
Transformation and cytotoxicity of iron in siderosis bulbi.
11
Transformation and Cytotoxicity of Iron in Siderosis Bulbi Akihiko Toworo Ocular tissues from two enucleated and one trabeculectomized human eyes with siderosis bulbi were studied by electron microscopy. Ferritin particles were demonstrated in various cell types of the three eyes. Other types of iron were not identifiable. The ferritin particles were scattered throughout the cytoplasm, with a few particles in the nucleus and extracellular space. More ferritin particles were seen in tissues near the iron foreign body. The cells which contained numerous ferritin particles also had siderosomes, most of which were thought to be conglomerates of the ferritin particles in the secondary lysosomes. Cells with numerous ferritin particles, particularly in the siderosomes, showed vacuolar degeneration. The present study indicated that in siderosis bulbi, iron released from the iron foreign body is deposited as ferritin scattered throughout the cytoplasm and is sometimes accumulated as sid- erosomes, in the affinitive cells. In siderosis bulbi, the cells become damaged by the deposition of ferritin in the cytoplasm, especially in the form of siderosomes. Invest Ophthalmol Vis Sci 27:226-236, 1986 Among intra-ocular foreign bodies, those of iron are the most numerous ones seen, as a result of industrial accidents. The retention of an iron foreign body in the eye almost always results in progressive iron deposition throughout the eye, inducing degeneration of the retina, cataract formation, and secondary glaucoma, in the late stage. This condition is known as siderosis bulbi, 1 but the pathophysiology of this condition remains ob- scure. Little is known of the transformation of the iron foreign body and its redistribution in ocular tissues nor of the relationship between iron and its toxicity to ocu- lar tissue. Leber 2 proposed that metallic iron was dis- solved by carbon dioxide in the tissues and, having diffused throughout the eye as a bicarbonate ofsubox- ide of iron, entered the cells, where it was oxidized and precipitated in insoluble form. Mayou 3 thought that intraocular iron was absorbed as colloidal ferric hy- droxide and was re-precipitated as the albuminate of iron in the cells. He considered colloidal iron had a toxic effect upon the cells. Some authors attributed the cytotoxic effect of the iron to a disturbance in enzy- matic activity, 4 " 7 and others reported that the oxidation of iron may play a detrimental role. 8 Cibis et al 9 "" suggested that inadequate blood supply, which may be induced by linkage of iron to siderophilic matter such as acid mucopolysaccharides in the eye, exerts dele- terious effects on intraocular structures. From the Department of Ophthalmology, Faculty of Medicine, Kyushu University, Fukuoka, Japan. Submitted for publication: February 4, 1985. Reprint requests: Akihiko Tawara, MD, Department of Ophthal- mology, Faculty of Medicine, Kyushu University, 3-1-1, Maidashi, Higashi-ku, Fukuoka 812, Japan. Ocular tissues obtained from three patients with in- tra-ocular iron foreign body were examined by electron microscopy, the objective being to study the transfor- mation and localization of iron and its toxic effect on the ocular tissue in cases of siderosis bulbi. Materials and Methods A total of five eyes, three with siderosis bulbi and two controls, was examined. Of three eyes with siderosis bulbi, two were enucleated and their ocular tissues, cornea, anterior chamber angle tissue, iris, ciliary body, choroid, retina, and sclera were studied histologically. The third eye had undergone trabeculectomy and the obtained anterior chamber angle tissue and iris were studied. One control eye was enucleated from a 27-yr- old woman with neuroepithelioma of the left zygomatic and orbital region. The other was obtained from an 81-yr-old man diagnosed as right orbital tumor (his- tological diagnosis was adenocarcinoma). Cornea, an- terior chamber angle tissue, iris, ciliary body, choroid, retina, and sclera from the control eyes were examined. The ocular tissues were fixed in cold 4% glutaral- dehyde with 0.1 M phosphate buffer (cases 1 and 3, and one control eye from a 27-yr-old woman), or in cold 4% glutaraldehyde with 0.1 M cacodylate buffer (case 2 and the other control eye), and postfixed in cold 1% osmium tetroxide with the same buffer for 1 hr. These tissues were dehydrated in graded concentrations of ethanol and embedded in Epon. One-micron thick sections were stained with toluidine blue for light mi- croscopy, and ultrathin sections cut on an ultramicro- tome and studied under an electron microscope with- out staining. Some sections were observed after staining 226.. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
-
Upload
truongtuong -
Category
Documents
-
view
226 -
download
1
Transcript of Transformation and cytotoxicity of iron in siderosis bulbi.

Transformation and Cytotoxicity of Ironin Siderosis Bulbi
Akihiko Toworo
Ocular tissues from two enucleated and one trabeculectomized human eyes with siderosis bulbi werestudied by electron microscopy. Ferritin particles were demonstrated in various cell types of the threeeyes. Other types of iron were not identifiable. The ferritin particles were scattered throughout thecytoplasm, with a few particles in the nucleus and extracellular space. More ferritin particles were seenin tissues near the iron foreign body. The cells which contained numerous ferritin particles also hadsiderosomes, most of which were thought to be conglomerates of the ferritin particles in the secondarylysosomes. Cells with numerous ferritin particles, particularly in the siderosomes, showed vacuolardegeneration. The present study indicated that in siderosis bulbi, iron released from the iron foreignbody is deposited as ferritin scattered throughout the cytoplasm and is sometimes accumulated as sid-erosomes, in the affinitive cells. In siderosis bulbi, the cells become damaged by the deposition of ferritinin the cytoplasm, especially in the form of siderosomes. Invest Ophthalmol Vis Sci 27:226-236, 1986
Among intra-ocular foreign bodies, those of iron arethe most numerous ones seen, as a result of industrialaccidents. The retention of an iron foreign body in theeye almost always results in progressive iron depositionthroughout the eye, inducing degeneration of the retina,cataract formation, and secondary glaucoma, in thelate stage. This condition is known as siderosis bulbi,1
but the pathophysiology of this condition remains ob-scure. Little is known of the transformation of the ironforeign body and its redistribution in ocular tissues norof the relationship between iron and its toxicity to ocu-lar tissue. Leber2 proposed that metallic iron was dis-solved by carbon dioxide in the tissues and, havingdiffused throughout the eye as a bicarbonate ofsubox-ide of iron, entered the cells, where it was oxidized andprecipitated in insoluble form. Mayou3 thought thatintraocular iron was absorbed as colloidal ferric hy-droxide and was re-precipitated as the albuminate ofiron in the cells. He considered colloidal iron had atoxic effect upon the cells. Some authors attributed thecytotoxic effect of the iron to a disturbance in enzy-matic activity,4"7 and others reported that the oxidationof iron may play a detrimental role.8 Cibis et al9""suggested that inadequate blood supply, which may beinduced by linkage of iron to siderophilic matter suchas acid mucopolysaccharides in the eye, exerts dele-terious effects on intraocular structures.
