Molecular epidemiology of human and animal tuberculosis in ...

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 1
Tuberculosis epidemiology: Using data to inform TB control approaches and priorities
Lisa Pascopella, PhD, MPHSenior EpidemiologistTuberculosis Control BranchCalifornia Department of Public HealthNovember 18, 2019
Objectives
• Describe the epidemiology of tuberculosis in the U.S. • Describe how epidemiologic and population data can
be used to inform TB prevention and control activities

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 2
Topics• Epidemiology of TB in the United States• Death with TB• Epidemiology of TB in California• TB prevention cascades in
Contacts to infectious TB cases
New arrivers with abnormal chest radiographs
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Tuberculosis in the United States1993–2018*
National Tuberculosis Surveillance System
Division of Tuberculosis Elimination
*Updated as of June 6, 2019

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 3
Reported Tuberculosis (TB) Cases and Rates United States, 1993–2018
Percentage of TB Cases by State, United States, 2018
DC, District of Columbia
DC
12.56.5
23.2
8.3

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 4
Tuberculosis Case Rates by Reporting Area United States, 2018
3.9
5.3
8.5
TB Incidence Rate (per 100,000 persons)8.4
5.3
8.5
3.9
NYC (6.7)
D.C. (5.1)
TB Incidence Rate (per 100,000 persons)
8.5
5.3
TB Cases and Rates Among U.S.-Born versus Non-U.S.–Born Persons, United States, 1993–2018
Cas
es
pe
r 1
00
,00
0 P
op
ula
tio
n

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 5
Countries of Birth Among Non-U.S.–Born Persons Reported with TB, United States, 2018*
*Percentages are rounded.
Percentage of Non-U.S.–Born TB Casesby Time in the United States at Diagnosis, 2018
Pe
rce
nta
ge o
f TB
Cas
es
Time in the United States

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 6
TB Case Rates by Race/Ethnicity,* United States, 2010–2018
* All races are non-Hispanic; multiple race indicates two or more races reported for a person, but does not include persons of Hispanic/Latino origin.† Asian race category reporting includes Pacific Islander from 1993–2002; Native Hawaiian/Other Pacific Islander race first reported separately in 2003.§ Multiple race rates first reported in 2003..
Cas
es
pe
r 1
00
,00
0 p
op
ula
tio
n
Reported TB Cases by Origin and Race/Ethnicity*, United States, 2018†
Non-U.S.–born persons § U.S.-born persons
* All races are non-Hispanic; multiple race indicates two or more races reported for a person, but does not include persons of Hispanic/Latino origin.† Percentages are rounded.§ American Indian/Alaska Native accounted for <1% of cases among non-U.S.–born persons and are not shown.
Native Hawaiian/Pacific Islander
American Indian/Alaska Native
Multiple Race
White
Hispanic/Latino
Black/African American
Asian

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 7
TB Case Rates by Age Group, United States, 1993–2018
Cas
es
pe
r 1
00
,00
0 p
op
ula
tio
n
Year
Distribution of Sex by Age Group, United States, 2018
Males Females
<5 yrs
5–14 yrs
15– 4 yrs
25–44 yrs
45–64 yrs
65+ yrs
Age Group

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 8
U.S. TB Cases by Site of Disease, 2018
*Any pulmonary involvement which includes cases that are pulmonary only and both pulmonary and extrapulmonary.Patients may have more than one disease site but are counted in mutually exclusive categories for surveillance purposes.
Note: Percentages are rounded.
National guidance: Assess pulmonary involvement for any form of TB
For diagnostic purposes, all persons suspected of having TB disease at any site should have sputum specimens collected for an AFB smear and culture, even those without respiratory symptomsfrom CDC’s Core Curriculum on TB Chapter 4

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 9
Isoniazid Resistance Among U.S.-Born versus Non-U.S.–Born Persons, United States, 1993–2018
Cases of MDR TB by History of TB, United States, 1993–2018*
* Based on initial isolates from persons with no prior history of TB; multidrug-resistant TB (MDR TB) is defined as resistance to at least isoniazid and rifampin.

