
Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma : A case...
5
APMIS 96: 206-210, 1988 Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma A case report DENIS BAILEY’, REUBEN BAUMAL’ and ALEXANDER MARKS’ The Departments of Pathology, ‘Toronto General Hospital, ’The Hospital for Sick Chrildren, and University of Toronto, and 3Banting and Best Department of Medical Research, University of Toronto Bailey, D., Baumal, R. & Marks, A. Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma. APMIS 96; 206-2 10, 1988. Chest x-ray in a 20-year-old man showed a large anterior mediastinal mass and a neddle aspirate was diagnosed by light microscopy (LM) as non-Hodgkin’s lymphoma. Treatment with CHOP (cyclophos- phamide, adriamycin, vincristine and prednisone) was ineffective and a tissue biopsy was performed. LM showed large, non-cohesive cells with abundant cytoplasm and rounded nuclei. Differential diagnoses included malignant lymphoma, seminoma, thymoma, anaplastic carcinoma, malignant melanoma and paraganglioma. Electron microscopy was not conclusive and immunoperoxidase staining was camed out. The malignant cells were negative for common leukocyte antigen, Leu M 1, alpha-fetoprotein, chorionic gonadotrophin, cytokeratin, epithelial membrane antigen, carcinoembryonic antigen, S- 100 protein and neuron-specific enolase but positive for placental alkaline phosphatase. In addition, there was strong positivity with a monoclonal antibody (mAb) which was recently shown to react with testicular seminomas. This case illustrates the value of this mAb in confirming the diagnosis of mediastinal seminoma. Key words: Anti-seminoma monoclonal antibody; mediastinal seminoma. R. Baumal, Department of Pathology, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario, Canada MSG 1x8. The presence of a mass in the anterior me- diastinum suggests a differential diagnosis which includes thymoma, malignant lymphoma (either Hodgkin’s or non-Hodgkin’s), metastatic car- cinoma, paraganglioma and extragonadal germ cell neoplasm (Ackerrnan and Rosai 1974). How- ever, it may be difficult to distinguish these solely by light microscopy (LM) or electron microscopy (EM).When a definite diagnosis is not obtained by these procedures, immunohistochemistry using various polyclonal and monoclonal antibodies (mAb) may be helpful. The present report de- scribes a patient with an anterior mediastinal mass who underwent a needle aspirate. LM examina- Accepted as submitted October 2, 1987. 206 tion of the aspirate suggested a diagnosis of non- Hodgkin’s lymphoma but the patient did not respond as expected to a course of CHOP. A tissue biopsy was then carried out and examination of this raised the possibility that the tumour was actually a mediastinal seminoma; this impression was confirmed by immunoperoxidase (IMP) stain- ing using an anti-seminoma mAb. CASE REPORT A 20-year-old man, who had previously been in good health, presented with a one-month history of non-pro- ductive cough and increasing shortness ofbreath. A chest X-ray showed a large anterior mediastinal mass with tracheal compression and the patient was referred to
-
Upload
denis-bailey -
Category
Documents
-
view
218 -
download
2
Transcript of Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma : A case...
APMIS 96: 206-210, 1988
Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma
A case report
DENIS BAILEY’, REUBEN BAUMAL’ and ALEXANDER MARKS’
The Departments of Pathology, ‘Toronto General Hospital, ’The Hospital for Sick Chrildren, and University of Toronto, and 3Banting and Best Department of Medical Research, University of Toronto
Bailey, D., Baumal, R. & Marks, A. Use of anti-seminoma monoclonal antibody to confirm the diagnosis of mediastinal seminoma. APMIS 96; 206-2 10, 1988.
Chest x-ray in a 20-year-old man showed a large anterior mediastinal mass and a neddle aspirate was diagnosed by light microscopy (LM) as non-Hodgkin’s lymphoma. Treatment with CHOP (cyclophos- phamide, adriamycin, vincristine and prednisone) was ineffective and a tissue biopsy was performed. LM showed large, non-cohesive cells with abundant cytoplasm and rounded nuclei. Differential diagnoses included malignant lymphoma, seminoma, thymoma, anaplastic carcinoma, malignant melanoma and paraganglioma. Electron microscopy was not conclusive and immunoperoxidase staining was camed out. The malignant cells were negative for common leukocyte antigen, Leu M 1, alpha-fetoprotein, chorionic gonadotrophin, cytokeratin, epithelial membrane antigen, carcinoembryonic antigen, S- 100 protein and neuron-specific enolase but positive for placental alkaline phosphatase. In addition, there was strong positivity with a monoclonal antibody (mAb) which was recently shown to react with testicular seminomas. This case illustrates the value of this mAb in confirming the diagnosis of mediastinal seminoma.
