillamine, corticosteroid, many
cancer chemotherapy agents, etc.)
Organ transplantations
…
Heterogeneous group of immunodeficiency
Wide spectrum of clinical manifestations
Both the innate and the adaptive immunodeficiencies affect
Increased morbidity and mortality
Continously increasing

Eibl MM & Wolf HM, 2015; IDSA, 2014
Type of SID Type of
infectious risk
Recommended vaccines Contraindicated vaccines
HIV Viral, bacterial
and fungal
infections
All Live attenuated vaccines if CD4<200 cells/μl
Hematological
and solid
malignancies
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level ID ptz.
Live attenuated vaccines during chemotherapy
HSCT Viral, bacterial
and fungal
infections
All inactivated vaccines. MMR-ZV up to 24mo post transplant, up to 3mo
after immunosuppressive therapy in chronic
GVHD.
Solid organ
tranplant
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level ID ptz.
Live attenuated vaccines.
Immunosuppre
ssive therapy
in AI diseases
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level immunosuppression: to be
considered.
Live attenuated vaccines in high-level
immunosuppressed pt (4ws before to 4ws after
high-dose cortcosteroid therapy; 4ws before to
3mo after biological modifiers therapy).
Asplenia Bacterial
infections
All LAIV

Eibl MM & Wolf HM, 2015; IDSA, 2014
Type of SID Type of
infectious risk
Recommended vaccines Contraindicated vaccines
HIV Viral, bacterial
and fungal
infections
All Live attenuated vaccines if CD4<200 cells/μl
Hematological
and solid
malignancies
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level ID ptz.
Live attenuated vaccines during chemotherapy
HSCT Viral, bacterial
and fungal
infections
All inactivated vaccines. MMR-ZV up to 24mo post transplant, up to 3mo
after immunosuppressive therapy in chronic
GVHD.
Solid organ
tranplant
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level ID ptz.
Live attenuated vaccines.
Immunosuppre
ssive therapy
in AI diseases
Viral, bacterial
and fungal
infections
All inactivated vaccines.
Live attenuated vaccines in low-
level immunosuppression: to be
considered.
Live attenuated vaccines in high-level
immunosuppressed ptz (4ws before to 4ws after
high-dose cortcosteroid therapy; 4ws before to
3mo after biological modifiers therapy).
Asplenia Bacterial
infections
All LAIV
High Level Immunosuppression
Combined PID
Receiving cancer chemotherapy
Within 2 months from SOT
Within 6 months from HSCT
HIV infection, CD4 T cell<200 cell/mm3
Receiving daily corticosteroid, dose>20 mg
of prednisone for >14 days
Receiving biologic immune modulators,
such as TNF-Alpha-blockers, rituximab, …
IDSA 2014

Paucity of efficacy and safety data
Undervaccination
Pro Cons
«The primary care clinician and
respective specialist following the patient
are responsible for assuring vaccination
of immunocompromised patients»
[IDSA, 2014]


Indications Schedule Recommendation,
Strength of
Recommendation and
Quality of Evidence
All immunocompromised subjects Inactivated influenza vaccines (IIV)
Single dose annualy
LAIV should not be administered
in immunocompromised patients
Recommended (S, M)
HSCT patients Pre-HSCT
Post- HSCT
IIV single dose annualy
IIV single dose annualy 6 months
after (4mo after if there is a
community outbreak of influenza)
Usual (S, L)
Recommended (S, M)
Administration (S, VL)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
IIV single dose annualy
Single dose annualy (Including the
first 2-month post-transplant period)
Usual (S, M)
Usual (S, M)
Administration (S, L)
HIV Low-level or no immunosuppression
High-level immunosuppression
IIV single dose annually
IIV single dose annually
Usual (S, H)
Usual (S, H) Some cases of increase
in viremia and a decrease of CD4+
cells, not clinical symptoms.
