Unrestricted Use of Drug-Eluting Stents Compared with Bare-Metal Stents in Routine Clinical...
18
Unrestricted Use of Drug- Unrestricted Use of Drug- Eluting Stents Compared with Eluting Stents Compared with Bare-Metal Stents in Routine Bare-Metal Stents in Routine Clinical Practice: Findings Clinical Practice: Findings From the National Heart, Lung, From the National Heart, Lung, and Blood Institute Dynamic and Blood Institute Dynamic Registry Registry J. Dawn Abbott, MD, FACC,* Matthew R. Voss, MD,* Mamoo Nakamura, MD,† Howard A. Cohen, MD, FACC,‡ Faith Selzer, PHD,† Kevin E. Kip, PHD, Helen A. Vlachos, MSC,†Robert L. Wilensky, MD, FACC,§ David O. Williams, MD, FACC* Providence, Rhode Island; Pittsburgh and Philadelphia, Pennsylvania; and New York, New York Abbott, J. D. et al. J Am Coll Cardiol 2007;50:2029-36
-
Upload
derek-mccoy -
Category
Documents
-
view
228 -
download
0
Transcript of Unrestricted Use of Drug-Eluting Stents Compared with Bare-Metal Stents in Routine Clinical...

Unrestricted Use of Drug-Eluting Stents Unrestricted Use of Drug-Eluting Stents Compared with Bare-Metal Stents in Compared with Bare-Metal Stents in
Routine Clinical Practice: Findings From Routine Clinical Practice: Findings From the National Heart, Lung, and Blood the National Heart, Lung, and Blood
Institute Dynamic RegistryInstitute Dynamic Registry
Unrestricted Use of Drug-Eluting Stents Unrestricted Use of Drug-Eluting Stents Compared with Bare-Metal Stents in Compared with Bare-Metal Stents in
Routine Clinical Practice: Findings From Routine Clinical Practice: Findings From the National Heart, Lung, and Blood the National Heart, Lung, and Blood
Institute Dynamic RegistryInstitute Dynamic Registry
J. Dawn Abbott, MD, FACC,* Matthew R. Voss, MD,* Mamoo Nakamura, MD,† Howard A. Cohen, MD, FACC,‡ Faith Selzer, PHD,† Kevin E. Kip, PHD, Helen A. Vlachos, MSC,†Robert L.
Wilensky, MD, FACC,§ David O. Williams, MD, FACC*
Providence, Rhode Island; Pittsburgh and Philadelphia, Pennsylvania; and New York, New York
Abbott, J. D. et al. J Am Coll Cardiol 2007;50:2029-36

Drug-eluting vs. Bare Metal Drug-eluting vs. Bare Metal Stents: BackgroundStents: BackgroundDrug-eluting vs. Bare Metal Drug-eluting vs. Bare Metal Stents: BackgroundStents: Background Stents are utilized almost uniformly in patients
undergoing percutaneous coronary intervention Until recently, drug-eluting stents have been the
preferred treatment Some have raised concerns that drug-eluting stents may
be associated with more frequent stent thrombosis leading to excess death and MI
Robust comparisons of drug-eluting and bare metal stents have been limited to highly selected, simple patient subgroups.
Comparisons between DES and BMS for non-protocol usage in North America have been limited

Drug-eluting vs. Bare Metal Drug-eluting vs. Bare Metal Stents: Purpose of InvestigationStents: Purpose of InvestigationDrug-eluting vs. Bare Metal Drug-eluting vs. Bare Metal Stents: Purpose of InvestigationStents: Purpose of Investigation
In the setting of routine clinical practice to: Determine and compare the baseline clinical and
angiographic features, procedural strategies and clinical outcomes of patients treated with a bare metal and drug-eluting stent
Compare outcomes following adjustments for baseline imbalances

Dynamic RegistryDynamic RegistryDynamic RegistryDynamic Registry Prospective observational multicenter study Enrollment of sequential “waves” of consecutive
patients having coronary intervention Exclusion: Refusal or inability to provide written
informed consent 2000 patients per wave separated by 18 months Trained research coordinators collect data Oversampling of women and minorities Follow-up obtained by phone at 30 days, 6 months, 1
year Funding just received to follow patients for five years

