Comparative effects of sirolimus-eluting versus bare metal stents on ...
description

Drug Eluting Drug Eluting Versus Bare Versus Bare Metal StentsMetal Stents
Prof. Dr. Raouf Mahran ;MRCPProf. Dr. Raouf Mahran ;MRCPProf. of cardiovasc. MedProf. of cardiovasc. Med
National Heart InstituteNational Heart Institute20092009


Evolution of PCIEvolution of PCI
19771977 : :Balloon Angioplasty (POBA)Balloon Angioplasty (POBA)
19941994 : :Bare Metal Stent (BMS)Bare Metal Stent (BMS)
20032003 : :Drug Eluting Stent (DES)Drug Eluting Stent (DES)

Coronary Angioplasty (PTCA) Coronary Angioplasty (PTCA) Andreas GruntzigAndreas Gruntzig

Coronary StentingCoronary StentingJulio PalmazJulio Palmaz


PCI Procedural refinements: PCI Procedural refinements: StentsStents
Expandable metal mesh tubes that buttresses the dilated segment, limit restenosis.
Drug eluting stents: further reduce cellular proliferation in response to the injury of dilatation.

What is a Drug-Eluting Stent (DES)What is a Drug-Eluting Stent (DES)??
DHHS/FDA/CDRH
Example: Cordis’ Cypher™ Sirolimus-Eluting Coronary Stent
Stent Platform & Stent Platform & Delivery SystemDelivery System
Carrier(s)Carrier(s)DrugDrug
Components

TAXUS TechnologyTAXUS Technology
Binds tubulinBinds tubulin
Microtubular Microtubular
dynamicsdynamics
MulticellularMulticellular
MultifunctionalMultifunctional
Binds tubulinBinds tubulin
Microtubular Microtubular
dynamicsdynamics
MulticellularMulticellular
MultifunctionalMultifunctional
PaclitaxelPaclitaxel PolymerPolymer PlatformPlatform
UniformityUniformity
DurabilityDurability
Biphasic Biphasic Controlled Controlled
Release Release KineticsKinetics
UniformityUniformity
DurabilityDurability
Biphasic Biphasic Controlled Controlled
Release Release KineticsKinetics
Express™ StentExpress™ Stent
Tandem Tandem
Architecture Architecture
FlexibilityFlexibility
Maverick™ Maverick™
Balloon Balloon
DeliverabilityDeliverability
Express™ StentExpress™ Stent
Tandem Tandem
Architecture Architecture
FlexibilityFlexibility
Maverick™ Maverick™
Balloon Balloon
DeliverabilityDeliverability

Drug-Eluting StentsDrug-Eluting Stents
The “HOLY GRAIL” of interventional The “HOLY GRAIL” of interventional cardiology is a stent with optimal cardiology is a stent with optimal
deliverability and scaffolding which is deliverability and scaffolding which is impervious to intimal hyperplasiaimpervious to intimal hyperplasia
The “HOLY GRAIL” of interventional The “HOLY GRAIL” of interventional cardiology is a stent with optimal cardiology is a stent with optimal
deliverability and scaffolding which is deliverability and scaffolding which is impervious to intimal hyperplasiaimpervious to intimal hyperplasia

Reduced Restenosis - EfficacyReduced Restenosis - Efficacy– Goal = <10% restenosis frequency for all patient Goal = <10% restenosis frequency for all patient
cohorts and all lesion subsetscohorts and all lesion subsets– Simulate normal wound healing with rapid Simulate normal wound healing with rapid
endothelialization and minimal (? no) neointima endothelialization and minimal (? no) neointima formation formation
Absence of Pathobiologic Responses - SafetyAbsence of Pathobiologic Responses - Safety– No early or late thrombosisNo early or late thrombosis– No “edge” hyperproliferative effectsNo “edge” hyperproliferative effects– No late aneurysms, delayed “catch-up” (late No late aneurysms, delayed “catch-up” (late
restenosis), accelerated atherosclerosisrestenosis), accelerated atherosclerosis
Clinical imperatives…Clinical imperatives…Drug-Eluting StentsDrug-Eluting Stents

