
UvA-DARE (Digital Academic Repository) Genetic and ... · Totall cholesterol , mg/dl LDLL...
17
UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) UvA-DARE (Digital Academic Repository) Genetic and biochemical riks factors in coronary artery disease Boekholdt, S.M. Link to publication Citation for published version (APA): Boekholdt, S. M. (2005). Genetic and biochemical riks factors in coronary artery disease. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date: 30 Apr 2020
Transcript of UvA-DARE (Digital Academic Repository) Genetic and ... · Totall cholesterol , mg/dl LDLL...

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Genetic and biochemical riks factors in coronary artery disease
Boekholdt, S.M.
Link to publication
Citation for published version (APA):Boekholdt, S. M. (2005). Genetic and biochemical riks factors in coronary artery disease.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 30 Apr 2020

Plasmaa concentration of macrophagee migration inhibitor y factorr and the risk of futur e myocardiall infarction or coronary arteryy disease death in men and womenn without prior myocardial infarctio nn or stroke; the EPIC-Norfolkk prospective population study y
Abstrac t t Background Background Macrophagee migration inhibitory factor (MIF), a pro-inflammatory cytokinee has been implicated in atherogenesis, and may predictive of futuree myocardial infarction or death of coronary artery disease (CAD) in apparentlyy healthy individuals.
Methodss and Results Wee performed a prospective case-control study nested in the EPIC-Norfolk cohort.. We selected men and women who did not report a history of myocardiall infarction or stroke at baseline. Baseline MIF concentrations weree measured among 777 individuals who suffered a myocardial infarctionn or CAD death during follow-up, and 1554 matched controls whoo remained free of CAD. Baseline MIF concentrations were higher in casess than controls (median 107.4 ug/1 versus 90.7 pg/1, p=0.001). The risk of futuree myocardial infarction or death from CAD increased with increasing MIFF quartiles (p for linearity <0.0001). Individuals in the highest MIF quartilee had an unadjusted odds ratio for future myocardial infarction orr CAD death of 1.6 (95%CI=1.2-2.0). After adjustment for traditional risk factorss and C-reactive protein, this odds ratio was 1.3 (95%CI=1.0-1.7). Upon additionall adjustment for white cell count, this relationship was no longer statisticallyy significant.
Conclusions Conclusions Amongg men and women who did not report a history of heart attack orr stroke, elevated levels of MIF were associated with an increased risk off myocardial infarction or CAD death independent of traditional cardiovascularr risk factors and C-reactive protein levels. However, this relationshipp was not very strong. These prospective data support a regulatoryy role for MIF inn the process of atherosclerosis.
Backgroun d d Inflammationn is involved in the initiation and progression of atherosclerosiss and in the development of acute coronary syndromes.1
Forr clinical purposes, C-reactive protein is gaining acceptance as the most usefull inflammatory plasma marker.2 However, the inflammatory processes thatt underlie atherosclerosis are mediated by a multitude of cytokines andd are unlikely to be reflected fully by C-reactive protein levels alone. Prospectivee evidence on other cytokines in apparently healthy individuals iss limited and exists only for interleukin-6,3^ and macrophage inhibitory cytokine-1.7 7
Macrophagee migration inhibitory factor (MIF) is considered to be a pleiotropicc cytokine but, in contrast to other cytokines, it has not only regulatoryy functions but also at least two enzymatic activities.8-9 MIF hass a homotrimeric structure and is expressed by a range of leukocytes includingg monocytes, macrophages, neutrophils, and mast cells, but also byy endocrine organs involved in stress response such as the hypothalamus andd adrenal glands.M1 Under physiological circumstances, MIF is thought too regulate host responses to infection and stress. Consistent with this hypothesis,, MIF was found to upregulate the expression of toll-like receptor-44 by macrophages12 and to counterbalance the immunosuppressive effectss of glucocorticoids by modulating intracellular pro-inflammatory pathways.13144 MIF is involved in several pathophysiological inflammation-mediatedd conditions such as sepsis,15 arthritis,16 bronchial asthma,17
glomerulonephritis,188 renal transplant rejection,19 and acute respiratory distresss syndrome.2021 In addition, MIF is thought to be involved in atherosclerosiss because it induced expression of intercellular adhesion molecule-11 by vascular endothelial cells and, interestingly, upregulation of MIFF was closely associated with adhesion of monocytes to the endothelium andd subsequent migration into the subendothelial space.22 Inhibition off MIF resulted in a shift in the cellular composition of neointimal atheroscleroticc plaques toward a more stabilized phenotype, possibly resultingg from a reduction of monocyte recruitment by endothelial MIF.23
Inn humans, evidence for a role of MIF in atherosclerosis is limited as only onee histological study has reported an upregulation of MIF during the progressionn of atherosclerosis towards inflammatory stages.24 Whether MIF plasmaa levels are predictive of the risk of clinical coronary artery disease remainss unclear. Itt was our objective to determine whether, in individuals who had never sufferedd a myocardial infarction or stroke, elevated plasma concentrations off MIF were associated with an increased risk of future coronary artery disease.. In addition, we investigated whether this relationship was modifiedd by other cardiovascular risk factors.
183 3