Asplenia and sickle cell disease IIV single dose annually Usual (S, M)
Chronic Inflammatory diseases on
immunosuppressive medications
IIV single dose annually Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo
Post Anti–B-Cell Antibodies
IIV single dose annually
IIV single dose annualy
Usual (S,L-M)
Usual (S,M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation,
Strength of
Recommendation and
Quality of Evidence
All immunocompromised subjects Inactivated influenza vaccines (IIV)
Single dose annualy
LAIV should not be administered
in immunocompromised patients
Recommended (S, M)
HSCT patients Pre-HSCT
Post- HSCT
IIV single dose annualy
IIV single dose annualy 6 months
after (4mo after if there is a
community outbreak of influenza)
Usual (S, L)
Recommended (S, M)
Administration (S, VL)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
IIV single dose annualy
Single dose annualy (Including the
first 2-month post-transplant period)
Usual (S, M)
Usual (S, M)
Administration (S, L)
HIV infected patients
Low-level or no immunosuppression
High-level immunosuppression
IIV single dose annually
IIV single dose annually
Usual (S, H)
Usual (S, H) Some cases of increase
in viremia and a decrease of CD4+
cells, not clinical symptoms.
Asplenic patients and sickle cell disease IIV single dose annually Usual (S, M)
Chronic Inflammatory diseases or
immunosuppressive medications
IIV single dose annually Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo
Post Anti–B-Cell Antibodies
IIV single dose annually
IIV single dose annualy
Usual (S,L-M)
Usual (S,M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
• Contraindicated in subjects receiving anti–B-cell antibodies such as rituximab or
alemtuzumab or intensive chemotherapy such as for induction or consolidation
chemotherapy for acute leukemia (W, L).
• Vaccines administered while receiving cancer chemotherapy should not be considered valid
doses (S, L).
• Administration of indicated inactivated vaccines 2 or more weeks prior to chemotherapy is
preferred.
• Inactivated influenza vaccine can be administered ≤3 months after chemotherapy, but
response rate may be low.

Indications Schedule Recommendation,
Strength of
Recommendation and
Quality of Evidence
Primary immunodeficiency disorders (classic pathway
(C1, C2, C3, C4), alternate pathway, or severeMBL
deficiency who are PCV13 naïve)
End-stage heart, kidney, liver or lung disease
Chronic inflammatory diseases on immunosuppressive
medications
First dose of PCV13, PPV23 > 8 weeks
after PCV13 and a second dose of
PPV23 5 years later.
For patients who were immunized with
PPv23, PCV13 should be administered
>1 year after the last PPv23 dose.
Well tolerated,
Recommended (S, L-M))
HSCT patients Pre-HSCT
Post- HSCT 3 doses PCV13 after 3-6 months (2
months interval)
1 dose PPv23 12 months after
transplantation
Recommended (S,VL-L)
Recommended (S, L)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
PCV13 >4weeks prior to transplant
If not administered pretransplant.
Recommended (S, VL)
Recommended (S, VL)
Asplenia and sickle cell disease PCV13 2 weeks after splenectomy or 2
weeks before surgery
Recommended (S, VL)
GVHD patients, after resolution A dose of PCV13 and a dose of PPV23
after at least 8 weeks
Recommended
HIV Low-level or no immunosuppression
High-level immunosuppression
A dose of PCV13 and a dose of PPSV23
after at least 8 weeks.
Recommended (S, L)
Recommended (S, VL)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Recommended (S,VL-L)
Usual (S, L)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
PID (Leukocyte adhesion deficiency,
Defects of cytotoxic granule release such as
Chediak-Higashi syndrome, defects of IFN
alpha or gamma production)
Controindicated (S, M)
HSCT (patients without evidence of MMR
immunity, no GVHD and no immunosuppres. drug)
Pre-HSCT
Post-HSCT At least 2 y after transplant, 2-doses
schedule of MMR at least 3 mo interval
Usual (S,VL)
Contraindicated (S; L) (not
administered combined with V)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
Usual (S, M)
Contraindicated (S, L)
HIV Low-level or no immunosuppression
High-level immunosuppression
2-doses schedule of MMR at least 3 mo
interval (not administered combined
with V vaccine)
Usual (W, VL)
Contraindicated (S, M)
Asplenic patients and sickle cell disease Usual (S, M)
Chronic Inflammatory diseases on immunosup.