Three Component SystemThree Component System
Stent designStent design
Pharmacologic Pharmacologic agentagent
Drug carrier Drug carrier vehiclevehicle
Drug-Drug-Eluting Eluting StentStent
Drug-Drug-Eluting Eluting StentStent
Drug-Eluting StentsDrug-Eluting Stents

Neointimal Hyperplasia (30%)Neointimal Hyperplasia (30%)Neointimal Hyperplasia (30%)Neointimal Hyperplasia (30%)
CausesCausesCausesCauses
SolutionSolutionSolutionSolution
1.1. A stent to block recoil and remodelingA stent to block recoil and remodeling2.2. A therapeutic agent to prevent neointimal hyperplasiaA therapeutic agent to prevent neointimal hyperplasia
Why DES??-Why DES??- Coz of Restenosis - Causes & Coz of Restenosis - Causes & SolutionSolution
Recoil & Negative Remodeling (70%)Recoil & Negative Remodeling (70%)


Growth Factors / Cytokines
RadiationActinomycin D, (DNA)
FKBP
S
G2
M
cell cycleG0
Rapamycin and Rapamycin and derivativesderivatives
X
Cell Division
Smooth muscle cell
• Signal
Transduction
Receptor
TOR
• Activation
p27, Cyclins/Cdks
Paclitaxel, (microtubules)
Therapeutic Mechanisms of Action
G1

Stent Design…Stent Design…
Optimized geometry for homogeneous drug Optimized geometry for homogeneous drug distribution (closed vs. open cell designs, distribution (closed vs. open cell designs, inter-strut distances)inter-strut distances)
Circumferential stent-vessel wall contact (to Circumferential stent-vessel wall contact (to insure drug delivery) - conformabilityinsure drug delivery) - conformability
Enhanced radiopacity for precise placement Enhanced radiopacity for precise placement (avoid overlap regions and inter-stent gaps)(avoid overlap regions and inter-stent gaps)
Maintained side-branch accessMaintained side-branch access
Advanced deliverability to complex anatomiesAdvanced deliverability to complex anatomies
Drug-Eluting StentsDrug-Eluting Stents

Drug Carrier Vehicle…requirementsDrug Carrier Vehicle…requirements
Non-inflammatory and non-thrombogenic Non-inflammatory and non-thrombogenic Predictable drug elution kinetics (timing Predictable drug elution kinetics (timing and dose)and dose)Elastomeric without surface integrity changes Elastomeric without surface integrity changes (e.g. cracking, peeling)(e.g. cracking, peeling)No alteration of incorporated drug activity No alteration of incorporated drug activity No alteration of the structural and operational No alteration of the structural and operational stent characteristicsstent characteristicsLogistic factors – sterilization, stability, shelf-life, Logistic factors – sterilization, stability, shelf-life, and expenseand expense
Drug-Eluting StentsDrug-Eluting Stents


Methods of Stent-Mediated DeliveryMethods of Stent-Mediated Delivery
StentStent
COOKCOOK
{ CORDIS CORDIS GUIDANTGUIDANT
Top-Top-coatcoat
Sub-Sub-layerlayer
22mm
55mm 55mm
}}
}
BioBiodivYsio divYsio Matrix HIMatrix HIBoston ScientificBoston Scientific BioBiodivYsio divYsio Matrix LOMatrix LO
}11mm 11mm
} + + + + +
CONOR-MedsystemsCONOR-Medsystems
Degradable inlaysDegradable inlays
Nanoporous Nanoporous ceramicceramic
SORINSORIN
JOMEDJOMED
DegradableDegradable stent stent
Igaki-TamaiIgaki-Tamai
Degradable polymerDegradable polymer
BiosensorBiosensor
PC coatingPC coating


RAVEL-Study (ESC, Stockholm, RAVEL-Study (ESC, Stockholm, September 2001) September 2001)
Bare Metal Bare Metal stentsstents
Cypher stentsCypher stents
PatientsPatientsN = 120N = 120N = 118N = 118
Results after 12 monthsResults after 12 months
RestenosisRestenosis26%26% 0 % 0 %

