
Treatment of urethral stricture disease by internal urethrotomy ...
4
136 Journal of the Royal Society of Medicine Volume 81 March 1988 Treatment of urethral stricture disease by internal urethrotomy followed by intermittent 'low-friction' self-catheterization: preliminary communication W T Lawrence FRCS R P MacDonagh MvB Urology Department, City Hospital, Nottingham Keywords: urethral stricture, urethrotomy, self-catheterization Summary The aim of this study was to determine whether the natural course of urethral stricture disease could be modified following urethrotomy by teaching patients intermittent self-catheterization. Preliminary results in 42 patients show that postoperative urine flow rates can be maintained if this method of 'low-friction' catheterization is adopted. The technique has been well received by an elderly group of patients and can be recommended for wider use. Introduction The treatment of urethral stricture disease is one of the oldest problems facing the urological surgeon and the earliest records of medicine are concerned with the management of strictures by means of catheters and sounds. Treatment by regular bouginage has been advocated for many years and, despite the vogue for blind urethrotomy during the 18th and 19th centuries, dilatation has remained the standard for comparison. In 1964 Helmsteinl advocated the use of urethroscopy before and after blind urethrotomy to enable the stricture to be accurately localized and checked for a satisfactory incision. However, during the last 10 years internal urethrotomy under direct vision, popularized by Sachse in 19742, has become the mainstay of treatment in many urological departments, while urethroplasty operations have often been reserved for complex strictures or for those cases where other simpler methods have failed. The objective using precision endoscopic surgery compared with traditional dilation has been to keep trauma to a Organizing granulation tissue 1, I contracted scar nature scar staying wide open / na! (1!) Splinting catheter 0141-0768/88/ 030136-04/$02.00/0 1988 The Royal Society of Medicine Figure 1. Cutting the stricture leaves a gap; the kernel of the problem in internal urethrotomy is how to stop the scar from shrinking. A splinting catheter may keep it widely open until the scar tissue is mature. (Reproduced from Blandy3, with kind permission) minimum, but the essential problem of how to stop the raw edges from sticking together again and how to stop the scar from shrinking still remains3 (Figure 1). Some surgeons have left catheters of different materials in the urethra for more or less prolonged periods of time4-7, some have instilled steroids in the hope of preventing fibrosis4'8, while others have used a regimen of autodilatation, instructing the patient to void against resistance formed by pinching his urethra at the tip9. We have used a different technique, teaching patients intermittent self-catheterization using a disposable Lofric catheter with a surface coating of hydrophilic polymer, polyvinylpyrrolidone (PVP), to enable easy lubrication when dipped in water and so reduce friction on the urethral mucosa10. Patients and methods Since November 1985, over 85 patients have been started on intermittent low friction self-catheterization (ILSC) following optical urethrotomy, in the hope of preventing or modifying restenosis of the urethra. The first 42 patients had the longest follow up period and are reported here. The majority (n=37) were under urological review for many years and had many urethral dilatations and multiple urethrotomies for recurrent stricture disease (recurrent stricture group). A small number (n=5) presented with a stricture for the first time (new stricture group). The age range of all 42 patients was 23-82 years (mean 62 years) compared with 23-58 years (mean 43 years) for the 5 patients in the new stricture group. The diagnosis of a recurrent or new stricture was confi'rmed by urethroscopic evaluation under general anaesthetic. The sites involved were the penile or bulbar urethra, and several had narrowing in more than one segment. In all cases the procedure suggested in 1974 by Sachse2, and more recently recorded by Smith et al.5 and Gaches et al.4, using the Storz urethrotome was adopted. In those cases where urethral narrowing was severe, after visualizing the face of the stricture, the channel was canulated by passing a small retrograde ureteric catheter (without stylet) down the instrument and through the stricture. Incision into the strictured urethra was confined to the 12 o'clock position, with the cutting blade extended and moving the whole instrument in an upward and outward direction. The length of the incision extended from normal urethra proximally to normal urethra distally and included the full thickness of the strictured segment. Bleeding points were occasionally diathermized using an electrode down the operating port of the urethrotome. Paper read to Section of Urology, 27 November 1986 a.I.
