Epidemiology of tuberculosis Prof. L.A. Hryshchuk.
60
Epidemiology of tuberculosis Prof. L.A. Hryshchuk
-
Upload
margaretmargaret-blair -
Category
Documents
-
view
220 -
download
0
Transcript of Epidemiology of tuberculosis Prof. L.A. Hryshchuk.

Epidemiology of tuberculosis
Prof. L.A. Hryshchuk

The World Health Organization (WHO) The World Health Organization (WHO) proclaimed tuberculosis to be the global danger. proclaimed tuberculosis to be the global danger. According to its forecasts there will be 90 million new According to its forecasts there will be 90 million new tuberulosis cases in the world during the decade. Of tuberulosis cases in the world during the decade. Of those who will fall ill approximately 30 million people those who will fall ill approximately 30 million people may die in the current decade unless the reaction to may die in the current decade unless the reaction to this global problem radicallythis global problem radically improves.improves.
Nowadays the world scientists distinguish threeunion Nowadays the world scientists distinguish threeunion tuberculosis epidemic: the first is the epidemic of tuberculosis epidemic: the first is the epidemic of typical tuberculosis that is treated well; the second is typical tuberculosis that is treated well; the second is the epidemic of chemioresistant tuberculosis and the the epidemic of chemioresistant tuberculosis and the third one is the epidemic of tuberculosis and the AIDS.third one is the epidemic of tuberculosis and the AIDS.

Source: Global TB control report, 2011
Incidence
TB/HIV incidence
Rat
e p
er 1
00
.00
0 p
op
ula
tio
n/y
ea
rPrevalence
MDG target for prevalence
Rat
e p
er 1
00
.00
0 p
op
ula
tio
n/y
ea
rR
ate
per
10
0.0
00
po
pu
lati
on
/ye
ar Mortality
MDG target for mortality
TB/HIV incidence, ,
Europe,1990-2010Europe,1990-2010
3

The incidence of TB has slowly declined during the past years, reaching 48 (confidence intervals 44-50) per 100 000 population in 2009.
However there is a big discrepancy between east and west.
The TB prevalence decreased from 96 (confidence intervals 70-130) to 63 (confidence intervals 49-81) per 100 000 population between 1990 and 2009 against a target of below the prevalence of 48 set out in the target for 2015.
Mortality from TB must further decline, from 6.9 (confidence intervals 5.7-8.3) per 100 000 persons in 2009 to 6 by 2015.

TB incidence

TB/HIV incidence, 2010, 2010
6

We will start with the patient since they are typically the source of infection. This slide shows a violent sneeze caught on film by high speed photography showing large liquid droplets.
Most of these large, visible droplets will fall to the ground. However, the small droplet nuclei that can reach the deep lung are not visible and are 1:5 micro meters in size.

According to the WHO criteria from 1995 tuberculosis epidemic has been registered in Ukraine in so far as tuberculosis patients comprise over 1 % of the total number of the population.
The statistics of sickness in all the forms of tuberculosis in 2009 was 72,7 persons per 100 thousand of the population.
Alarming is the fact that tuberculosis “has turned younger”, its number among children, able-bodied and reproductive ages increases.

THE WORLD TUBERCULOSIS EPIDEMIOLOGICAL SITUATION
More than 2 billion people (about one-third of the world
population) are estimated to be infected with tuberculosis . The global incidence of TB peaked around 2003 and now appears to be declining slowly . In 2006 the World Health Organization (WHO) issued the following estimates :
The prevalence of active infection was 14.4 million, corresponding to a prevalence rate of 219/100,000 persons.
The incidence of new cases was estimated to be 9.2 million, corresponding to an incidence rate of 139/100,000.
Twelve of the 15 countries with the highest estimated TB incidence are in Africa, where the TB incidence rate was 363/100,000 .
In 2006 there were 1.7 million deaths from TB worldwide, a death rate of 25/100,000.

Every year 7-10 million people fall ill with tuberculosis all over the world, including 4-4,5 mln. – with bacterial secretion and about 3 mln. adults die of it (of these 97 % – in the developing countries) and approximately 300 thousand children. The total number of tuberculosis patients reaches 50-60 mln.Nowadays tuberculosis is the most menacing illness for the whole mankind. It kills more patients worldwide than all the infectious and parasitic illnesses taken together. Present tuberculosis epidemic has acquired the global scales. In many parts of the world tuberculosis epidemic is beyond the control.