Study DesignStudy Design
Identified patients treated with DES in Wave 4 (2004) and compared them to patients treated with a BMS in Wave 3 (2002)
Wave 3 represented the last wave before the routine availability of DES
Intent of excluding wave 4 BMS patients was to eliminate selection bias seen in Wave 4
Patients treated with BMS in Wave 3 would likely have been treated with DES had one been available
One-year follow-up data was available in 93% of wave 3 patients and 96% of wave 4 patients

DES vs. BMS: Study PopulationDES vs. BMS: Study PopulationBMS Era
October 2001 to March 2002N=2047
DES EraFebruary to May 2004
N=2112
Exclude if no stentN=284
Exclude if only BMS or no stentN=652
BMS GroupN=1763
2551 lesions
DES GroupN=1460
1995 lesionsSES 59.8%PES 31.5%

Statistical AnalysisStatistical Analysis Univariate differences between BMS and DES
Categorical variables: chi-square test Continuous data: Wilcoxon rank-sum test
Cumulative one-year event rates Kaplan-Meier approach and compared by log-rank
statistic Multivariable analysis
Cox proportional hazards regression used to estimate unadjusted and adjusted hazard ratios of adverse clinical outcomes
Probability values <0.05 were considered significant

Variable BMS
n=1763
DES
n=1460
p-value
Mean Age (years) 64.4 63.7 0.07
% Female 35.8 33.3 0.14
Diabetes, % 29.1 34.3 0.001
Hypertension, % 74.1 79.1 0.001
Hypercholesterolemia, %69.8 77.5
<0.0001
Current smoking, % 24.4 21.4 0.05
Prior myocardial infarction, % 26.2 26.4 0.90
Prior coronary bypass, % 17.4 19.1 0.21
Prior angioplasty, % 27.3 32.4 0.002
Renal insufficiency 7.1 9.1 0.03
DES vs. BMS:Baseline Characteristics

Variable BMS
n=1763
DES
n=1460
p-value
Vessel Disease 0.098
Single 37.6 33.8
Double 32.0 32.5
Triple 30.1 33.5
Indication for procedure, %
<0.0001
Acute MI 29.8 23.8
Unstable Angina 39.9 35.9
Stable Angina 19.7 25
Other 10.6 15.3
Ejection Fraction, mean 51.5 52.3 0.09
Cardiogenic Shock 2.1 0.5 <0.0001
DES vs. BMS:Baseline Characteristics

Variable BMS
n=2551
DES
n=1995
p-value
Mean Reference Vessel Diameter
3.1 3.0 0.07
Mean Lesion Length 13.4 15.9 <0.0001
Lesion Types, %
Total Occlusion 9.2 7.4 0.03
Thrombus 15.4 11.0 <0.0001
Calcified 22.3 26.5 0.001
Bifurcation 13.2 10.2 0.002
Ostial 6.9 8.8 0.02
Lesion Tortuosity, %
None/Mild 75.0 73.2 0.19
Moderate/Severe Tortuosity 25 26.8
DES vs. BMS:Attempted Lesion Characteristics

DES vs. BMS: DES vs. BMS: Procedural Characteristics
DES vs. BMS: DES vs. BMS: Procedural Characteristics
BMS
n= 2551
DES
n=1995
p-value
Lesion Complication, %
Abrupt Closure 0.2 0.0 0.03
Dissection 1.9 2.1 0.80
Side Branch Occlusion 2.1 2.2 0.85
Persistent flow reduction
0.7 0.9 0.68
Procedural Success, % 0.16
Complete 96.5 97.3
Partial 3.2 2.2
Failure 0.3 0.5
Angiographic success, % 97.5 98.0 0.33

Variable BMS
n=1763
DES
n=1460
p-value
Death 4.3 3.6 0.32
MI 4.7 4.6 0.93
CABG 3.1 1.2 <0.001
Target Vessel Revascularization
9.2 5.0 <0.001
Repeat PCI 12.7 9.0 0.001
MACE
(Death, MI, Repeat Revascularization)
20.9 15.5 <0.001
DES vs. BMS: DES vs. BMS: Cumulative Unadjusted One-Year Event Rates

Stent ThrombosisStent Thrombosis
Definite stent thrombosis reported Over 1 year 1.0% of DES patients (n=14)
0.8% (n=11) subacute 0.2% (n=3) late
Data were not collected during wave 3 not available for BMS patients