Transcript of Treatment of urethral stricture disease by internal urethrotomy ...

136 Journal of the Royal Society of Medicine Volume 81 March 1988
Treatment of urethral stricture disease by internal urethrotomyfollowed by intermittent 'low-friction' self-catheterization:preliminary communication
W T Lawrence FRCS R P MacDonagh MvB Urology Department, City Hospital, Nottingham
Keywords: urethral stricture, urethrotomy, self-catheterization
SummaryThe aim of this study was to determine whether thenatural course of urethral stricture disease could bemodified following urethrotomy by teaching patientsintermittent self-catheterization. Preliminary resultsin 42 patients show that postoperative urine flowrates can be maintained if this method of 'low-friction'catheterization is adopted. The technique has beenwell received by an elderly group ofpatients and canbe recommended for wider use.
IntroductionThe treatment of urethral stricture disease is one ofthe oldest problems facing the urological surgeon andthe earliest records of medicine are concerned withthe management of strictures by means of cathetersand sounds. Treatment by regular bouginage has beenadvocated for many years and, despite the vogue forblind urethrotomy during the 18th and 19th centuries,dilatation has remained the standard for comparison.In 1964 Helmsteinl advocated the use of urethroscopybefore and after blind urethrotomy to enable thestricture to be accurately localized and checked fora satisfactory incision. However, during the last 10years internal urethrotomy under direct vision,popularized by Sachse in 19742, has become themainstay oftreatment in many urological departments,while urethroplasty operations have often beenreserved for complex strictures or for those caseswhere other simpler methods have failed. The objectiveusing precision endoscopic surgery compared withtraditional dilation has been to keep trauma to a
Organizinggranulation tissue
1, I
contractedscar
nature scar stayingwide open
/ na!
(1!)Splinting catheter
0141-0768/88/030136-04/$02.00/0
1988The RoyalSociety ofMedicine
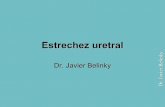
Figure 1. Cutting the stricture leaves a gap; the kernel oftheproblem in internal urethrotomy is how to stop the scar fromshrinking. A splinting catheter may keep it widely open untilthe scar tissue is mature. (Reproduced from Blandy3, withkind permission)
minimum, but the essential problem of how to stopthe raw edges from sticking together again and how tostop the scar from shrinking still remains3 (Figure 1).Some surgeons have left catheters of different
materials in the urethra for more or less prolongedperiods of time4-7, some have instilled steroids in thehope of preventing fibrosis4'8, while others have useda regimen of autodilatation, instructing the patient tovoid against resistance formed by pinching his urethraat the tip9. We have used a different technique,teaching patients intermittent self-catheterizationusing a disposable Lofric catheter with a surfacecoating of hydrophilic polymer, polyvinylpyrrolidone(PVP), to enable easy lubrication when dippedin water and so reduce friction on the urethralmucosa10.
Patients and methodsSince November 1985, over 85 patients have beenstarted on intermittent low friction self-catheterization(ILSC) following optical urethrotomy, in the hope ofpreventing or modifying restenosis ofthe urethra. Thefirst 42 patients had the longest follow up period andare reported here. The majority (n=37) were underurological review for many years and had manyurethral dilatations and multiple urethrotomies forrecurrent stricture disease (recurrent stricture group).A small number (n=5) presented with a stricture forthe first time (new stricture group). The age range ofall 42 patients was 23-82 years (mean 62 years)compared with 23-58 years (mean 43 years) for the5 patients in the new stricture group.The diagnosis of a recurrent or new stricture was
confi'rmed by urethroscopic evaluation under generalanaesthetic. The sites involved were the penile orbulbar urethra, and several had narrowing in morethan one segment. In all cases the procedure suggestedin 1974 by Sachse2, and more recently recorded bySmith et al.5 and Gaches et al.4, using the Storzurethrotome was adopted. In those cases whereurethral narrowing was severe, after visualizing theface of the stricture, the channel was canulated bypassing a small retrograde ureteric catheter (withoutstylet) down the instrument and through the stricture.Incision into the strictured urethra was confinedto the 12 o'clock position, with the cutting bladeextended and moving the whole instrument in anupward and outward direction. The length of theincision extended from normal urethra proximallyto normal urethra distally and included the fullthickness of the strictured segment. Bleeding pointswere occasionally diathermized using an electrodedown the operating port of the urethrotome.
