Type 1 diabetes review · 2019-11-18 · Unmet Needs in Type 1 Diabetes •A1C should be lower,...
31
BEYOND INSULIN FOR GLYCEMIC TREATMENT OF TYPE 1 DIABETES John B. Buse, MD, PhD Verne S. Caviness Distinguished Professor Chief, Division of Endocrinology Director, Diabetes Center Director, NC Translational and Clinical Sciences Institute Executive Associate Dean, Clinical Research University of North Carolina School of Medicine
Transcript of Type 1 diabetes review · 2019-11-18 · Unmet Needs in Type 1 Diabetes •A1C should be lower,...

BEYOND INSULIN FOR GLYCEMIC TREATMENT OF TYPE 1 DIABETES
John B. Buse, MD, PhD
Verne S. Caviness Distinguished Professor
Chief, Division of Endocrinology
Director, Diabetes Center
Director, NC Translational and Clinical Sciences Institute
Executive Associate Dean, Clinical Research
University of North Carolina School of Medicine

T1D is a Burdensome Disease
1
People with T1D never get
a day off from managing it
It requires constant
monitoring of blood
glucose levels
People with T1D must wear
a pump or use injections to
dose insulin
It requires constant
management, 24 hours
a day
Must count the carbs and
account for everything
they eat
It is exhausting and
has long term
dangerous long-term
complications
Risk of nighttime hypoglycemia
and seizures
Risk of hypoglycemia

Comorbidities and Complications of T1D
Acute
• Hypoglycemia
• Diabetic Ketoacidosis (DKA)
Chronic
• Retinopathy
• Nephropathy
• Neuropathy
• Cardiovascular disease

The Impact of Diabetes Technology To Treat and
Manage T1D
CGM adoption continues to rise
(38% in 2018) in all age groups
No significant increase in
pump adoption
3Foster & T1D exchange clinic network (2019). DIABETES TECHNOLOGY & THERAPEUTICS

Despite Improved and More Widely Adopted Diabetes Technology, Clinical Outcomes Continue to Decline
What can be done now
▪ Support increased use of CGM in all ages and stages
▪ Transform device data to enhance self-management
(ex; decision support tools, etc.)
▪ Personalize treatment options (ex; adaptive algorithms,
open protocol, etc.)
▪ Use of adjunct therapies for added glycemic and
metabolic benefits
2016-18
2010-12
(Foster et al. Diabetes Technology and Therapeutics (2019) 21:66-72; DOI: 10.1089/dia.2018.0384)

Unmet Needs in Type 1 Diabetes
• A1C should be lower, particularly early in the course of the disease
• Weight is a concern for many patients and their providers
• Severe hypoglycemia is an important and immediate complication
• DKA remains an issue, even in patients who are apparently well managed
• While blindness and amputations have been largely eliminated in type 1 diabetes populations with good access to care, chronic kidney disease and cardiovascular disease remain important causes of morbidity and mortality
Will emerging technologies (closed loop, novel insulin analogs, glucose responsive insulin) solve these issues?
October 2019 9

Type 2 Diabetes Drugs in Type 1 DiabetesDrugs studied – improvements - harms
• Metformin: BMI (1), insulin, cholesterol – hypo, GI adverse events1
• Alpha-glucosidase inhibitors: nocturnal hypoglycemia, post-prandial hyperglycemia – GI
adverse events2
• Thiazolidinediones: insulin, mixed effects on progression – weight gain3
• GLP-1 receptor agonists: A1C (~0.3%), weight (~4 kg) – GI adverse effects, hypoglycemia,
ketosis4,5
• Pramlintide: A1C (~0.3%), weight (1.5-3 kg), PPG – GI adverse effects, hypoglycemia 5
• SGLT inhibitors: A1C (~0.4%), TIR improvement – DKA, genital infections 5
• GKA: A1C (~0.7%), TIR improvement – none reported thus far (only phase 2 data available
for 20 subjects)6
Exemplar references: 1. Vella S, et al. Diabetologia 2010; 53:809. Meng H, et al. Diabet Metab Res Rev 2018; Epub. Petrie JR, et al. Lancet D&E 2017; 5:597. 2. Raju B, et al. J Clin Endocrinol Metab. 2006; 91:2087-92. Riccardi G, et al. Diabet Med. 1999; 16:228. 3. Strowig SM, Raskin P. Diabetes Care. 2005; 28:1562. Shimada A, et al. Diabetes Metab Res Rev. 2011; 27:951. Yang Z, et al. Diabetes Res Clin Pract. 2009; 83:54-60.4. Wang W, et al Diabetes Ther 2017; 8:727. Ahren B, et al. Diabetes Care 2016; 39:1693. Mathieu C, et al. Diabetes Care 2016 39:1702.5. Warnes H, et al. Diabetes Ther. 2018; 9:1831-1851.6. Valcarce C, Freeman J, Dunn I, Dvergsten C, Soeder T and Buse J. Results from the sentinel and learning phase of the Simplici-T1 study, the first clinical trial to test activation of glucokinase as an adjunctive treatment for type 1 diabetes. Presented at 55th EASD conference, Barcelona, Spain, September 2019
October 2019 10