Medications Planned Immunosuppression
Low-high level Immunosuppression
Usual (S, M)
Contraindicated (W, VL)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
3 mo after chemoterapy, 2-doses
schedule of MMR at least 3 mo interval
Contraindicated (S, M)
Usual (S, L)
Patients receiving anti-B-cell antibodies After at least 6 mo, 2-doses schedule of
MMR at least 3 mo interval
Should receive vaccine (not
administered combined with V)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
PID (Leukocyte adhesion deficiency,
Defects of cytotoxic granule release such as
Chediak-Higashi syndrome, defects of IFN
alpha or gamma production)
Controindicated (S, M)
HSCT (patients without evidence of MMR
immunity, no GVHD and no immunosuppres. drug)
Pre-HSCT
Post-HSCT At least 2 y after transplant, 2-doses
schedule of MMR at least 3 mo interval
Usual (S,VL)
Contraindicated (S; L) (not
administered combined with V)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
Usual (S, M)
Contraindicated (S, L)
HIV Low-level or no immunosuppression
High-level immunosuppression
2-doses schedule of MMR at least 3 mo
interval (not administered combined
with V vaccine)
Usual (W, VL)
Contraindicated (S, M)
Asplenic patients and sickle cell disease Usual (S, M)
Chronic Inflammatory diseases on immunosup.
Medications Planned Immunosuppression
Low-high level Immunosuppression
Usual (S, M)
Contraindicated (W, VL)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
3 mo after chemoterapy, 2-doses
schedule of MMR at least 3 mo interval
Contraindicated (S, M)
Usual (S, L)
Patients receiving anti-B-cell antibodies After at least 6 mo, 2-doses schedule of
MMR at least 3 mo interval
Should receive vaccine (not
administered combined with V)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
Chemiotherapy4 weeks 3 months 3 monthsX X X
Anti-B-cell Ab4 weeks 6 months 3 monthsX X X
HSCT4 weeks Administer, at 24 months, if
- Seronegative
- Not immunosuppr.
- No GVHD
X X
SOT4 weeksX X
U – patient not current with recommendation
for immunocompetent individuals

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
All immunocompromised patients Not licensed Potential risk of severe disease
PID disorder without defective T-cell–mediated
immunity
2-dose schedule separated by a
3-month interval
Recommended (not administered
combined with MMR vaccine)
HSCT
Pre-HSCT
Post-HSCT
See later
See later
Usual (S, L)
Contraindicated (S, L)
SOT recipients
Pretransplant
Starting 2-6 mo Posttransplant
See later
See later
Usual (S, L)
Contraindicated (S, L)
Immunosuppressive therapy
Planned Immunosuppression
Low-high level Immunosuppression
See later
See later
Usual (S, M)
Contraindicated (W-S, VL-M)
HIV Low-level or no immunosuppression
High-level immunosuppression
Usual (S, VL)
Contraindicated (S, M)
Asplenia and sickle cell disease Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Starting at 3 month
Contraindicated (S, M)
Usual (W, VL)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
All immunocompromised patients Not licensed Potential risk of severe disease
PID disorder without defective T-cell–mediated
immunity
2-dose schedule separated by a
3-month interval
Recommended (not administered
combined with MMR vaccine)
HSCT
Pre-HSCT
Post-HSCT
See later
See later
Usual (S, L)
Contraindicated (S, L)
SOT recipients
Pretransplant
Starting 2-6 mo Posttransplant
See later
See later
Usual (S, L)
Contraindicated (S, L)
Immunosuppressive therapy
Planned Immunosuppression
Low-high level Immunosuppression
See later
See later
Usual (S, M)
Contraindicated (W-S, VL-M)
HIV Low-level or no immunosuppression
High-level immunosuppression
Usual (S, VL)
Contraindicated (S, M)
Asplenia and sickle cell disease Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Starting at 3 month
Contraindicated (S, M)
Usual (W, VL)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
Chemiotherapy4 weeks 3 months 2 monthsX X X
Anti-B-cell Ab4 weeks 6 months 2 monthsX X X
HSCT4 weeks Administer, at 24 months, if
- Seronegative
- Not immunosuppr.