Paper read toSection ofUrology,27 November 1986
a.I.

Journal of the Royal Society of Medicine Volume 81 March 1988 137
It has not been our routine policy to catheterizepatients following urethrotomy, but a few patientswere catheterized for up to 48 hours for urethralbleeding. All the patients were discharged home whenvoiding comfortably and were followed up as out-patients in a weekly 'stricture clinic' started forthis purpose.Patients were first seen 3-7 days after their
urethrotomy and a flow rate was obtained. For thepurpose of the study this initial visit was designatedtime 0. Forty patients were then taught the techniqueof intermittent self-catheterization using 16 Ch or18 Ch Lofric (Astra Meditec) hydrophilized disposableurinary catheters. The remaining 2 patients wereunable to catheterize themselves due to tetraplegiaand a right hemiparesis respectively. In these casesa relative and the district nurse were invited to theclinic to be shown the procedure.All patients were given enough catheters to pass a
new one twice a week for a month. They were givena 'diary card' to fill in, recording whether urinedrained during catheterization and if any difficultywas encountered. After this first month the frequencyof catheterization was reduced to once a week, andthe patients were reviewed at 2-3 monthly intervals.A flow rate was obtained at each ofthese clinic visits.All patients were encouraged to attend the clinic onan 'open access' basis if any problems arose.Catheterization was continued for 3 months in
patients with new strictures and for a longer periodof 6 months or more in the recurrent stricture group.The reason for the different times in this second groupis that they were randomized at 6 months to a groupcontinuing catheterization and a group who havestopped catheterization, but in this paper all theresults refer to patients on or at the end oftheir periodof catheterization (Figure 2). Flow rate traces wereanalysed and the maximum flow rate (QMAX) wasrecorded.
ResultsNew stricture groupThis comprised 5 patients, mean age 43 years, all ofwhom were able to catheterize satisfactorily andmaintain urinary flow rates over the 3-month period.The mean values were 32 ml/sec at time 0 and36 ml/sec at 3 months (Figure 3).
Recurrent stricture groupThis comprised 37 patients, mean age 64 years, 32of whom were able to catheterize satisfactorily and
NO OFPATIENTS
40i i40-
30_
20_
10-
39 39 39
NEW STRICTURES
34 34 34 34
10
7
4
Figure 2. Cumulative follow up ofpatients
OMAXFLOW RATEMLS/SEC
50
40-
30-
20_
10_
NEW RECURRENTto t3 to t6(+)
TIME (MONTHS)
FAILURESto t6(+)
Figure 3. Paired results for maximum flow rate postoperatively(tO), and at 3 months (t3) for new strictures and at 6 monthsor more (t6(+)) for the recurrent stricture group
maintain urinary flow rates for 6 months or more(range 6-10 months, mean 6.6 months) (Figure2). Despite satisfactory catheterization, urodynamicassessment was not possible in 3 patients: 2 hadneurological disease and the third debilitatingcarcinoma of the prostate, making hospital visitsimpractical. Urinary flow rates were assessed in 29patients, the mean values being 19 ml/sec at time 0 and20 ml/sec at 6 months plus (Figure 3). Using theWilcoxon signed rank test for paired data, there was nosignificant difference between the two values (P> 0.1).The remaining 5 patients either had some difficulty
or failed with this technique. The ages ofthese patientsare widely scattered and are not just an elderly groupas might be expected. The mean flow rates fell from25 ml/sec at time 0 to 12 ml/sec at 6 months plus(Figure 3). Details of these patients follow.
