UIC Clinic & Research Day 2014 Critically Appraised Topics An approach to pre-doctoral research...
21
UIC Clinic & Research Day 20 itically Appraised Topi pproach to pre-doctoral research opportuniti Fifth Annual Competition
-
Upload
michelle-lounsbury -
Category
Documents
-
view
220 -
download
0
Transcript of UIC Clinic & Research Day 2014 Critically Appraised Topics An approach to pre-doctoral research...
UIC Clinic & Research Day 2014
Critically Appraised TopicsAn approach to pre-doctoral research opportunities
Fifth Annual Competition

L&L Agenda
ObjectivesParametersHow to find casesCaseCAT Poster TemplateCaseCAT WorksheetCaseCAT Literature WorksheetJudging CriteriaOnce you have identified a caseContact information

Objectives
To provide an opportunity for pre-doctoralstudents to engage in a patient based study tothe level of scientific inquiry
To facilitate the transformation of a patientbased study to a case presentation that can bepresented at Clinic and Research Day

Parameters
How were treatment plans or outcomes for yourpatient affected by: Treatment procedure Patient health concerns Therapeutic problems concerning patient Unusual medications Treatment consideration for medically
compromised or patients with disabilitiesExample: Blood pressure medication that
causes xerostomiaWhatare causes, how do you evaluate, how do you treat?

Where do I find cases?
1.Portfolio
On medically compromised patients i.e. diabetes,hypertensionPatients on 3 or more medically significant therapeuticmedications
2.Screening Clinic/Urgent CareDiagnosis of an interesting patient issue
3.Rotations with specialty clinics
Working with residentsExamples include: Ortho (craniofacial anomaly), Perio(diabetes), Endo (implants)

Important Elementsto Consider
Patient issue exemplifies problemThoughtful description of caseAdequate Documentation (must be de-identified)
Photos and radiographsAxium page with chartingPatient medical, dental history, chief complaintDifferential Diagnosis
In many cases already preexisting diagnosisDevelop case to level of CAT
Faculty, journals and internet as resources IRB Issues
Must be single case, case series not acceptable

SituationofConcern(Calibrifontsize60)StudentNameAdvisor
CASEPlacethecriticalelementsofyourcasehere…e.g.,ChiefComplaint,Hx,AXIUMdata,photos,etc.
SCENARIO(preferablyinfontCalibri-minimumsize20)P…
P:I…
I:C…
C:O…
O:Placethecriticalelementsofyourcasehere…e.g.,ChiefComplaint,Hx,AXIUMdata,photos,etc.(preferablyinfontCalibri-minimumsize20)
MESHTerms:CRITICALQUESTIONTerms…Typeyoursearchablequestionhere…(preferablyinfontCalibri-minimumsize20)
CASESIGNIFICANCEStudentSummaryTypeyourbottomlinehere…(preferablyinfontCalibri-minimumsize20)
CAT1TypeyourCAThere…(preferablyinfontCalibri-minimumsize20)
CAT2TypeyourCAThere…(preferablyinfontCalibri-minimumsize20)
CAT3TypeyourCAThere…(preferablyinfontCalibri-minimumsize20)
FUTUREDIRECTIONSWritefuturedirectionshere…(preferablyinfontCalibri-minimumsize20)

