TREATMENT OF VTE IN DIFFERENT PATIENT PROFILES 1- Treatment VTE different patient profiles... ·...
50
TREATMENT OF VTE IN DIFFERENT PATIENT PROFILES David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
Transcript of TREATMENT OF VTE IN DIFFERENT PATIENT PROFILES 1- Treatment VTE different patient profiles... ·...

TREATMENT OF VTE IN
DIFFERENT PATIENT PROFILES
David Jiménez, MD, PhD, FCCP
Ramón y Cajal Hospital, IRYCIS
Madrid, Spain

TREATMENT OF VTE IN DIFFERENT PATIENT PROFILES
David Jiménez, MD, PhD, FCCP
Ramón y Cajal Hospital, IRYCIS
Madrid, Spain

• Advisory board : Bayer HealthCare Pharmaceuticals; Boehringer
Ingelheim Pharmaceuticals; Bristol-Myers Squibb; Leo Pharma; ROVI;
Sanofi
• Lectures : Bayer HealthCare Pharmaceuticals; Boehringer Ingelheim
Pharmaceuticals; Bristol-Myers Squibb; Daiichi Sankyo; Leo Pharma;
ROVI; Sanofi
• Research funding : Sanofi; ROVI
Potential conflicts of interest



Cohen AT. Thromb Haemost 2007
Annual incidence of VTE

VTE incidence

PE is frequent in hospitalized patients

Fanikos J, Am J Med 2013
PE expenses

Case-fatality rate of PE

Cohen AT. Thromb Haemost 2007
Mortality from VTE

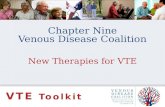
Annual burden of VTE in the US

100.000
200.000
300.000
400.000
500.000
600.000 543.000
87.000 64.000 53.0005.800
VTE Breastcancer
Prostatecancer
Caraccidents AIDS
Dea
ths
per
year
Cohen AT. Thromb Haemost 2007
VTE burden

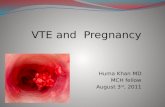
47 EMERGENCY EMBOLECTOMIES
J Thorac Cardiovasc Surg 2005;129:1018 Courtesy, Samuel Z. Goldhaber


UpToDate 2006

Prophylaxis
Diagnosis
Treatment
Asymptomatic DVT
Death
PE
Post-thrombotic syndrome
Symptomatic DVT
Pulmonary hypertension
With the aim to reduce the burden of VTE

Patient
66-year-old female with acute PE
No comorbidities
HR 90/min SBP 120 mm Hg Saturation 93%
Would you treat this patient on an outpatient basis?

1. Yes
2. First, I would order a BNP testing
3. First, I would order an echocardiogram
4. First, I would order a troponin testing
Would you treat this patient on an
outpatient basis?

Pulmonary Embolism Severity Index
Aujesky D, AJRCCM 2005

OTPE trial
Outpatient
(n=171)
Inpatient
(n=168)
P*
N (%)
Recurrent VTE 1 (0.6) 0 0.011
Major bleeding
14 days 2 (1.2) 0 0.031
90 days 3 (1.8) 0 0.086
Overall
mortality
1 (0.6) 1 (0.6) 0.005
*Non-inferiority margin = 4% Aujesky D, Lancet 2011

OTPE trial
Outpatient
(n=171)
Inpatient
(n=168)
P
Length of hospital stay, days 0.5 3.9 <0.001
Readmissions, n 18 23 0.60
Emergency department visits, n 36 36 0.94
Primary-care doctor visits, n 202 216 0.67
Home nursing visits, n 348 105 0.53
Aujesky D, Lancet 2011

Simplified PESI
Jiménez D. Arch Intern Med 2010
Age > 80 1 point
Cancer 1 point
Cardiopulmonary disease 1 point
HB > 110/min 1 point
SBP < 100 mm Hg 1 point
O2 saturation < 90% 1 point
995 patients from a single centre

sPESI: validation
369 patients from 18 hospitals
(SWIVTER)
30-day all-cause mortality:
4.3%
Low-risk: 28.7%
Negative predictive value:
100% Spirk D, Thromb Haemost 2011