The highest tuberculosis statistics of sickness is noted in African and Asian regions, in the countries of the Pacific Ocean coast. Tuberculosis epidemic situation got worse in the countries of Europe too, especially in the countries of the former Socialist community.
In 2009 the lowest tuberculosis index was registered in the highly developed countries, such as Malta (4,2), Sweden (5), Norway (5,5), Iceland (6,2), Italy (8,4 per 100000 of the population), the highest – in Romania (114,6), in the former Soviet Union, as in Kirgistan (127,8), Kazakhstan (126,4), Georgia (124,4), Turkmenistan (86,1 per 100.000 of the population) (fig.3).


Morbility on tuberculosisMorbility on tuberculosis and HIV and HIV in Ukraine in Ukraine The statistics of morbidity in all forms of tuberculosis in
Ukraine from 1990 to 2012 increased from 32 to 68,1 per 100 thousand population/
0
20
40
60
80
100
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2012
ВІЛ Туберкульоз

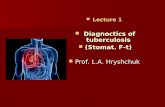
EtiologyEtiology M. tuberculosisM. bovisM. africanum

Basic TB FactsBasic TB FactsTuberculosis (TB) is a contagious, air-borne
disease caused by a mycobacterial infection.It primarily affects the lungs but can also
affect any other part of the body.It is spread through the air when someone
with active TB disease coughs, sneezes, etc.TB is a curable disease, with effective, low-
cost treatment available worldwide.

TB Infection TB Infection vs TB Diseasevs TB Disease
TB infection – organism is present, but dormant, cannot infect others
TB disease (active TB) – person is sick and can transmit disease to others if TB is in lungs
Active disease:•cough > 3 weeks •+/- blood in sputum•decreased appetite•weight loss•weakness•night sweats
Atypical presentation: in HIV-infected

Basic TB FactsBasic TB Facts Approximately one-third of the world's population is
latently infected with Mycobacterium tuberculosis
– 10% lifetime risk of active disease (from birth)
Each year, approximately 9 million persons become ill from TB
– 1.7 million die
– 709,000 of them are people living with HIV/AIDS
TB disproportionately affects the poor

Epidemiology of TBEpidemiology of TBin the worldin the world

Global EstimatesClassificati
onEstimated Number
of CasesEstimated Number of
Deaths
All forms TB
9.2 million 1.7 million
MDR TB 500,000 110,000 +
XDR TB 40,000 ?

22 Countries Account for 80% of the Global TB Burden

Estimated new TB cases (all forms) per 100 000 population
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2006. All rights reserved
No estimate
0-24
50-99
300 or more
25-49
100-299
Highest TB rates per capita: Highest TB rates per capita: AfricaAfrica

Threats & OpportunitiesThreats & Opportunities

Threat: TB in PrisonsThreat: TB in Prisons
Breeding ground for the spread of TB– Enclosed spaces – Overcrowded conditions – Lack of adequate ventilation systems – Prison Community
Rates of TB are often higher in the penitentiary system compared to the civilian population in many E&E countries (ex. Russia 20 times higher).

Threat: TB and HIVThreat: TB and HIV
Greater chance of progression to TB disease if HIV-infected (10%/year)
More rapid progression– from 2 years to weeks/months
Higher mortality (15%-50%)
– Higher with MDR TB (75%-100%)
TB is most common OI and most common cause of death among HIV-infected persons

Estimated HIV prevalence in Estimated HIV prevalence in new TB cases, 2006new TB cases, 2006
No estimate
0–4
20–49
50 or more
5–19
HIV prevalence in TB cases, (%)
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2006. All rights reserved

0
100
200
300
400
500
600
700
800
2002(9, 37%) 2003(92, 53%) 2004(84, 61%) 2005(118, 83%) 2006(112, 90%)
Th
ou
san
ds
HIV testing for TB patients all countries, 2006
2
4
6
8
10
12
14
0.5%
4%3.2%
8.5%
12%