CaseCATWorksheet

CaseCAT Worksheet
Should I use CavitTM, IRMTM, or KetacFillTM? Student: Michael P. Munaretto Advisor: Bradford Johnson, DDS MHPE, UIC Department of Endodontics CASE SCENARIO CAT (1) CAT (2) CAT (3)
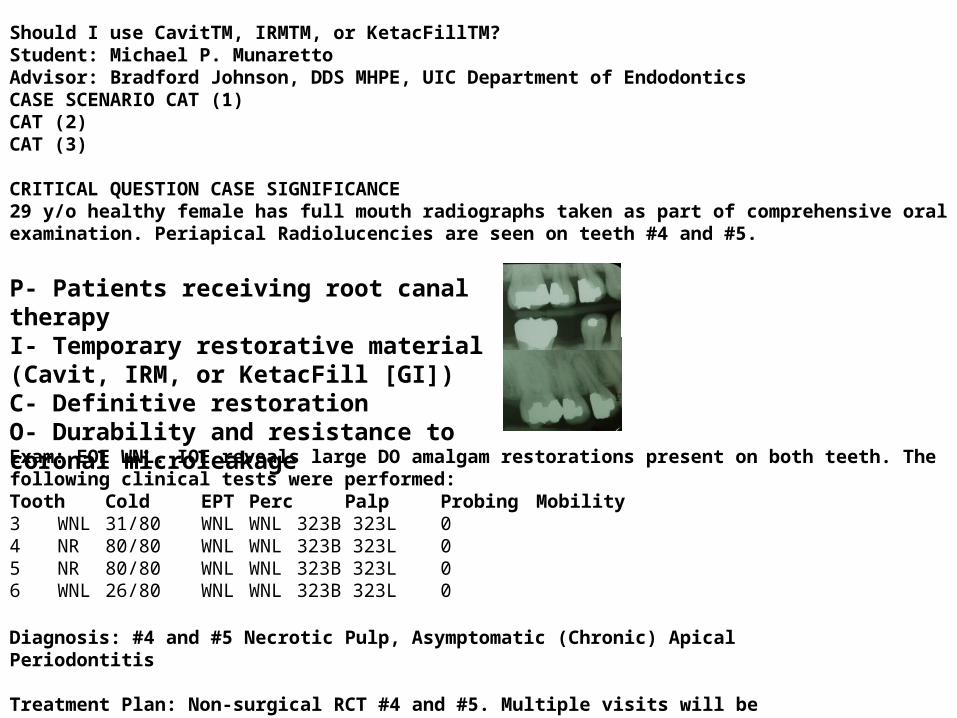
CRITICAL QUESTION CASE SIGNIFICANCE 29 y/o healthy female has full mouth radiographs taken as part of comprehensive oral examination. Periapical Radiolucencies are seen on teeth #4 and #5.
Exam: EOE WNL. IOE reveals large DO amalgam restorations present on both teeth. The following clinical tests were performed:Tooth Cold EPT Perc Palp Probing Mobility 3 WNL 31/80 WNL WNL 323B 323L 0 4 NR 80/80 WNL WNL 323B 323L 0 5 NR 80/80 WNL WNL 323B 323L 0 6 WNL 26/80 WNL WNL 323B 323L 0
P- Patients receiving root canal therapy I- Temporary restorative material (Cavit, IRM, or KetacFill [GI]) C- Definitive restoration O- Durability and resistance to coronal microleakage
Diagnosis: #4 and #5 Necrotic Pulp, Asymptomatic (Chronic) Apical Periodontitis
Treatment Plan: Non-surgical RCT #4 and #5. Multiple visits will be required.

Tooth Cold EPT Perc Palp Probing Mobility
3 WNL 31/80 WNL WNL 323B323L 0
4 NR 80/80 WNL WNL 323B323L 0
5 NR 80/80 WNL WNL 323B323L 0
6 WNL 26/80 WNL WNL 323B323L 0