From the Department of Ophthalmology, Faculty of Medicine,Kyushu University, Fukuoka, Japan.
Submitted for publication: February 4, 1985.Reprint requests: Akihiko Tawara, MD, Department of Ophthal-
mology, Faculty of Medicine, Kyushu University, 3-1-1, Maidashi,Higashi-ku, Fukuoka 812, Japan.
Ocular tissues obtained from three patients with in-tra-ocular iron foreign body were examined by electronmicroscopy, the objective being to study the transfor-mation and localization of iron and its toxic effect onthe ocular tissue in cases of siderosis bulbi.
Materials and Methods
A total of five eyes, three with siderosis bulbi andtwo controls, was examined. Of three eyes with siderosisbulbi, two were enucleated and their ocular tissues,cornea, anterior chamber angle tissue, iris, ciliary body,choroid, retina, and sclera were studied histologically.The third eye had undergone trabeculectomy and theobtained anterior chamber angle tissue and iris werestudied. One control eye was enucleated from a 27-yr-old woman with neuroepithelioma of the left zygomaticand orbital region. The other was obtained from an81-yr-old man diagnosed as right orbital tumor (his-tological diagnosis was adenocarcinoma). Cornea, an-terior chamber angle tissue, iris, ciliary body, choroid,retina, and sclera from the control eyes were examined.
The ocular tissues were fixed in cold 4% glutaral-dehyde with 0.1 M phosphate buffer (cases 1 and 3,and one control eye from a 27-yr-old woman), or incold 4% glutaraldehyde with 0.1 M cacodylate buffer(case 2 and the other control eye), and postfixed in cold1% osmium tetroxide with the same buffer for 1 hr.These tissues were dehydrated in graded concentrationsof ethanol and embedded in Epon. One-micron thicksections were stained with toluidine blue for light mi-croscopy, and ultrathin sections cut on an ultramicro-tome and studied under an electron microscope with-out staining. Some sections were observed after staining
226..
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018

No. 2 CYTOTOXICITY OF IRON IN SIDEROSIS / Toworo 227
with uranyl acetate and lead citrate, or lead citrate only.Sections ranging from 0.1-0.3 nm were used for ana-lytical electron microscopy (ORTEC, EEDS).
Case Reports
Case 1. A 48-yr-old man was first seen in 1960 with rightintraocular foreign body. Ophthalmoscopically, the foreignbody, which was thought to be iron, was recognized on theretina just beneath the optic disc. There was not much in-traocular bleeding. An attempt to remove the foreign bodyby Riesenmagnet was unsuccessful. In 1974, he again visitedour clinic complaining of severe pain.
Visual acuity of the right eye (OD) was 0 and the left eye(OS) was 20/16, with spectacles. Ocular tension was OD:17.3 mm Hg and OS: 14.5 mm Hg. Slit-lamp examinationrevealed keratic precipitates and a small quantity of floatersin the right anterior chamber. The right disc was pale withoutglaucomatous cupping. The retina was degenerated. Theelectroretinogram was extinguished in the right eye. His righteye was enucleated following a diagnosis of siderosis bulbiassociated with intractable endophthalmitis.
Case 2. This 56-yr-old woman had had an intraocular for-eign body in the left eye since 1962, as removal had beenunsuccessful. Sight in the left eye gradually decreased. In 1983,she visited our clinic complaining of left ocular pain.
Visual acuity was OD: 20/20 with spectacles and OS: 0.The ocular tension was OD: 13 mm Hg and OS: 30 mm Hg.The left eye showed ciliary injection and moderate anteriorchamber floaters. Gonioscopically, the anterior chamber anglewas closed completely. Mild rubeosis was seen on the iris.Severe cataract prevented fundus examination.
Her left eye was enucleated following a diagnosis of side-rosis bulbi with secondary angle-closure glaucoma. An ironforeign body was present in the lens. There was no bleedingor opacity in the vitreous body, as determined using a bio-cular-microscope.
Case 3. This 31-yr-old man, with no abnormalities beforehaving gradually advanced visual disturbance in the righteye, visited our clinic in 1975. Visual acuity of the right eyewas perception of hand movement. The lens had a brownopacity with rust spots of brown pigmentation on the surface.Head X-ray which showed a foreign body at the ciliary bodyconfirmed the diagnosis of right intra-ocular iron foreign bodywith complicated cataract. Removal of the iron foreign bodyby Riesenmagnet followed by extracapsular lens extractionled to an improvement of visual acuity to 20/20, with use ofa contact lens.