Method s s StudyStudy design Wee performed a nested case-control study among participants of the EPIC-Norfolkk study (EPIC, European Prospective Investigation into Cancer and Nutrition),, a prospective population study of 25,663 men and women aged betweenn 45 and 79 years, resident in Norfolk, United Kingdom.25 EPIC-Norfolkk is part of a nine-country collaborative study designed to investigate dietaryy and other determinants of cancer. Additional data were obtained to enablee the assessment of determinants of other diseases. Participants were recruitedd by post from age-sex registers of general practices in Norfolk.25
Thee study sample was closely similar to United Kingdom samples with respectt to many characteristics including anthropometry, blood pressure, andd plasma lipids, but with a lower proportion of smokers.26 At the baseline surveyy between 1993 and 1997, participants attended a baseline clinic visit andd completed a detailed health and lifestyle questionnaire. Alll individuals have been flagged for death certification at the United Kingdomm Office of National Statistics, with vital status ascertained for the entiree cohort. In addition, participants admitted to hospital were identified usingg their unique National Health Service number by data linkage with ENCORE,, the East Norfolk Health Authority database, which identifies all hospitall contacts throughout England and Wales for Norfolk residents. Thee underlying cause of death or hospital admission was coded by trained nosologistss according to the International Classification of Diseases 9th revision.. Fatal coronary artery disease during follow-up was defined as deathh with the underlying cause coded as International Classification off Diseases codes 41CM14. Non-fatal coronary artery disease was defined ass hospital admission with the underlying cause coded as International Classificationn of Diseases codes 410-414. In 1996, we conducted a validation studyy of coronary artery disease cases ascertained from death certificates andd hospital admissions. Confirmation of the cause of death was sought inn general practice and hospital notes or the post mortem report. For coronaryy deaths identified from death certificates, the cause of death wass coded as a definite coronary death, possible coronary death, or not a coronaryy death using standard WHO-MONICA criteria.27 Out of 39 deaths, 388 were confirmed as such by inspection of the notes. For cases identified basedd on linkage with hospital admission databases, the admission diagnosiss was evaluated by inspection of hospital notes. The event was thenn coded as a definite myocardial infarction, possible myocardial infarctionn or not a myocardial infarction on the basis of the clinical history, ECGG changes and enzyme changes using standard WHO-MONICA criteria.27
Alll 26 patients with a hospital discharge diagnosis of myocardial infarction hadd either a definite or possible myocardial infarction by WHO-MONICA criteria.. This validation study indicates that identification of events of coronaryy artery disease from death certification or hospital admissions providess a valid ascertainment of events. We report results with follow-up upp to January 2003, an average of about 6 years. The study was approved