SIRIUSSIRIUS - Study Flow - Study FlowAll Randomized All Randomized
PatientsPatientsn = 1101n = 1101
All Randomized All Randomized PatientsPatientsn = 1101n = 1101
Sirolimus-elutingSirolimus-eluting Bx VELOCITY Bx VELOCITYTMTM
n = 533n = 533
Sirolimus-elutingSirolimus-eluting Bx VELOCITY Bx VELOCITYTMTM
n = 533n = 533
Control Control Bx VELOCITYBx VELOCITYTMTM
n = 525n = 525
Control Control Bx VELOCITYBx VELOCITYTMTM
n = 525n = 525
Angio FU at 8 Months = 85.4%
Clinical FU at 9 Months = 95.7%
Angio FU at 8 Months = 85.4%
Clinical FU at 9 Months = 95.7%Angio FU at 8 Months = 84.7%
Clinical FU at 9 Months = 95.8%
Angio FU at 8 Months = 84.7%
Clinical FU at 9 Months = 95.8%
De-registeredSirolimus-elutingBx VELOCITYTM
(n=23)
De-registeredSirolimus-elutingBx VELOCITYTM
(n=23)
De-registeredControl
Bx VELOCITYTM
(n=20)
De-registeredControl
Bx VELOCITYTM
(n=20)

FIM- Two Sites, 45 patients
0% Restenosis
RAVEL Multicenter, Randomized 238 patients
0% Restenosis
SIRIUS 400- Multicenter, Randomized 400 pts
9.2% Restenosis
SIRIUS Final Results 1058 pts
8.9% Restenosis
The Realism of Drug Eluting StentsThe Realism of Drug Eluting Stents
Than
NOW
Than
First
MACE at MACE at 24 Months24 Months
5/45=11.1%5/45=11.1%
MACE at MACE at 24 Months24 Months
5/45=11.1%5/45=11.1%








Current Indications for Drug-Current Indications for Drug-eluting Stentseluting Stents::
1.1. Why do we need DES ?Why do we need DES ?
2.2. Which DES should we use ? Which DES should we use ?
3.3. Indications for DES ? Indications for DES ?

RestenosisRestenosis
Elastic recoilElastic recoil: : after balloon deflation, the large after balloon deflation, the large number of elastic fibers in the tunica media number of elastic fibers in the tunica media
cause a mechanical collapsecause a mechanical collapse . .
Neointimal proliferation (NI):Neointimal proliferation (NI): formation of an inner formation of an inner layer at the site of injury, composed of cells layer at the site of injury, composed of cells and ECM on the intimal surfaceand ECM on the intimal surface
Negative remodelingNegative remodeling: : constriction of the vessel by constriction of the vessel by the formation of a fibrotic scar within the the formation of a fibrotic scar within the
adventitiaadventitia..






49%70% 76% 80% 84% 88%
45%25% 19% 17% 13% 10%
0%
20%
40%
60%
80%
100%
120%
1997 1998 1999 2000 2001 2002
Stents Balloon Angioplasty Atherectomy
49%70% 76% 80% 84% 88%
45%25% 19% 17% 13% 10%
0%
20%
40%
60%
80%
100%
120%
1997 1998 1999 2000 2001 2002
Stents Balloon Angioplasty Atherectomy
Intervention 2003Intervention 2003Stents: the dominant strategy in Stents: the dominant strategy in interventional cardiologyinterventional cardiology•Improved procedural safety•Predictable angiographic results•Better late outcomes (lower restenosis)
Stents: the dominant strategy in Stents: the dominant strategy in interventional cardiologyinterventional cardiology•Improved procedural safety•Predictable angiographic results•Better late outcomes (lower restenosis)



Current Indications for Drug-eluting Current Indications for Drug-eluting StentsStents::
1.1. Why do we need DES ?Why do we need DES ?
2.2. Which DES should we use ? Which DES should we use ?
3.3. Indications for DES ? Indications for DES ?

Streptomyces hygroscopicus
Sirolimus (Rapamycin) Streptomyces hygroscopicus

Paclitaxel Taxus brevifolia


DES ever received CE-Certificate !