Outbreak

Drug Resistant TBDrug Resistant TB Multi-drug resistant TB (MDR TB)
• TB patient’s M. tuberculosis isolate is resistant to at least Isoniazid and Rifampicin
XDR-TB (Extensively Drug Resistant TB)– MDR-TB, plus resistant to – Any fluoroquinolones (Ciprofloxacin, Ofloxacin,
Moxifloxacin, Gatifloxacin, and – One of the injectables (Amikacin, Capreomycin,
Kanamycin) Treatment longer, more costly, more difficult to treat
– More side effects

XDR-TB and HIV/AIDS: XDR-TB and HIV/AIDS: A Lethal CombinationA Lethal Combination
Immune compromised people more vulnerable to TB Diagnosis is more difficult in HIV positive people
– Smear negative; Extra-pulmonary Treatment is challenging
– Drug interactions – Intolerance and adherence
Protecting health care workers (HCWs) is important– Special risk for HIV+ HCWs
Increased burden on health care system– need for hospitalization, heavier workload, stricter
infection control Fear and stigma
– Alarmist messages increase stigma– Negative impact on health seeking behaviourSource WHO/CDC

XDR TB Confirmed in 45 XDR TB Confirmed in 45 CountriesCountries
Source: WHO Anti-TB Drug Resistance in the World Report 4, 2008
Countries reporting XDR TB as of Feb 2008

27 MDR TB High Priority Countries27 MDR TB High Priority Countries
Country
% of all TB cases with MDR-TB
Number of MDR-TB
cases
China 8.3 130,548
India 4.9 110,132
Russian Federation 19 36,037
Pakistan 5 15,233
Bangladesh 4 14,583
South Africa 2.6 14,034
Ukraine 22 13,429
Indonesia 2.2 12,142

Global ResponseGlobal Response

Global Stop TB Strategy

Number of countries implementing Number of countries implementing DOTS (out of a total of 212 countries), DOTS (out of a total of 212 countries),
1991-20061991-2006
0
20
40
60
80
100
120
140
160
180
200
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Nu
mb
er
of
co
un
trie
s
184

The Global Plan to Stop TB The Global Plan to Stop TB 2006-2015: Actions for Life2006-2015: Actions for Life
Millennium development goal: to have halted and begun to reverse the incidence of TB by 2015
Stop TB partnership goal to reduce by 50%, relative to 1990 levels, disease prevalence and deaths from TB by 2015
Case detection: at least 70% of people with infectious TB will be diagnosed
Treatment success: at least 85% of those diagnosed will be successfully treated

The Global Plan to Stop TBThe Global Plan to Stop TB2006-20152006-2015
- Achieve the Millennium Development Goal to have halted and begun to reverse the incidence of TB by 2015- Save an additional 14 million lives
- Treat 50 million people for TB
- Expand access to high-quality TB diagnosis and treatment for all
- Put 3 million TB patients co-infected with HIV on ARVs
-Treat 800,000 people for MDR-TB – [to be adjusted for XDR]
- Produce the first new anti-TB drug in 40 years by 2010
- Develop a new vaccine by 2015
- Provide rapid and inexpensive diagnostic tests at the point of care
Expected Results

Global MDR TB & XDR TB Response Plan
“Main activities to be conducted at global, regional and country levels in 2007 in 2008 to operationalize the anti-drug resistance component of the Global Plan.”
“Marks the beginning of the integration of MDR TB and XDR TB activity thing to general TB control activities”

Global Response: Priority Activities for MDR Global Response: Priority Activities for MDR and XDR-TBand XDR-TB
Strengthen basic TB and HIV/AIDS control Scale-up programmatic management of MDR/XDR-TB Strengthen lab services for diagnosis Expand MDR/XDR TB surveillance Strengthen infection control measures to avoid
transmission Increase advocacy, communication and social
mobilization Mobilize resources at all levels Promote research and development-new diagnostics,
drugs and vaccines

The Global Fund to Fight AIDS, The Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM)Tuberculosis and Malaria (GFATM)

Engaging GFATMEngaging GFATM
At country level, missions on CCMsBilateral program complements GFATMWorking relationship with portfolio managerIdentify issues and get support for addressing
problemsAssistance to countries to prepare proposalsUSG GFATM $$ programmed for TA grants

USAID ResponseUSAID Response

USAID’s Goal and ObjectiveUSAID’s Goal and ObjectiveGoal: By 2015, to reduce by
50% the number of deaths due to TB in 19 USAID focus countries.
Objective: To detect at least 70% of estimated TB cases and successfully treat at least 85% of those cases in USAID focus countries by 2011.