1. LMWH
2. UFH
3. Warfarin
4. Lytics
How would you treat this patient?

Narrow therapeutic window

Baker. J Manag Care Pharm 2009
Time in therapeutic range

Van Bladel ER. Thromb Res 2010
Outpatient therapy and OAC
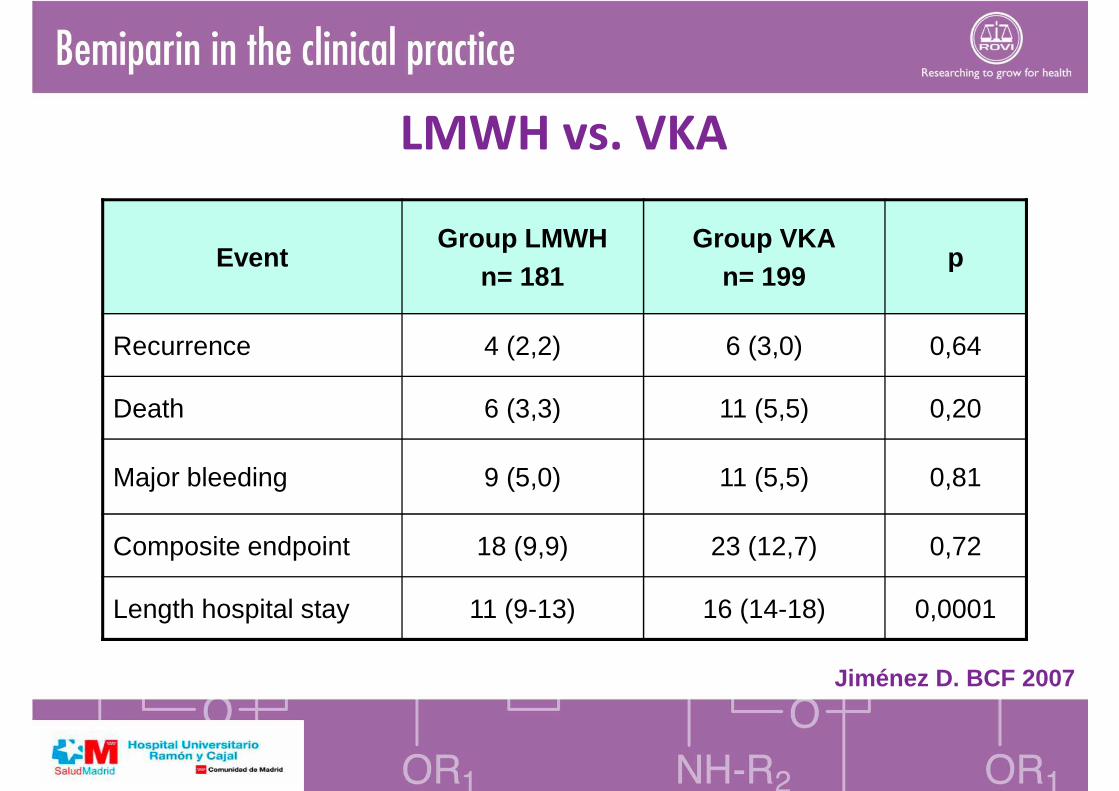
LMWH vs. VKA
Jiménez D. BCF 2007
EventGroup LMWH
n= 181Group VKA
n= 199p
Recurrence 4 (2,2) 6 (3,0) 0,64
Death 6 (3,3) 11 (5,5) 0,20
Major bleeding 9 (5,0) 11 (5,5) 0,81
Composite endpoint 18 (9,9) 23 (12,7) 0,72
Length hospital stay 11 (9-13) 16 (14-18) 0,0001

