unilateral & bilateral limb weakness , stroke approach
18
Limb Weakness STROKE: APROACH AND MANAGEMENT BY DR. MUSTAFA F. AL BAGHDADI
-
Upload
mustafa92albaghdadi -
Category
Education
-
view
37 -
download
0
Transcript of unilateral & bilateral limb weakness , stroke approach

Limb WeaknessSTROKE: APROACH AND MANAGEMENT
BY DR. MUSTAFA F. AL BAGHDADI

Approach

Approach

Assess power, ask about pre-existing weakness & measure glucose.
Immobilize the cervical spine
Disk prolapse, pathological fracture & Spinal stroke
(severe back pain)Increase tone, Brisk reflexes, extensor planter responseSuggest
myelopathy Do MRI
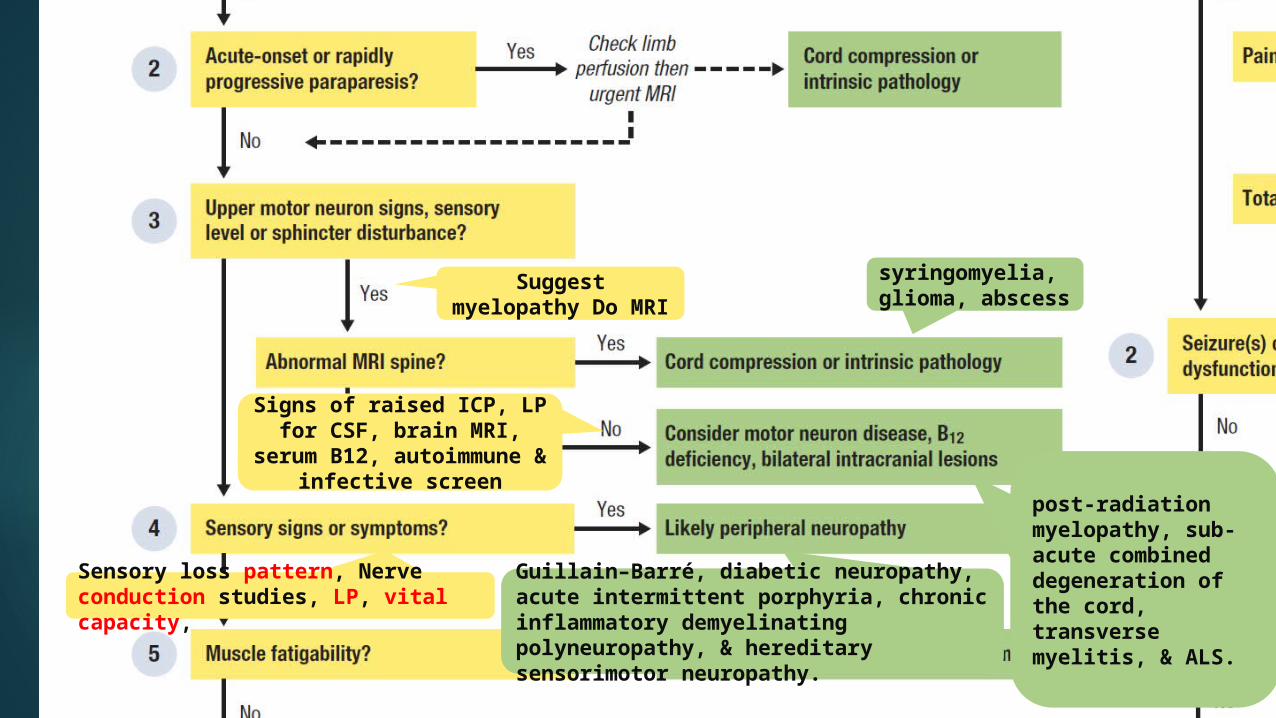
syringomyelia,glioma, abscess
post-radiation myelopathy, sub-acute combineddegeneration of the cord, transverse myelitis, & ALS.
Signs of raised ICP, LP for CSF, brain MRI,
serum B12, autoimmune & infective screen
Guillain–Barré, diabetic neuropathy, acute intermittent porphyria, chronic inflammatory demyelinating polyneuropathy, & hereditary sensorimotor neuropathy.
Sensory loss pattern, Nerve conduction studies, LP, vital capacity,
Suggest myelopathy Do
MRI