byy the Norwich District Health Authority Ethics Committee and all participantss gave signed informed consent.
Participants Participants Forr the present analysis, we excluded individuals who reported a history of heartt attack or stroke at the baseline clinic visit. Cases were 777 individuals whoo developed a myocardial infarction or died of coronary artery disease duringg follow-up. Controls were study participants who remained free of coronaryy artery disease during follow-up. Two controls were matched to eachh case by sex, age (within 5 years), and date of visit {withi n 3 months).
BiochemicalBiochemical analyses Bloodd was taken by venepuncture into plain and citrate tubes and processedd for assay at the Department of Clinical Biochemistry, University off Cambridge, or storage at -80° C. Serum levels of total cholesterol, high-densityy lipoprotein cholesterol, and triglycerides were measured onn fresh samples with the RA1000 (Bayer Diagnostics, Basingstoke, Unitedd Kingdom) and low-density lipoprotein cholesterol levels were calculatedd with the Friedewald formula.28 From 1994, full blood count was additionallyy measured on fresh EDTA samples using a Coulter Counter and thiss measure was available on approximately 60% of the cohort. In 2003, plasmaa samples for cases and controls were retrieved from frozen storage, thawed,, and MIF was measured by use of a commercially available assay (R&DD Systems, Minneapolis, Minnesota). The lower detection limi t was 62.5 Mg/1,, the upper detection limi t was 2000 |jg/l, and the intra-assay variation amongg duplicates was 9.5 %. C-reactive protein levels were measured with aa sandwich-type enzyme-linked immunosorbent assay in which polyclonal rabbitt anti-C-reactive protein antibodies were used as catching antibodies andd biotinylated monoclonal antibodies against C-reactive protein (Sanquin Research,, Amsterdam, the Netherlands) as the detecting antibody. Results weree related to a standard consisting of commercially available C-reactive proteinn (Behringwerke AG, Marburg, Germany). The lower detection limi t wass 0.1 mg/1. Samples were analyzed in random order to avoid systemic bias.. Researchers and laboratory personnel had no access to identifiable informationn and could identify samples by number only.
StatisticalStatistical analysis Subjectss with MIF concentrations below the lowest detection limi t were assumedd to have the lowest detectable concentration and subjects with concentrationss above the upper detection limi t were assumed to have thee highest detectable concentration. Baseline characteristics were comparedd between cases and controls taking into account the matching betweenn them. A mixed effect model was used for continuous variables andd conditional logistic regression was used for dichotomous variables. Becausee MIF and triglyceride levels had a skewed distribution, values were log-transformedd before statistical analysis but untransformed medians
185 5
186 6
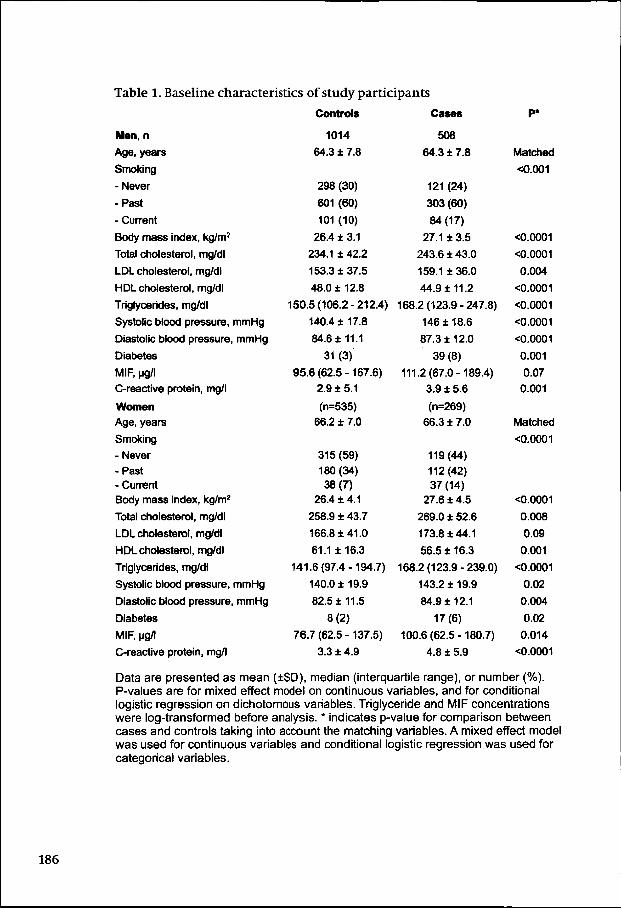
Tablee 1. Baseline characteristics of study participants
Men,, n
Age,, years
Smoking g
-Never r
-Past t
-- Current
Bodyy mass index, kg/m2
Totall cholesterol, mg/dl
LDLL cholesterol, mg/dl
HDLL cholesterol, mg/dl
Triglycerides,, mg/dl
Systolicc blood pressure, mmHg
Diastolicc blood pressure, mmHg
Diabetes s
MIRR ug/l
C-reactivee protein, mg/l
Women n Age,, years
Smoking g
-- Never
-Past t -- Current Bodyy mass index, kg/m2
Totall cholesterol, mg/dl
LDLL cholesterol, mg/dl
HDLL cholesterol, mg/dl
Triglycerides,, mg/dl
Systolicc blood pressure, mmHg
Diastolicc blood pressure, mmHg
Diabetes s
MIF,, ug/l
C-reactivee protein, mg/l
Control s s
1014 4
64.33 7.8
2988 (30)
601(60) )
1011 (10)
26.44 3.1
234.11 42.2
153.33 5
48.00 12.8
150.5(106.2-212.4) )
140.44 17.8
84.66 1
31(3) )
95.66 (62.5 -167.6)
2.99 5.1
(n=535) ) 66.22 7.0
315(59) ) 1800 (34) 38(7) )
26.44 4.1
258.99 43.7
166.88 0
61.11 3
141.6(97.4-194.7) )
140.00 19.9
82.55 5
8(2) )
76.7(62.5-137.5) )
3.33 4.9
Cases s
508 8
64.33 7.8
1211 (24)
303(60) )
84(17) )
27.11 3.5
243.66 43.0
159.11 0
44.99 2
168.22 (123.9 - 247.8)
1466 18.6
87.33 12.0
39(8) )
111.2(67.0-189.4) )
3.99 5.6
(n=269) )
66.33 7.0
1199 (44)
1122 (42) 377 (14)
27.66 4.5
269.00 52.6
173.88 1
56.55 16.3
168.2(123.9-239.0) )
143.22 9
84.99 1
17(6) )
100.6(62.5-180.7) )
4.88 5.9
P* *
Matched d
<0.001 1
<0.0001 1
<0.0001 1
0.004 4
O.0001 1
<0.0001 1
<0.0001 1
<0.0001 1
0.001 1
0.07 7
0.001 1
Matched d
<0.0001 1
<0.0001 1
0.008 8
0.09 9
0.001 1
<0.0001 1
0.02 2
0.004 4
0.02 2
0.014 4
<0.0001 1
Dataa are presented as mean , median (interquartile range), or number (%). P-valuess are for mixed effect model on continuous variables, and for conditional logisticc regression on dichotomous variables. Triglyceride and MIF concentrations weree log-transformed before analysis. * indicates p-value for comparison between casess and controls taking into account the matching variables. A mixed effect model wass used for continuous variables and conditional logistic regression was used for categoricall variables.