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 10
HIV Coinfection by Age Among Persons Reported with TB, United States, 2011–2018
Reported TB Cases by Risk Factor, United States, 2018
Non-HIV immunosuppression
Contact to Infectious TB
Diabetes Mellitus
Contact to Infectious TB Diabetes Mellitus
Comparison of Selected Risk Factors by Origin of BirthMost Common Risk Factors Reported Among TB Patients

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 11
*Correctional facilities include federal prisons, state prisons, local jails, juvenile correctional facilities, other correctional facilities, or unknown type of
correctional facility.
TB Cases among Residents of Correctional Facilities Ages ≥15, 1993–2018*
TB Cases Ages ≥15 with Other Selected Risk Factors, 2018
Risk Factor

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 12
Substance Misuse Among TB Patients ≥15 years, United States, 2018
Risk factors for TB
Born in a non-US country where TB is endemicLiving with HIV, diabetes, other immunosuppressionExperiencing homelessnessUsing substances (e.g. injection drugs)Living in certain institutional settings

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 13
TB treatment outcomes
The majority of TB patients complete their treatment within 12 monthsFew TB patients are lost to followupTB patients who move may be provided with continuity of careAlmost 10% of TB patients die while on treatment
TB Cases by Reason Therapy Stopped, 2016*
*Data available through 2016 only.
Outcomes for patients that did not complete treatment

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 14
Death with TB
Reported Tuberculosis (TB) Deaths* and Rates United States, 1993–2017
*National Vital Statistics System Multiple Causes of Death (accessed from CDC Wonder)

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 15
TB Surveillance data is more accurate than Vital Statistics data for TB patients who die
We have reviewed the characteristics of the population who has TBNow let’s review what we know about persons who die with TB
Although TB is a preventable and curable disease, approximately 10% of persons with TB die with TBWhy?Can we prevent death with TB?

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 16
Published in Annals ATS, Vol 15 June 2018
TB Epidemiologic Studies Consortium Mortality Study Objectives
Assess the frequency of TB-related deathsIdentify risk factors for TB-related death

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 17
Methods
• Reviewed deaths of TB cases reported 2005-2006
• Inpatient and outpatient medical records
• Laboratory records
• Used standardized and piloted algorithm to determine TB-relatedness
• Trained data abstractors
• 2 reviewers per case (at least 1 TB clinician)
• 3rd reviewer to resolve disagreements
• Classification
• Definitely or probably TB-related
• Definitely not or unlikely TB-related
• Unclassifiable
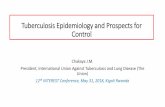
TB relatedness and timing of deaths
1,304 adults who died
942 (72%)TB-related deaths
272 (21%) TB-unrelated
deaths
90 (7%) could not be classified
705 (75%) TB-related deaths during
treatment
237 (25%) TB-related deaths before
treatment
329 (47%) TB-related deaths
within 30 days of diagnosis
371 (53%) TB-related deaths >31
days after diagnosis

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 18
Time to deathTB related vs TB-unrelated
TB unrelated
TB related
Days to death
Study algorithm/Death cert TB was not an immediate,
underlying, or contributing
cause of death
TB was an immediate,
underlying, or
contributing cause of
death
Totala
Not TB-related death 185 (75) 61 (25) 246 (23)
TB-related death 378 (45) 469 (55) 847 (77)
Totala 563 (52) 540 (48) 1093 (100)
Study algorithm vs. Death certificate
aDeath certificates were not available for 10% of decedents
Kappa = 0.21 (0.16, 0.26)
Sensitivity of death certificate=55.4% (51.9,58.7)Specificity of death certificate=75.2% (69.3, 80.5)

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 19
Risk factors for TB-related death
Delayed diagnosis
Extensive TB disease
Immune suppression
Comorbidities
Started anti-TB treatment as inpatient
TBESC study conclusions
• 72% TB deaths were TB-related• Death certificates were not reliable
• and underestimate TB-related death• Need information from medical/hospitalization charts• Increased death risk when TB was diagnosed in hospital

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 20
What do we know about TB deaths in CA?
Reviewed recent surveillance data for 2 types
• Dead at diagnosis
• Died during treatment
Report of Verified Case of TuberculosisWas TB a cause of death?
1. Dead at diagnosis