About 3 yr later, in 1979, he again visited our clinic com-plaining of right ocular pain with visual disturbance. Visualacuity was OD: perception of hand movement and OS: 20/14. The ocular tension was OD: 45 mm Hg and OS: 14 mmHg, and the aqueous outflow rate was OD: 0.04 mm3/min/mm Hg and OS: 0.26 mm'/min/mm Hg. The right corneahad a light brown opacity, diffusely, but the anterior chamberwas clear. The iridocorneal angle was open without abnor-mality. Severe glaucomatous cupping was found in the rightoptic disc. The retinal vessels were thin. Goldmann perimetryrevealed severe glaucomatous loss in the right visual field.Electroretinogram was markedly reduced in the right eye.
This case was diagnosed as right siderosis bulbi associatedwith secondary open-angle glaucoma. Trabeculectomy withperipheral iridectomy had to be done twice to control theintraocular pressure.
Results
Siderosis Bulbi
In the ocular tissue from all three patients, examinedwithout staining, electron-dense uniform particles weredemonstrated diffusely throughout the cytoplasm ofthe cells (Figs. 1A-4). Under a higher magnification,many of the particles were 6-7 nm-sided squares andconsisted of 4 subunits about 3 nm in diameter (Figs.2,4B). Some of the particles appeared as paired parallellines, open rings, triads, and pentads (Figs. 2, 4B). Afew electron-dense particles were demonstrated in thenucleus (Fig. 5) and in the extracellular connective tis-sue (Fig. 4 A). Some of these cells with diffuse particlesalso contained electron-dense elliptical deposits, vary-ing in diameter from 0.1 /im to 3 fim (Figs. 1 A, 3, 4A).Usually, the deposits were surrounded by a singlemembrane (Figs. 1 A, 3). In the electron-lucent area ofthe deposits, isolated electron-dense square particles6-7 nm long were observed (Fig. 3). Analytical electronmicroscopy revealed a high content of iron in the elec-tron-dense deposits (Figs. IB, C). The cells with nu-merous electron-dense particles and deposits showedvacuolar degeneration (Fig. 4A).
The retina of case 1 showed atrophic change withgliosis. In some places, the retinal pigment epithelialcells had disappeared. Electron-dense particles weredemonstrated mainly in the cytoplasm of the retinalpigment epithelial cells (Figs. 1A, 3) and Miiller cells(Fig. 5). Some of these cells with the particles also hadelliptical electron-dense deposits in the cytoplasm (Figs.1A, 3). In the retinal pigment epithelial cells, somedeposits included pigment granules as well as the elec-tron-dense particles (Fig. 1A), and others containedshed photoreceptor outer segment discs and particles,within the same membrane. Several cells had large cy-toplasmic vacuoles which included both electron-denseand electron-lucent parts, showing degenerative change(Fig. 6). The neural cells of the retina, including conesand rods, horizontal, amacrine, bipolar and ganglioncells, showed few electron-dense particles and deposits(Fig. 5). These findings were observed throughout pos-terior, equatorial, and peripheral portions of the retina.In the ciliary body, pigmented and nonpigmentedepithelial cells, muscle cells, and fibroblasts had bothelectron-dense particles and deposits in the cytoplasm(Fig. 7). Some cytoplasmic organelles which weresurrounded by mono-layered membrane containedphagocytized materials as well as numerous electron-dense particles (Fig. 7). The cells which comprised thechoroid and the iris included diffuse electron-denseparticles and small amounts of deposits. In the cornea,anterior chamber angle tissue, and sclera, electron-dense particles were rarely demonstrated, either in thecells or in the extracellular spaces.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
228 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / February 1986 Vol. 27
0.5
[ SIDEROSQAE EEM-lIlD: CONTROL
LT-12ISOS 2=76
BB95.12E=8.4I
e-i§IBKEV 7. (7118 1= t
LT«B
1 2 8 ^
m• • •
12ISET=
^̂ BBB
121S
|^B
.1382
18 EV/CH
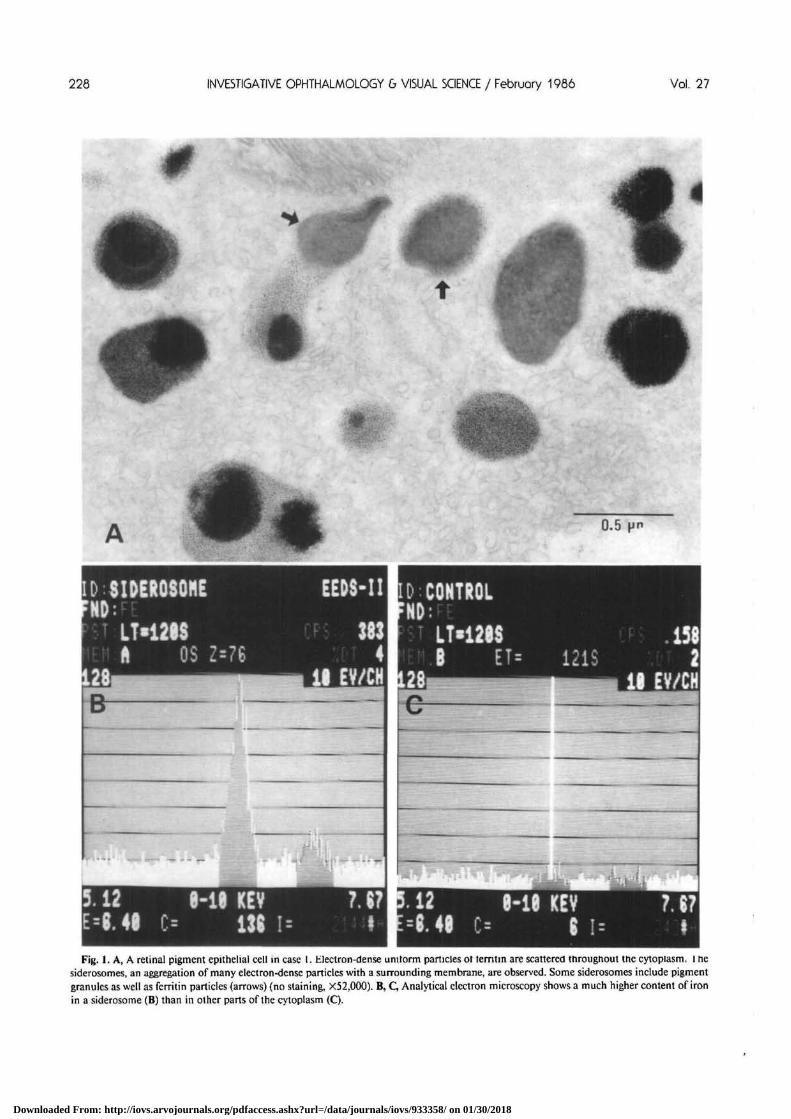
Hi^B•Fig. 1. A, A retinal pigment epithelial cell in case 1. Electron-dense unitorm particles or terntin are scattered throughout the cytoplasm. 1 ne
siderosomes, an aggregation of many electron-dense particles with a surrounding membrane, are observed. Some siderosomes include pigmentgranules as well as ferritin particles (arrows) (no staining, X52,000). B, C, Analytical electron microscopy shows a much higher content of ironin a siderosome (B) than in other parts of the cytoplasm (C).