withh corresponding interquartile range are shown in the tables. Mean riskrisk factor levels per MIF quartile were calculated in order to determine relationshipss between MIF levels and traditional cardiovascular risk factors. Forr continuous risk factors, we also calculated Spearman correlation coefficientss and corresponding p-values. Conditional logistic regression analysiss was used to calculate odds ratios (OR) and corresponding 95% confidencee intervals (95%CI) as an estimate of the relative risk of incident coronaryy artery disease. MIF concentrations were analysed as categorical variabless after division into quartiles. The lowest quartile was used as referencee category. Odds ratios were adjusted for the following traditional cardiovascularr risk factors: age, sex, smoking, systolic blood pressure, total cholesterol,, high-density lipoprotein cholesterol, diabetes, and body mass index.. Odds ratios were also estimated after additional adjustment for C-reactivee protein and after additional adjustment for both C-reactive protein andd white cell count. The interaction between sex and MIF was calculated too assess the validity of pooling sexes. Statistical analyses were performed usingg SPSS software (version 10.1, Chicago, Illinois). A p-value less than 0.05 wass considered significant.
Result s s Fromm the total number of 777 cases, 194 (25%) died with coronary artery diseasee as underlying cause and 583 (75%) had a non-fatal myocardial infarction.. Owing to matching, age was comparable between cases andd controls. As expected, both women and men who developed a cardiovascularr event during follow-up were more likely than controls to smokee and have diabetes (table 1). Among both sexes, total cholesterol levels,, systolic and diastolic blood pressure, and body mass index were significantlyy higher in cases than controls and high-density lipoprotein cholesteroll levels were significantly lower in cases than controls. Baseline mediann MIF concentrations were higher in cases (107.4 ug/1, interquartile rangee = 62.5-185.3) than in controls (90.7 pg/1, interquartile range = 62.5-156.4,, p=0.001). Tablee 2 shows the distribution of traditional cardiovascular risk factors per sex-specificc MIF quartile. A linear relationship was observed between MIF quartiless and body mass index, total cholesterol, high-density lipoprotein cholesterol,, triglycerides, C-reactive protein and white cell count. Among bothh men and women, the unadjusted odds ratio for future myocardial infarctionn or death from coronary artery disease was elevated in the highestt MIF quartiles (p for linearity = 0.003 for men and p for linearity == 0.006 for women; table 3). For both the unadjusted and adjusted odds ratios,, the interaction between sex and MIF did not reach statistical significancee which justifies pooling of the sexes. For sexes combined, the relationshipp between MIF and risk of future coronary artery disease was slightlyy attenuated but still significant after adjustment for classical risk factorss (odds ratio = 1.3, 95%CI = 1.0-1.7 inn the highest quartile), and after adjustmentt for classical risk factors and C-reactive protein (odds ratio = 1.3,
187 7

95%CII = 1.0-1.7 in the highest quartile. Upon adjustment for classical risk factors,, C-reactive protein, and white cell count, the observed relationship wass substantially attenuated and no longer statistically significant. This relationshipp between MIF quartiles and cardiovascular risk did not differ whenn instead of white cell count, adjustment was made for the number of monocytes,, lymphocytes, or granulocytes {for each analysis: OR=1.2, 95%CI == 0.8-1.7 in the highest MIF quartile). All white cell count-adjusted risk estimatess were based on approximately 60% of individuals because white celll count was not available in all subjects.
Discussio n n Inn the present prospective nested case-control study, plasma levels of MIF, a proinflammatoryy cytokine, were elevated in men and women who did not reportt a history of heart attack or stroke at baseline but who did suffer a myocardiall infarction or died of coronary artery disease during follow-up. Afterr adjustment for traditional cardiovascular risk factors and C-reactive proteinn levels, individuals in the highest MIF quartile had an odds ratio for futuree myocardial infarction or coronary artery disease death of 1.3 (95%CI == 1.0-1.7, p=0.03), compared to those in the lowest quartile. Upon additional adjustmentt for white cell count, the odds ratio was no longer statistically significant.. These results suggest that MIF is involved in the inflammatory processess that underlie atherosclerosis. Inflammationn is a key process in the initiation and progression of atherosclerosiss and in the development of clinical cardiovascular events. AA number of cytokines have been found to predict future cardiovascular eventss in individuals with prevalent cardiovascular disease including tumorr necrosis factor-a,29 interleukin-18,30 interleukin-10,31 and soluble CD400 ligand.32 However, in individuals without prevalent cardiovascular diseasee a predictive role has been established only for C-reactive protein,51433344 interleukin-6,M and macrophage inhibitory cytokine-1.7 For clinicall purposes, C-reactive protein is considered to be the most useful inflammatoryy marker due to its relative stability over time, the availability off standardized commercial assays, and the abundance of clinical evidence forr its strong relationship with the risk of future cardiovascular events. However,, the inflammatory processes involved in atherosclerosis are likely too be much more complex than can be reflected by C-reactive protein plasmaa levels only. MIFF is a pleiotropic cytokine is thought to regulate the host response to stresss and infection. Stress-induced increases in circulating glucocorticoid levelss have immunosuppressive effects but these effects may endanger the integrityy of the host should an offending pathogen survive the primary hostt defense system. A principal role of MIF is to counterbalance these stress-inducedd immunosuppressive effects. A second important role of MIF iss to facilitate the host to raise an adequate immune response to infectious stimuli.. The upregulation of MIF plasma levels, either by the release of preformedd MIF or by its de novo synthesis,35 can be triggered by indirect
188 8