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 21
CA TB surveillance data 2010-2016Dead at diagnosis
2% (n=304) TB cases dead at diagnosis
• 30% TB-related
• 40% not TB-related
• 30% unknown relatedness
Report of Verified Case of Tuberculosis Was death related to TB disease or TB therapy?
2. Died during treatment

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 22
CA TB surveillance data 2010-2016Died during treatment
8.4% (n= 1267) TB cases died on treatment
• 36% related to TB disease
• 1.6% related to TB therapy
• 41% not TB-related
• 21% unknown
Deaths on treatment for select local TB programsCA TB surveillance data 2010-2016
LHJ Unrelated to TB disease
Related to TB disease
Related to TB therapy
Unknown
a 40% 21% 0.5% 39%
b 43% 47% 2.8% 7%
c 24% 56% 1.9% 19%
d 55% 16% 0 29%
e 19% 70% 0 12%
Large range of responses across CA

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 23
Why the difference in TB-related deathTBESC study (72%) vs.CA surveillance (38%)?
• Diversity of responses to RVCT questions in CA• Variability in methods to ascertain TB-relatedness?• Role for independent review?
TB programs should review every death using a standardized approach that includes medical and hospital records
• To identify potential missed prevention opportunities• To monitor trends• To identify areas for working with partners

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 24
Consider using algorithm developed in CA for review of deaths
https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/TBCB-RVCT-Death-Algorithm-v1.0.pdf

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 25
TB epidemiology in California
How do TB Cases Occur in California?
TB in new arrivers TB within 6 months of arrival in US 2015-2017
Recent TransmissionRT recipient 2014-2016
Reactivation of remote
infection. Cases not from importation or recent transmission
2,000 TB cases/yr
12%
82%
6%
50

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 26
The Long View: Dramatic ProgressCalifornia Tuberculosis Epidemic 1930–2018
0
20
40
60
80
100
120
140
160
180
200
0
2,000
4,000
6,000
8,000
10,000
12,000
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
51
The Medium View: Dramatic ProgressCalifornia Tuberculosis Epidemic 1991–2018
0
2
4
6
8
10
12
14
16
18
20
0
1,000
2,000
3,000
4,000
5,000
6,000
1991 1996 2001 2006 2011 2016
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
52

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 27
The Medium View: Slowing ProgressCalifornia Tuberculosis Epidemic 1991–2018
0
2
4
6
8
10
12
14
16
18
20
0
1,000
2,000
3,000
4,000
5,000
6,000
1991 1996 2001 2006 2011 2016
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
-4.3%
53
-6.2%
-1.2%
Progress StalledCalifornia Tuberculosis Epidemic 2014–2018
0
1
2
3
4
5
6
7
8
9
10
0
500
1,000
1,500
2,000
2,500
2014 2015 2016 2017 2018
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
54

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 28
Progress StalledCalifornia Tuberculosis Epidemic 2014–2018
2091
5.3
0
1
2
3
4
5
6
7
8
9
10
0
500
1,000
1,500
2,000
2,500
2014 2015 2016 2017 2018
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
55
Progress StalledCalifornia Tuberculosis Epidemic 2014–2018
2133 2131 2058 2059 2091
5.3
0
1
2
3
4
5
6
7
8
9
10
0
500
1,000
1,500
2,000
2,500
2014 2015 2016 2017 2018
Nu
mb
er
of
TB C
ase
s
TB Cases TB Rate
Cas
e R
ate
pe
r 1
00
,00
0
56

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 29
Photograph by Jodie JoOx http://yourshot.nationalgeographic.com/photos/6232126/ 57
Match the TB program strategy to the TB mechanism
58
TB in recent arrivers
Recent transmission
Reactivation of LTBI
• Overseas screening and treatment• Domestic evaluation and treatment
• Outbreak investigation• Contact investigation
• Risk assessment• LTBI testing• LTBI treatment

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 30
83% of cases in people born outside U.S.TB Cases by country of birth California, 2018
0% 20% 40% 60% 80% 100%
60
Other Countries
Mexico PhilippinesVietnam
China
India
83%
CentralAmerica
17%
U.S.