CaseCAT Worksheet

TMTMTM
ShouldIuseCavit,IRM,orKetacFill?Student:MichaelP.MunarettoAdvisor:BradfordJohnson,DDSMHPE,UICDepartmentofEndodontics
CASESCENARIO29y/ohealthyfemalehasfullmouthradiographstakenaspartofcomprehensiveExam:EOEWNL.IOErevealslargeDOamalgamrestorationspresentonbothoralexamination.PeriapicalRadiolucenciesareseenonteeth#4and#5(seeteeth.Thefollowingclinicaltestswereperformed:arrowsbelow).P-PatientsreceivingrootcanaltherapyI-Temporaryrestorativematerial(Cavit,IRM,orKetacFill[GI])C-DefinitiverestorationDiagnosis:#4and#5NecroticPulp,Asymptomatic(Chronic)ApicalPeriodontitisO-DurabilityandresistancetocoronalmicroleakageTreatment Plan:Non-surgicalRCT#4and#5.Multiplevisitswillberequired.
CRITICALQUESTIONMESHTerms:Forpatientsreceivingrootcanaltherapy,whichtemporaryrestorativematerial(Cavit,IRM,orRootCanalTherapy;KetacFillGI)comparesmostfavorablytothepropertiesofthedefinitiverestorationasmeasuredDentalRestoration,bydurabilityandresistancetocoronalmicroleakage?Temporary;Leakage
CASESIGNIFICANCEFUTUREDIRECTIONSWritefuturedirectionshere…(preferablyinfontCalibri-minimumsize20)
CAT(1)Beachetal.“ClinicalEvaluationofBacterialLeakageofEndodonticTemporaryFillingMaterials.”JournalofEndodontics22:9pp459-462.1996.Methods:51humanteethreceivedRCTinvivo.Afterobturationasterilepaperdiskwasplacedbelowa4mmfillingofCavit,IRM,orTERM.Threeweekslaterthepatientswererecalled,thefillingswereremoved,andthepaperdiskswereanalyzedforbacterialgrowth.Results/Conclusion:1/18IRMsamplesshowedbacterialgrowth,whereas0/19Cavitsamplesshowedgrowth.NosignificantdifferencewasfoundbetweenIRMandCavit.Validity/Applicability:Restorationtypewasrandomlyassigned.Followupwas100%.invivostudy.3weekfollow-uprealisticatUICCOD.LevelofEvidence:2(RandomizedControlledTrial)
CAT(2)Bartheletal.“LeakageinRootsCoronallySealedwithDifferentTemporaryFillings.”JournalofEndodontics25:11pp731-734.1999.Methods:103extractedsingle-rootedteethreceivedRCTandwerethenfilledwitheitherCavit,IRM,GI,Cavit/GI,orIRM/GI.Teethwerethenimmersedintoatwo-chambersystemwhichwasinspecteddailyovera30-dayperiodforbacterialmicroleakage.Results/Conclusion:GIgavethebestsealagainstbacteria(1/20samplesleaked),whereasCavitgavethepoorestseal(13/20samplesleaked).11outof20IRMsamplesleaked.Validity/Applicability:Resultsofinvitrostudiescannotdirectlybeappliedtoclinicalpractice.However,allavailablefillingmaterialstoUICCODstudentsweretested.LevelofEvidence:6(Preclinicalstudy).
CAT(3)Naoum&Chandler.“TemporizationforEndodontics.”InternationalEndodonticJournal35:pp964-978.2002.Methods:AliteraturereviewwasperformedusingMEDLINEandcontemporarytextbookstoassessvariousendodontictemporaryfillingmaterialsandtomakeclinicalrecommendations.Results/Conclusion:CavitpossessesfavorablemarginalsealbutinferiormechanicalpropertiescomparedtoIRM.StudieshaveshownthatIRMalsoprovidesafavorablemarginalseal,especiallywhenthepowder:liquidratioisdecreased.GIismorecostly,buthasbeenfoundtobeantibacterialandtohaveasuperiorseal;thusitmaybeusedforcasesoflong-termtemporization.Validity/Applicability:Authorsdidnotprovideadetailedselectioncriteriaforarticlesreviewed.LevelofEvidence:5(ExpertOpinion)
Tooth Cold EPT Perc Palp Probing Mobility
3 WNL 31/80 WNL WNL 323B323L 0
4 NR 80/80 WNL WNL 323B323L 0
5 NR 80/80 WNL WNL 323B323L 0
6 WNL 26/80 WNL WNL 323B323L 0