100100 randomised DES Studies in 49.993 randomised DES Studies in 49.993
PatientsPatients ABSOLUTE, ACTION, APPLAUSE, ASPECT, AVELLINO, BASKET, ABSOLUTE, ACTION, APPLAUSE, ASPECT, AVELLINO, BASKET, BBK, BRADES, CACTUS, CARDIA, CHINA-1, CHINA-2, CHREDIT, BBK, BRADES, CACTUS, CARDIA, CHINA-1, CHINA-2, CHREDIT,
CORPAL, CORPAL-Bif-1, CORPAL-Bif-2, COSTAR-II, C-SIRIUS, CORPAL, CORPAL-Bif-1, CORPAL-Bif-2, COSTAR-II, C-SIRIUS, Cypher/ BeStent, Cypher/ BeStent, Cypher/Vision, DEDICATION-DES, DECODE, Cypher/Vision, DEDICATION-DES, DECODE, DELIVER-I, DESSERT, DEXA, DELIVER-I, DESSERT, DEXA, DEXAMET, DIABETES, EAGLE, DEXAMET, DIABETES, EAGLE,
ELUTES, ENDEAVOR-II, ENDEAVOR-III, ENDEAVOR-IV, E-SIRIUS, ELUTES, ENDEAVOR-II, ENDEAVOR-III, ENDEAVOR-IV, E-SIRIUS, ESTRADIOL, ETHOS-I, EUROSTAR-II, FUTURE- I, FUTURE-II, ESTRADIOL, ETHOS-I, EUROSTAR-II, FUTURE- I, FUTURE-II,
GENESIS, GENOUS-STEMI, HAAMU, HORIZONS-AMI, ISAR- DESIRE, GENESIS, GENOUS-STEMI, HAAMU, HORIZONS-AMI, ISAR- DESIRE, ISAR-DIABETICS, ISAR-LM, ISAR-PEACE, ISAR-SMART-3, ISAR- ISAR-DIABETICS, ISAR-LM, ISAR-PEACE, ISAR-SMART-3, ISAR- TEST, TEST,
ISAR-TEST-3, JUPITER-II, LABEM, LEADERS, LONG-DES-II, ISAR-TEST-3, JUPITER-II, LABEM, LEADERS, LONG-DES-II, MISSION, NOBORI-I Phase 1, NOBORI-I Phase 2, NORDIC-Bif-I, MISSION, NOBORI-I Phase 1, NOBORI-I Phase 2, NORDIC-Bif-I,
NORDIC- Bif-II, PAINT, PASSION, PATENCY, PISA-LAD, NORDIC- Bif-II, PAINT, PASSION, PATENCY, PISA-LAD, PRISON-II, PROSIT, RAPPAC, RAVEL, RIGA-LM, RRISC, REALITY, PRISON-II, PROSIT, RAPPAC, RAVEL, RIGA-LM, RRISC, REALITY,
RIBS-II, SCANDSTENT, SCORE, SCORPIUS, SESAMI, SES-SMART, RIBS-II, SCANDSTENT, SCORE, SCORPIUS, SESAMI, SES-SMART, SEVILLA, SIRIUS, SIRIUS-Bif, SIRTAX, SISR, SORT-OUT-II, SORT-SEVILLA, SIRIUS, SIRIUS-Bif, SIRTAX, SISR, SORT-OUT-II, SORT-
OUT-III, SOS, SPIRIT-I, SPIRIT-II, SPIRIT-III, STEALTH-I, OUT-III, SOS, SPIRIT-I, SPIRIT-II, SPIRIT-III, STEALTH-I, STRATEGY, SYNTAX, TAXI, TAXUS-I, TAXUS-II, TAXUS-IV, STRATEGY, SYNTAX, TAXI, TAXUS-I, TAXUS-II, TAXUS-IV, TAXUS-V, TAXUS-V-ISR, TAXUS-VI, TYPHOON, ZEST, TAXUS-V, TAXUS-V-ISR, TAXUS-VI, TYPHOON, ZEST,
ZOOMAX-I, ZOOMAX-IIZOOMAX-I, ZOOMAX-II

1. High Evidence (primary clinical endpoint reached) 1. High Evidence (primary clinical endpoint reached) Cypher Cypher
SirolimusSirolimus Taxus (Cordis / J&J) (Boston Scientific) Taxus (Cordis / J&J) (Boston Scientific)
PaclitaxelPaclitaxel Endeavor (Medtronic) Endeavor (Medtronic)
ZotarolimusZotarolimus Xience V / Promus (Abbott / Boston Sc.) Xience V / Promus (Abbott / Boston Sc.)
EverolimusEverolimus Biomatrix (Biosensors/Krauth) Biomatrix (Biosensors/Krauth)
Biolimus A9Biolimus A9
2.2. Medium Evidence (primary surrogate reached) Medium Evidence (primary surrogate reached) Yukon (Translumina) Yukon (Translumina)
SirolimusSirolimus Nobori (Terumo) Nobori (Terumo)
Biolimus A9Biolimus A9

Current Indications for Drug-eluting Current Indications for Drug-eluting StentsStents::
1.1. Why do we need DES ?Why do we need DES ?
2.2. Which DES should we use ?Which DES should we use ?
3.3. Indications for DES ? Indications for DES ?

