Ultrastructure of fallopian tube carcinoma
7
ULTRASTRUCTURE OF FALLOPIAN TUBE CARCINOMA LEWIS JOHNSON, MD, ISRAEL DIAMOND, MD, AND GRANT JOLLY Fallopian tube carcinoma is one of the rarest of primary gynecologic malig- nancies. Normal tubal epithelium is composed of secretory, ciliated, and inter- calary cells. To determine the cellular composition and ultrastructural details of this rare neoplasm, a moderately well-differentiated tubal carcinoma was studied with the electron microscope. A prominent feature was the formation of numerous ultramicro alveolar spaces lined by cell surface microvilli. The nuclei of the neoplastic cells demonstrated a variety of fine structural abnor- malities. Based on cell size and shape criteria, a possible dual tumor cell population was suggested. However, no cilia were seen in any of the tumor cells and almost all were devoid of secretory granules. These latter observa- tions suggest that this tumor was primarily a proliferation of intercalary cells. Cancer 42: 1291 - 1297, 1978. ALLOPIAN TUBE CARCINOMA is one of the F rarest of female reproductive organ malignancies; its incidence being about 0.16% of all primary gynecologic cancer^.^ Although they have been observed in women aged 17- 80, they most commonly occur in the fifth and sixth decades.6 Because of the more frequent involvement of the Fallopian tubes by meta- static carcinoma, several morphologic criteria are accepted for the pathologic diagnosis of primary tubal carcinoma, e.g., 1) the entire endosalpinx is replaced by the tumor, 2) the tumor bears close histologic resemblance to normal tubal epithelium, 3) the endometrium and ovaries are either normal or contain only minute amounts of histologically similar tu- mor, 4) prime tubal involvement is endosal- pingeal, and 5) salpingeal tuberculosis has been excluded.2 Based on histologic features, they have been divided into three groups, e.g., papillary grade 1, papillary-alveolar grade 2, and alveolar-medullary grade 3.3 Normal tubal epithelium is composed of cili- ated, secretory, and intercalary cells, but the latter cell may represent a degranulated secre- tory cell4 To determine the cell composition and ultrastructural details of this rare human tumor, a papillary-alveolar grade 2 tubal car- From the Section of Pathology and Laboratory Medi- cine, Brown University Program in Medicine, Roger Williams General Hospital, Providence, Rhode Island. Address for reprints: Lewis Johnson, MD, Department of Pathology and Laboratory Medicine, Roger Williams General Hospital, 825 Chalkstone Avenue, Providence, RI 02908. The authors thank Ms. Sally Virta for preparation of the illustrations. Accepted for publication December 12, 1977. cinoma was studied with the electron micro- scope. CASE REPORT Because of a recent dark brownish copious hemorrhage per vagina, a 66-year-old para 8-0-1-7 was admitted to the Roger Williams General Hospi- tal on April 25, 1977. There was no history of pelvic inflammatory disease, and her menopause had occurred at age 49. She had undergone a chole- cystectomy for chronic calculous cholecystitis in 1965 and a sigmoid resection for acute diverticuli- tis in 1966. Since then, she had been in fair general health except for mild benign hypertension and mild diabetes mellitus. She was a very heavy ciga- rette smoker. Physical examination on admission revealed an elderly woman with a recurrent non- productive cough. The vital signs were as follows: temperature 37 C, pulse 95 and regular, respira- tions 18/minute, and BP 140/80. Examination of the heart and lungs was unremarkable. The abdo- men was negative except for well-healed right subcostal and left paramedian laparotomy scars. The pelvic examination revealed an anteverted small uterine corpus, a clean cervix, a small amount of brownish blood in the vaginal vault, normal right uterine adnexal structures, and a small non- cystic left uterine adnexal mass. Admission labora- tory examinations revealed the following data: hemoglobin 15.2 gidl, hematocrit 4676, leukocyte count 1 1,900/mm3 with 55% segmented granulo- cytes, 38% lymphocytes, 3% monocytes, and 4% eosinophils; serum sodium 139 meqiliter, potassium 4.1 meqiliter, chloride 99 meqiliter, COz 30 mmoli liter, glucose 146 mgidl, and urea 16 mgidl. An SMA-12 serum chemistry profile, consisting of total protein, albumin, calcium, phosphorus, cholesterol, uric acid, creatinine, total bilirubin, alkaline phos- phatase, creatine phosphokinase, lactic dehydro- 0008-543X/78/0900/1291 $0.85 0 American Cancer Society 1291
-
Upload
lewis-johnson -
Category
Documents
-
view
213 -
download
0
Transcript of Ultrastructure of fallopian tube carcinoma