USAID’s TB Program USAID’s TB Program PrioritiesPriorities
Scale up the STOP TB Strategy Improve quality of basic DOTS to slow
the emergence of drug resistance Implement recommendations outlined
in Global MDR-TB and XDR-TB Response plan
Develop/disseminate new tools and approaches
– Drugs, diagnostics and operations research – Introduction into country programs
Address special challenges – TB-HIV/AIDS co-infection

USAID’s TB Program ApproachUSAID’s TB Program Approach Focus on country level Concentrate resources in highest
burden countries Support NTP strategic plans Ensure success of GFATM grants Leverage PEPFAR Standardized indicators to measure
outcome Invest in the future – new tools Expand partnerships Global and technical leadership –
active in STOP TB Partnership board and technical working groups

USAID TB program USAID TB program relationship to PEPFARrelationship to PEPFAR
Globally Coordination and implementation of technical
assistance for Global Fund TB grants. Includes preparation of grant proposals and TA to approved
grants Partners include: Green Light Committee, Stop TB
Partnership, and TBCAP Management of mechanisms which receive PEPFAR
funding for TB/HIV (TBCAP, TB Task Order 2/PATH).
Support for global norms/guidelines (TB/HIV, infection control).
Operations research related to TB/HIV (IPT, Barriers to HIV testing of TB patients).

TB Funding Trends 1998 – TB Funding Trends 1998 – 20082008
* Excludes Global Fund
0$10
$15 $22
$56
$78 $74 $84
$93$91
$92
$162
0
20
40
60
80
100
120
140
160
180
Fu
nd
i ng
Level ( M
illion
s
US
$)

TB Funding by Regional Bureau
E&E12%
ANE*27%
AFR27%
GH19%
GDF9%
LAC6%
$30.1M
$9.2M
$19.9M $43.9M
$44.1M
$14.9M
FY 2008 Total = $162 million
Source: USAID CBJ 2008*Includes $7.4M for Central Asian Republics

Selection Criteria for Selection Criteria for
Country ProgramsCountry Programs Countries of greatest need as defined by:
– Greatest burden of TB– High incidence of TB (cases notification rates over
100/100,000) – High HIV/AIDS prevalence – Prevalence or potential for drug resistance (MDR-TB
or XDR-TB)*– Lagging case detection and treatment success rates*
Technical & managerial feasibility Political commitment

USAID Priority TB USAID Priority TB Countries Countries
Category Countries
Focus (20) Afghanistan, Bangladesh, Brazil, Cambodia, Democratic Republic of Congo, Ethiopia, India, Indonesia, Kenya, Mozambique, Nigeria, Pakistan, The Philippines, Russia, South Africa, Tanzania, Uganda, Ukraine, Zambia, Zimbabwe
Non Focus (19)
Angola, Bolivia, Dominican Republic, Georgia, Ghana, Haiti, Honduras, Kazakhstan, Kyrgyzstan, Malawi, Mexico, Moldova, Namibia, Peru, Senegal, Southern Sudan, Tajikistan, Turkmenistan, Uzbekistan
Red = High Burden Country

USAID TB USAID TB PartnersPartners
National TB Programs Local partners and NGOs Stop TB Partnership GDF WHO CDC TB CAP/TBCTA
(KNCV, IUATLD, WHO, ATS, MSH, FHI JATA, CDC)
Gorgas (JHU and UAB) IUATLD

Best PracticesBest PracticesLink to 5-year plans of National TB Program (NTP)
Sprinkling should be avoided
STOP TB Strategy should guide USAID support
Collaboration/leveraging – with other partners (WB, WHO, CDC, GFATM, GDF, etc.)
M and E – Programs should undertake external M and E every one to two years