Kearon C. Chest 2012
Once vs. twice daily regimen

Initial treatment with bemiparin
Kakkar VV. Thromb Haemost 2003
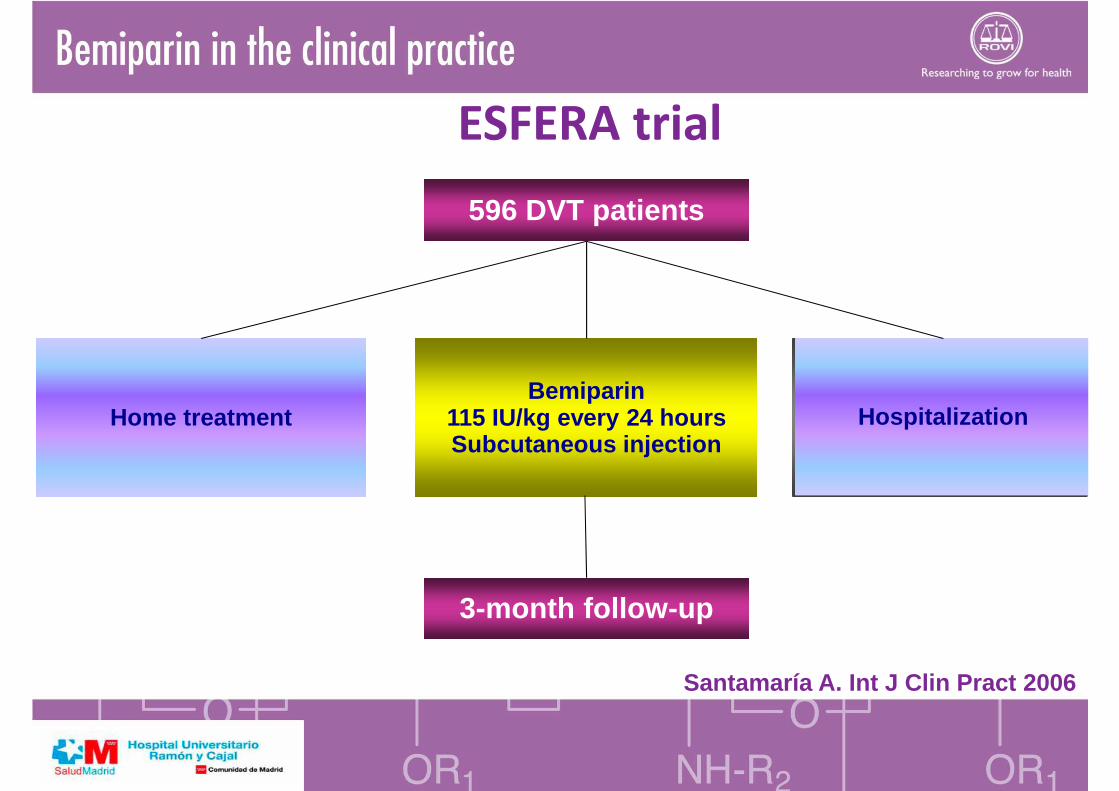
Bemiparin115 IU/kg every 24 hoursSubcutaneous injection
Hospitalizado
596 DVT patients
3-month follow-up
Home treatment Hospitalization
ESFERA trial
Santamaría A. Int J Clin Pract 2006

Home treatment
N = 434
Hospitalization
N = 149
P
PE 0 (0) 0.7 (1) 0.256
Recurrent VTE 0.5 (2) 0 (0) 0.554
Major bleeding 1.4 (6) 0 (0) 0.169
Death 1.2 (5) 0 (0) 0.227
Adverse events 5.1 (22) 7.4 (11) 0.196
Santamaría A. Int J Clin Pract 2006
ESFERA trial

Patient
66-year-old male with gastric cancer
Sudden onset of dyspnea
HR 115/min SBP 110 mm Hg Saturation 90%
Objective diagnosis of PE
How would you treat this patient?


1. VKA
2. LMWH
3. Rivaroxaban
4. Apixaban
How would you treat this patient?

Khorana A, J Clin Oncol 2009
Treatment in patients with cancer

Khorana A, J Clin Oncol 2009
Treatment in patients with cancer

Lee A, N Engl J Med 2003
Treatment in patients with cancer

Meyer G, Arch Intern Med 2002
Treatment in patients with cancer

ESFERA trial
601 patients with DVT w/wo PE
HOSPITALIZATION
OUTPATIENTREGIMEN
TREATMENT
BASELINE(month 0)
INTERMEDIATE (day 7 + 2)
FINAL (month 3)
FOLLOW-UP
• Combined incidence of DVT + PE + death at 3 months
• Major bleeding• Health
outcome measures
Bemiparin(5,000/7,500/
10,000 IU/day SC)
Santamaria A, Int J Clin Pract 2006