- No GVHD
X X
SOT4 weeksX X
U – patient not current with recommendation
for immunocompetent individuals

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
All immunocompromised subjects Not licensed Potential risk of severe disease
Subject aged > 50 years 4 weeks before beginning
immunosuppressive therapy
Should be considered
50-59 years (W, L)
>60 years (S, L)
PID
HSCT
Pre-HSCT
Post-HSCT
See later
See later
Usual (S, L)
Contraindicated (S, L)
SOT recipients
Pretransplant
Starting 2-6 mo Posttransplant
See later
See later
Usual (S, L)
Contraindicated (S, L)
HIV
Low-level or no immunosuppression
High-level immunosuppression
Contraindicated (S, L)
Contraindicated (S, M)
Immunosuppressive therapy
Planned Immunosuppression
Low-high level Immunosuppression
See later
See later
Usual (S, L)
Contraindicated (W-S, VL-M)
Asplenia and sickle cell disease Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Starting at 3 mo
Contraindicated (S, VL)
Usual (W, VL)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
All immunocompromised subjects Not licensed Potential risk of severe disease
Subject aged > 50 years 4 weeks before beginning
immunosuppressive therapy
Should be considered
50-59 years (W, L)
>60 years (S, L)
PID
HSCT
Pre-HSCT
Post-HSCT
See later
See later
Usual (S, L)
Contraindicated (S, L)
SOT recipients
Pretransplant
Starting 2-6 mo Posttransplant
See later
See later
Usual (S, L)
Contraindicated (S, L)
Immunosuppressive therapy
Planned Immunosuppression
Low-high level Immunosuppression
See later
See later
Usual (S, L)
Contraindicated (W-S, VL-M)
Patients with leukemia in remission and who have not
received chemoterapy or radiation
3 months after therapy Recommended
HIV
Low-level or no immunosuppression
High-level immunosuppression
Contraindicated (S, L)
Contraindicated (S, M)
Asplenia and sickle cell disease Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Starting at 3 mo
Contraindicated (S, VL)
Usual (W, VL)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
Chemiotherapy4 weeks 3 monthsX X
Anti-B-cell Ab4 weeks 6 monthsX X
HSCT4 weeksX
SOT4 weeksX
U – patient not current with recommendation for
immunocompetent individuals

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
All immunocompromised
subjects
A single dose
Contraindicated (S, M)
In asymptomatic HIV-infected
adults with CD4 T-cell lymphocyte
count ≥200 cells/mm³
who travel to an endemic area