NEW STRICTURES (5) 3/2
RECURRENT STRICTURES (29) /;2
FAILURES (5)
Follow up flow rates as a percentageof postoperative value followingurethrotomy & LS.C.
Figure 4. The 'Three Flow' test applied to patients in thisstudy. It should be noted that 4 of the 5 'failures' are now
well on ILSC
1 2 3 4 5 6 7 a 9 10 MONTHS

138 Journal of the Royal Society of Medicine Volume 81 March 1988
cow 110F-
[L FZ000
0 10-z ,-rww5MI
5 -
1985 - ,~ 1986(100) (60)
16 1713
8
JULY OCTOBER JANUARYAUGUST NOVEMBER FEBRUARY
SEPTEMBER DECEMBER MARCH
Figure 5. Analysis ofoperating theatre logbook showing thenumber of urethrotomies per month
Case 1 (age 37): The patient stopped catheterizing after someweeks as he felt 'so much better'. A urethroscopy showeda recurrence of his stricture, and another urethrotomy hasbeen performed. His flow has been maintained on ILSCpostoperatively.
Case 2 (age 57): The patient stopped catheterizing after afew weeks as his urinary flow was 'much better'; howeverthe stricture returned within two months and a urethrotomywas needed. For a second time he failed to use the cathetersas directed, and the same sequence ofevents took place. Hisflow has now been maintained on ILSC for several months.
Case 3 (age 64): The patient stopped catheterizing after a fewweeks and has failed to attend several outpatient appoint-ments. We are awaiting his return with recurrent symptoms.
Case 4 (age 74): The patient was unable to drain urine whencatheterizing even from the outset; however, he was unwillingfor a repeat urethroscopy, but eventually after many monthswith a flow of 3 ml/sec agreed to a further examination
which showed a wide urethra with no stricture but a verytight bladder neck stenosis which was incised. His urinaryflow has improved and he is continuing on ILSC.
Case 5 (age 82): The patient has some difficulty passingcatheters 'now and again' but symptomatically maintainsa good flow.
It can be seen that 4 ofthese 5 patients are now beingmaintained on intermittent low friction catheterization
APRILand flow rates are being well maintained.
MAYJUNE
ComplicationsTwo ofthe 42 patients developed a symptomatic urinaryinfection and one of these developed epididymitis.Both were successfully treated with antibiotics andhave subsequently continued catheterization.
DiscussionIntermittent self-catheterization is a well recognizedand widely practised technique which we have appliedto prevent recurrent urethral stenosis after opticalurethrotomy. Many patients were elderly and themajority had been subjected to multiple previousoperations and urethral dilatations for recurrentstricture disease. This new form of treatment usingLofric catheters has been well received by thisgroup of patients. The simplicity of catheterizationwithout the need for extra lubrication or localanaesthetic gel has resulted in very good patientcompliance. In only 3 patients whose neurologicaldisease or debility prevented self-catheterization, didwe encourage a relative or district nurse to passthe catheters.
Figure 6. Mr. Hunter's opinion recommending intermittent self-bouginage. (From Practical Observations on the Treatmentof Strictures in the Urethra by Everard Home, 1797)

Journal of the Royal Society of Medicine Volume 81 March 1988 139
Following urethrotomy, surgeons have advisedcontinuous catheterization ofthe urethra for varyinglengths of time4-7, and have used different cathetermaterials6. Some have claimed that indwellingcatheterization for up to 6 weeks has given a morelasting effect in maintaining urinary flow. Significantdisadvantages of this policy are risk of urinaryinfection and inconvenience of emptying a leg-bag,particularly for elderly patients. Furthermore, ifILSCis adopted as a method of treatment in the post-operative period, indwelling catheterization can becompletely avoided in the majority of cases, therebyshortening any postoperative hospitalization.George and his colleagues" have described the
'Three Flow' test to identify patients with 'problematicurethral stricture' disease. Performing urinary flowrates preoperatively, postoperatively and after aperiod of3 months, they found that this 3-month valuewas accurate in discriminating cases effectively curedby one urethrotomy (mean 88% ofpostoperative value)from those who repeatedly deteriorated despitemultiple further optical urethrotomies (mean 33% ofpostoperative value). We analysed our new stricturegroup at 3 months but have taken a flow at 6 monthsor more for the recurrent stricture group. Our patientshave maintained their flow rates and the mean valueswere 112% (postoperative value) for the new stricturesand 105% (postoperative value) for the recurrentstricture group (Figure 4).