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 31
Cases from >120 countriesCountry of origin of TB cases 2014-2018, California
61
62
60
40
20
0
TB Incidence by Country of Birth,California, 2001−2016
Cas
es p
er
10
0,0
00
Philippines
Vietnam
IndiaChina
Mexico
U.S.
2004 2008 2012 2016

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 32
Large disparity by place of birthTB case rate by nativity California 2009–2018
2.21.2
18.9
16.1
0
2
4
6
8
10
12
14
16
18
20
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
63
Non-U.S.-born
U.S.-born
Disparity by place of birth increasingTB case rate by nativity California 2009–2018
2.21.2
18.9
16.1
9
13
0
2
4
6
8
10
12
14
16
18
20
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
FB:USB Ratio
64
U.S.-born
Non-U.S.-born

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 33
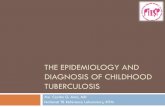
20x-60x higher rates among non-U.S.-born
minorities compared with U.S.-born whitesTB rate by race/ethnicity and nativity, 2018
0.5
1.7
2.7
2
4
11
19
29
0 10 20 30 40
White
Hispanic
Black
Asian
Rate per 100,000
Non-U.S.-born
U.S.-born
65
Most People with TB have been U.S. residents for many yearsYears in U.S. at TB diagnosis California, 2014-2018
0
200
400
600
800
1000
1200
0-1
2-3
4-5
6-7
8-9
10
-11
12
-13
14
-15
16
-17
18
-19
20
-21
22
-23
24
-24
26
-27
28
-29
30
-31
32
-33
34
-35
36
-37
38
-39
40
-41
42
-43
44
-45
46
-47
48
-48
50
-51
52
-53
54
-55
56
-57
58
-59
60
-61
62
+
TB C
ase
s
Years in U.S.
66
>50% in US >18 yrs

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 34
Half of TB cases are older than 55Age at Report of TB, 2018
0
5
10
15
20
25
30
35
40
45
50
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100
Nu
mb
er
of
case
s
Age
Median
Median age continues to increase: 53 (2014) 55 (2018)2018: Born outside US=57 years US-born=36 years 67
More TB Cases are Older% of TB Cases Aged 65+, 1993-2018
18%
23%
34%
0
5
10
15
20
25
30
35
40
1993 2008 2018
% o
f C
ases
68

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 35
More TB Cases are Older% of TB Cases Aged 65+, 1993-2018
5%9%
12%
0
5
10
15
20
25
30
35
40
1993 2009 2018
% o
f C
ases
80+
69
Decreasing TB in youngest kidsPediatric Cases <5yrs, California, 2009‒2018
82
28
3.5%
1.3%
0
1
2
3
4
0
20
40
60
80
100
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Pe
rce
nt
of
Cas
es
Nu
mb
er
of
Cas
es
70

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 36
Correctional cases increased in 2018Cases Diagnosed in a Correctional Facility, 2009-2018
38 (1.8%)
67 (3.2%)
0
0.5
1
1.5
2
2.5
3
3.5
4
0
10
20
30
40
50
60
70
80
90
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Pe
rce
nt
of
case
s
Nu
mb
er
of
Cas
es
Correctional case Percent correctional71
Cases increased most in local jails and others*Type of Correctional Facility, 2017-2018
10
3
11
1412
4
28
22
0
5
10
15
20
25
30
Federal State Local Other*
Nu
mb
er
of
case
s 2017 2018
* Includes ICE detention centers
72

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 37
Low education associated with high TB rateTB rate by % of adults in census tract with HS education
United States, 4.5
China, 3.3
India, 1.4
Mexico, 1.5
Philippines, 1.7
Vietnam, 2.7
0
10
20
30
40
50
60
<72% 72.1-86.4% 86.5-94% >94%
Inci
de
nce
rat
e p
er
10
0,0
00
Percent of adults with HS education
Country, Rate Ratio
73
Lower SES associated with higher TB rate.TB Rate by SES Level and Country of Birth
0
10
20
30
40
50
60
Un
ited
Sta
tes
Me
xico
Ind
ia
Ch
ina
Vie
tnam
Ph
ilip
pin
es
Un
ited
Sta
tes
Me
xico
Ind
ia
Ch
ina
Vie
tnam
Ph
ilip
pin
es
Un
ited
Sta
tes
Me
xico
Ind
ia
Ch
ina
Vie
tnam
Ph
ilip
pin
esInci
den
ce r
ate
per
100
,000
Low SES High SES
74