O) )
ö ö 1*. . o o 8 8 SS 3
oo o o o o o VV V V V
CO O
O)) £ 33 C
i i 9 9
COO y-r
©© -ö
11 ? 2 S i § oo 9 o ö ö o
f f ? ?
CD D
1-4 4
rr r U H H 1—1 1
s s T3 3 Ö Ö n) ) X X (U U C/5 5
* * fH H O O
u u ,tf f
CO O
$ $ «« ,
CO O
& &
«> > a a CMMI A A CM M to o
»~~ co t o AA S
o o co o H H
O O
COO «j m. t o
tt I r r n , j
"*** ÏÏ "H ^" ^^ ^ ^* * "̂" ^ T l JJ 4J T l T ï I J
coo ei «J to co o, a; *i e» «,
TT T
O O
Ö Ö
coo a> oo ö
K)) O) S f (O O)
r-- T- ö, o> o co
óó ö <9 ö o ö
? ?
~~ — _ 5 § ( dé -H H
o»» 8 +11 4*
ss T ^ rt «
££ g s? si 3 88 S I
CM M < S k T ^ " ' - * — » §§ CM o £
ss is r ie T f **
s s Ö.. e £ & * ^
33 5 2 K co o
^^ cll +** ** 44 © PP Q «i T~
:: T » *~
O) )
44 4 I O O
8 8
o> > f f
P«--co o
** * ^--co o r--
o o T-" "
1* . . ^p . .
* * CO O
<o o
o> > CJ J 44 4
co o CM M
IO O co o ss i § ** fl -H ^ ** tri rrt t>
0> > O)) CO
§ 8 §f f
eoo - . o> co ^
Q .. ^ ^ , S - 44 ^ 44 -H -M ^ $ 4 4
S a o r o o ) ( 0 a q i o oo : ^^ co 3: i*. ^ - CM ™ co
CMM ^ «- T-
. ,, I O - , " .
G.. Ö £ S 44 ^ 4) 41 # J g 4»
T-- (M ^
S? ? r-r- *f —. «t <* f3.. n . 3*, 44 44
N.. ,_
I f j O O i - C O ^ ^ t - U Ï Ï COO «tf CM CO' -^ cd có
ww «Q s g
coo « *~~ có MM 41
O) ) on n 0>> T-
8»» - *
CMM CM
8 8
I O O
mm co eo *~* ^ ^
oo « «ï K"" * O h-
ww w ^ 5= ^ N ^ -̂^^ w" r i +f 44 ^ 44 44 ^
COO to K °. a> "? ^ CB
88 8 si 8 S « CM M
CM M
tóó ' " " " ** *— T"
O) ) X X
I I II i 1»
55 "§ p" I? o. S
f * 3 | f | g ^ ^
?? r
coo 2 a>> ai "coo ' F
^^ ®
cc ^ == CD
** £ .. Q.
o o
Ei i OO CO cc ®
ss s .«5-5 5 >> c 0)) — "OO IL
ES S CD D T33 «D CC 3 iSS co »» * 444 Q. cc a>
CDD c
s ! !
coo É
.22 o 455 co - >> CD
S3 3 'Il l ^^ CD
'öö ' o 033 fc O-- <r> «« O XX o a>> c coo o
^^ co COO P (D
«f f «« 8
w w
0 0
22 E s CDD fc (ö
cc co c3
oo co -
coo .E o Q 4 - J 5 5
189 9

stress-inducedd stimuli or by direct pro-inflammatory stimuli such as tumor necrosiss factor and lipopolysaccharide.36 In turn, MIF facilitates the host too raise an adequate immuneresponse by influencing various intracellular pro-inflammatoryy pathways13 " and by upregulating the expression in macrophagess of toll-like receptor-4, the innate immune receptor for lipopolysaccharide.122 Although MIF is required to combat infection, highh plasma levels of MIF are harmful during acute infections. The administrationn of recombinant MIF alone did not induce shock in mice but whenn co-administered with lipopolysaccharide or E.Coli, recombinant MIF levelss did exacerbate lethal endotoxemia.37 The MIF-induced upregulation off toll-like receptor4 may be one of the mechanism linking MIF to cardiovascularr risk because the toll-like receptor-4 has been shown to be involvedd to the progression of atherosclerosis and the risk of cardiovascular events.3839 9
MIFF is not only produced by immune cells but was also detected in vascularr endothelial cells and smooth muscle cells in histologically normal arteries.244 In early stages of atherosclerosis, oxidized low-density lipoprotein cholesteroll accumulates in the subendothelial space. Oxidized low-densityy lipoprotein cholesterol affects the expression pattern of adhesion moleculess on endothelial cells thereby promoting the immigration of macrophagess and other inflammatory cells into the vessel wall. MIF is one off the cytokines that are upregulated in endothelial cells after incubation withh oxidized low-density lipoprotein cholesterol and its expression is upregulatedd as early atherosclerotic plaques progress towards advanced stages.222 In vitro studies have shown that macrophages stimulated with MIFF secrete tumor necrosis factor andinterleukin-8, both proinflammatory cytokiness abundantly present in atherosclerotic lesions.20 In addition, MIFF can upregulate the expression of intercellular adhesion molecule-1 byy endothelial cells and this upregulation is associated with monocyte adhesionn onto the endothelium and subsequent migration into the subendotheliall space.22Thus, oxidized low-density lipoprotein cholesterol mayy promote the immigration of macrophages into the subendothelial spacee and endothelium-derived MIF may facilitate process. Interestingly, inn apolipoprotein E-deficient mice, inhibition of MIF resulted in a shift inn the cellular composition of neointimal atherosclerotic plaques toward aa stabilized phenotype with reduced macrophage/foam cell content and increasedd smooth muscle cell content content.23 This observation in combinationn with the results of our study supports the hypothesis that MIF mayy increase the risk of coronary artery disease by enhancing the number off macrophages in prevalent atherosclerotic plaque, thereby increasing plaquee instability and proneness to rupture. AA number of issues have to be taken into account when interpreting thee results of the present study. Plasma levels of MIF were determined inn a single sample that was obtained at a non-uniform time of the day. Diurnall variation and variation over time could have affected the MIF concentrationss that we measured. However, this would lead to random