Injected Adjunctive Therapies
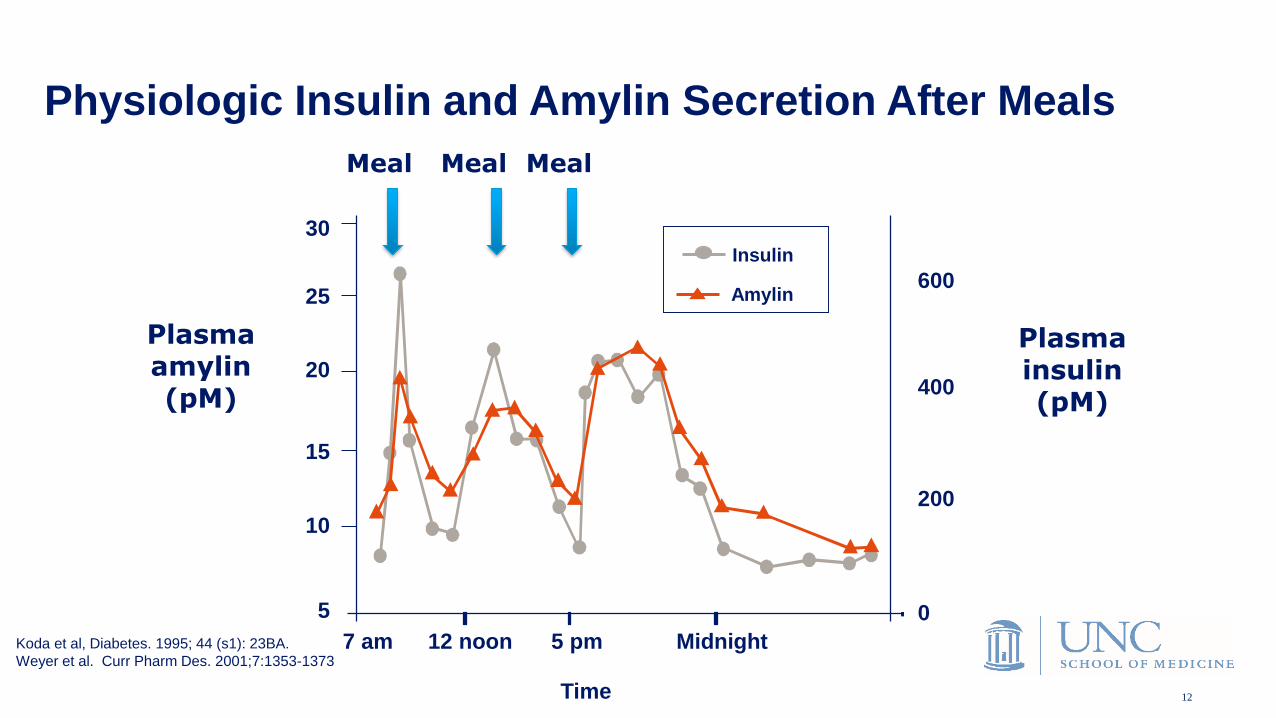
Physiologic Insulin and Amylin Secretion After Meals
Plasma insulin (pM)
Plasma amylin (pM)
30
25
20
15
10
5
7 am Midnight5 pm12 noon
Time
600
400
200
0
Meal Meal Meal
Koda et al, Diabetes. 1995; 44 (s1): 23BA.
Weyer et al. Curr Pharm Des. 2001;7:1353-1373
Amylin
Insulin
12