ULTRASTRUCTURE OF FALLOPIAN TUBE CARCINOMA
LEWIS JOHNSON, MD, ISRAEL DIAMOND, MD, AND GRANT JOLLY
Fallopian tube carcinoma is one of the rarest of primary gynecologic malig- nancies. Normal tubal epithelium is composed of secretory, ciliated, and inter- calary cells. To determine the cellular composition and ultrastructural details of this rare neoplasm, a moderately well-differentiated tubal carcinoma was studied with the electron microscope. A prominent feature was the formation of numerous ultramicro alveolar spaces lined by cell surface microvilli. The nuclei of the neoplastic cells demonstrated a variety of fine structural abnor- malities. Based on cell size and shape criteria, a possible dual tumor cell population was suggested. However, no cilia were seen in any of the tumor cells and almost all were devoid of secretory granules. These latter observa- tions suggest that this tumor was primarily a proliferation of intercalary cells.
Cancer 42: 1291 - 1297, 1978.
ALLOPIAN TUBE CARCINOMA is one of the F rarest of female reproductive organ malignancies; its incidence being about 0.16% of all primary gynecologic cancer^.^ Although they have been observed in women aged 17- 80, they most commonly occur in the fifth and sixth decades.6 Because of the more frequent involvement of the Fallopian tubes by meta- static carcinoma, several morphologic criteria are accepted for the pathologic diagnosis of primary tubal carcinoma, e.g. , 1) the entire endosalpinx is replaced by the tumor, 2) the tumor bears close histologic resemblance to normal tubal epithelium, 3) the endometrium and ovaries are either normal or contain only minute amounts of histologically similar tu- mor, 4) prime tubal involvement is endosal- pingeal, and 5 ) salpingeal tuberculosis has been excluded.2 Based on histologic features, they have been divided into three groups, e .g . , papillary grade 1, papillary-alveolar grade 2, and alveolar-medullary grade 3.3 Normal tubal epithelium is composed of cili- ated, secretory, and intercalary cells, but the latter cell may represent a degranulated secre- tory cell4 To determine the cell composition and ultrastructural details of this rare human tumor, a papillary-alveolar grade 2 tubal car-
From the Section of Pathology and Laboratory Medi- cine, Brown University Program in Medicine, Roger Williams General Hospital, Providence, Rhode Island.
Address for reprints: Lewis Johnson, MD, Department of Pathology and Laboratory Medicine, Roger Williams General Hospital, 825 Chalkstone Avenue, Providence, RI 02908.
The authors thank Ms. Sally Virta for preparation of the illustrations.
Accepted for publication December 12, 1977.
cinoma was studied with the electron micro- scope.
CASE REPORT
Because of a recent dark brownish copious hemorrhage per vagina, a 66-year-old para 8-0-1-7 was admitted to the Roger Williams General Hospi- tal on April 25, 1977. There was no history of pelvic inflammatory disease, and her menopause had occurred at age 49. She had undergone a chole- cystectomy for chronic calculous cholecystitis in 1965 and a sigmoid resection for acute diverticuli- tis in 1966. Since then, she had been in fair general health except for mild benign hypertension and mild diabetes mellitus. She was a very heavy ciga- rette smoker. Physical examination on admission revealed an elderly woman with a recurrent non- productive cough. The vital signs were as follows: temperature 37 C, pulse 95 and regular, respira- tions 18/minute, and BP 140/80. Examination of the heart and lungs was unremarkable. The abdo- men was negative except for well-healed right subcostal and left paramedian laparotomy scars. The pelvic examination revealed an anteverted small uterine corpus, a clean cervix, a small amount of brownish blood in the vaginal vault, normal right uterine adnexal structures, and a small non- cystic left uterine adnexal mass. Admission labora- tory examinations revealed the following data: hemoglobin 15.2 gidl, hematocrit 4676, leukocyte count 1 1,900/mm3 with 55% segmented granulo- cytes, 38% lymphocytes, 3% monocytes, and 4% eosinophils; serum sodium 139 meqiliter, potassium 4.1 meqiliter, chloride 99 meqiliter, COz 30 mmoli liter, glucose 146 mgidl, and urea 16 mgidl. An SMA-12 serum chemistry profile, consisting of total protein, albumin, calcium, phosphorus, cholesterol, uric acid, creatinine, total bilirubin, alkaline phos- phatase, creatine phosphokinase, lactic dehydro-
0008-543X/78/0900/1291 $0.85 0 American Cancer Society
1291