CaseCAT Worksheet

TMTMTM
ShouldIuseCavit,IRM,orKetacFill?Student:MichaelP.MunarettoAdvisor:BradfordJohnson,DDSMHPE,UICDepartmentofEndodontics
CASESCENARIO29y/ohealthyfemalehasfullmouthradiographstakenaspartofcomprehensiveExam:EOEWNL.IOErevealslargeDOamalgamrestorationspresentonbothoralexamination.PeriapicalRadiolucenciesareseenonteeth#4and#5(seeteeth.Thefollowingclinicaltestswereperformed:arrowsbelow).P-PatientsreceivingrootcanaltherapyI-Temporaryrestorativematerial(Cavit,IRM,orKetacFill[GI])C-DefinitiverestorationDiagnosis:#4and#5NecroticPulp,Asymptomatic(Chronic)ApicalPeriodontitisO-DurabilityandresistancetocoronalmicroleakageTreatment Plan:Non-surgicalRCT#4and#5.Multiplevisitswillberequired.
CRITICALQUESTIONMESHTerms:Forpatientsreceivingrootcanaltherapy,whichtemporaryrestorativematerial(Cavit,IRM,orRootCanalTherapy;KetacFillGI)comparesmostfavorablytothepropertiesofthedefinitiverestorationasmeasuredDentalRestoration,bydurabilityandresistancetocoronalmicroleakage?Temporary;Leakage
CASESIGNIFICANCEFewinvivostudiesandnosystematicreviewsexiststudyingthistopic.However,fromtheavailableevidencethefollowingconclusionscanbedrawn:1.Cavitprovidesanadequatesealoveratleast3weeksasrevealedbyaninvivostudy(1).However,duetoitspoormechanicalproperties,itsuseshouldbereservedonlyforconservativeaccesseswhereocclusalforcesareminimal(3).2.IRMprovidesanadequatesealoveratleast3weeksasrevealedbyaninvivostudy(1).ItsmechanicalpropertiesaresuperiortoCavitanditisthereforeindicatedforwheneverthetoothwillberegularlysubjectedtoocclusalforces.Asthepowder:liquidratioisdecreased,thesealimproves(attheexpenseofmechanicalproperties).(3)3.GIhasbeenfoundinaninvitrostudytohaveasuperiorsealtoCavitandIRM(2).Becauseofthis,GIhasbeenrecommendedforlongertermtemporization(3).4.Studieshaverecommendedthatadefinitiverestorationbeplacedassoonaspossiblefollowingobturation(2,3).
CAT(1)Beachetal.“ClinicalEvaluationofBacterialLeakageofEndodonticTemporaryFillingMaterials.”JournalofEndodontics22:9pp459-462.1996.Methods:51humanteethreceivedRCTinvivo.Afterobturationasterilepaperdiskwasplacedbelowa4mmfillingofCavit,IRM,orTERM.Threeweekslaterthepatientswererecalled,thefillingswereremoved,andthepaperdiskswereanalyzedforbacterialgrowth.Results/Conclusion:1/18IRMsamplesshowedbacterialgrowth,whereas0/19Cavitsamplesshowedgrowth.NosignificantdifferencewasfoundbetweenIRMandCavit.Validity/Applicability:Restorationtypewasrandomlyassigned.Followupwas100%.invivostudy.3weekfollow-uprealisticatUICCOD.LevelofEvidence:2(RandomizedControlledTrial)
CAT(2)Bartheletal.“LeakageinRootsCoronallySealedwithDifferentTemporaryFillings.”JournalofEndodontics25:11pp731-734.1999.Methods:103extractedsingle-rootedteethreceivedRCTandwerethenfilledwitheitherCavit,IRM,GI,Cavit/GI,orIRM/GI.Teethwerethenimmersedintoatwo-chambersystemwhichwasinspecteddailyovera30-dayperiodforbacterialmicroleakage.Results/Conclusion:GIgavethebestsealagainstbacteria(1/20samplesleaked),whereasCavitgavethepoorestseal(13/20samplesleaked).11outof20IRMsamplesleaked.Validity/Applicability:Resultsofinvitrostudiescannotdirectlybeappliedtoclinicalpractice.However,allavailablefillingmaterialstoUICCODstudentsweretested.LevelofEvidence:6(Preclinicalstudy).
CAT(3)Naoum&Chandler.“TemporizationforEndodontics.”InternationalEndodonticJournal35:pp964-978.2002.Methods:AliteraturereviewwasperformedusingMEDLINEandcontemporarytextbookstoassessvariousendodontictemporaryfillingmaterialsandtomakeclinicalrecommendations.Results/Conclusion:CavitpossessesfavorablemarginalsealbutinferiormechanicalpropertiescomparedtoIRM.StudieshaveshownthatIRMalsoprovidesafavorablemarginalseal,especiallywhenthepowder:liquidratioisdecreased.GIismorecostly,buthasbeenfoundtobeantibacterialandtohaveasuperiorseal;thusitmaybeusedforcasesoflong-termtemporization.Validity/Applicability:Authorsdidnotprovideadetailedselectioncriteriaforarticlesreviewed.LevelofEvidence:5(ExpertOpinion)
Tooth Cold EPT Perc Palp Probing Mobility
3 WNL 31/80 WNL WNL 323B323L 0
4 NR 80/80 WNL WNL 323B323L 0
5 NR 80/80 WNL WNL 323B323L 0
6 WNL 26/80 WNL WNL 323B323L 0