Pramlintide Reduces
FBG, PPG and Glucose Fluctuations
120
140
160
180
200
220
Glu
co
se
(m
g/d
L)
pre-bf post-bf pre-lu post-lu pre-di post-di bedtimeClinical Practice Study, 120 g SYMLIN
bf, breakfast; lu, lunch; di, dinner
N=166; *p-values for all data points <0.05
Edelman,S et al. Diabetes. 56 (Suppl 1):1826-P.
*
*
*
*
*
* *
insulin alone
insulin plus pramlintide
13
Pramlintide Summary
• A1C reduction versus placebo: 0 to -0.4%
• Insulin dose reduction: minimal
• Weight loss: 0 to 3 kg
• Hypoglycemia: Variable increase in severe hypoglycemia
• Substantial post-prandial glucose lowering
• Anecdotal improvement in sense of well-being
• GI adverse effects, particularly early in therapy
• Whether due to the need for taking an injection with each meal with waning adherence or due to tachyphylaxis, most patients did not continue on pramlintide long-term
Warnes H, et al. Diabetes Ther. 2018; 9:1831-1851.
Buse, personal observations
14

Liraglutide in Type 1 Diabetes:
Change in HbA1c from Baseline to End of Treatment
Data are estimated means. Full analysis setBL, baseline, HbA1c, glycosylated haemoglobin1. Mathieu C et al. Diabetes Care 2016;39:1702–1710; 2. Ahrén B et al. Diabetes Care 2016;39:1693–1701
HbA1c: –0.09% to –0.20%
Time since randomisation (week)
Hb
A1
c(%
) 8.0
7.0
0 8 12 16 20 26 32 38 44 52
HbA1c: –0.23% to –0.35%
7.5
7.6
7.7
7.8
7.9
8.0
8.1
8.2
0 8 12 16 20 26
Hb
A1
c(%
)
Time since randomisation (week)
Liraglutide 1.8 mg Liraglutide 1.2 mg Liraglutide 0.6 mg Placebo
ADJUNCT ONE1
ADJUNCT TWO2
7.2
7.4
7.6
7.8
8.2
8.4
Mean BL value Mean BL value
0.1299
0.0164
0.0019
p value vs placebo
0.0011
0.0021
<0.0001
p value vs placebo
15

Liraglutide in T1D: Conclusion
• “In conclusion, the current trial demonstrated that adding liraglutide to insulin
therapy for a population generally representative of people with type 1 diabetes
resulted in:
• better glycemic control, less insulin, greater body weight loss, and a greater proportion
of subjects achieving the ADA target of HbA1c <7%.”
• “This dose-dependent effect was accompanied by a higher rate of:
• symptomatic hypoglycemia and hyperglycemic episodes with ketosis, limiting the
clinical use of GLP1-RAs in people with type 1 diabetes.”
HbA1c, glycosylated haemoglobin
Mathieu C et al. Diabetes Care 2016;39:1702–1710
16

Oral Adjunctive Therapies

Meal
SGLT1 Glucose
Absorption
Glucose Filtration
Blood Glucose
Increased Urinary Glucose Excretion
X
Post-meal Glucose Levels
Zambrowicz et al 2012 Clin Pharmacol TherNishimura et al 2015 Cardiovasc Diabetol
Tissues
SGLT2(SGLT1)Glucose
Reabsorption
X
Intestinal SGLT1-Mediated Glucose Absorption
Renal SGLT2 (SGLT1) Mediated Glucose Reabsorption
October 2019 18