1292 CANCER September 1978 Vol. 42
genase, and glutamic oxalacetic transaminase, were all within normal limits except for a borderline high alkaline phosphatase, 11 1 units (normal 30- 105). The urinalysis was within normal limits. The VDRL was nonreactive. A serum protein electro- phoresis scan was normal. A negative anterior- posterior chest roentgenogram was reported. The electrocardiogram demonstrated mild right axis deviation and minimally depressed ST segments in leads 11, 111, AVF, and V3+ On the first hospital day, the endometrium was curetted, but only a small amount of brownish blood was found in uterine cavity. The pathologic study of this speci- men revealed clotted blood elements only. Cytologic examinations of the cervix and vaginal pool were not ordered, and culdoscopy was not performed. On the third hospital day, an exploratory pelvic
FIG. 1. An exclusively endosal- pingeal epithelial tumor on the right superficially infiltrating into the mus- cularis on the left, completely filled the distended tubal lumen from fim- briated to corneal portions (H & E, X30).
laparotomy was done and a sausage-like, swollen, firm left tubal mass adherent to the left ovary was found. A total hysterectomy with bilateral salpingo- oophorectomy was performed. The patient was discharged on the eighth postoperative day.
MATERIALS AND METHODS
The uterine corpus, cervix, right and left Fallopian tubes and ovaries were examined immediately after removal. All these structures were grossly normal except for the left Fal- lopian tube, which was diffusely swollen and hyperemic. Loose fibrous adhesions were ob- served between the fimbriated portion of the left tube and the left ovary. This swollen tube
FIG. 2. Moderately well-differen- tiated grade 2 tubal carcinoma. Note both the papillary structure and the numerous microscopic alveolar spaces formed by the tumor cells. Neverthe- less, the neoplastic epithelium bears fairly close resemblance to normal tubal epithelium (H & E, X 125).

No. 3 TUBAL CARCINOMA ULTRASTRUCTURE * Johnson et al. 1293
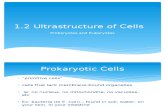
FIG. 3. Possibly dimorphic tumor cell population. Suggesting a possible dual tumor cell population, columnar cells, 3.0 microns in width and u p to 20.0 microns in length, are admixed with ovoid cells, 3.0-5.5 microns in diameter. The latter cells, however, may only represent the larger columnar cells in cross section. Note the ultra- microscopic alveolar space filled with cell surface microvilli in the lower left (Uranyl acetate-lead citrate stain, X4500).
had the appearance of a small sausage, meas- uring 7.0 cm in length and 4.0 cm in diameter throughout its entire length. Multiple imme- diate sections through the left tube revealed the enlargement to be due to a moderately firm, whitish-tan, completely intralumenal tumor. Multiple representative portions of this tumor and all the other above structures were placed in Zenker’s fixative for 24 hours, embedded in paraffin, sectioned, stained with hematoxylin-eosin, and examined with the light microscope. Further multiple minute samples of the tumor were also immediately minced, fixed in 2.5% glutaraldehyde for 3 hours, post-fixed in 1.0% osmic acid for 1.5 hours, dehydrated, embedded in Epon, thick sectioned at 1.0 micron with the pyramitone, toluidine blue stained, and examined with the light microscope for tumor cells. Multiple representative thick sections of tumor cells from all portions of the tube were thin sec- tioned with the LKB-3, stained with uranyl acetate-lead citrate, and examined with the RCA-4C electron microscope.
RESULTS All the histologic sections from the fimbri-
ated, isthmic, and cornual portions of the left Fallopian tube revealed complete endosal- pingeal replacement by an epithelial tumor, which superficially infiltrated into the muscu- lark but otherwise was exclusively endosal- pingeal (Fig. 1). The histologic sections of the endometrium, right Fallopian tube, and right ovary demonstrated no evidence of primary or metastatic tumor involvement, but microscopic epithelial tumor histologi- cally similar to that in the left tube was ob- served within left ovarian hilar lymphatic channels. There was no evidence of tubercu- losis in any of the left tubal histologic sections, and the neoplasm, which bore close resem- blance to normal tubal epithelium, had the microscopic features of a moderately well- differentiated grade 2 tubal carcinoma (Fig. 2).
By electron microscopy, the tumor cells were somewhat pleomorphic in size and shape, being composed of larger oblong columnar cells and smaller ovoid cells all having abun-