DES vs. BMS: Adjusted and Unadjusted Events at One-Year
DES vs. BMS: Adjusted and Unadjusted Events at One-Year
Adverse Outcome
HR
95% CI
p-value
Death Unadjusted Adjusted
0.83 0.97
0.57-1.20 0.66-1.43
0.32 0.87
Myocardial infarction (MI) Unadjusted Adjusted
0.99 1.02
0.71-1.37 0.73-1.43
0.93 0.90
Coronary artery bypass graft Unadjusted Adjusted
0.39 0.34
0.22-0.68 0.19-0.60
<0.001 <0.001
Death/MI Unadjusted Adjusted
0.88 0.88
0.68-1.13 0.68-1.15
0.31 0.34
Repeat angioplasty Unadjusted Adjusted
0.69 0.65
0.55-0.87 0.52-0.82
0.001
<0.001 Repeat revascularization Unadjusted Adjusted
0.64 0.38
0.52-0.79 0.25-0.60
<0.001 <0.001
MACE Unadjusted Adjusted
0.72 0.67
0.60-0.85 0.56-0.81
<0.001 <0.001

Copyright ©2007 American College of Cardiology Foundation. Restrictions may apply.Abbott, J. D. et al. J Am Coll Cardiol 2007;50:2029-2036
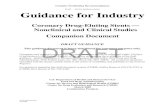
Adjusted Kaplan-Meier Event Curves at 1 Year Freedom from (A) Death/MI (B) Repeat RevascularizationAdjusted Kaplan-Meier Event Curves at 1 Year Freedom from (A) Death/MI (B) Repeat Revascularization

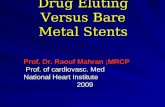
One-year Event Rates for complex lesion types According to Stent TypeOne-year Event Rates for complex lesion types According to Stent Type
BMS DES p-value n Percent n Percent Death or MI Bifurcation + 261 9.3 189 6.4 0.32 Bifurcation - 1502 8.6 1271 7.8 0.44 Ostial + 163 12.1 168 11.4 0.92 Ostial - 1600 8.3 1292 7.1 0.22 Thrombus + 329 13.1 189 10.9 0.45 Thrombus - 1434 7.7 1262 7.1 0.59 Calcification + 424 9.7 407 9.2 0.89 Calcification - 1339 8.3 1053 6.9 0.20 Ulceration + 282 9.8 225 9.5 0.91 Ulceration - 1481 8.5 1235 7.2 0.26 TO + 212 12.1 143 12.9 0.93 TO - 1551 8.2 1371 7.0 0.27 Any present 1053 10.3 852 8.6 0.24 None present 710 6.3 608 6.2 0.93 TVR via PCI† Bifurcation + 225 8.6 182 7.2 0.67 Bifurcation - 1229 9.3 1230 4.6 <0.001 Ostial + 137 10.5 163 5.6 0.12 Ostial - 1317 9.1 1249 4.9 <0.001 Thrombus + 258 7.6 190 3.4 0.058 Thrombus - 1196 9.6 1222 5.2 <0.001 Calcification + 362 9.3 399 6.2 0.11 Calcification - 1092 9.2 1013 4.5 <0.001 Ulceration + 225 5.9 220 5.1 0.70 Ulceration - 1229 9.8 1192 4.9 <0.001 TO + 168 8.6 136 2.3 0.023 TO - 1286 9.3 1276 5.2 <0.001 Any 871 8.8 828 5.2 0.004 None 583 9.9 584 4.6 <0.001 * Rates calculated using Kaplan-Meier methodology.

Copyright ©2007 American College of Cardiology Foundation. Restrictions may apply.Abbott, J. D. et al. J Am Coll Cardiol 2007;50:2029-2036
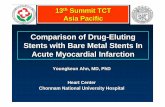
Adjusted HRs and 95% CIs for 1 Year (A) Death/MI (B) TVR

DES vs. BMS: ConclusionsDES vs. BMS: Conclusions DES as used in routine clinical practice in patients with
complex lesions resulted in a substantial reduction in clinically driven target vessel revascularization compared with BMS-treated patients
Overall risk of repeat revascularization after adjustment was 43% lower in DES patients
No excess hazard of death/MI and a low rate of stent thrombosis observed in DES patients at one-year
These findings support the use of DES in routine clinical practice
Extended follow-up is needed to determine incidence of very late stent thrombosis