ESFERA trial
0.0471.7%0.4%Major bleeding
n.s.0%0%Recurrent DVT
n.s.0%0.4%Deaths related to VTE/bleeding
0.0482.6%0.4%Thrombocytopenia
n.s.0%0%PE
0.0326.0%1.8%Minor bleeding
P-valueBEMI/VKA
n = 116BEMI/BEMI
n = 279
Venous thromboembolism and bleeding depending on the drugadministered during secondary prevention (Days 1-98)
Santamaria A, Int J Clin Pract 2006
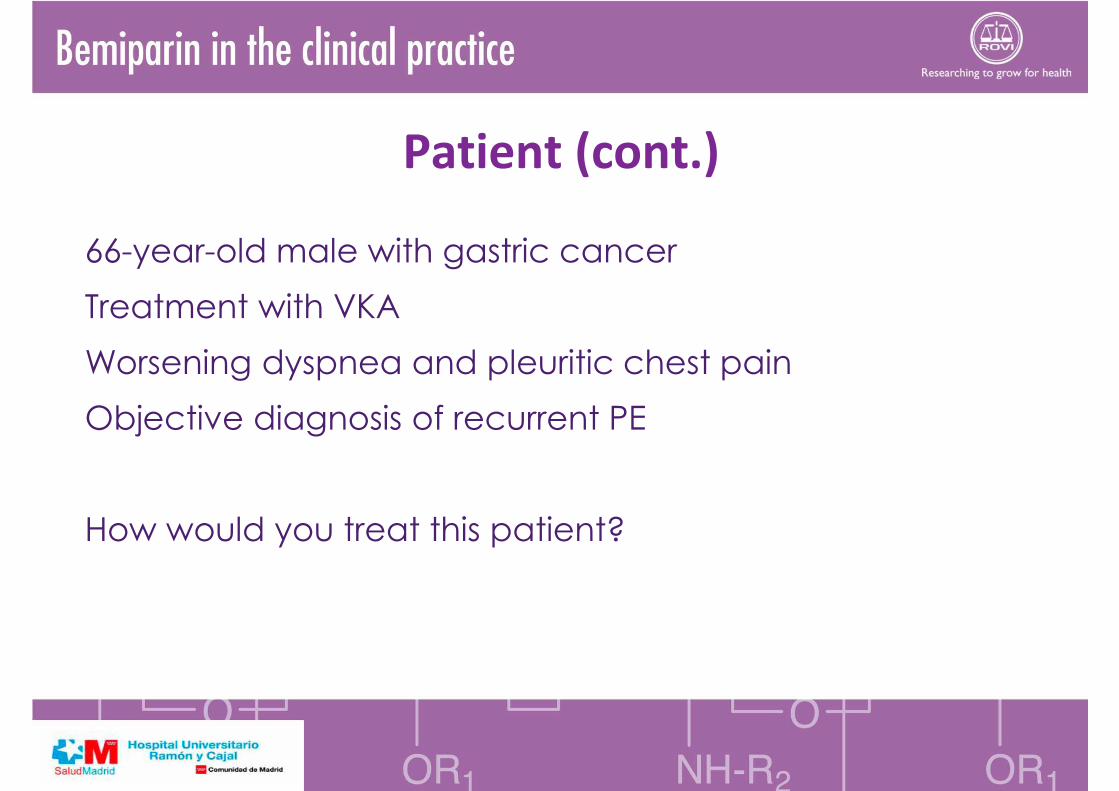
Patient (cont.)
66-year-old male with gastric cancer
Treatment with VKA
Worsening dyspnea and pleuritic chest pain
Objective diagnosis of recurrent PE
How would you treat this patient?

9% with LMWH
20% with VKA
Metastasis, younger age, short interval between VTE and cancer diagnosis (< 3 months)
Trujillo-Santos J, J Thromb Haemost 2008
Recurrent VTE on anticoagulation

PREPIC, Circulation 2005
Inferior vena cava filters

Hull RD, Am J Med 2006
Switch to LMWH

Retrospective study
70 patients with cancer and recurrent VTE while on LMWH or VKA
VKA: Switch to LMWH, LMWH: dose escalation
67% LMWH; 33% VKA
Carrier M, J Thromb Haemost 2009
Dose escalation

Patient
46-year-old female
Renal cell carcinoma
Staging CT scan: segmental PE
Should we treat this asymptomatic incidental thrombosis?

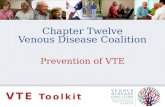
Incidental PE
UPE location 6-month survival Overall survival
HR (95% CI) P-value HR (95% CI) P-value
None1
(reference)
1
(reference)
Any1.97
(1.09-3.58)0.025
1.51
(1.01-2.27)0.048
Proximal2.28
(1.20-4.33)0.011
1.70
(1.06-2.74)0.027
Subsegmental0.80
(0.16-3.97)0.78
1.04
(0.44-2.39)0.92
O’Connell C, J Thromb Haemost 2011UPE, unsuspected PE

Incidental PE
Multivariate survival analysis revealed:
Overall HR 1.51 for UPE vs. matched controls (p=0.048)
HR 2.28 for proximal UPE at 6 months (p=0.01)
No significant impact of incidental ISSPE on survival
Results remained significant when:
Patients who did not receive anticoagulation (n=7 with proximal UPE)
were excluded
Controls with age outside of the 5-year restriction were excluded
Survival measured from date of malignancy diagnosis
O’Connell C, J Thromb Haemost 2011UPE, unsuspected PEISSPE, isolated subsegmental PE