Tooth
Cold EPT Perc Palp Probing Mobility
7 WNL 35/80 - - 323B/323L
0
8 WNL 24/80 - - 324B/423L
0
9 WNL 36/80 - - 423B/323L
0
10 WNL 32/80 - - 323B/323L
0
Direct Pulp Capping: Mineral Trioxide Aggregate (MTA) orCalcium Hydroxide (Dycal)?
Student: Andrea VenizelosAdvisors:Satish Alapati, BDS,MS,PhD; BradfordJohnson, DDS, MHPE, UIC Department of Endodontics
CRITICAL QUESTIONDuring caries excavation on a mature adult tooth a pinpoint pulp exposure (<1mm) is noticed, forincreased survival of the tooth, which material should be used for pulp capping: MTA (MineralTrioxide Aggregate) or Calcium Hydroxide (Dycal)?
CAT 1Olsson et al. “Formation of a Hard TissueBarrier After Pulp Capping in Humans. ASystematic Review.” International EndodonticJournal 36pp429-442.2006.Methods: A PubMed and Central literaturesearch with specific terms were made. Level ofevidenceof the publications was assessed.Results/Conclusion: 21 publications remainedafter interpretation. None had a high level ofevidence, one had moderate level of evidence,and 20 had a low level of evidence. Evidencegrade was determined to be insufficient. Doesnot imply that there is no effect of a pulpcapping procedure, but rather a need for high-quality studies. Capping material includedcalcium hydroxide, bonding materials,Vitrebond, synthetic hydroxyapatite, isobutylcyanoacrylate, andMTA.Validity: Had valid inclusion criteria, andevaluated LOE.LOE: 1(Systematic Review)
CAT 2Aeinehchi et al. “Mineral Trioxide Aggregate(MTA) and Calcium Hydroxide as Pulp-CappingAgents in Human Teeth: A Preliminary Report.”International Endodontic Journal 36 pp 225-231.2003.Methods: 22 maxillary third molars weresubjected to mechanical pulp exposure. Pulpcapping material was either MTA or calciumhydroxide, covered with ZOE and restored withamalgam. Extractions were after periods of 1week, 2 months,and 6 months.Results/Conclusion: Less inflammation,hyperemia and necrosis plus thicker dentinalbridge and more common odontoblast layerformation with MTA was found than withcalcium hydroxide.Validity: Direct pulp capping material wasrandomly assigned. Small sample size, largedrop-outof patients.LOE: 2(RandomizedControlledTrial)
CAT 3Nair et al. “Histological, Ultrastructural andQuantitative Investigations on the Response ofHealthy Human Pulps to experimental Cappingwith Mineral Trioxide Aggregate: ARandomized Controlled Trial.” InternationalEndodonticJournal 42pp422-444.2009.Methods: A pulpal exposure was made in 35healthy maxillary third molars from 23patients. Pulp capping material was either MTAor Dycal. 33 of these teeth were histo-morphologically processed. Cavities wererestored with IRM. Extractions were afterperiodsof 1 week, 1 month,and 3 months.Results/Conclusion: Pulp exposures treatedwith MTA were essentially free frominflammation and covered with hard tissuebridges. Teeth treated with Dycal had less hardtissue formation, more pulpal inflammation,and seepageof material into thepulp.Validity: Direct pulp capping material wasrandomlyassigned.Follow upwas 100%
LOE: 2(RandomizedControlledTrial)
CASE SIGNIFICANCEStudent SummaryFew in vivo studies are available on this topic.However, from the available evidence the
following conclusionscan bedrawn:
1. Calcium hydroxide does not adhere to thedentin and lacks the ability to seal. Seepage ofmaterial into the pulp is probable. Hard tissuebridges that form are incomplete and presentwith tunnel defects that act as a pathway formicroleakage.
2. Pulp defects treated with MTA have lessinflammation, less hyperemia, more stable hardtissue bridges with increased thickness, and arefree from tunnel defects. MTA shows greaterability to providea fluid-tight seal.
3. MTA has a much greater cost than calciumhydroxide.
4. There is a need for more high-quality studiesfor MTA to definitively be the material of choicefor direct pulpcapping.
CASE SCENARIODuringcaries excavationona mature adult tootha pinpointpulpexposureis noticedand pulpcappingis indicated.
P… Adult with pinpointpulp exposure(<1mm)
I…Direct pulpcapping
C…Material ((Mineral Trioxide Aggregate(MTA)orCalcium Hydroxide(Dycal))
O…Increasedsurvival of tooth
MESH Terms:Dental Pulp Capping; PulpalResponse; Mineral TrioxideAggregate; CalciumHydroxide
Exam:EOEWNL. IOEreveals large DBIL carious lesion.
Diagnosis: #8 Normal Pulp with NormalPeriapical
TreatmentPlan: Excavatecaries and restore.RCT notindicated