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018

No. 2 CYTOTOXICITY OF IRON IN 5IDERO5I5 / Toworo 229
JiA pm
: • * • <
, * .
- • « * •
Fig. 2. A higher magnification of electron-dense particles in case 1. The particles show regular squares 6-7 nm long, consisting of 4 subunits(arrows), and several variations, including paired parallel lines (double arrows), open rings (arrowheads), and triads (opened arrow) (no staining,X300,000).
The retina of case 2 had a fairly normal structureexcept for reduction in the number of ganglion cells.In the cytoplasm of the retinal pigment epithelial andMuller cells, scattered electron-dense particles wereobserved (Fig. 8A), while the neural cells were free fromthe particles. The quantity of the particles was less thanthat in the anterior part of the eye, and electron-densedeposits were rarely demonstrated. In some retinal pig-ment epithelial cells, phagosomes located near the basalportion of the cells contained not only discs but alsomany particles (Fig. 8 A), despite the absence of particlesin the photoreceptor outer segments and in the inter-cellular spaces (Fig, 8B). In the choroid and sclera, thecells contained small numbers of electron-dense par-ticles in the cytoplasm. The nonpigmented and pig-mented epithelial cells, muscle cells, fibroblasts, andmelanocytes of the ciliary body and the iris had bothscattered electron-dense particles and elliptical deposits(Fig. 9), some of which included phagocytized pigmentgranules (Fig. 9A). Some cells had large vacuoles con-taining many electron-dense particles and electron-lu-cent areas with a single limiting membrane (Fig. 9A).In the corneal endothelial cells and fibroblasts, electron-
dense particles and deposits were seen. Some of thecells showed degeneration with large vacuoles whichappeared as enlarged electron-dense deposits.
In the anterior chamber angle tissue of case 3,Schlemm's canal had an open lumen (Fig. 10), and thetrabecular mesh work was compact with narrow inter-trabecular spaces. The endothelial cells in the endo-thelial meshwork or covering trabecular sheets showeddegeneration (Figs. 4A, 10). In the section not stained,endothelial cells covering Schlemm's canal and tra-becular sheets and located in the endothelial meshwork,contained electron-dense diffuse particles in the cyto-plasm (Fig. 4). Cells with many particles also includedoval electron-dense deposits (Figs. 4A, 10). The en-dothelial cells which had numerous electron-denseparticles as well as many large deposits appeared to bedegenerated (Fig. 4A). There were a few electron-denseparticles and no deposits in the extracellular connectivetissues (Fig. 4A). The corneal fibroblasts included inthe trabeculectomized specimen had diffuse electron-dense particles and deposits. There were many cellswith large cytoplasmic vacuoles. In the iris obtainedby iridectomy, the electron-dense particles and deposits
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018

200 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / February 1966 Vol. 27
