To understand the risk behaviours for HIV among male STD clinic attendees
37
To understand the risk behaviours for HIV among male STD clinic attendees Dr.Dilmini Mendis, Senior registrar NSACP Dr.P.S.K.Gunathunga, Medical Officer NSACP Dr. M. Jayalath, Medical Officer NSACP Dr.R.C. Fernando Medical Officer NSACP Dr.L.I. Rajapaksa, Consultant Venereologist,NSACP 1 28/09/2013
-
Upload
college-of-venereologists -
Category
Documents
-
view
218 -
download
1
description
Â
Transcript of To understand the risk behaviours for HIV among male STD clinic attendees

To understand the risk behaviours for HIV among male STD clinic attendees
Dr.Dilmini Mendis, Senior registrar NSACP Dr.P.S.K.Gunathunga, Medical Officer NSACP
Dr. M. Jayalath, Medical Officer NSACP Dr.R.C. Fernando Medical Officer NSACP
Dr.L.I. Rajapaksa, Consultant Venereologist,NSACP
1
28/09/2013

• According to the data available at the National STD AIDS Control Programme, Sri Lanka -
– More males seek services at STD clinics (During year 2011-8511 males-gov STD Clinics
– male attendance to STD clinics are increasing. – Increasing STI among MSM – Increasing injecting drug use
2

Few similar studies on male population in STD
Clinics, Sri Lanka -
1973 –Arulananthan T STD Clinic, Jaffna, 70% (236)Syphilis 71.7% (2532) gonorrhoea due to FSW. 1977 – STD Clinic, Anuradapura 70% STI due to FSW 1999 – Rajapaksa L STD Clinic, Katugasthota, 30-34% STI due to FSW 2006- Rajapaksa L STD Clinic Kalubowila,40% STI due to CSW
3

Study Objectives
• General objective
To determine the sexual partners responsible for transmitting STI/HIV and practices of safer sex among males attending Central STD Clinic Colombo
4

5
To determine the sexual partners responsible for transmitting STI/HIV among males attending
Central STD Clinic Colombo
To understand other related risk behaviour of the same population
To determine the safer sex practices in this population
To identify the relationship between the type of partner and STI
Specific objectives

Methodology
• Study design
Clinic based prospective study
Study setting
Central STD Clinic Colombo
6

Study sample
• Newly registered males – 1623
• Excluded – – Needle stick injuries
– Denied sexual exposure
– Less than 15 years old
– Prisoners /court referrals
– Those who refuse to give consent
– Study sample - 983
7

Study instrument
Interviewer administered questionnaire
• Data collected by medical officers having experience. for >1 year
• Data collected for a 1 year period from 1st August 2012 to 31st July 2013
• Included socio demographic characteristics and details about the last sexual exposure, type of partner, safer sex practices, other related risk behaviours
• Diagnosis through case records
8

Definitions
• Marital partner: spouse
• Regular partner: live-in sexual partner/ cohabiting partner
• Non regular partner (NRP)- sexual partner the respondent is not living with; had sex rarely or only once with whom money is not involved
• Sex worker: MSW/FSW- sexual partner to whom respondent paid money/ material in exchange for sex
• According to PIMS
9

Key Findings
10

Age
11
Mean-34.0
SD-11.407
N-983
Range-15-84

Education
12

Occupation
13
40% of the comprised
Skilled labourers/Drivers
and Forces
50% with unskilled labourers

Marital Status
14
52.5% married
11% denied sex exposures
Other than the MP

Reason for attendance
15

Last Sexual Partner/other than MP
16 N=875
50% sample admitted
LSE with a NRP
13.6% FSW/ 13.4% MSM
MSW exposures were
minimal

17
Further Questioning were done on
among males who admitted having
sexual exposures with partners
other than the marital partner