Ideal Luting Agent for a Zirconia AbutmentStudent: Shivam Patel
Advisor: Dr. Satish Alapati
CASE SIGNIFICANCEStudent Summary
CRITICAL QUESTIONFora patient receivingan imlpant in an estheticzonewith a Zirconia basedabutment,what is theideal luting agentthat will provideadequateretentionto preventdislodgement?
CAT 1NejatidaneshF, Savabi O, ShahtoosiM.“Retentionofimplant-supportedzirconiumoxideceramic restorationsusingdifferentluting agents.”Clin Oral Implants Res.2011Nov14.
Methods:20ITI abutments(5.5mmheight)andITI implant analogs mountedto acrylic blocks.90ZrO2copings(Al2O3 abraded).Copingsconditionedin artificial saliva and thermocycledand cementedw/ various cements.
Results/Conclusion: Resinbasedand RMGIluting agentsare mostretentive.Cementselection shouldbebaseduponsite as well asoptionfor retrievability.
Validity/Applicability: Studylimitations weremonotonicstatic load, in vivo forceshavedynamicloading.Fatigueof cementsunderloadnotanalyzedbutdata presentedand eachspecimenonlysubjectedto onevariable (lutingagent).
Levelof Evidence:Level 5 – Benchtopresearch
CAT 2Kim, Min-Jeong,et al. "ShearBondStrengthsofvarious LutingCementsto Zirconia Ceramic:SurfaceChemical Aspects." Journalof dentistry39.11(2011):795-803..
Methods:Mutiple cementtypeswerebondedto sandblastedZrO2(Lava). Specimenswerestoredin water at 37 degreesC and other½thermocycled.Shearbondstrengthsandsurface energyparameterswererecorded.
Results/Conclusion: Panavia F 2.0andPrincipleproducedhigherbondstrengthsthan othercementsw/ nosignificant differencesbeforeorafter thermocycling.
Validity/Applicability: Thestudysuggeststhatsurface energyparametersshouldbeimportantconsiderationsin determiningwhichluting agentshouldbeutilized for properadhesion.Various surface treatmentsshouldbeincorporatedfor comparison
Levelof Evidence:Level 5 – Benchtopresearch
CAT 3EkfeldtA, FürstB, Carlsson GE. “Zirconiaabutmentsforsingle-toothimplant restorations:a retrospectiveand clinical follow-upstudy.”Clin Oral Implants Res. 2011Nov;22(11):1308-14.
Methods:Part 1 – Retrospectiveevaluationof130patientsw/ 185STIrestorations w/ ZrO2abutments.Part 2 – Clinical examof 25 patientsw/ 40restorationsplaced >3 yrs ago.93cementedw/ zinc phosphate,1 w/ resin cement,1 w/ TempBond
Results/Conclusion: ZrO2abutmentshad lowrate of technical andbiological complications,soft tissue respondedwell.
Validity/Applicability: Multiple focusparametersw/ short follow up butvast datacollection. Protocolfor surgeryandrestorationstandardizedand positive3-5year success.
Levelof Evidence:Low Level 3 – Retrospecitveanalysis and clinical follow upstudy
Many studies have been conducted on ZrO2plates/discs and the vast majority of searchresults were in vitro studies. Systematic reviewswere not available as the material in question isstill fairly newin thescopeof dental practice.
The topic has helped me realize the importanceof material science and its place in dentistry.Bonding concepts, biocompatibility, andphysical/chemical properties are factors thatcontribute a great deal to success within theoral cavity.
Based on my research resin based luting agentsare the best candidates for cementation onto aZrO2substrate such as an implant abutment. Airabrasion, priming, and trebochemicaltreatments are all areas for future research todetermine the best alternative to increase bondstrengths in the zirconia material withoutcompromisingits physical/chemical integrity.
CASE SCENARIOP – Patientreceivinga zirconia implant abutment
I – Resin basedluting cement
C – Conventionalcement
O – Adequatebondstrengthbetweenfinal restoration andabutment
MESH Terms:Zirconia abutmentLutingAgent
ImplantBonding
Meanmicrotensile bondstrengthsforceramic bondedtocompositegroups.
24 y/o hispanic female presents after traumatic avulsion #25. She would like to have a fixed restoration,preferably a dental implant. Esthetics and function are her primary concern. IOE reveals a thin soft tissuebiotypewhich may havean adverseoutcomeif stock/titanium abutmentis utilized.
Mean(standarddeviation)of dislodgining forcesof thestudiedcement(N) groups.

CaseCATLiteratureWorksheet

Evaluation Sheet

Once you have identified a case:
Identify a mentorPrimary Contact: Group Practice ManagerAll project Titles should turned in toKatherine Long at [email protected]
ASAPTalk to previous participants

Questions?
CaseCAT contacts:
Dr. CroweDr. KnightElizabeth Razdolsky