Key words: Anti-seminoma monoclonal antibody; mediastinal seminoma.
R. Baumal, Department of Pathology, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario, Canada MSG 1x8.
The presence of a mass in the anterior me- diastinum suggests a differential diagnosis which includes thymoma, malignant lymphoma (either Hodgkin’s or non-Hodgkin’s), metastatic car- cinoma, paraganglioma and extragonadal germ cell neoplasm (Ackerrnan and Rosai 1974). How- ever, it may be difficult to distinguish these solely by light microscopy (LM) or electron microscopy (EM). When a definite diagnosis is not obtained by these procedures, immunohistochemistry using various polyclonal and monoclonal antibodies (mAb) may be helpful. The present report de- scribes a patient with an anterior mediastinal mass who underwent a needle aspirate. LM examina-
Accepted as submitted October 2, 1987.
206
tion of the aspirate suggested a diagnosis of non- Hodgkin’s lymphoma but the patient did not respond as expected to a course of CHOP. A tissue biopsy was then carried out and examination of this raised the possibility that the tumour was actually a mediastinal seminoma; this impression was confirmed by immunoperoxidase (IMP) stain- ing using an anti-seminoma mAb.
CASE REPORT
A 20-year-old man, who had previously been in good health, presented with a one-month history of non-pro- ductive cough and increasing shortness ofbreath. A chest X-ray showed a large anterior mediastinal mass with tracheal compression and the patient was referred to

MAB AGAINST MEDIASTINAL SEMINOMA
hospital. His past medical history was unremarkable. He had not had fever, night sweats, weight loss or haemopt- ysis. Physical examination was normal except for wheez- ing and an area of dullness to percussion over the left anterior chest. There was no lymphadenopathy or hep- atosplenomegaly, and no testicular mass was detected. Laboratory studies showed normal haematology, urinal- ysis and blood chemistry.
A needle aspiration biopsy ofthe mediastinal mass was interpreted as positive for malignant cells, consistent with non-Hodgkin’s lymphoma. On this basis, the pa- tient was started on a course of CHOP therapy (cy- clophosphamide, 750 mg/m2; adriamycin, 50 mg/m2; vincristine, 2 mg and prednisone, 25 mg four times a day for 5 days), but the mass did not shrink appreciably. A mediastinoscopic directed tissue biopsy was then per- formed under local anaesthesia to confirm the diagnosis. The tissue obtained was examined by LM, EM and IMP staining. IMP staining indicated that the tumour was actually a seminoma. The patient was given a 5-day chemotherapeutic regimen, including bleomycin, cis- platinum and VP- 16, which was considered clinically to be more appropriate for this type of tumour. He was lost to follow-up before treatment was completed.
MATERIALS AND METHODS
Slides of the needle aspirate of the mass were fixed in ethanol and stained with the Papanicolaou stain. The tissue obtained from the mediastioscopic biopsy was divided into 3 portions. The first was fixed in 10% neutral buffered formalin for LM. Sections were cut at 4p thickness and stained with haemotoxylin and eosin (H and E). In addition, IMP staining was performed on the formalin-fixed tissue sections using the peroxidase-anti- peroxidase method of Sternberger and associates (Srein- herger et a/. 1970). The following antibodies were used: mouse mAb to common leukocyte antigen, Leu M1 (both from Becton-Dickenson, Mountain View, Cal.), epithelial membrane antigen (Dakopatts, Copenhagen, Denmark) and placental alkaline phosphatase (Dr. A . Epenetos, Hammersmith Hospital, London, England) and rabit antibodies to cytokeratin, S-100 protein, neu- ron-specific enolase, carcinoembryonic antigen, alpha- fetoprotein and chorionic gonadotropin (all from Dako- patts). The second portion of the biopsy was fixed in glutaraldehyde, cut at 50 nm, stained with uranyl acetate and lead citrate and examined by EM on a Philips 300 electron microscope. The third portion was snap frozen in OCT compound, cut into 6 1 sections, and used for IMP staining by the indirect method using a mouse mAb (M2A) (ascitic fluid diluted 1 : 100) which has been shown to react with seminomas ofthe testis and dysgerminomas of the ovary (Bailey er a/. 1986). In the case of the mAb, peroxidase-conjugated anti-mouse immunoglobulin was used for staining (Bailey er a/. 1986). Negative controls consisted of normal rabbit serum and mouse ascites.