Tablee 3. Odds ratios for future coronary artery disease by MIF quartile Mirr quanii e
Quartil ee range , ug/t
Menn and women , n Unadjuste d d
Adjuste dd (1)
Adjuste dd (2) Adjuste dd (3)
Men,, n
Unadjuste d d
Adjuste dd (1)
Adjuste dd (2)
Adjuste dd (3)
Women ,, n
Unadjuste d d
Adjuste dd (1)
Adjuste dd (2)
Adjuste dd (3)
\ \ <62,5 5
189/489 9
1.0 0
1,0 0
1,0 0
1,0 0
106/289 9
1.0 0
1,0 0
1.0 0
1.0 0
83/200 0
1.0 0
1.0 0 1,0 0
1,0 0
2 2
62,5-94,5 5
124/288 8
1,11 (0,9-1,4)
1,0(0,8-1,4) )
1,0(0,7-1,3) ) 0,9(0,6-1,4) )
86/181 1 1,3(0,9-1,8) )
1,4(1,0-2,1) )
1.4(1,0-2,0) )
1,4(0,8-2,3) )
38/107 7
0.9(0,6-1,3) )
0,6(0,4-1,0) )
0,6(0,4-1,1) )
0,6(0,3-1,1) )
3 3
94,6-166,6 6
183/343 3 1,4(1,1-1,8) )
1,11 (0,9-1,5)
1,11 (0.8-1,4)
1,0(0,7-1,4) )
129/237 7
1,4(1,1-1,9) )
1,3(0,9-1,8) )
1,3(0,9-1,8) ) 1,1(0,7-1,8) )
54/106 6
1,3(0,9-2,0) )
1,0(0,6-1,5) )
1,0(0,6-1,5) )
0,9(0,5-1,5) )
4 4
>> 166,6
205/324 4
1,6(1,2-2,0) )
1,3(1,0-1,7) )
1,3(1,0-1,7) ) 1,2(0,8-1,7) )
141/228 8
1,5(1,1-2,1) )
1,5(1,1-2,1) )
1,5(1,1-2,1) )
1,3(0,8-2,1) )
64/96 6 1,7(1,1-2,4) )
1,2(0,8-1,9) )
1,2(0,8-2,0) )
1,11 (0,6-1,9)
P P
<< 0,0001
0,03 3
0,03 3 0,4 4
0,003 3
0,03 3
0,03 3
0,3 3
0,006 6
0,3 3
0,3 3
0,8 8
Oddss ratios for the risk of myocardial infarction or death from coronary artery diseasee for sexes combined adjusted for sex, and for men and women separately. (1)) Adjustment for age, systolic blood pressure, total cholesterol, high-density lipoproteinn cholesterol, body mass index (continuous variables), smoking and diabetes.. (2) Adjustment for variables above and in addition,, C-reactive protein. (3) Adjustmentt for variables above and in addition, C-reactive protein and white cell count.. The numbers in parentheses indicate the number of cases/controls within thatt quartile. The total number of cases/controls for the unadjusted odds ratio, the adjustedd odds ratio (1), adjusted odds ratio (2), and adjusted odds ratio (3) were 777/1551,, 703/1449, 701/1448, 442/911, respectively. * indicates p-value for x2
linearr trend with 1 degree of freedom.
misclassificationn in our data and therefore to an underestimation of our findings.. Second, the relationship between MIF plasma concentrations, MIF concentrationss in the subendothelial space, and MIF activity levels requires furtherr exploration. Third, whether or not MIF is instrumental in the developmentt of future cardiovascular events remains to be established. It iss unlikely that differences in MIF plasma levels occurred as a consequence off previous cardiovascular events because individuals with symptomatic cardiovascularr disease were excluded from our analysis but we cannot excludee the possibility that MIF levels reflect the extent of subclinical atherosclerosis. . MIFF plasma levels were strongly correlated with most traditional cardiovascularr risk factors. It is therefore not surprising that adjustment forr these parameters substantially attenuated the relationship between MIFF and the risk of coronary artery disease. Despite the fact that C-reactive proteinn was also strongly correlated with MIF, additional adjustment for
191 1

C-reactivee protein did not affect the observed relationship. Therefore, thesee data suggest that MIF may represent an inflammatory pathway thatt is relevant for atherogenesis and independent of C-reactive protein. Thee observed relationship was substantially attenuated upon additional adjustmentt for white cell count which is an established risk factor for cardiovascularr disease independent of classical risk factors.4041 White cell countt was available in approximately 60% of the individuals resulting in losss of statistical power but the point estimates for the risk of coronary arteryy disease were also substantially reduced after adjustment for white celll count. MIF is expressed by a range of leukocytes including monocytes, macrophages,, neutrophils, and mast cells. It is constitutively expressed andd stored in intracellular pools and therefore does not require de novo proteinn synthesis before secretion. This observation may explain why thee relationship between MIF and the risk of coronary artery disease disappearedd upon adjustment for white cell count. Inn conclusion, these prospective data support a role for MIF in determining thee risk of coronary artery disease. However, the relationship between MIFF levels and the risk of future myocardial infarction or death from coronaryy artery disease was weak and was attenuated upon adjustment for traditionall cardiovascular risk factors. Because in mice, inhibition of MIF resultedd in a shift in the cellular composition of atherosclerotic plaques towardd a stabilized phenotype, MIF may be a therapeutic target that warrantss further exploration in humans.
Acknowledgements Acknowledgements Wee thank the participants, general practitioners and staff in EPIC-Norfolk. Wee thank Anke Eerenberg for her expert help in the quantification of C-reactivee protein. EPIC-Norfolk is supported by programme grants from the Medicall Research Council UK and Cancer Research UK and with support fromm the European Union, Stroke Association, British Heart Foundation, Departmentt of Health, Food Standards Agency and the Wellcome Trust.