0.1 Hm
2V
B
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
No. 2 CYTOTOXICITY OF IRON IN SIDERO5IS / Toward 201
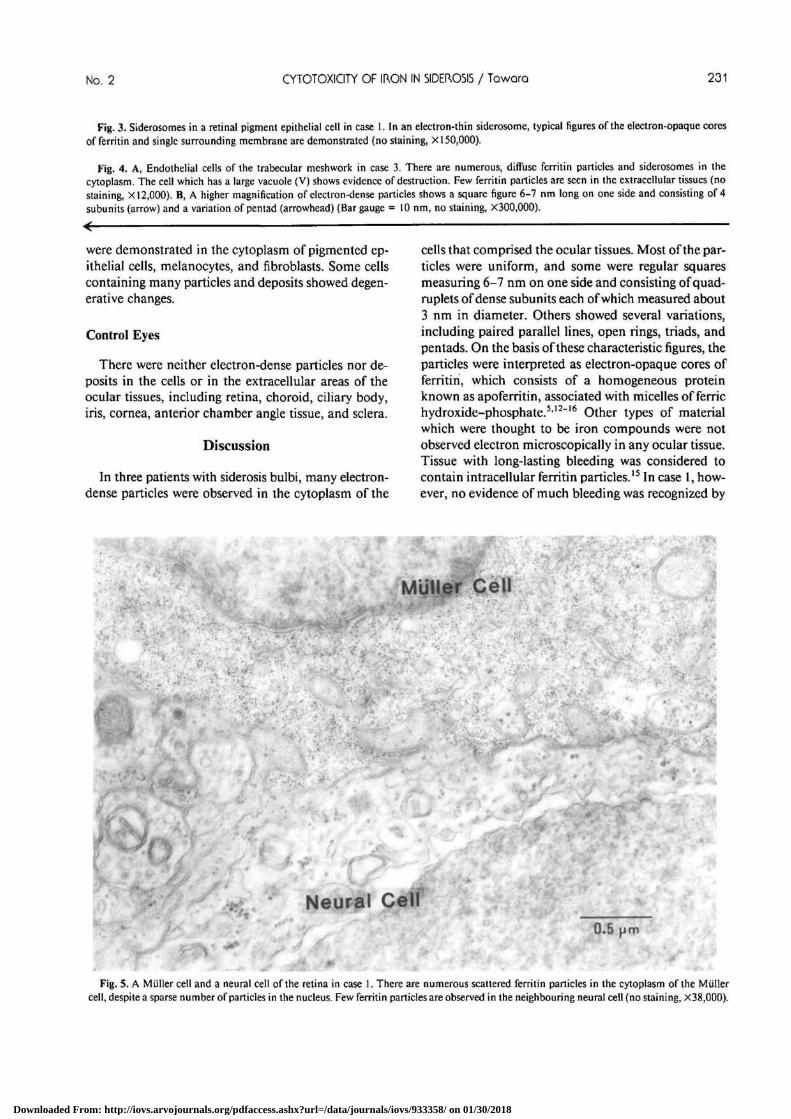
Fig. 3. Siderosomes in a retinal pigment epithelial cell in case 1. In an electron-thin siderosome, typical figures of the electron-opaque coresof ferritin and single surrounding membrane are demonstrated (no staining, X 150,000).
Fig. 4. A, Endothelial cells of the trabecular meshwork in case 3. There are numerous, diffuse ferritin particles and siderosomes in thecytoplasm. The cell which has a large vacuole (V) shows evidence of destruction. Few ferritin particles are seen in the extracellular tissues (nostaining, X 12,000). B, A higher magnification of electron-dense particles shows a square figure 6-7 nm long on one side and consisting of 4subunits (arrow) and a variation of pentad (arrowhead) (Bar gauge = 10 nm, no staining, X300,000).
were demonstrated in the cytoplasm of pigmented ep-ithelial cells, melanocytes, and fibroblasts. Some cellscontaining many particles and deposits showed degen-erative changes.
Control Eyes
There were neither electron-dense particles nor de-posits in the cells or in the extracellular areas of theocular tissues, including retina, choroid, ciliary body,iris, cornea, anterior chamber angle tissue, and sclera.
Discussion
In three patients with siderosis bulbi, many electron-dense particles were observed in the cytoplasm of the
cells that comprised the ocular tissues. Most of the par-ticles were uniform, and some were regular squaresmeasuring 6-7 nm on one side and consisting of quad-ruplets of dense subunits each of which measured about3 nm in diameter. Others showed several variations,including paired parallel lines, open rings, triads, andpentads. On the basis of these characteristic figures, theparticles were interpreted as electron-opaque cores offerritin, which consists of a homogeneous proteinknown as apoferritin, associated with micelles of ferrichydroxide-phosphate.512"16 Other types of materialwhich were thought to be iron compounds were notobserved electron microscopically in any ocular tissue.Tissue with long-lasting bleeding was considered tocontain intracellular ferritin particles.15 In case 1, how-ever, no evidence of much bleeding was recognized by
r
MUUef Cell
Neural Cell0.5 pm
Fig. 5. A Muller cell and a neural cell of the retina in case 1. There are numerous scattered ferritin particles in the cytoplasm of the Mullercell, despite a sparse number of particles in the nucleus. Few ferritin particles are observed in the neighbouring neural cell (no staining, X38,OOO).
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018

232 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / February 1986 Vol. 27
0.5
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
No. 2 CYTOTOXICITY OF IKON IN SIDERO5IS / Toworo 233
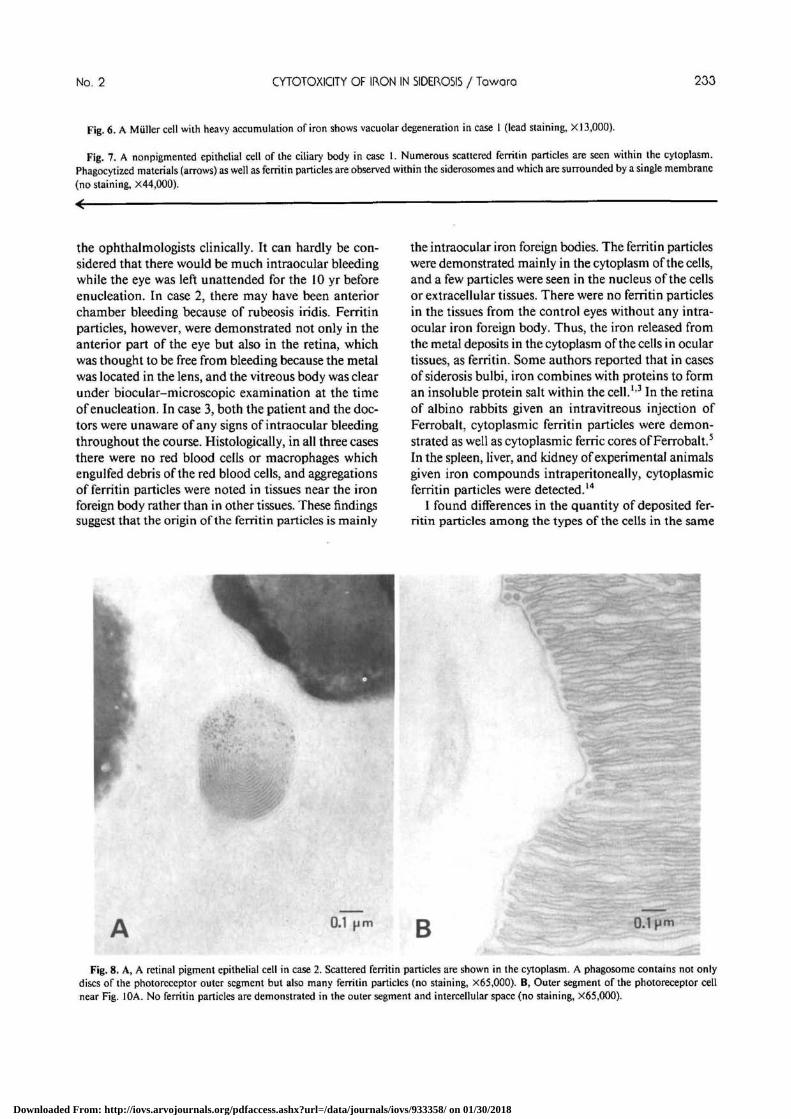
Fig. 6. A Miiller cell with heavy accumulation of iron shows vacuolar degeneration in case 1 (lead staining, XI 3,000).