Fig. 1. Light microscopy of needle aspirate of anterior mediastinal mass, showing cluster of anaplastic malig- nant cells. Papanicolaou stain. Mag X 300.
RESULTS
LM of the Papanicolaou-stained smear obtained by needle aspiration from the mediastinal mass showed anaplastic malignant cells consistent with non-Hodgkin’s lymphoma (Fig. 1).
LM of H and E stained slides (Fig. 2) showed several fragments of tissue with extensive crush artefact. In the better preserved areas, there was an infiltrate consisting of large non-cohensive cells with well-defined borders, abundant eosinophilic cytoplasm and round to oval nuclei. In one area, the infiltrate appeared to invade skeletal muscle. Individual cell necrosis was not uncommon, but there were no extensive areas of necrosis. Mitoses were rare. Scattered among the large tumour cells were small lymphocytes, sometimes in aggregates. The cells in the infiltrate showed granular cytoplas- mic staining by PAS which was diastase sensitive, indicating the presence of glycogen. The differen- tial diagnosis included non-Hodgkin’s lymphoma
207

BAILEY o al.
Fig 2. Light microscopy of mediastinoscopic biopsy ofanterior mediastinal mass, showing large non-cohesive tumour cells with round nuclei. Haematoxylin and eosin. Mag X 200.
(large cell type), Hodgkin’s disease, seminoma (primary or metastatic), anaplastic thymoma, anaplastic carcinoma, malignant melanoma and paraganglioma. Special stains for mucin and melanin were negative.
By EM, the infiltrate consisted of large cells with a high nucleo-cytoplasmic ratio. The nuclei were round and giant nucleoli, with a loose nucleolone- ma, were seen in some of the cells. The cytoplasm contained many organelles, including Golgi ap- paratus, mitochondria, lysozymes and smooth endoplasmic reticulum, as well as lipid inclusions and glycogen. No filaments were present. The cell surfaces showed projections, blebs and rare primi- tive junctions but no desmosomes. The EM results were interpreted as being suggestive of seminoma.
IMP staining of both formalin-fixed and frozen tissue sections showed that the malignant cells were negative for common leukocyte antigen, Leu M 1, alpha-fetoprotein, human chorionic go-
208
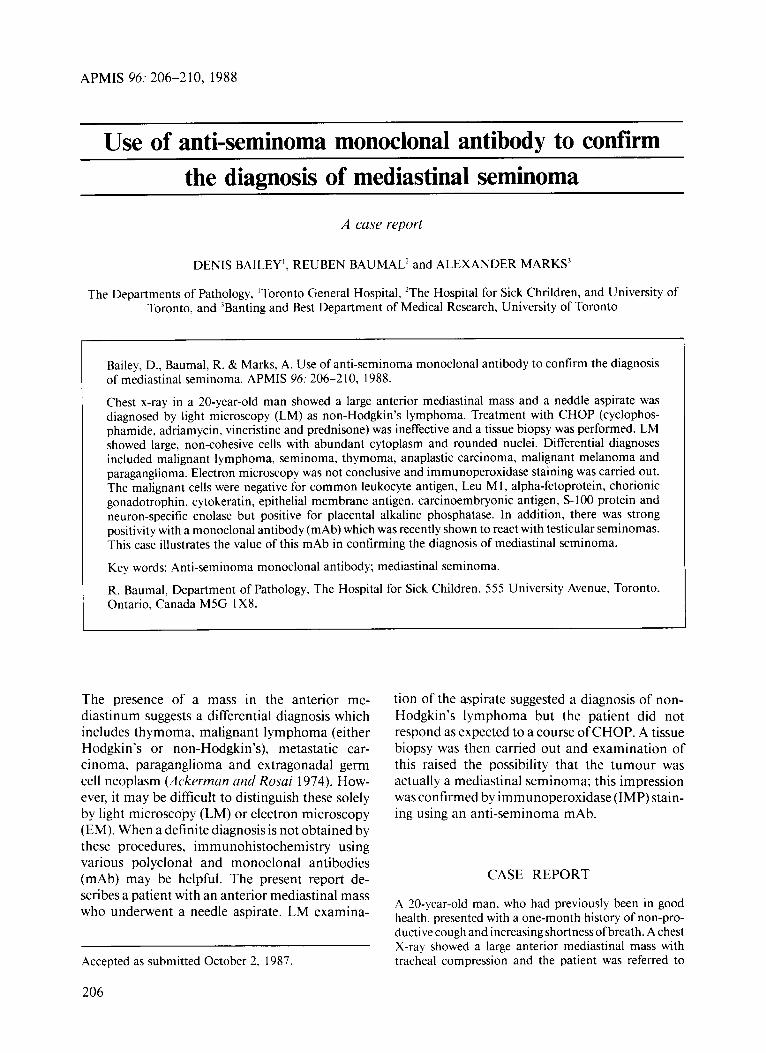
nadotropin, cytokeratin, epithelial membrane antigen, carcinoembryonic antigen, S- 100 protein and neuron-specific enolase but positive for pla- cental alkaline phosphatase. In addition, IMP staining of frozen tissue sections showed strong plasma membrane positivity of the malignant cells with the anti-seminoma mAb M2A (Fig. 3 ) .