NONO
Just Play it Smart
Should We Use Drug-Eluting Stents in All Patients and in All Lesions?

Indications Indications Anticipated ApprovalAnticipated Approval
De-Novo Lesions Length 15-30 mm Vessel sizes 2.5-3.5
Not Approved (off label use) Acute MI (Yes Recent data:Sirolimus), Acute Coronary
Syndrome? In-Stent Restenosis (ISAR 11 favours Sirolimus) Bifurcations, long lesions>30 mm, small vessels< 2.5mm SVG ?? Multivessel (Syntax approves LMS+1,2vessels).


DRUG COATED STENTS BETTER… DRUG COATED STENTS BETTER… Show me the Data ???Show me the Data ???
1) 1) Long lesion >18-50mm Long lesion >18-50mm lessless RestenosisRestenosis
2) 2) Small vessel (<2.5mm) Small vessel (<2.5mm) lessless RestenosisRestenosis3) 3) Acute myocardial infarction Acute myocardial infarction Thrombosis?Thrombosis? Sirolomus is safe(Recent publication!!)..Sirolomus is safe(Recent publication!!)..
10) Chronic occlusion 10) Chronic occlusion No DataNo Data
4) Multi-vessel disease 4) Multi-vessel disease Syntax Syntax D/LMS+1.2,VesselsD/LMS+1.2,Vessels
5) Bifurcation 5) Bifurcation lessless RestenosisRestenosis6) Main stem, 6) Main stem, settled following All Comapre!!settled following All Comapre!!
7) 7) In-stent restenosis In-stent restenosis Mixed Results Mixed Results
8) Diabetes8) Diabetes Restenosis lessRestenosis less9) Saphenous Vein Grafts 9) Saphenous Vein Grafts No Data No Data






Cypher sirolimus-eluting Cypher sirolimus-eluting stentstent
Cypher sirolimus-eluting Cypher sirolimus-eluting stentstent
Primary Endpoint:Primary Endpoint: In-stent and late lumen loss at 9 months (determined by In-stent and late lumen loss at 9 months (determined by
QCA) QCA)
Secondary Endpoints:Secondary Endpoints: MACE (cardiac death, MI, TLR) at 30 days, 9, 12, and 24 MACE (cardiac death, MI, TLR) at 30 days, 9, 12, and 24
monthsmonths Mean in-stent and edge neointimal hyperplasiaMean in-stent and edge neointimal hyperplasia Percent volume obstruction (determined by IVUS)Percent volume obstruction (determined by IVUS) Complications Complications
Primary Endpoint:Primary Endpoint: In-stent and late lumen loss at 9 months (determined by In-stent and late lumen loss at 9 months (determined by
QCA) QCA)
Secondary Endpoints:Secondary Endpoints: MACE (cardiac death, MI, TLR) at 30 days, 9, 12, and 24 MACE (cardiac death, MI, TLR) at 30 days, 9, 12, and 24
monthsmonths Mean in-stent and edge neointimal hyperplasiaMean in-stent and edge neointimal hyperplasia Percent volume obstruction (determined by IVUS)Percent volume obstruction (determined by IVUS) Complications Complications
DIABETES trialDIABETES trial
Presented at TCT 2004Presented at TCT 2004
149 patients with type 2 diabetes (1/3 on insulin) and native coronary lesions appropriate for stent implantation
149 patients with type 2 diabetes (1/3 on insulin) and native coronary lesions appropriate for stent implantation
Bare-metal stentBare-metal stentBare-metal stentBare-metal stent