Fig. 7. A nonpigmented epithelial cell of the ciliary body in case 1. Numerous scattered ferritin particles are seen within the cytoplasm.Phagocytized materials (arrows) as well as fenitin particles are observed within the siderosomes and which are surrounded by a single membrane(no staining, X44,000).
the ophthalmologists clinically. It can hardly be con-sidered that there would be much intraocular bleedingwhile the eye was left unattended for the 10 yr beforeenucleation. In case 2, there may have been anteriorchamber bleeding because of rubeosis iridis. Ferritinparticles, however, were demonstrated not only in theanterior part of the eye but also in the retina, whichwas thought to be free from bleeding because the metalwas located in the lens, and the vitreous body was clearunder biocular-microscopic examination at the timeof enucleation. In case 3, both the patient and the doc-tors were unaware of any signs of intraocular bleedingthroughout the course. Histologically, in all three casesthere were no red blood cells or macrophages whichengulfed debris of the red blood cells, and aggregationsof ferritin particles were noted in tissues near the ironforeign body rather than in other tissues. These findingssuggest that the origin of the ferritin particles is mainly
the intraocular iron foreign bodies. The ferritin particleswere demonstrated mainly in the cytoplasm of the cells,and a few particles were seen in the nucleus of the cellsor extracellular tissues. There were no ferritin particlesin the tissues from the control eyes without any intra-ocular iron foreign body. Thus, the iron released fromthe metal deposits in the cytoplasm of the cells in oculartissues, as ferritin. Some authors reported that in casesof siderosis bulbi, iron combines with proteins to forman insoluble protein salt within the cell.1'3 In the retinaof albino rabbits given an intravitreous injection ofFerrobalt, cytoplasmic ferritin particles were demon-strated as well as cytoplasmic ferric cores of Ferrobalt.5
In the spleen, liver, and kidney of experimental animalsgiven iron compounds intraperitoneally, cytoplasmicferritin particles were detected.14
I found differences in the quantity of deposited fer-ritin particles among the types of the cells in the same
0.1 B 0.1 H m
Fig. 8. A, A retinal pigment epithelial cell in case 2. Scattered ferritin particles are shown in the cytoplasm. A phagosome contains not onlydiscs of the photoreceptor outer segment but also many ferritin particles (no staining, X65,000). B, Outer segment of the photoreceptor cellnear Fig. 10A. No ferritin particles are demonstrated in the outer segment and intercellular space (no staining, X65.OOO).
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018

234 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / February 1986 Vol. 27
0.1 i m
Fig. 9. A, Fibroblasts and a meianocyte of the iris in case 2. There are numerous scattered ferritin particles and some siderosomes within thecytoplasm. A large vacuole which contains ferritin particles (V) and a siderosome which includes both a pigment granule (arrow) and ferritinparticles are shown. Few ferritin particles are observed in the extracellular tissues (no staining, X21,000). B, A higher magnification of electron-dense particles. Typical square figures of the cores of ferritin are diffuse (no staining, XI 50,000),
tissue. In the retina, the particles of ferritin were ob-served mainly in Miiller cells and retinal pigment ep-ithelial cells, in contrast to a few particles in the neuralcells. Similar findings were reported in experimentalsiderosis5 and experimental subretinal hemorrhage.15
In cases of siderosis bulbi, the concentration of theiron is said to differ among the cells.117 The reasonsfor this difference remain unknown.
The distribution of deposited ferritin particles variedwith the case. In case 1, many more ferritin particleswere seen in the cytoplasm of the cells in the retinathan in the anterior part of the eye, despite more par-ticles in the anterior part of the eye in cases 2 and 3.This difference in iron distribution is thought to dependon the location of the intraocular iron foreign body,as Declercq et al8 reported. When the iron is locatedin the posterior part of the eye, as in case 1, iron ionsspread mainly by diffusion and are concentrated morein the posterior part of the eye. In those with an ironforeign body in the anterior part of the eye, as in cases2 and 3, iron ions spread by diffusion and with theflow of aqueous humor, and they accumulate mainlyin the anterior part of the eye. Therefore, in eyes with
an iron foreign body, iron ions, released from the metalprobably spread by diffusion and by the flow of aqueoushumor, convert to ferric hydroxide-phosphate, andcombine with apoferritin to deposit as ferritin in thecytoplasm of certain cells of the ocular tissues.