DISCUSSION
Initial diagnosis in this patient on the basis of a needle aspirate of the anterior mediastinal mass was non-Hodgkin’s lymphoma. However, when his response to a course of CHOP was incomplete, a tissue biopsy was performed. LM did not provide conclusive proof for a specific diagnosis but sug- gested a number of possibilities. As a result, further studies were done using IMP staining. IMP was
MAB AGAINST MEDIASTINAL SEMINOMA
(?
s. %@ B 4,
Fig 3 lmmunoperoxidase staining of mediastinoscopic biopsy of anterior mediastinal mass, showing A) positive staining of the plasma membrane of tumour cells with anti-seminoma monoclonal antibody M2A (left panel) and B) no staining of the tumour cells with a non-specific ascites (right panel). Mag X 200.
negative for the epithelial markers cytokeratin, epithelial membrane antigen and carcinoembry- onic antigen, pointing away from a diagnosis of thymoma or carcinoma. Common leukocyte anti- gen and Leu MI were also negative, making the diagnoses of non-Hodgkin’s lymphoma and Hodgkin’s disease unlikely. In addition, S- 100 protein and neuron-specific enolase were negative, which probably excluded a diagnosis of malignant melanoma and paraganglioma respectively. Final- ly, negative staining for alpha-fetoprotein and chorionic gonadotrophin appeared to exclude ele- ments of non-seminomatous germ cell tumours. However, positive IMP staining of the malignant cells was observed with mAb to placental alkaline phosphatase, which is seen in many but not all seminomas (Uchidu et ul. 198 1 , Bluustein 1982, Puivu et a/. 1983, Epenetos et a/. 1984) and with the anti-seminoma mAb M2A, which is seen in all seminomas (Builcy et a/. 1986). Moreover, the fact
that mAb to placental alkaline phosphatase often shows positive IMP staining with non-seminoma- tous germ cell tumors, while the anti-seminoma mAb M2A does not, emphasizes the superiority of the latter for the diagnosis of testicular and extra- testicular seminomas. Hence, we feel that the correct diagnosis of our case was mediastinal seminoma, a possibility which had been raised by EM.
Seminomas account for approximately 40% of primary testicular tumous, whereas dysgermi- nomas, their counterparts in women, account for 1-2% of primary ovarian tumous (Bluustein 1982, Most& 1973). In addition, embryonal nests of germ cells may give rise to extragonadal semi- nomas and dysgerminomas in the mediastinum (Bush eta/. 198 I) , retroperitoneum (Houston el a!. 197 1 ) and supra-sellar region of the brain (Kasper et al. 1983). The anterior mediastinal mass in the patient reported here presumably arose from em-
209

BAILEY ('i ui.