A single dose Administration (W, L)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Vaccines Indications and Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
Inactivated vaccines Usual (S, H)
Influenza vaccine
TIV and QIV
LAIV
Single dose IM/intradermal (ID) 0.5 mL annually
Healthy, not pregnant, 2-49 years
Contact with HSCT recipiens within 2 months after transplant
or with GVHD and contact with severe combined immune
deficiency (If administered, contact between the
immunocompromised patient and household member should
be avoided for 7days)
Administer (S, H)
Administer (S, L)
Contraindicated (W, VL)
Measles, mumps and
rubella
Administer (S, M)
Rotavirus vaccine Highly immunocompromised pts, avoid handling diasper
of vaccinated infants for 4 weeks
Administer (S, L)
Varicella Vaccine If skin lesion develop, avoid close contact with
immunocompromised persons
Administer (S, M)
Zoster Vaccine >60 years
If skin lesion develop, avoid close contact with
immunocompromised persons
Administer (S, M)
OPV Contraindicated ( S, M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

PID and SID subjects are largely undervaccinated
In PID and SID, vaccination may
improve quality of life and prognosis
reduce infectious complications and be life saving
Raising awareness of the importance of vaccination to
physicians is needed
New studies based on the level of immune suppression
and vaccine effectiveness may provide more results

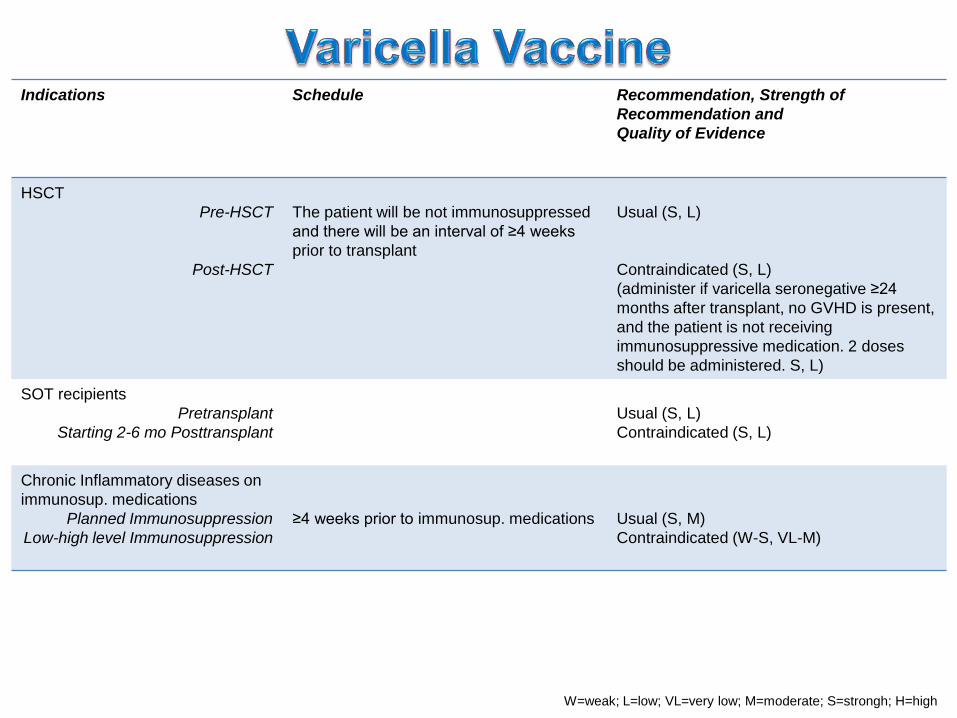
Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
HSCT
Pre-HSCT
Post-HSCT
The patient will be not immunosuppressed
and there will be an interval of ≥4 weeks
prior to transplant
Usual (S, L)
Contraindicated (S, L)
(administer if varicella seronegative ≥24
months after transplant, no GVHD is present,
and the patient is not receiving
immunosuppressive medication. 2 doses
should be administered. S, L)
SOT recipients
Pretransplant
Starting 2-6 mo Posttransplant
Usual (S, L)
Contraindicated (S, L)
Chronic Inflammatory diseases on
immunosup. medications
Planned Immunosuppression
Low-high level Immunosuppression
≥4 weeks prior to immunosup. medications Usual (S, M)
Contraindicated (W-S, VL-M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation,
Strength of
Recommendation and
Quality of Evidence
HIV Low-level or no
immunosuppression
High-level immunosuppression
2-doses Usual (S, M)
Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post Anti–B-Cell