Key Documents and Web SitesKey Documents and Web Sites Key Documents: Stop TB Strategy The Global Tuberculosis Control Report 2006 The Global Plan to STOP TB 2006 - 2015 International Standards for Tuberculosis Care The Patients Charter for Tuberculosis Care www.stoptb.org/resource_center/documents.aspWeb Sites: WHO TB Publications www.who.int/gtb/whats-new/new_publications.htm USAID Tuberculosis Home Page
www.usaid.gov/our_work/global_health/id/tuberculosis/index.html IUATLD www.iuatld.org CDC www.cdc.gov/nchstp/od/nchstp.html Global Fund www.theglobalfund.org GDF www.stoptb.org/gdf/ JHU www.hopkins-tb.org TASC 2 www.tasc2.org TBCTA www.tbcta.org/

Where to go for more information on Where to go for more information on TuberculosisTuberculosis
World Health Organization
Geneva, Switzerlandwww.stoptb.org

ORGANIZATION OF ANTITUBERCULOUS ORGANIZATION OF ANTITUBERCULOUS ACTIVITY IN THE PERIOD OF ACTIVITY IN THE PERIOD OF
TUBERCULOSIS EPIDEMYTUBERCULOSIS EPIDEMY Tuberculosis is a social disease and is a mirror of social-economic
prosperity of the state and the well-being of its people, therefore antituberculous measures under present conditions must be taken on the national level by the government of the country.
At present time, the principal task in fighting tuberculosis in Ukraine is to take the epidemy of the illness under control (I stage), to stabilize the epidemiological indices (infestation, morbidity, sickliness and death rate) of tuberculosis (2 stage), and then their gradual decrease (3 stage).
For the successful organization of antituberculous measures close cooperation of the medical system, sanitary-epidemiological service and the organs of the state power is necessary. The general organization and methodological guidance of antituberculosis activity in this country is realized by the Ministry of Health Protection of Ukraine and Acad. F.G.Yanovsky Ukrainian phthisiology and pulmonology research institute (scheme 1).

STRUCTURE OF ANTITUBERCULOSIS SERVICESTRUCTURE OF ANTITUBERCULOSIS SERVICEIN UKRAINIANIN UKRAINIAN
The Ministry of Health Protection Acad. F.G.Yanovsky Ukrainian phthisiology and
pulmonology research institute Regional of antituberculous dispensary Distric(town) of antituberculous dispensaries Tubcabinet At child’s policlinic At policlinic At medical parts

Antituberculous dispensary (Engl. dispensation – distribution) is a specialized medicative-prophylactic institution, which work is aimed at lowering morbidity, sikliness, infestation with tuberculosis and death rate caused by it as well as at conducting a complex of organizational and methodical, prophylactic antituberculous measures among the district population.
The main tasks of an antituberculous dispensary are: 1) prophylaxis; 2) early revealing; 3) treatment of tuberculosis patients; 4) registration of groups of tuberculosis patients and
contingents of persons

Other very important tasks of an antituberculous dispensary are revealing, registration and treating tuberculosis patients. The results of treating tuberculosis patients to a considerable degree depend on the disease being timely revealed. In this connection, firsty diagnozed tuberculosis patients are divided into three groups: timely, untimely and lately revealed. For children and teenagers the fourth group is separated – early revealing.
The main criteria of dividing patients into groups are the character of a specific process, the presence or absence of destruction (cavern) and bacterial excretion, peculiarities of the prognosis at treatment, the degree of a patient’s danger for healthy persons.

Children and teenagers, in whom the following factors are diagnosed, compose a group of early revealed:
1) tuberculin test range;2) primary tubinfestation;3) hyperergic Mantoux test;4) tuberculous intoxication.

DISPENSARY DISPENSARY CATEGORYCATEGORY Contingents of antitubercular dispensaries are
divided into categories, which enables to examine them differentially, define the treatment tactics, perform prophylactic and rehabilitation actions.
Contingents of adult persons, children and teenagers due to being observed at an antitubercular dispensary, are divided into 5 dispensary categories: 1, 2, 3, 4 and 5.
To 5 categories (Cat 5) are referred dispensary contingents of risk to disease to a tuberculosis and its relapse.

Thank You!Thank You!