Partners according to the age group
18
Younger males- more contacts with males & Older males with FSW
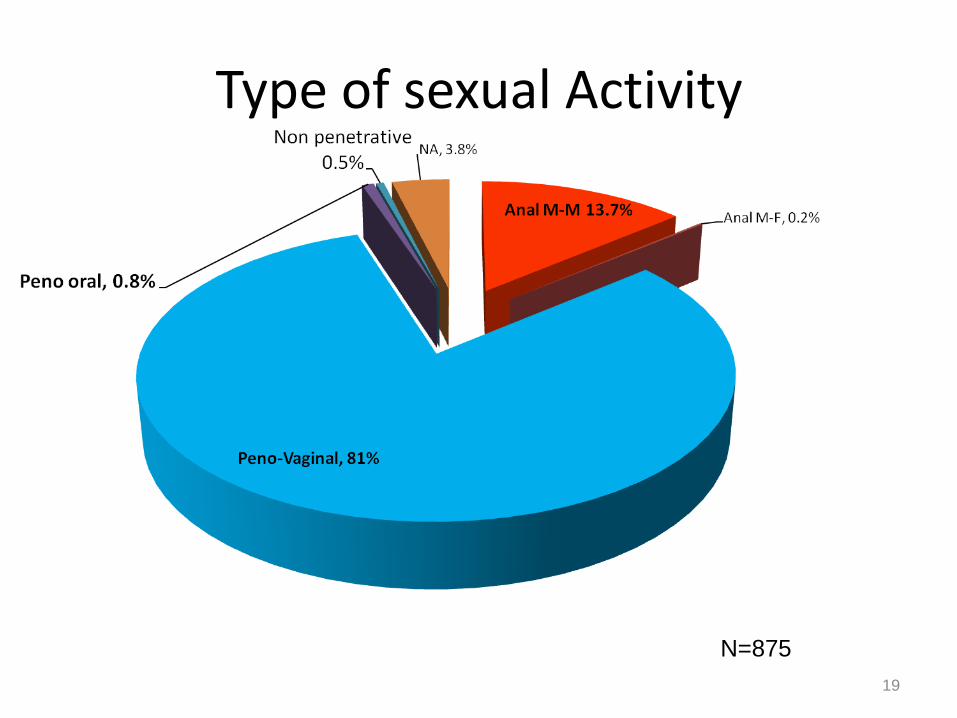
Type of sexual Activity
19
N=875

Males with MSM exposures
20
N=127

Relationship with marital status and partner
21

Coitarche
22

Other related risks
23

Drug Users- 5.9% of total
24
According to the BSS 2006-2007 5.5% drug use among factory workers

Safer Sex
25

Reasons for Non use of condoms
26

Information/ Condoms
Friends, 29.30%
Newspaper 9.60%
Doctor, 21.60%
NGO, 1.30%
Forces, 9.20%
Internet, 8.10% Friends
TV
School
Newspaper
Relative
Doctor
Teacher
NGO
Forces
Internet
Missing
NA
27

• Only STI with a short incubation period Gonorrhoea, Genital Herpes and Non gonococcal urethritis were considered.
28

Relationship/Partner/STI
29

MSM/STI
30

31

Contribution of each category
32
Conclusions • Male population in the sample had satisfactory education
• More males had contacts with Non regular partners
• Availability of NRP for unsafe sex
• MSM / FSW /NRP are equally important sources of infection
• Other related risk behaviours were similar to the findings of BSS done in 2006-2007 among factory workers
• Early Syphilis and GC were more seen among MSM
• However unsafe sex contacts are common
• Low condom use was not due to unavailability, but for other reasons – satisfaction/faith
• Apart from doctors and friends Newspapers /Forces/ Internet were more important sources of information on condoms
36

Suggestions
• The strategies used for prevention interventions need to be revisited in the context
• Current programmes organized by NGO’s aim at MSM &FSW
• There are no programmes to reach the general population- which is priority since most of the clients and NRP are representing the general population
• Increase the awareness among males and females through mass media,primary health care teams and multisectoral involvement may be important
• Changing attitudes regarding condoms should be an ongoing activity in prevention programmes
37
Limitations
• Study was done at Central STD Clinic Colombo- Sri Lanka
• Findings cannot be generalized to the general population as this is a convenient sample
• Non condom users may seek more STD services
• Low condom use among STD clinic attendees can be also interprited as non condom users seek more STD services
• Only last sexual exposure was considered
• Increase of injecting drug user population may be due to referral of IDU by the National Dangerous Drug control Board during the study period
38

Acknowledgement
• Director and Staff at NSACP
SLCOV
Dr.P.S.K.Gunathunga, Medical Officer NSACP
Dr. M. Jayalath, Medical Officer NSACP
Dr.R.C. Fernando Medical Officer NSACP
Dr.L.I. Rajapaksa, Consultant Venereologist,NSACP
39

40