Antibodies
2-doses
Usual (W, L)
Usual (S, VL)
Chronic inflammatory diseases on Immunosuppressive
Medications
2-doses Usual (S, L-M)
Asplenia and sickle cell disease 2-doses Usual (S, M)
HSCT
Pre-HSCT
Post-HSCT
2 doses
2 doses; 6 mo
Usual (S, VL)
Recommended (W, L)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
2 doses pre-transplantation or 6
months after transplantation
Recommended (S, M)
Recommended (S, M
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
Chronic inflammatory diseases on immunosuppressive
medications
3-doses Usual (S, L-M)
Asplenia and sickle cell disease 3-doses Usual (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
3-doses, 2 or 3 wks
3-doses
Usual (W, VL)
Recommended (S, VL)
HSCT
Pre-HSCT
Post-HSCT
3 doses
3 doses, 6 mo
Usual (S, L)
Recommended (S, M)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
3 doses schedule pre-
transplantation or 6 months after
transplantation
Recommended (S, M)
Recommended (S, M)
HIV Low-level or no immunosuppression
High-level immunosuppression
High-dose HBV vaccine (40 µg) Recommended (S, M)
Recommended (S, M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
Asplenia and sickle cell disease Recommended (W, L)
HSCT patients Pre-HSCT
Post- HSC 3-doses schedule, 6-12 months
after transplantation
Usual (S, M)
Recommended (S, M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Usual (W, L)
usual (S, M)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
Usual (S, M)
Usual (S, M)
Chronic Inflammatory diseases on
immunosuppressive medications
Usual (S, L-M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
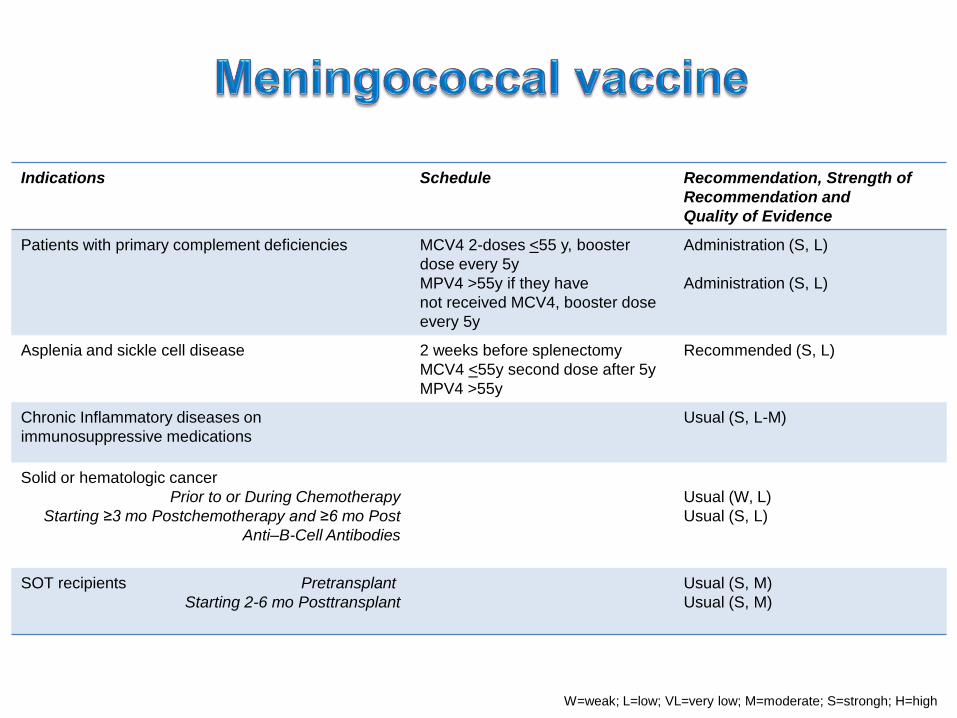
Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
Patients with primary complement deficiencies MCV4 2-doses <55 y, booster
dose every 5y
MPV4 >55y if they have
not received MCV4, booster dose
every 5y
Administration (S, L)
Administration (S, L)
Asplenia and sickle cell disease 2 weeks before splenectomy
MCV4 <55y second dose after 5y
MPV4 >55y
Recommended (S, L)
Chronic Inflammatory diseases on
immunosuppressive medications
Usual (S, L-M)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
Usual (W, L)
Usual (S, L)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
Usual (S, M)
Usual (S, M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high
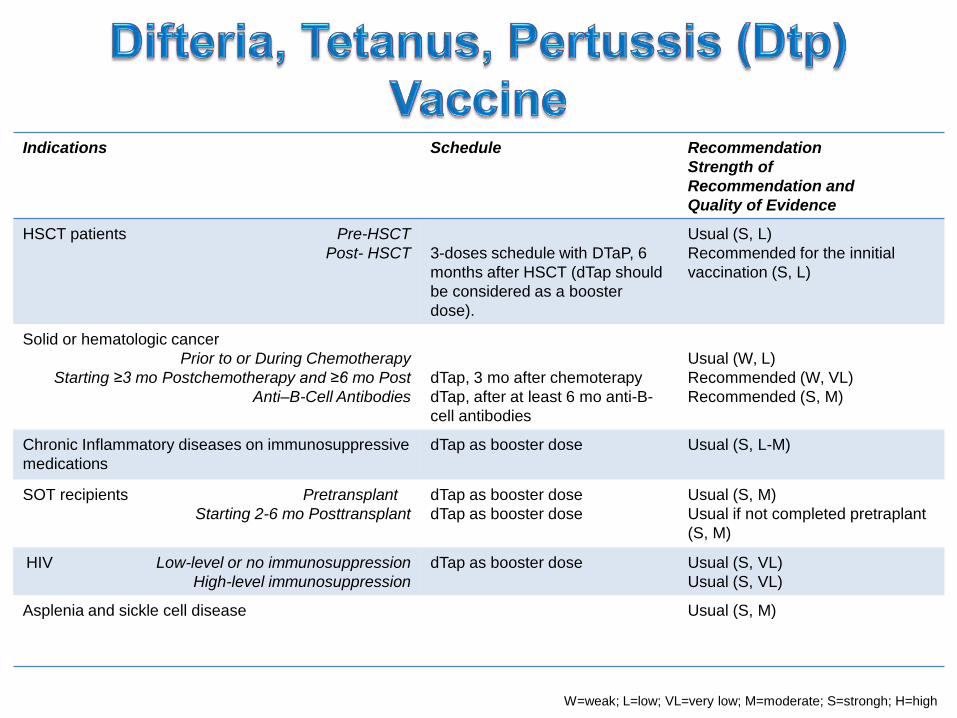
Indications Schedule Recommendation
Strength of