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 38
2018 CA TB Epi Highlights Summary
Stall in decline confirmedSimilar epi patterns continue: disparitiesHigh TB rate in older age groupsFalling number of peds cases reason for optimismCases in local jails and other facilities bears monitoringTB is associated with lower socioeconomic status!(even in California and after accounting for country of birth)
75
Contacts Care Cascade: EvaluationARPE Data California, 2016‒2017
23,589 19,2040
5,000
10,000
15,000
20,000
25,000
Contactsto Smr +
Evaluated
Nu
mb
er
of
con
tact
s
81%
76NTIP data for California based on ARPE reporting for cohorts reported in 2016 and 2017

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 39
TB prevention cascade amongContacts to infectious TB, California, 2016-2017
3,117 2,125 1,5100
500
1000
1500
2000
2500
3000
3500
With LTBI Started treatment Completedtreatment
Started treatment Completed treatment
68%
71%
77
NTIP data based on ARPE California data, 2016-2017
Contacts with LTBI
Improving treatment completionContacts Completing LTBI Treatment (of those who start)
62% 62% 73% 69% 72% 70%0%
10%
20%
30%
40%
50%
60%
70%
80%
2012 2013 2014 2015 2016 2017
78ARPE data reported to California 2012-2017

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 40
<50% of contacts with LTBI complete treatmentARPE Data California, 2012-2017
12,787 8,022 5,3870
2000
4000
6000
8000
10000
12000
14000
Latent TB infection Started Treatment Completed treatment
63%
42%
79
New legal permanent resident evaluations:B-notification
80

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 41
81
Class B1 arriver care cascade2014-2018
32215
1994562%
711936%
310444% 1574
51%
0
5000
10000
15000
20000
25000
30000
35000
ClassB arrivers
Evaluated& reported
LTBI*
Started Tx Completed Tx
*Excludes B1 arrivers who reported a history of treatment for active TB
Potential room for program improvement?
• Only 42% of contacts with LTBI completed treatment
• Only 22% of B1 arrivers with LTBI completed treatment
82

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 42
TB programs are responsible for at least 2 populations at risk of TB: Contacts and New arrivers with B-notifications
Improved evaluation and treatment to prevent TB
83
Contacts for California TB programs
• CDPH TB Branch 510-620-3865• Program Liaisons
– Lisa True– Stephanie Spencer– Leslie Henry– Anne Cass– Michael Joseph
• Epi Liaisons– Lisa Pascopella– Melissa Ehman– Adam Readhead– Phil Lowenthal– Varsha Hampole
• TB Registry Chief– Janice Westenhouse
• Surveillance and Epidemiology Section Chief
– Pennan Barry
• Program Development Section Chief– Kristen Wendorf
• You can reach me at [email protected]

Tuberculosis epidemiology: using data to inform tuberculosis control approaches and priorities 43
National and California resourcesDivision of Tuberculosis Elimination National Center for HIV/AIDS, Viral Hepatitis,
STD, and TB PreventionCenters for Disease Control and Preventionhttp://www.cdc.gov/tb/
• National data slidesethttps://www.cdc.gov/tb/statistics/surv/surv2018/default.htm
• Core curriculum on TB https://www.cdc.gov/tb/publications/slidesets/corecurr/default.htm
Tuberculosis Control Branch
Division of Communicable Disease Control
Center for Infectious Diseases
California Department of Public Health• https://www.cdph.ca.gov/Programs/CID/DCDC
/Pages/TBCB.aspx
• https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/TBCB-Program-Liaison-Epi-Assignments.pdf
• https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/TBCB-RVCT-Death-Algorithm-v1.0.pdf
Acknowledgements
CDC DTBE slidesetCDPH TBCB:• Pennan Barry• Phil Lowenthal• Melissa Ehman