In cases of siderosis bulbi, cells with numerous scat-tered ferritin particles also contained intracytoplasmicelectron-dense deposits. These deposits are thought tobe siderosomes, which have been reported to be anaggregation of iron.5'15'18 In our cases, electron micro-analysis showed peaks of iron in the siderosomes, asnoted in cases of post-traumatic hyphema,18 and ofsiderotic cataract.19 In relatively electron-thin areas ofthe siderosomes, characteristic structures of the elec-tron-opaque cores in ferritin were demonstrated. Manysiderosomes had a single limiting membrane, and someincluded phagocytized materials as well as aggregationof ferritin. In the retina, phagosomes of retinal pig-mented epithelial cells contained not only discs of thephotoreceptor outer segment but also ferritin particles.Neighboring discs and intercellular spaces were freefrom ferritin particles. From these findings, it is con-sidered that the origin of most of the siderosomes is
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
No. 2 CYTOTOXICITY OF IRON IN SIDEROSIS / Toworo 235
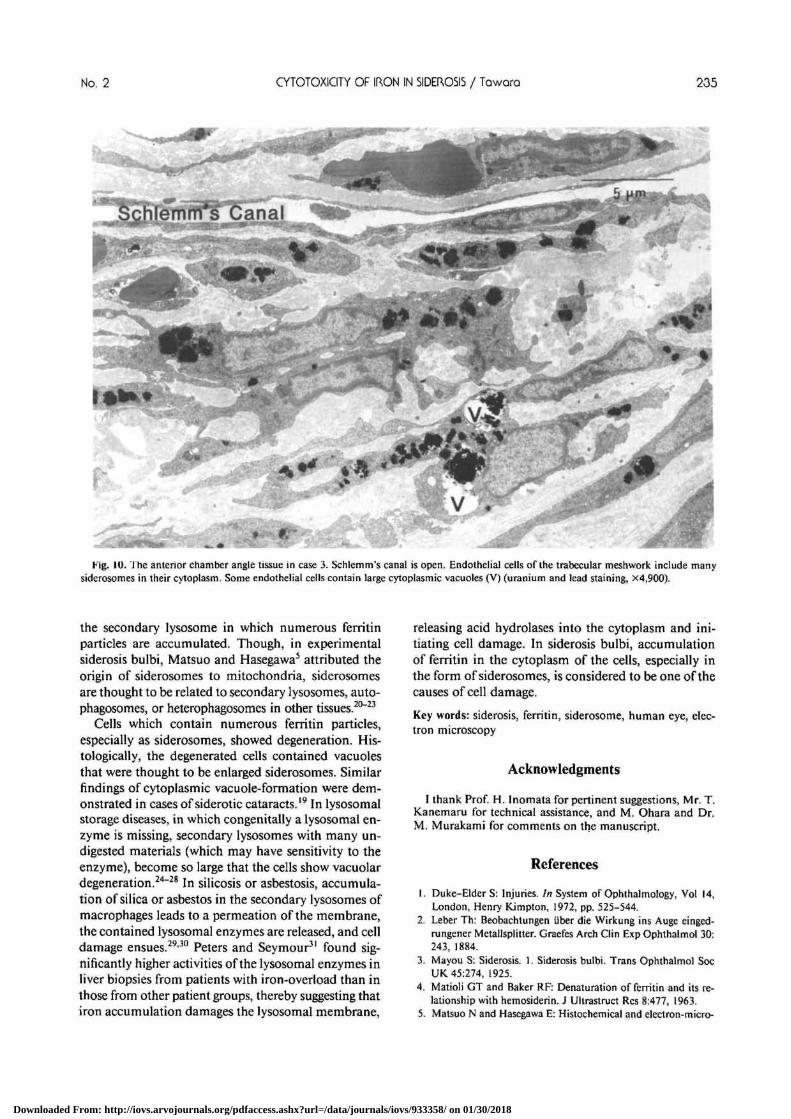
Fig. 10. The anterior chamber angle tissue in case 3. Schlemm's canal is open. Endothelial cells of ihe trabecular meshwork include manysiderosomes in their cytoplasm. Some endothelial cells contain large cytoplasmic vacuoles (V) (uranium and lead staining, X4.900).
the secondary lysosome in which numerous ferritinparticles are accumulated. Though, in experimentalsiderosis bulbi, Matsuo and Hasegawa5 attributed theorigin of siderosomes to mitochondria, siderosomesare thought to be related to secondary lysosomes, auto-phagosomes, or heterophagosomes in other tissues.20"23
Cells which contain numerous ferritin particles,especially as siderosomes, showed degeneration. His-tologically, the degenerated cells contained vacuolesthat were thought to be enlarged siderosomes. Similarfindings of cytoplasmic vacuole-formation were dem-onstrated in cases of siderotic cataracts.19 In lysosomalstorage diseases, in which congenitally a lysosomal en-zyme is missing, secondary lysosomes with many un-digested materials (which may have sensitivity to theenzyme), become so large that the cells show vacuolardegeneration.24"28 In silicosis or asbestosis, accumula-tion of silica or asbestos in the secondary lysosomes ofmacrophages leads to a permeation of the membrane,the contained lysosomal enzymes are released, and celldamage ensues.2930 Peters and Seymour31 found sig-nificantly higher activities of the lysosomal enzymes inliver biopsies from patients with iron-overload than inthose from other patient groups, thereby suggesting thatiron accumulation damages the lysosomal membrane,
releasing acid hydrolases into the cytoplasm and ini-tiating cell damage. In siderosis bulbi, accumulationof ferritin in the cytoplasm of the cells, especially inthe form of siderosomes, is considered to be one of thecauses of cell damage.