Recommendation and
Quality of Evidence
HSCT patients Pre-HSCT
Post- HSCT 3-doses schedule with DTaP, 6
months after HSCT (dTap should
be considered as a booster
dose).
Usual (S, L)
Recommended for the innitial
vaccination (S, L)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
dTap, 3 mo after chemoterapy
dTap, after at least 6 mo anti-B-
cell antibodies
Usual (W, L)
Recommended (W, VL)
Recommended (S, M)
Chronic Inflammatory diseases on immunosuppressive
medications
dTap as booster dose Usual (S, L-M)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
dTap as booster dose
dTap as booster dose
Usual (S, M)
Usual if not completed pretraplant
(S, M)
HIV Low-level or no immunosuppression
High-level immunosuppression
dTap as booster dose Usual (S, VL)
Usual (S, VL)
Asplenia and sickle cell disease Usual (S, M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

Indications Schedule Recommendation, Strength of
Recommendation and
Quality of Evidence
In all immunocompromised subjects for disease or
medication
3 doses at 0,1-2 and 6 mo Recommended (S, L)
HIV Low-level or no immunosuppression
High-level immunosuppression
HPV4 3 doses 0, 2, 6 mo
HPV4 3 doses 0, 2, 6 mo
Usual (S, VL)
Usual (S, VL)
Solid or hematologic cancer
Prior to or During Chemotherapy
Starting ≥3 mo Postchemotherapy and ≥6 mo Post
Anti–B-Cell Antibodies
3 doses at 0,1-2 and 6 mo
3 doses at 0,1-2 and 6 mo
Usual (W, VL)
Usual (S, VL)
HSCT patients Pre-HSCT
Post- HSCT
3 doses at 0,1-2 and 6 mo
6mo after transplant 3 doses at 0,1-2
and 6 mo
Usual (S, VL)
Usual (W, VL)
SOT recipients Pretransplant
Starting 2-6 mo Posttransplant
3 doses at 0,1-2
3 doses at 0,1-2
Usual (S, L-M)
Usual (S, L-M)
Chronic Inflammatory diseases on
immunosuppressive medications
3 doses at 0,1-2 Usual (S, VL-M)
Asplenia and sickle cell disease 3 doses at 0,1-2 Usual (S, M)
W=weak; L=low; VL=very low; M=moderate; S=strongh; H=high

PID and SID subjects are largely undervaccinated
Vaccination may improve quality of live and prognosis
of PID
Vaccination could reduce infectious complications and
be life saving in SID patients
Raising awareness of the importance of vaccination to
physicians is needed
New studies based on the level of immune suppression
and vaccine effectiveness may provide more results
Evaluation and monitoring of the immune response
could improve treatment decisions, reduce
complications of disease, hospitalization and costs.