Ocular and bulbar involvement (ptosis, diplopia, voice weakening), +ve tendon reflex, AChRAb,& chest CT.
myopathies
Stop statins, exclude other drugs,& antibody screen(anti-jo1).UMN or LMN ‘patchy’ pattern of
weaknessa
lumbosacral plexopathy, malignant, vasculitic or infiltrative disorder

Compare pulses, color, temperature,& capillary refill. Limb x-ray, CK, ask about seizure,& previous stroke.
Assess the risk of
impending stroke

Assessing the risk of impending stroke
Admit if ABCDD score ≥4 Or >1 TIA
Otherwise consider discharge with
appropriate secondary prevention and specialist follow-up within a week.
Arrange neuroimaging prior to discharge in any patient taking warfarin.
carotid Doppler USS

Compare pulses, color, temperature,& capillary refill. Limb x-ray, CK, ask about seizure,& previous stroke.
Assess the risk of
impending stroke

Further assessment of
strokeStep 1 Assess eligibility for thrombolysis Potentially disabling
stroke.
Less than 3 hours
immediate CT brain to exclude hemorrhagic stroke.

Step 2 Classify stroke according to clinicaland radiological findings
Perform a CT brain urgently if:
• the patient is eligible for thrombolysis
• coagulation is impaired
• ↓GCS
• symptoms include a severe headache
• there is a rapidly progressive neurological deficit
• cerebellar hemorrhage is suspected (to
exclude obstructive hydrocephalus).
Otherwise, perform CT within 24 hours
Click icon to add pictureClick icon to add picture

Acute treatment & Prevention Acute Supportive treatment (airway protection,
oxygen, IV fluids) is initiated.
Aspirin is best if given within 24 hours of symptom onset.
Assess the patient’s ability to protect his or her airway, keep NPO, and elevate the head of the bed 30°.
Do not give antihypertensive agents unless one of the following three:
Prevention according to the cause:• atherosclerosis of the carotid arteries (Aspirin, Control HTN, DM, smoking, hypercholesterolemia, obesity, Surgery carotid endarterectomy in Symptomatic patients)• embolic disease anticoagulation (aspirin), reduction of atherosclerotic risk factors • lacunar strokes—control of hypertension
So if patient presents within 3 hours of stroke onset, thrombolytics areindicated. If after 3 hours, give aspirin. If patient cannot take aspirin, giveclopidogrel.
1- BP is very high >220/>120.2- medical indication for antihypertensive(MI, HF)3- receiving thrombolytic therapy

Step 3 Evaluate for risk factors/underlying cause
Suspect a cardiac source if :
• evidence of AF or MI• features suggesting endocarditis ,e.g. fever & new murmur• ≥2 cerebral infarcts• systemic emboli e.g. lower limb
Investigate for an unusual cause of stroke in younger patients without vascular risk factors:
• thrombophilia screen.
• echocardiography
• Consider MRA
Complications of Stroke
1. Progression of neurologic insult 2. Cerebral edema occurs within 1 to 2 days and
can cause mass effects for up to10 days. Hyperventilation and mannitol may be needed to lower intracranial pressure.
3. Hemorrhage into the infarction—rare 4. Seizures—fewer than 5% of patients

Compare pulses, color, temperature,& capillary refill. Limb x-ray, CK, ask about seizure,& previous stroke.
Assess the risk of
impending stroke

If no result do LP ± MRI
fever, meningism, purpuric rash, or features of shock blood cultures, give empirical IV treatment
Slowly progressive
suddenExclude
spinal cord
Or sensory level
If you can’t do brain CT or MRI if cranial nerve or cerebellar
signs +ve
Single peripheral n.
MRI spine
Still possible so we should do CT

ReferencesDAVISON’S PRINCIPLES
MACLEOD’S CLINICAL DIAGNOSIS
STEP UP TO MEDICINE

Thank youFOR YOUR ATTENTION






![Unilateral lower-limb loss: Prosthetic device use and functional · 2010-06-23 · 318 JRRD, Volume 47, Number 4, 2010 [1]. Prolonged lower-limb prosthetic device use and satis-faction](https://static.fdocuments.net/doc/165x107/5f6c546e58ba42037c0f0d32/unilateral-lower-limb-loss-prosthetic-device-use-and-functional-2010-06-23-318.jpg)