Key words: siderosis, ferritin, siderosome, human eye, elec-tron microscopy
Acknowledgments
I thank Prof. H. Inomata for pertinent suggestions, Mr. T.Kanemaru for technical assistance, and M. Ohara and Dr.M. Murakami for comments on the manuscript.
References
1. Duke-Elder S: Injuries. In System of Ophthalmology, Vol 14,London, Henry Kimpton, 1972, pp. 525-544.
2. Leber Th: Beobachtungen iiber die Wirkung ins Auge einged-rungener Metallsplitter. Graefes Arch Clin Exp Ophthalmol 30:243, 1884.
3. Mayou S: Siderosis. 1. Siderosis bulbi. Trans Ophthalmol SocUK 45:274, 1925.
4. Matioli GT and Baker RF: Denaturation of ferritin and its re-lationship with hemosiderin. J Ultrastruct Res 8:477, 1963.
5. Matsuo N and Hasegawa E: Histochemical and electron-micro-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018
236 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / February 1986 Vol. 27
scopical studies on the retinal siderosis. Acta Societatis Ophthal-mologicae Japonicae 68:1702, 1964.
6. Wise JB: Treatment of experimental siderosis bulbi, vitreoushemorrhage, and corneal bloodstaining with deferoxamine. ArchOphthalmol 75:698, 1966.
7. Masciulli L, Anderson DR, and Charles S: Experimental ocularsiderosis in the squirrel monkey. Am J Ophthalmol 74:638, 1972.
8. Declercq SS, Meredith PCA, and Rosenthal AR: Experimentalsiderosis in the rabbit. Arch Ophthalmol 95:1051, 1977.
9. Cibis PA, Brown EB, and Hong S: Ocular effects of systemicsiderosis. Am J Ophthalmol 44(part II): 158, 1957.
10. Cibis PA, Yamashita T, and Rodriguez F: Clinical aspects ofocular siderosis and hemosiderosis. Arch Ophthalmol 62:180,1959.
11. Cibis PA and Yamashita T: Experimental aspects of ocular sid-erosis and hemosiderosis. Am J Ophthalmol 48(part II):465,1959.
12. Farrant JL: An electron microscopic study of ferritin. BiochimBiophys Acta 13:569, 1954.
13. Richter GW: A study of hemosiderosis with the aid of electronmicroscopy. J Exp Med 106:203, 1957.
14. Richter GW: The cellular transformation of injected colloidaliron complexes into ferritin and hemosiderin in experimentalanimals. J Exp Med 109:197, 1959.
15. Koshibu A: Ultrastructural studies of absorption of an experi-mentally produced subretinal hemorrhage. III. Absorption oferythrocyte break down products and retinal hemosiderosis atthe late stage. Acta Societatis Ophthalmologicae Japonicae 83:386, 1979.
16. Kerr DNS and Muir AR: A demonstration of the structure anddisposition of ferritin in the human liver cell. J Ultrastruct Res3:313, 1960.
17. Yanoff M and Fine BS: Surgical and nonsurgical trauma. InBiomedical Foundations of Ophthalmology, Chapter 6, DuaneTD and Jaeger EA, editors. Philadelphia, Harper & Row Pub-lishers, 1982, p. 41.
18. Ghadially FN, Schneider RJ, and Lalonde JMA: Haemosiderindeposits in the human cornea. J Submicrosc Cytol 13:455, 1981.
19. Hamai H, Takahashi S, Yanagita Y, Sanada T, and Takeda K:
The electron microscopic studies of the siderotic cataract. Jap-anese Journal of Clinical Ophthalmology 32:119, 1978.
20. Miller F and Palade GE: Lytic activities in renal protein absorp-tion droplets. An electron microscopical cytochemical study. JCell Biol 23:519, 1964.
21. Trump BF, Valigorsky JM, Arstila AU, Mergner WJ, and KinneyTD: The relationship of intracellular pathways of iron metabolismto cellular iron overload and the iron storage diseases. Am JPathol 72:295, 1973.
22. Bergeron C and Kovacs K: Pituitary siderosis. A histologic, im-munocytologic, and ultrastructural study. Am J Pathol 93:295,1978.
23. Richter GW: The iron-loaded cell—the cytopathology of ironstorage. Am J Pathol 91:363, 1978.
24. Baudhuin P, Hers HG, and Loeb H: An electron microscopicand biochemical study of type II glycogenosis. Lab Invest 13:1139, 1964.
25. Lagunoff D and Gritzka TL: The site of mucopolysaccharideaccumulation in Hurler's syndrome: an electron microscopic andhistochemical study. Lab Invest 15:1578, 1966.
26. Topping TM, Kenyon K.R, Goldberg MF, and Maumenee AE:Ultrastructural ocular pathology of Hunter's syndrome. Systemicmucopolysaccharidosis type II. Arch Ophthalmol 86:164, 1971.
27. Kenyon KR, Topping TM, Green WR, and Maumenee AE:Ocular pathology of the Maroteaux-Lamy syndrome (systemicmucopolysaccharidosis type VI): histologic and ultrastructuralreport of two cases. Am J Ophthalmol 73:718, 1972.
28. Libert J, Martin JJ, Ceuterick C, and Danis P: Ocular ultrastruc-tural study in a fetus with type II glycogenosis. Br J Ophthalmol61:476, 1977.
29. Allison AC, Harington JS, and Birbeck M: An examination ofthe cytotoxic effects of silica on macrophages. J Exp Med 124:141, 1966.
30. Allison AC: Lysosomes and the toxicity of paniculate pollutants.Arch Intern Med 128:131, 1971.
31. Peters TJ and Seymour CA: Acid hydrolase activities and lyso-somal integrity in liver biopsies from patients with iron overload.Clin Sci Mol Med 50:75, 1976.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933358/ on 01/30/2018


