In Segment Restenosis In Segment Restenosis Small Vessel Size and DiabetesSmall Vessel Size and Diabetes
18.6 17.6
42.9
50.5
0
10
20
30
40
50
60
Sirolimus Control
Small Vessel Diabetes

Secondary end points – Restenosis, TLR, Secondary end points – Restenosis, TLR, MACEMACE
7.7 7.511.3
33.0 31.336.3
0
5
10
15
20
25
30
35
40
Angiographic restenosisrate
TLR in segment MACE
CYPHER Bare Stent
7.7 7.511.3
33.0 31.336.3
0
5
10
15
20
25
30
35
40
Angiographic restenosisrate
TLR in segment MACE
CYPHER Bare Stent
%
TCT 2004TCT 2004
p=<0.0001 p =<0.0001p =<0.001
Angiographic restenosis, TLR, and overall MACE were significantly reduced. (Reduction in overall MACE was primarily due to the
reduction in TLR – rates of cardiac death and MI were not significantly different between the two groups.)

0.08 0.08
0.44
0.66
0.000
0.200
0.400
0.600
0.800
1.000
In-segmentlate loss (mm)
In-stent lateloss (mm)
CYPHER Bare Stent
0.08 0.08
0.44
0.66
0.000
0.200
0.400
0.600
0.800
1.000
In-segmentlate loss (mm)
In-stent lateloss (mm)
CYPHER Bare StentIn-stent and overall in-segment In-stent and overall in-segment late lumen loss was significantly late lumen loss was significantly reduced in the drug eluting stent reduced in the drug eluting stent group. group.
No significant difference was No significant difference was seen in the degree of late loss seen in the degree of late loss reduction between insulin-reduction between insulin-dependent patients (99% dependent patients (99% reduction) and patients on oral reduction) and patients on oral agents (72 % reduction.)agents (72 % reduction.)
Presented at ACC Scientific Sessions 2004Presented at ACC Scientific Sessions 2004
Primary End Point – Late Loss at 9 Primary End Point – Late Loss at 9 MonthsMonths
Primary End Point – Late Loss at 9 Primary End Point – Late Loss at 9 MonthsMonths
mm
p=<0.0001p=<0.0001

DIABETES trial – 9 month resultsDIABETES trial – 9 month results
Among patients with native coronary lesions and type 2 diabetes (insulin Among patients with native coronary lesions and type 2 diabetes (insulin requiring and noninsulin requiring), treatment with a sirolimus-eluting stent was requiring and noninsulin requiring), treatment with a sirolimus-eluting stent was associated with a reduction in late loss (in-stent and in-segment) at 9 months associated with a reduction in late loss (in-stent and in-segment) at 9 months compared with treatment with a bare stent compared with treatment with a bare stent
Consistent with other drug-eluting stent trials, the sirolimus –eluting stent was Consistent with other drug-eluting stent trials, the sirolimus –eluting stent was not associated with a reduction in death or MInot associated with a reduction in death or MI
A subanalysis of the SIRIUS trial showed that diabetics treated with a drug-A subanalysis of the SIRIUS trial showed that diabetics treated with a drug-eluting stent had significant reductions in TLR, MACE, late loss and restenosis eluting stent had significant reductions in TLR, MACE, late loss and restenosis compared with diabetics treated with bare stent, but the degree of improvement in compared with diabetics treated with bare stent, but the degree of improvement in diabetic patients was less than in nondiabetic patients, with no significant benefit diabetic patients was less than in nondiabetic patients, with no significant benefit in the insulin-dependent patientsin the insulin-dependent patients
The current trial showed no significant difference in late loss reduction between The current trial showed no significant difference in late loss reduction between insulin-dependent and noninsulin-dependent diabetics, but the sample size of insulin-dependent and noninsulin-dependent diabetics, but the sample size of insulin-dependent patients (and the overall trial) was smallinsulin-dependent patients (and the overall trial) was small
Among patients with native coronary lesions and type 2 diabetes (insulin Among patients with native coronary lesions and type 2 diabetes (insulin requiring and noninsulin requiring), treatment with a sirolimus-eluting stent was requiring and noninsulin requiring), treatment with a sirolimus-eluting stent was associated with a reduction in late loss (in-stent and in-segment) at 9 months associated with a reduction in late loss (in-stent and in-segment) at 9 months compared with treatment with a bare stent compared with treatment with a bare stent
Consistent with other drug-eluting stent trials, the sirolimus –eluting stent was Consistent with other drug-eluting stent trials, the sirolimus –eluting stent was not associated with a reduction in death or MInot associated with a reduction in death or MI
A subanalysis of the SIRIUS trial showed that diabetics treated with a drug-A subanalysis of the SIRIUS trial showed that diabetics treated with a drug-eluting stent had significant reductions in TLR, MACE, late loss and restenosis eluting stent had significant reductions in TLR, MACE, late loss and restenosis compared with diabetics treated with bare stent, but the degree of improvement in compared with diabetics treated with bare stent, but the degree of improvement in diabetic patients was less than in nondiabetic patients, with no significant benefit diabetic patients was less than in nondiabetic patients, with no significant benefit in the insulin-dependent patientsin the insulin-dependent patients
The current trial showed no significant difference in late loss reduction between The current trial showed no significant difference in late loss reduction between insulin-dependent and noninsulin-dependent diabetics, but the sample size of insulin-dependent and noninsulin-dependent diabetics, but the sample size of insulin-dependent patients (and the overall trial) was smallinsulin-dependent patients (and the overall trial) was small