Study DEPICT1,2 inTandem3-5 EASE6
Drug, dose Dapagliflozin • 5 mg • 10 mg • Placebo
Sotagliflozin• 200 mg • 400 mg • Placebo
Empagliflozin• 2.5 mg• 10 mg• 25 mg• Placebo
3 SGLT Development Programs have Completed Phase 3:
DEPICT, inTandem, EASE
1. Dandona P, et al. Lancet Diabetes Endocrinol. 2017;5:864-876.
2. Mathieu C, et al. Diabetes Care. 2018;41:1938-1946.
3. Garg SK, et al. N Engl J Med. 2017;377:2337-2348.
4. Buse JB, et al. Diabetes Care. 2018;41:1970-1980.
5. Danne T, et al. Diabetes Care. 2018;41:1981-1990.
6. Rosenstock J, et al. Diabetes Care. 2018 Oct 4. [Epub ahead of print]
October 2019 19

*Lower doses retain much of the glycemic efficacy with lesser effect on weight and blood pressure.
Efficacy (Placebo Adjusted) At Highest Dose*
HbA1C reduction ~0.4%
Time in range (blinded CGM) ~3-hour increase
Time in hypoglycemia (CGM) No change or some reduction
Insulin dose 10%-15% reduction
Weight ~3-kg reduction
Systolic blood pressure ~3 mm Hg reduction
Patient reported outcomes Improved
To Summarize the Findings . . . (difficult to make precise efficacy comparisons across trials due to design and analysis differences)
In selected patients with T1D with inadequate glycemic control, consider the
use of an SGLT inhibitor as an adjunct to insulin therapy
20

Case: The ResultBefore: Glargine 46 Units/day + Aspart 30 Units/day; HbA1C: 8.8%
After: Glargine 32 Units/day + Aspart 24 Units/day + SGLT inhibitor
HbA1C: 6.5%; total daily dose reduced by ≈25%
14 pound weight loss
Statistics
Average glucose 148 mg/dL
Sensor usage 14 of 14 days
Calibrations per day 1.9
Standard deviation ±6.3 mg/dL
39% high
57% target
3% low
Target range 70 to 150 mg/dL
Nighttime 10 PM to 6 AM
39
57
3
Images courtesy of Satish K. Garg, MD.

Garg SK, Strumph P. N Engl J Med. 2018; 378:967-968
Comparison of Diabetic Ketoacidosis
Incidences in Phase 3 Studies
• Dapagliflozin and sotagliflozin are not approved in the US. Approved in the EU as oral
adjunctive treatments to insulin in T1D patients with BMI ≥ 27 (~1/4 of T1D patients).
• Empagliflozin EMDAC hearing scheduled November 13, 2019
22

DKA hazard ratios in SGLT2 trials of T1D
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

T1D SGLT inhibitor patient selection
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

T1D SGLTi Rx: Initial treatment
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

T1D SGLTi Rx: DKA risk mitigation
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

T1D SGLTi Rx: Wallet card (face)
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

T1D SGLTi Rx: Wallet card (back)
Goldenberg RM, et al. DOM. https://doi.org/10.1111/dom.13811

Investigational Agent

Glucokinase: The Physiological Glucose-sensor
vTv Therapeutics LLC, October 2019 30
❑ In humans, abnormal GK activity due to activating or inactivating mutations is linked to hyperglycemic and hypoglycemic conditions respectively
❑ In humans, loss of function mutations on the GKRP are associated with increased plasma lipids (Rees et al. J Clin Invest. (2012) 122, 205-217)
❑ In rodents, GKRP KO mice showed:▪ Decrease of GK expression in the liver▪ Glucose intolerance▪ Insulin resistance
Targeting hepatic glucokinase to treat diabetes with TTP399, a hepatoselective glucokinase activator A. Vella, J. L. R. Freeman, I. Dunn, K. Keller, J. B. Buse and C. Valcarce, Science Translational Medicine 16 Jan 2019: Vol. 11, Issue 475, eaau3441. DOI: 10.1126/scitranslmed.aau3441