Reference s s 1.. Libby P. Inflammation in atherosclerosis. Nature 2002; 420: 868-874. 2.. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd,
Criquii M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC Jr, Taubertt K, Tracy RP, Vinicor F, Centers of Disease Control and Prevention, Americann Heart Association. Markers of inflammation and cardiovascular disease:: application to clinical and public health practice: A statement forr healthcare professionals from the Centers for Disease Control and Preventionn and the American Heart Association. Circulation 2003; 107:499-511. .
3.. Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration off interleukin-6 and the risk of future myocardial infarction among apparentlyy healthy men. Circulation 2000; 101:1767-1772.
4.. Pradhan AD, Manson JE, Rossouw JE, Siscovick DS, Mouton CP, Rifai N,, Wallace RB, Jackson RD, Pettinger MB, Ridker PM. Inflammatory biomarkers,, hormone replacement therapy, and incident coronary heartt disease: prospective analysis from the Women's Health Initiative observationall study. JAMA 2002; 288:980-987.
5.. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markerss of inflammation in the prediction of cardiovascular disease in women.. New England Journal of Medicine 2000; 342: 836-843.
6.. Jenny NS, Tracy RP, Ogg MS, Luong Ie A, Kuiler LH, Arnold AM, Sharrett AR, Humphriess SE. In the elderly, interleukin-6 plasma levels and the -174G>C polymorphismm are associated with the development of cardiovascular disease.. Arteriosclerosis Thrombosis and Vascular Biology 2002; 22: 2066-2071. .
7.. Brown DA, Breit SN, Buring J, Fairlie WD, Bauskin AR, Liu T, Ridker PM. Concentrationn in plasma of macrophage inhibitory cytokine-1 and risk of cardiovascularr events in women: a nested case-control study. Lancet 2002; 359:: 2159-2163.
8.. Calandra T, Roger T. Macrophage migration inhibitory factor: a regulator of innatee immunity. Nature Reviews Immunology 2003; 3: 791-800.
9.. Lue H, Kleemann R, Calandra T, Roger T, Bernhagen J. Macrophage migrationn inhibitory factor (MIF): mechanisms of action and role in disease.. Microbes and Infection 2002; 4:449-460.
10.. Calandra T, Bernhagen J, Mitchell RA, Bucala R. The macrophage is an importantt and previously unrecognized source of macrophage migration inhibitoryy factor. Journal of Experimental Medicine 1994; 179:1895-1902.
11.. Fingerle-Rowson G, Koch P, Bikoff R, Lin X, Metz CN, Dhabhar FS, Meinhardtt A, Bucala R. Regulation of macrophage migration inhibitory factorr expression by glucocorticoids in vivo. American Journal of Pathology 2003;; 162:47-56.
12.. Roger T, David J, Glauser MP, Calandra T. MIF regulates innate immune responsess through modulation of Toll-lik e receptor 4. Nature 2001; 414: 920-924. .
13.. Leng L, Metz CN, Fang Y, Xu J, Donnelly S, Baugh J, Delohery T, Chen Y, Mitchelll RA, Bucala R. MIF signal transduction initiated by binding to CD74.. Journal of Experimental Medicine 2003; 197:1467-1476.
14.. Mitchell RA, Metz CN, Peng T, Bucala R. Sustained mitogen-activated proteinn kinase (MAPK) and cytoplasmic phospholipase A2 activation by macrophagee migration inhibitory factor (MIF). Regulatory role in cell
193 3

proliferationn and glucocorticoid action. Journal of Biological Chemistry 1999;; 274:18100-18106.
15.. Lehmann LE, Novender U, Schroeder S, Pietsch T, von Spiegel T, Putensen C, Hoeftt A, Stuber F. Plasma levels of macrophage migration inhibitory factor aree elevated in patients with severe sepsis. Intensive Care Medicine 2001; 27:1412-1415. .
16.. Meazza C, Travaglino P, Pignatti P, Magni-Manzoni S, Ravelli A, Martini A, Dee Benedetti F. Macrophage migration inhibitory factor in patients with juvenilee idiopathic arthritis. Arthriti s and Rheumatology 2002; 46: 232-237.
17.. Yamaguchi E, Nishihira J, Shimizu T, Takahashi T, Kitashiro N, Hizawa N, Kamishimaa K, Kawakami Y. Macrophage migration inhibitory factor (MIF) inn bronchial asthma. Clinical and Experimental Allergy 2000; 30:1244-1249. .
18.. Lan HY, Yang N, Nikolic-Paterson DJ, Yu XQ, Mu W, Isbel NM, Metz CN, Bucalaa R, Atkins RC. Expression of macrophage migration inhibitory factor inn human glomerulonephritis. Kidney International 2003; 57:499-509.
19.. Lan HY, Yang N, Brown FG, Isbel NM, Nikolic-Paterson DJ, Mu W, Metz CN, Bacherr M, Atkins RC, Bucala R. Macrophage migration inhibitory factor expressionn in human renal allograft rejection. Transplantation 1998; 66: 1465-1471. .
20.. Donnelly SC, Haslett C, Reid FT, Grant IS, Wallace WA, Metz CN, Bruce LJ, Bucalaa R. Regulatory role for macrophage migration inhibitory factor in acutee respiratory distress syndrome. Nature Medicine 1997; 3: 320-323.
21.. Lai KN, Leung JC, Metz CN, Lai FM, Bucala R, Lan HY. Role for macrophage migrationn inhibitory factor in acute respiratory distress syndrome. Journal off Pathology 2003; 199:496-508.
22.. Lin SG, Yu XY, Chen YX, Huang XR, Metzz C, Bucala R, Lau CP, Lan HY. Dee novo expression of macrophage migration inhibitory factor in atherogenesiss in rabbits. Circulation Research 2000; 87:1202-1208.
23.. Schober A, Bernhagen J, Thiele M, Zeiffer U, Knarren S, Roller M, Bucalaa R, Weber C. Stabilization of atherosclerotic plaques by blockade off macrophage migration inhibitory factor after vascular injury in apolipoproteinn E-deficient mice. Circulation 2004; 109: 380-385.
24.. Burger-Kentischer A, Goebel H, Seiler R, Fraedrich G, Schaefer HE, Dimmelerr S, Kleemann R, Bernhagen J, Ihling C. Expression of macrophage migrationn inhibitory factor in different stages of human atherosclerosis. Circulationn 2002; 105:1561-1566.
25.. Day N, Oakes S, Luben R, Khaw KT, Bingham S, Welch A, Wareham N. EPIC-Norfolk:: study design and characteristics of the cohort. European Prospectivee Investigation of Cancer. British Journal of Cancer 1999; 80: 95-103. .
26.. Edfeldt K, Swedenborg J, Hansson GK, Yan ZQ. Expression of toll-lik e receptorss in human atherosclerotic lesions: a possible pathway for plaque activation.. Circulation 2002; 105:1158-1161.
27.. World Health Organization. WHO MONICA Project. MONICA Manual. 1990. Geneva. .
28.. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration off low-density lipoprotein cholesterol in plasma, without use of the preparativee ultracentrifuge. Clinical Chemistry 1972; 18:499-502.
29.. Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E. Elevation off tumor necrosis factor-alpha and increased risk of recurrent coronary