68
RECENTRECENT
Recommendations Recommendations for the use of stents in for the use of stents in
STEMISTEMI

69
Use of stents in STEMI
NEW Recommendation
It is reasonable to use a drug-
eluting stent as an alternative to a
bare-metal stent for primary PCI in
STEMI
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
* Consideration for the use of stents (DES or BMS) in STEMI should include the ability of the patient to comply with prolonged dual antiplatelet therapy, the bleeding risk in patients on chronic oral anticoagulation, and the possibility that the patient may need surgery during the ensuing year

70
Use of stents in STEMI
MODIFIED Recommendation
A DES may be considered forclinical and anatomic
settings† inwhich the efficacy/safety
profileappears favorable
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

ConclusionsConclusions● Progressive adoption of DESProgressive adoption of DES programmes is intuitively programmes is intuitively
correct for physicians, patients and healthcare systemscorrect for physicians, patients and healthcare systems● Changing referral patterns in favour of PCI/DES present Changing referral patterns in favour of PCI/DES present
a significant challenge to current and future resourcesa significant challenge to current and future resources● Future developments seem unlikely to halt this advanceFuture developments seem unlikely to halt this advance
● Stent platformsStent platforms – increased deliverability and decreased vascular – increased deliverability and decreased vascular injuryinjury
● Biodegradable polymersBiodegradable polymers – no consequences of retained drug or – no consequences of retained drug or polymerpolymer
● PharmacokineticsPharmacokinetics – sustained drug release – sustained drug release● Combination therapy – directed luminal and abluminal release of Combination therapy – directed luminal and abluminal release of
vasculoprotective agents and cell cycle inhibitorsvasculoprotective agents and cell cycle inhibitors

DES appears to have the DES appears to have the edge over BMS in:edge over BMS in:1-Diabetics:1-Diabetics:
a)Less TLR, Less Restenosis rate , less Macea)Less TLR, Less Restenosis rate , less Mace
2-In vessels 2.5 to 3.5mm2-In vessels 2.5 to 3.5mm up to 30 mm up to 30 mm
lenght:lenght: Less TLR,TVR,Mace.Less TLR,TVR,Mace. 3-In ISR3-In ISR: : favouring Sirolimus in particular. favouring Sirolimus in particular. 4-In LMS: 4-In LMS: In main Compare+Syntax Trials(growing In main Compare+Syntax Trials(growing Future Role)Future Role)

Thank YouThank You
73





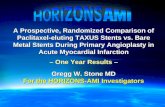
IntimaMedia
Adventitia
ANGIOPLASTY / STENT INSERTION
Intimal and medial tears
Acute stent-induced damage to the plaque
Longitudinal translocation of plaque
Embolisation of necrotic core
Endothelial loss
Necrotic core
Fibrous cap
Thrombosis


PCI Procedural refinements: PCI Procedural refinements: StentsStents
Expandable metal mesh tubes that buttresses the dilated segment, limit restenosis.
Drug eluting stents: further reduce cellular proliferation in response to the injury of dilatation.







Stent releasing an antiproliferative drug