TTP399: The Importance of Tissue Selectivity and Preservation of Physiological Regulation to Avoid Pitfalls
vTv Therapeutics LLC, October 2019 31
▪ Based on genetic information, TTP399 was designed to avoid the expected pitfalls of GK activation:
• Liver selective: TTP399 does not activate GK in the beta-cells, i.e. no risk of hypoglycemia
• MoA preserves the natural interaction of GK-GKRP in the liver, i.e. no increase in lipids
Two essential criteria, validated by human mutations, to sustain glucose control without
causing hypoglycemia or hyperlipidemia
Targeting hepatic glucokinase to treat diabetes with TTP399, a hepatoselective glucokinase activator A. Vella, J. L. R. Freeman, I. Dunn, K. Keller, J. B. Buse and C. Valcarce, Science Translational Medicine 16 Jan 2019: Vol. 11, Issue 475, eaau3441. DOI: 10.1126/scitranslmed.aau3441

❑ 11 clinical studies completed with TTP399 in healthy volunteers and T2DM patients ▪ 9 phase I studies ▪ 2 phase II studies ▪ Safety results included in TTP399 IB V7
❑ 1 ongoing clinical study with TTP399 in T1DM patients▪ Sentinel phase – 5 patients▪ Part 1 – 20 patients
❑ Approximately 500 subjects have received one or more doses of TTP399
❑ TTP399 was well tolerated at all doses tested
❑ The clinical results obtained to date are consistent with preclinical data and the MOA of a liver-selective GKA
Clinical Trials with TTP399
vTv Therapeutics LLC, October 2019 32
Targeting hepatic glucokinase to treat diabetes with TTP399, a hepatoselective glucokinase activator A. Vella, J. L. R. Freeman, I. Dunn, K. Keller, J. B. Buse and C. Valcarce, Science Translational Medicine 16 Jan 2019: Vol. 11, Issue 475, eaau3441. DOI: 10.1126/scitranslmed.aau3441

TTP399-203 (Simplici-T1): Adaptive Phase 1b/2 Study Trial Design
vTv Therapeutics LLC, October 2019 33
Completed June 2019 Results expected in Q1 2020
Phase 2-Part 1 (Learning Phase)
Study Design:
▪ Double-blind Placebo control
▪ 12 weeks dosing 800mg QD
▪ ~20 adult subjects with T1D on CSII and CGM
▪ Primary Endpoint: change in HbA1c
TTP399 was well tolerated➢ No incidents of severe hypoglycemia or DKA➢ Indications of improved glycemic control, while
reducing insulin dose • Increase % time in range • Reduce % time in hyperglycemia without increasing
% time in hypoglycemia
Q1 2020June 2019
Phase 2-Part 2 (Confirming Phase)
Study Design:
▪ Double-blind Placebo control
▪ 12 weeks dosing 800mg QD
▪ ~90 adult subjects with T1D (all comers)
▪ Primary Endpoint: change in HbA1c
Phase 1 (Sentinels)
Study Design:
▪ Open-label
▪ 7 day dose escalation up to 1200mg QD
▪ 5 adult subjects with T1D on CSII and CGM
March 2018
ClinicalTrials.gov Identifier: NCT03335371
Valcarce C, Freeman J, Dunn I, Dvergsten C, Soeder T and Buse J. Results from the sentinel and learning
phase of the Simplici-T1 study, the first clinical trial to test activation of glucokinase as an adjunctive
treatment for type 1 diabetes. Presented at 55th EASD conference, Barcelona, Spain, September 2019
Subjects with Continuous Subcutaneous Insulin Infusion (CSII) and Continuous Glucose Monitoring (CGM)

• Multiple unmet needs in type 1 diabetes:
• A1C should be lower, particularly early in the course of the disease
• Weight is a concern for many patients and their providers
• Severe hypoglycemia is an important and immediate complication
• DKA remains an issue, even in patients who are apparently well managed
• Chronic kidney disease and cardiovascular disease in type 1 diabetes is high and completely
unaddressed by clinical trials
• Pramlintide FDA-approved but challenging to use
• Metformin, alpha-glucosidase inhibitors, thiazolidinediones, GLP-1 receptor agonists not moving
towards regulatory approval
• SGLT inhibitors partially address those unmet needs, but is the balance of efficacy and safety adequate
for FDA approval?
• GKA TTP339 shows promise as an adjunctive therapy in T1D
Summary
34