It is not yet clear whether low-friction catheteriza-tion needs to be continued indefinitely for patientswith difficult recurrent stricture disease or whethersome degree of urethral stabilization occurs when acritical time has passed. We have not found anyobvious difference using 16 Ch or 18 Ch catheters,but routinely now prefer the larger size as thisenables easy instrumentation at a later date whennecessary.Analysis of the operating theatre logbook, as an
independent record, showed that there has been adramatic reduction in the number of urethrotomiesperformed since this treatment was started (Figure 5).To conclude we have found this a very satisfactory
method of managing patients with recurrent strictures.
The Lofric catheterization is new, but many referencescan be found in 18th and 19th century literature whenself-bouginage was clearly commonplace. An examplefrom 1797 (Figure 6) records Mr Hunter's opinionrecommending intermittent self-bouginage.
Acknowledgment: We thank Messrs C P Bates, M C Bishop,M Dunn and R J Lemberger who have kindly allowed usto study patients under their care.
References1 Helmstein K. Internal urethrotomy modifications in the
operative technique. Urethroscopic control for evaluationofboth the primary results of the operation and of longterm healing. A discussion of68 cases. Acta Chir Scand1964;(Suppl 340):1-80
2 Sachse H. Zur behandlung der Harnrohrenstriktur. Dietransurethrale Schlitzung unter Sicht mit sharfemSchnitt. Fortschr Med 1974;92:12-15
3 Blandy JP. Urethral stricture. Postgrad Med J 1980;66:383-418
4 Gaches CGC, Ashken MH, Dunn M, Hammonds JC,Jenkins IL, Smith PJB. The role of selective internalurethrotomy in the management of urethral stricturedisease: a multi-centre evaluation. Br J Urol 1979;51:579-83
5 Smith PJB, Dunn M, Dounis A. The early results oftreatment of stricture of the male urethra using theSachse optical urethrotome. Br J Urol 1979;51:224-8
6 Wise HA, Engel REM, Whitaker RH. Treatment ofurethral strictures. J Urol 1972;107:269-72
7 Carlton FE, Scardino PL, Quattlebaum RB. Treatmentofurethral strictures with internal urethrotomy and sixweeks of sialastic catheter drainage. J Urol 1974;111:191-3
8 Sachse H. Die Sichturethrotomie mit scharfem Schnitt.Indikation - Technik - Ergebnisse. Urology 1978;17:177-81
9 Marshall S, Lyon RP, Olsen S. Internal urethrotomywith hydraulic urethral dilatations. J Urol 1972;106:553-6
10 Jensen SE. Mindre problem med hal kateter. MediciniskTeknik 1986; No. 6, November
11 George NJR, Grant JB, Lupton EW. 'Three Flow' testidentifies patients with problematic urethral stricture.Personal communication
(Accepted 5 August 1987)










![A new technique of double-face buccal graft urethroplasty ...cal techniques used in the treatment of female urethral stricture. Eur Urol 2013;64:965-73. [CrossRef] 5. Palminteri E,](https://static.fdocuments.net/doc/165x107/60a97c5fb327f06e035f2315/a-new-technique-of-double-face-buccal-graft-urethroplasty-cal-techniques-used.jpg)