1294 CANCER September 1978 Vol. 42

No. 3 TUBAL CARCINOMA ULTRASTRUCTURE * Johnson et al. 1295
FIG. 4. Tumor cell nuclear ultrastructural abnormalities. Irregular corrugated nuclear envelopes, multiple nucleoli, coarse nuclear chromatin clumps, and multiple nuclear bodies can be observed in these tumor cells. An ultra- microscopic alveolar space lined by cell surface microvilli can be seen in the lower right (Uranyl acetate-lead citrate stain, X4500).
FIG. 5. Tumor cell cytoplasmic ultrastructural details. Note the presence of normal cytoplasmic organelles in these cells, which are representative of most of the tumor cells by being devoid of cilia and secretory granules. A micro- villi lined ultramicroscopic alveolar space is depicted in the lower left (Uranyl acetate-lead citrate stain, X 10,900).
dant amounts of cytoplasm (Fig. 3). Nuclear abnormalities, such as multiple nucleoli, nu- merous coarse chromatin clumps, multiple nuclear bodies, and irregular corrugated nuclear envelopes, were frequently observed in the neoplastic cells (Fig. 4). The cytoplasm of the tumor cells demonstrated an assort- ment of normal organelles, e .g . , mitochondria, ribosomes, polyribosomes, smooth and rough endoplasmic reticulum, and surface micro- villi (Fig. 5), but none of the tumor cells re- vealed cilia (Figs. 3-5). Although a very rare neoplastic cell showed cytoplasmic secretory granules (Fig. 6), almost all the tumor cells were devoid of secretory activity (Figs. 3-5).
N o viral particles were o.bserved in any of the cancer cells. A prominent feature noted in all thin sections of the tumor was the presence of numerous ultrastructural alveolar spaces lined by tumor cell surface microvilli (Figs. 3- 5) . An occasional tumor cell demonstrated one or two cytoplasmic membrane bound and nonmembrane bound dense bodies, and a very rare neoplastic cell demonstrated nu- merous such structures (Fig. 7).
DISCUSSION A moderately well-differentiated, grade 2,
primary Fallopian tube carcinoma was studied with the electron microscope. No virus parti-
FIG. 6. Rare tumor cell with cytoplasmic secretory granules. Fairly uniform sized, large, pale, secretory granules fill the cytoplasm of this tumor cell, which also demonstrates an abnormal, deeply indented, nuclear envelope. Such cells were extremely rare in the tumor samples (Uranyl acetate-lead citrate stain, x7900).

1296 CANCER September 1978 Vol. 42
FIG. 7. A rare tumor cell demonstrating numerous membrane bound and a few nonmembrane bound cytoplasmic dense bodies is shown. Note the hemi-desmosomes on the tumor cell surface at the left border (Uranyl acetate-lead citrate stain, ~ 7 9 0 0 ) .
cles were observed but various nuclear abnor- malities were seen. On the basis of cell size and shape criteria there was a suggestion that the tumor was composed of two cell populations, e.g., a larger oblong columnar cell and a smaller ovoid cell. However, the smaller cell may only represent the larger cell in cross-section. A prominent pattern produced by the tumor cells was the formation of numerous ultra- microscopic alveolar spaces lined by cell sur- face microvilli. These probably represent a fine structural counterpart of the larger micro- scopically visible alveolar spaces. Similar micro- villi lined ultramicroscopic alveolar spaces were observed in a primary Fallopian tube adenocarcinoma described by others as being histologically poorly differentiated.' An ultra- structural feature reported by these same investigators as being typical in the neoplastic cells of both tubal adenocarcinomas and serous
ovarian cancers was a large amount of cyto- plasmic membrane-bound dense bodies.' We observed only a rare tumor cell with numerous cytoplasmic dense bodies, and some of these appeared to be nonmembrane bound. Accord- ing to others, the number of ciliated neoplastic tubal epithelial cells found by transmission or scanning electron microscopy is inversely pro- portional to the histologic grade of the tumor.' If this were true, then at least a few neoplastic ciliated epithelial cells should have been ob- served in the tumor studied in this report. Since they were not, it is suggested that per- haps the number of neoplastic ciliated or secretory cells observed electron microscopi- cally in a particular tubal adenocarcinoma may be unrelated to its histologic grade. The tumor described in this report appears to have been primarily a proliferation of intercalary type tubal epithelial cells.

No. 3 TUBAL CARCINOMA ULTRASTRUCTURE Johnson et al. 1297
REFERENCES
1 . Ferenczy, A., and Richart, R. W.: Fallopian tube adenocarcinoma. In Female Reproductive System: Dynamics of Scan and Transmission Electron Microscopy. New York, John Wiley, 1974; pp. 242-244.
2. Finn, W. F., and Javert, C. T.: Primary and meta- static carcinoma of the Fallopian tube. Cancer 2:803-814, 1949.
3. Hertig, A. T., and Gore, H.: Tumors of the Female Sex Organs. In Atlas of Tumor Pathology, Section IX, Fascicle 33, Washington, D. C., Armed Forces Institute of Pathology, 1961; pp. 166-169.
4. Lentz, T. L.: Female reproductive system. In Cell Fine Structure. Philadelphia, W. B. Saunders, 1971; pp. 276-279.
5. Lofgren, K. A,, and Dockerty, M. B.: Primary car- cinoma of the Fallopian tubes. Surg. Gynecol. Obstet. 82: 199-206, 1946.
6. Weekes, L. R., Anz, U. E., and Whiting, C. G.: Pri- mary carcinoma of the Fallopian tube. Am. J . Obstet. Gynecol. 64:62-71, 1952.