upper git bleeding
27
Upper Gastrointestinal Bleeding PROF/ GOUDA ELLABBAN
-
Upload
scu-hospital -
Category
Health & Medicine
-
view
66 -
download
0
Transcript of upper git bleeding

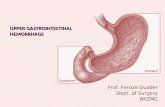
Upper Gastrointestinal
Bleeding PROF/ GOUDA ELLABBAN

It is an acute bleeding occurring from a lesion proximal to the level of Treitz ligament .
Definition

Treitz ligament is a well defined peritoneal fold that ascend to the Rt. Crus of the diaphragm & it demarcate the dudeno-jejunal junction.

Etiology
General Local

Hemorrhagic hereditary
telangactasia.
anticoagulant
thrombocytopenia
leukemia
hemophilia
Bleeding diathesis
General

Local GI Problem
Chronic peptic ulcer 65%
Acute peptic ulcer Multiple erosions
Esophageal varieces30%
Ca of stomach Mallory-Weiss synd PU in meckles Hemophilia Purpura Anemia
5%

Classification according to anatomical locations :
Esophagus: Varieces, peptic esophegitis, foreign body &
rarely Ca. Stomach: Peptic ulcer, gastric erosion, gastritis, Ca, hiatus
hernia, Mallory Weiss syndrome. Duodenum (commonest): Peptic ulcer, diverticulim.

Cont:
Miscellaneous: Aneurysm of splenic artery, uremia,
disorder of GI blood vessels.

Clinical features
General apearance:pale, anxious w/ moderate to sever Hg, sweating or shock.
Vital signs: hypotension, tachycardia, fever if associated with infection, shallow & rapid breathing.
skin: jaundice, palmer erythema, spider navei & other signs of portal HTN including gynecomastia.

Cont:
Head & neck: pale or dry mucous memb. Abdomen: distention, bowle sound
increase, tenderness, ascites, hepatosplenomegaly.

1) Peptic ulcer dis
Despite the decrease in the frequency of peptic ulcer dis in the last 3 decades it remains the most common cause of upper GI bleeding.
Most duodenal ulcers are located in the post wall pf duodenal bulb just beyond the pylorice.
Majority of gastric ulcers are located in the lesser curvature.

Cont;
Bleeding from a gastric ulcer is more severe than a duodenal ulcer.
Approximately ¾ of these bleeding will stop spontaneously.

Treatment
Medical treatment Surgical
treatment( duodenal ulcer)
1. Selective vagotomyA-highly selective cell
vagotomyB-vagotomy &
antrectomy

Cont;
C-vagotomy & pyloroplasty.
Gastric ulcer:
Distal gastrectomy to include the ulcer.

2) Esophageal varices
It take place anywhere from the lesser curvature upward into the esophagus.

Treatment
Medical treatment:
1. Somatostatin administration.
2. Balloon tamponad. Surgical treatment:
1. Esophageal devascularisation by:
Transection & reanastomosis

3) Esophagitis & Gastritis. 4) stress induced bleeding (as seen after head trauma or surgery). 5) use of medications (NSAIDs, i.e., aspirin). 6) Mallory-Weiss Tear .7) Esophageal Cancer and Stomach Cancer.

Mallory-Weiss Tear

Diagnosis
CORRECT the hypovolemia & the shock then take a good HX of peptic ulcer, liver dis, any NSAID ingestion or any predisposition cause.
Physical EX Investigation:1. NG tube to differ upper from lower
bleeding.

Cont:
1. Fibroptic endoscopy which will detect 80-90%.
2. Fibroptic esophgeogastroduodenoscopy.
3. Barium meal.
4. arteriography(only if bleeding is more than 1-2ml/min.

Cont:
The aim of investigation is to:
1. Pin point the exact cause of bleeding.
2. To asses the effect of bleeding on the pt.
3. To plan for treatment.

Treatment
Upper GI bleeding stops spontaneously in about 80-90% of pt.
1. Endoscopic coagulation(eg:injection sclerosis, heater probes, laser)
2. Infusion of vasopressin or embolic therapy by angiography.
3. Specific surgical treatment.

Cont;
Surgical treatment should be done within 48hrs of bleeding based on indication for surgery & failure of conservative management.
Absolute indication for surgery:1. Deterioration of vital signs in spite of IV
resuscitation.2. Inability to correct hypovolemia with 2L of bld.3. Bld loss/requirement estimated at > 4 units of
bld/24hrs.

Cont;
1. Visible bleeding vessel visualized by endoscopy.
2. Presence of co-existing lesion.
Relative indication:
3. Massive Hrg in pt > 60y
4. Previous major bleeding episode.
5. Past Hx of recurrent bleeds, ch ulcer, arteriosclerosis.

Cont;
Factors affecting prognosis:
1. Old age >60y
2. Shock on admission
3. Gastric ulcer
4. Ch liver dis
5. Arterial spurting from ulcer, visible vessel in ulcer base, adherent fresh clot.

Cont;
Prognosis: Overall mortality 10% >80y 20%

Thank you