eventss after myocardial infarction. Circulation 2000; 101: 2149-2153. 30.. Blankenberg S, Tiret L, Bickel C, Peetz D, Cambien F, Meyer J, Rupprecht
HJ,, Atherogene Investigators. Interleukin-18 is a strong predictor of cardiovascularr death in stable and unstable angina. Circulation 2002; 106: 24-30. .
31.. Heeschen C, Dimmeler S, Hamm CW, Fichtlscherer S, Boersma E, Simoonss ML, Zeiher AM, CAPTURE Study Investigators. Serum level of thee antiinflammatory cytokine interleukin-10 is an important prognostic determinantt in patients with acute coronary syndromes. Circulation 2003; 107:: 2109-2114.
32.. Heeschen C, Dimmeler S, Hamm CW, van den Brand MJ, Boersma E, Zeiher AM,, Simoons ML, CAPTURE Study Investigators. Soluble CD40 ligand in acutee coronary syndromes. New England Journal of Medicine 2003; 348: 1104-1111. .
33.. Danesh J, Whincup P, Walker M, Lennon L, Thomson A, Appleby P, Gallimoree JR, Pepys MB. Low grade inflammation and coronary heart disease:: prospective study and updated meta-analyses. BMJ 2000; 321:199-204. .
34.. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation,, aspirin, and the risk of cardiovascular disease in apparently healthyy men. New England Journal of Medicine 1997; 336: 973-979.
35.. Bernhagen J, Calandra T, Mitchell RA, Martin SB, Tracey KJ, Voelter W, Manoguee KR, Cerami A, Bucala R. MIF is a pituitary-derived cytokine that potentiatess lethal endotoxaemia. Nature 1993; 365: 756-759.
36.. Nishihira J, Koyama Y, Mizue Y. Identification of macrophage migration inhibitoryy factor (MIF) in human vascular endothelial cells and its inductionn by lipopolysaccharide. Cytokine 1998; 10:199-205.
37.. Calandra T, Echtenacher B, Roy DL, Pugin J, Metz CN, Hultner L, Heumann D,, Mannel D, Bucala R, Glauser MP. Protection from septic shock by neutralizationn of macrophage migration inhibitory factor. Nature Medicinee 2000; 6:164-170.
38.. Kiechl S, Lorenz E, Reindl M, Wiedermann CJ, Oberhollenzer F, Bonora E,, Willei t J, Schwartz DA. Toll-lik e receptor 4 polymorphisms and atherogenesis.. New England Journal of Medicine 2002; 347:185-192.
39.. Boekholdt SM, Agema WR, Peters RJ, Zwinderman AH, van der Wall EE,, Reitsma PH, Kastelein JJ, Jukema JW. Variants of toll-lik e receptor 4 modifyy the efficacy of statin therapy and the risk of cardiovascular events. Circulationn 2003; 107: 2416-2421.
40.. Lee CD, Folsom AR, Nieto FJ, Chambless LE, Shahar E, Wolfe DA. White bloodd cell count and incidence of coronary heart disease and ischemic strokee and mortality from cardiovascular disease in African-American andd White men and women: atherosclerosis risk in communities study. Americann Journal of Epidemiology 2001; 154: 758-764.
41.. Brown DW, Giles WH, Croft JB. White blood cell count: an independent predictorr of coronary heart disease mortality among a national cohort. Journall of Clinical Epidemiology 2001; 54: 316-322.
195 5

196 6














![Renard-17-30Maig13.ppt [Modo de compatibilidad]CASO CLINICO • Sobrina de 23 años : • Calcio 10,9 mg/dl • Fósforo 2,6 mg/dl • Magnesio 2,2 mg/dl • Creatinina 0,94 mg/dl](https://static.fdocuments.net/doc/165x107/5fe880661572c17d762f0376/renard-17-modo-de-compatibilidad-caso-clinico-a-sobrina-de-23-aos-a-calcio.jpg)