bryonic nests of germ cells in the mediastinum. Although most seminomas have a typical appear- ance by LM (Le., they are clasical seminomas) and present no problem in diagnosis, some may be anaplastic and difficult to diagnose using morpho- logical criteria alone (Mostofi and Price 1973), especially if only small amounts of tissue are available for examination. Attempts to confirm the diagnosis of such tumours by immunohisto- chemical techniques have been frustrated by the lack of antibodies directed against specific anti- genic markers associated with seminoma cells. Placental alkaline phosphatase has been used in immunohistochemical studies as a marker for seminomas (Uchida et al. 198 1, Paiva et al. 1983, Epenetos et al. 1984), including mediastinal semi- nomas (Burns andMcCaughey 1986), but variable results have been obtained. The recent characteri- zation of an anti-seminoma mAb (M2A), which produced positive IMP staining of the seminoma type of testicular tumour but no other germ cell or extragonadal tumours or normal adult tissues, has proved to be a reliable marker for seminomas of the testis (Bailey et al. 1986). In the present study, this mAb has also been shown to be satisfactory for the diagnosis of an extragonadal seminoma. Previ- ously, it was shown to react with foetal testis, indicating that it was directed against an onco- foetal antigen and was characterized as a glyco- protein of molecular weight 40,000 (Bailey et al. 1986). Reactivity with mAb M2A of the malignant cells constituting the mediastinal mass in this case of mediastinal seminoma was an indispensable aid in diagnosis.
This work was supported by the National Cancer Insti- tute of Canada. The paper was prepared with the assistance of the Medical Publications Department, The Hospital for Sick Children, Toronto.
REFERENCES
Ackrrman. L. V. & Rosai, J. (Eds.): Mediastinum, Surgical pathology, fifth edition. The C. V. Mosby Co., St. Louis 1974, p. 274.
Bailej., D., Buurnal, R., Law, J., Sheldon, K., Kannam- puzha, P., Stratis, M., Kahn, H. & Marks, A,: Production of a monoclonal antibody specific for seminomas and dysgerminomas. Proceedings of the National Academy of Sciences (USA) 83: 5291- 5295, 1986.
Bluustein, A . (Ed.): Pathology ofthe female genital tract, second edition. Springer-Verlag, New York. 1982, p. 603.
Biirns, B. F. & McCatcghey, W. T. E.: Unusual thymic seminomas. Archives of Pathology and Laboratory Medicine 110: 539-541, 1986.
Bush, S. E., Martinez, A. & Bagshaw. M. A.: Primary mediastinal seminoma. Cancer 48: 1877- 1882, 1981.
E p m t m , A . A., Truvers, P., Gutter, K. C., Olivec R. D., Mason, D. Y. & Bodrner, W. F.: An immunohisto- logical study of testicular germ cell tumours using two different monoclonal antibodies against placen- tal alkaline phosphatase. British Journal of Cancer
Houston, R. R., HJinlhec C. C., Smith, J. P. & Brenner, M. A , : Primary retroperitoneal seminoma without gonadal involvement: a report of 3 cases. Journal of Urology 106: 841-844, 1971.
Kasper, C. S., Schneider, N . R., Childers, J. H. & Wilson, J. D.: Suprasellar germinoma: unresolved problems in diagnosis, pathogenesis, and management. Amer- ican Journal of Medicine 75: 705-7 1 1, 1983.
Mostqfi, F. J.: Testicular tumors: epidemiologic, etiolog- ic, and pathologic features. Cancer 32: 1 186-120 1, 1973.
Mostqfi, F. K. & Price, E . B.. Jr. (Eds.): Tumors of the male genital system. Armed Forces Institute of Pathology, Washington, second series, fascicle 8, pp.
Paiva, J., Darnjunov. I . , Lange, P. H. & Harns, H.: Immunohistochemical localization of placental-like alkaline phosphatase in testis and germ-cell tumors using monoclonal antibodies. American Journal of
Sternherger. L. A. , Hardy, P. H., Jr., Cuculis, J. J. & Mejvr, H . G.: The unlabeled antibody enzyme method of immunohistochemistry: preparation and properties of soluble antigen-antibody complex (horseradish-peroxidase-antihorseradish peroxi- dase) and its use in identification of spirochetes. Journal of Histochemistry and Cytochemistry 18:
Uchida, T., Shimodu, T., Miyata, H., Shikuta. T., Iiono, S., Suzuki, H., Odu, T., Hiruno, K & Sigiura, M.: Immunoperoxidase study ofalkaline phosphatase in testicular tumor. Cancer 48: 1455-1462, 1981.
49: 11-15, 1984.
1-310, 1973.
Pathology 111: 156-165, 1983.
3 15-333, 1970.
210

















![Does primary tumor localization has prognostic importance ... · groups; seminoma and non-seminoma. The group called pure seminoma constitutes approximately 60% of the whole GCT [1,2].](https://static.fdocuments.net/doc/165x107/5f3d5bded6321624f4620c6d/does-primary-tumor-localization-has-prognostic-importance-groups-seminoma-and.jpg)